Impact of the Built Environment and the Neighborhood in Promoting the Physical Activity and the Healthy Aging in Older People: An Umbrella Review

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
- lower rates of coronary heart disease, hypertension, stroke, diabetes, colon and breast cancer
- a higher level of cardiorespiratory and muscular fitness
- healthier body mass and composition and enhanced bone health
- higher levels of functional health, a lower risk of falling, and better cognitive function.
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Search Strategy
2.3. Study Selection and Data Extraction
2.4. Data Synthesis and Analysis
- Overall physical activity (PA), when the activity was not otherwise specified
- Leisure time physical activity (LTPA)
- Walking
- Active travel (AT), which means a mode of transport which involves physical activity to get from one destination to another [27].
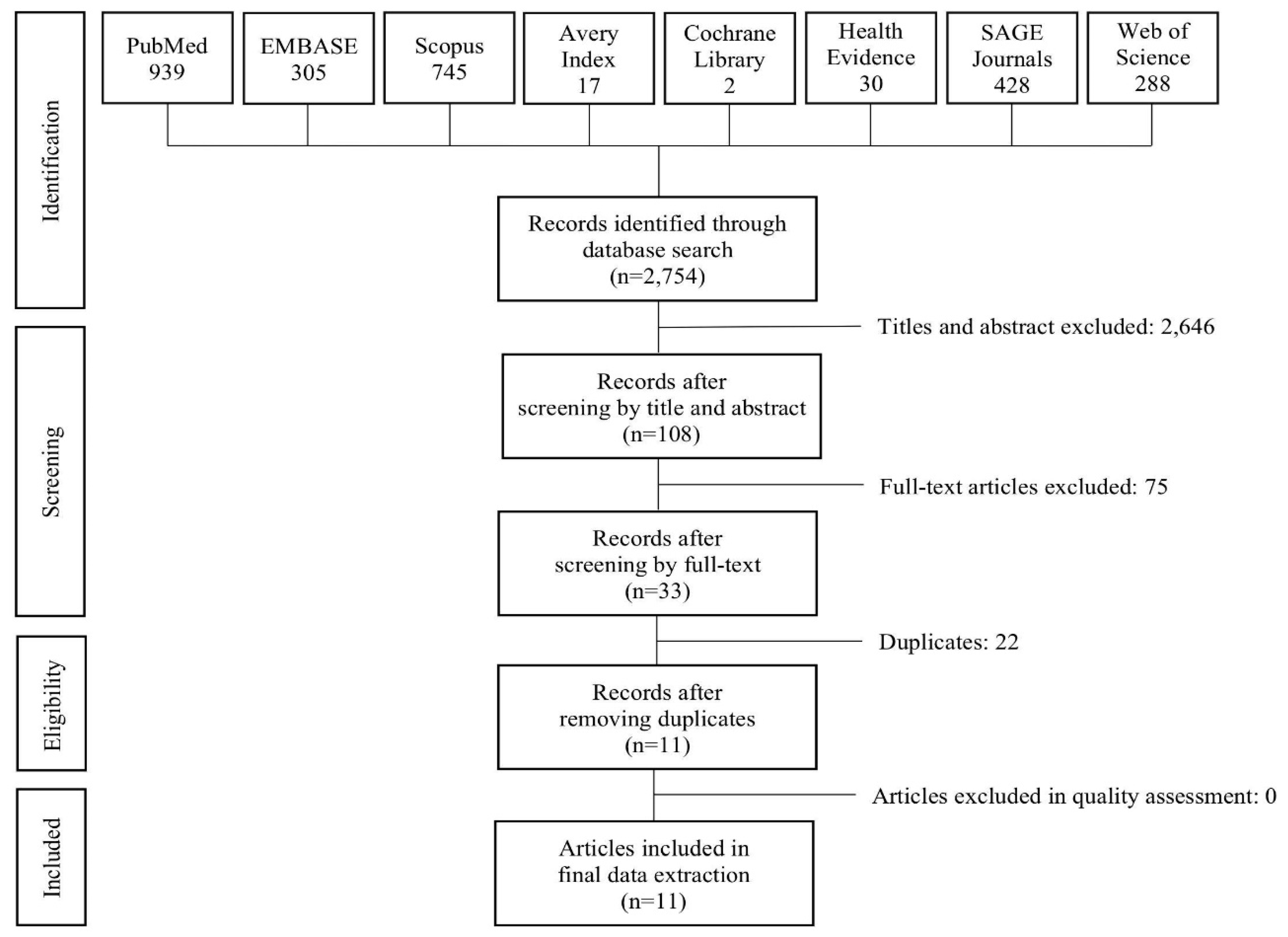
3. Results
3.1. Description of the Included Studies
3.2. Built Environment Features
3.3. Outcome Measures
3.4. Quality Assessment and Moderator of Associations
- individual moderators: sociodemographic (age, sex, level of education, income, employment status, race/ethnicity, marital status), health status/functionality, psychosocial factors, duration of residency, vehicle ownership or driving status;
- environmental moderators: area-level socioeconomic status, residential density/urbanization, pedestrian/cycling infrastructure and streetscape, aesthetics and cleanliness/order, safety and traffic, geographical scale, neighborhood definition).
3.5. Findings: Associations between Outcomes and Built Environment Features
4. Discussion
4.1. Built Environment Evidences
4.2. The Importance of the Local Context
4.3. Limits of the Reviews Included in the Umbrella
4.4. Limits of Our Review
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Search Strings
Appendix A.1. Pubmed
| 1 | ((((“Environment”[Mesh]) OR “Social Environment”[Mesh]) OR “Environment Design”[Mesh]) OR “Environment and Public Health”[Mesh]) OR “Built Environment”[Mesh] OR environment OR “built environment” OR “environment design” OR “social environment” OR “walkable environment” OR neighborhood OR “neighborhood design” | 8,250,202 |
| 2 | (“motor activity”[MeSH Terms] OR (“motor”[All Fields] AND “activity”[All Fields]) OR “motor activity”[All Fields]) OR (“exercise”[MeSH Terms] OR “exercise”[All Fields] OR (“physical”[All Fields] AND “activity”[All Fields]) OR “physical activity”[All Fields] OR “Walking”[Mesh] OR “walking” [All Fields] OR walk*) | 761,446 |
| 3 | #1 AND #2 | 318,600 |
| 4 | older* OR senior* OR elder* | 642,438 |
| 5 | #3 AND #4 | 33,182 |
| 6 | Health [MEsh] OR health* | 4,415,198 |
| 7 | #5 AND #6 | 21,104 |
| 8 | Review[ptyp] OR systematic[sb] OR Meta-Analysis[ptyp] | 2,542,516 |
| 7 | # 7 AND # 8 | 1878 |
| 8 | (“2004/01/01”[PDAT]: “2019/12/31”[PDAT]) | 13,652,503 |
| 9 | #7AND #8 | 1506 |
| 10 | “aged” [MeSH Terms] | 2,903,733 |
| 11 | #9 AND #10 | 913 |
| 1 | (built AND environment) OR (“built environment”) | 12,390 |
| 2 | older* OR senior* OR elder* | 642,245 |
| 3 | #1 AND #2 | 590 |
| 4 | (review AND systematic OR meta-analysis) | 391,036 |
| 5 | #3 AND #4 | 26 |
Appendix A.2. Sage Journals
| 1 | built environment OR neighborhood) AND (physical activity OR walk*) AND (old* OR elder* OR adult*) NOT adolescent* NOT therapy NOT fruit NOT child* Limits: years 2004–2019, review | 304 |
| 2 | [Title review] AND [All built] AND [[All environment] OR [All neighborhood]] AND [All physical] AND [[All activity] OR [All walk*]] AND [[All old*] OR [All elder*] OR [All adult*]] AND NOT [All adolescent*] AND NOT [All therapy] AND NOT [All fruit] AND NOT [All child*] Limits: years 2004–2019, research articles | 124 |
Appendix A.3. Health Evidence
| 1 | Built environment AND physical activity | 30 |
Appendix A.4. Cochrane Library
| 1 | Built environment | 2 |
Appendix A.5. EMBASE
| 1 | Built environment | 6638 |
| 2 | aging | 666,599 |
| 3 | #1 AND #2 | 216 |
| 4 | Physical activity OR walkability | 424,281 |
| 5 | #3 AND 4 | 93 |
| 6 | [systematic review]/lim OR [meta analysis]/lim | 279,440 |
| 7 | #5 AND #6 | 2 |
| 1 | Built environment | 6638 |
| 2 | Physical activity | 193,737 |
| 3 | #1 AND #2 | 1440 |
| 4 | [systematic review]/lim OR [meta analysis]/lim | 279,440 |
| 5 | #3 AND #4 | 50 |
| 6 | [2009–2019]/py | 13,972,704 |
| 7 | #5 AND #6 | 50 |
| 1 | (built AND environment) OR (“built environment”) | 12,688 |
| 2 | (older* OR senior* OR elder*) | 1,002,054 |
| 3 | #1 AND #2 | 763 |
| 4 | (review AND systematic OR meta–analysis) | 432,343 |
| 5 | #3 AND #4 | 29 |
| 6 | [2009–2019]/py | 13,972,704 |
| 7 | #5 AND #6 | 28 |
| 1 | (‘built environment’ OR ‘neighborhood’ OR ‘environment’) | 864,917 |
| 2 | (older* OR senior* OR elder*) | 4,178,606 |
| 3 | #1 AND #2 | 66,062 |
| 4 | (‘physical activity’ OR ‘walkability’) | 193,972 |
| 5 | #3 AND #4 | 4614 |
| 6 | [2009–2019]/py | 13,972,704 |
| 7 | #5 AND #6 | 3859 |
| 8 | [systematic review]/lim OR [meta analysis]/lim | 279,440 |
| 9 | #7 AND #8 | 72 |
| 1 | (‘environment’ OR ‘traffic and transport’ OR ‘walking’) | 972,155 |
| 2 | ‘health service’ | 533,699 |
| 3 | #1 AND #2 | 19,922 |
| 4 | (‘physical activity’ OR ‘walkability’) | 193,972 |
| 5 | #3 AND #4 | 4614 |
| 6 | (‘adult’ OR ‘aged’) | 8,449,129 |
| 7 | #5 AND #6 | 6123 |
| 8 | [2009–2019]/py | 13,972,704 |
| 9 | #7 AND #8 | 4088 |
| 10 | [review]/lim | 2,545,959 |
| 11 | #9 AND #10 | 153 |
Appendix A.6. SCOPUS
| 1 | (built environment OR neighborhood) AND (aging OR old* OR elder* OR adult*) AND (physical activity OR walk*) Limits: review and years 2004–2019 | 61 |
| 2 | built AND environment AND elderly AND population AND health AND review limit: years 2014–2019 | 25 |
| 3 | built AND environment AND elderly AND population limit: years 2014–2019 | 147 |
| 4 | (“built environment” OR “neighborhood environment”) AND (walking OR mobility) AND (adult OR aged OR “older adult”) limit: years 2014–2019 | 512 |
Appendix A.7. Avery Index
| 1 | Built environment OR neighborhood | 17 |
Appendix A.8. Web of Science
| 1 | (built environment OR neighborhood) AND (aging OR old* OR elder* OR adult *) AND (physical activity OR walk*) Limits: only review and years 2004–2019 | 220 |
| 2 | (“built environment” OR “neighborhood environment”) AND (walking OR mobility) AND (adult OR aged OR “older adult”) Limits: only review and years 2004–2019 | 68 |
Appendix B. Settings and Neighborhood Definitions of the Studies Included in the Reviews. For Every Review Included in the Paper Continent/Country, Urban/Rural Setting and Neighborhood Definition Used by the Included Studies Are Specified
| Author(s) (Year) | Continent/Country | Urban/Rural | Neighborhood Definition |
| Barnett et al. (2017) |
|
| Objective
|
| Cerin et al. (2017) |
|
| Objective
Perceived
|
| Cunningham & Michael (2004) |
| Defined by an index including suburban to traditional, transit accessibility, pedestrian accessibility, and neighborhood shopping, though no single definition is consistent. | |
| Gadais et al. (2018) | Canada 100% | x | x |
| Levasseur et al. (2015) | Asia 8% Europe 21%; North America 69%; South America 3%. |
| x |
| Moran et al. (2014) |
|
| x |
| Tuckett et al. (2018) | x | x | x |
| Van Cauwenberg et al. (2011) |
|
| Objective
|
| Van Cauwenberg et al. (2018) |
|
| Objective
Variable/not fixed: 5, 7%) Perceived
|
| Won et al. (2016) | USA 100% |
|
|
| Yen et al. (2009) |
| Objective
|
References
- Bangsbo, J.; Blackwell, J.; Boraxbekk, C.-J.; Caserotti, P.; Dela, F.; Evans, A.B.; Jespersen, A.P.; Gliemann, L.; Kramer, A.F.; Lundbye-Jensen, J.; et al. Copenhagen Consensus statement 2019: Physical activity and ageing. Br. J. Sports Med. 2019, 53, 856–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Promoting Health in the SDGs. Report on the 9th Global Conference for Health Promotion, Shanghai, China, 21–24 November 2016: All for Health, Health for All; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. World Report on Ageing and Health 2015. Available online: https://www.who.int/ageing/healthy-ageing/en/ (accessed on 4 June 2020).
- Law, M. The Environment: A Focus for Occupational Therapy. Can. J. Occup. Ther. 1991, 58, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Choo, J.; Kim, H.-J.; Park, S. Neighborhood Environments: Links to Health Behaviors and Obesity Status in Vulnerable Children. West. J. Nurs. Res. 2017, 39, 1169–1191. [Google Scholar] [CrossRef] [PubMed]
- United Nations, Department of Economic and Social Affairs, Population Division. 2019 Revision of World Population Prospects; United Nations: New York, NY, USA, 2019. [Google Scholar]
- United Nations, Department of Economic and Social Affairs, Population Division. World Urbanization Prospects: The 2018 Revision; United Nations: New York, NY, USA, 2019. [Google Scholar]
- Pinter-Wollman, N.; Jelic, A.; Wells, N.M. The impact of the built environment on health behaviours and disease transmission in social systems. Philos. Trans. R. Soc. B 2018, 373, 20170245. [Google Scholar] [CrossRef] [PubMed]
- Lenzi, M.; Vieno, A.; Santinello, M.; Perkins, D.D. How neighborhood structural and institutional features can shape neighborhood social connectedness: A multilevel study of adolescent perceptions. Am. J. Community Psychol. 2013, 51, 451–467. [Google Scholar] [CrossRef] [PubMed]
- Buffel, T.; Verté, D.; de Donder, L.; de Witte, N.; Dury, S.; Vanwing, T.; Bolsenbroek, A. Theorising the relationship between older people and their immediate social living environment. Int. J. Lifelong Educ. 2012, 31, 13–32. [Google Scholar] [CrossRef]
- Andrews, G.J.; Phillips, D.R. (Eds.) Ageing and Place: Perspectives, Policy, Practice. (Routledge Studies in Human Geography); Routledge: Abington, UK, 2004. [Google Scholar] [CrossRef]
- Bond, J.; Peace, S.; Dittmann-Kohli, F.; Westerhof, G.J. (Eds.) Ageing in Society: European Perspectives on Gerontology; SAGE Publications Ltd.: London, UK, 2007. [Google Scholar] [CrossRef]
- Gilleard, C.; Hyde, M.; Higgs, P. The Impact of Age, Place, Aging in Place, and Attachment to Place on the Well-Being of the Over 50s in England. Res. Aging 2007, 29, 590–605. [Google Scholar] [CrossRef]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.F.; Martin, B.W.; Alkandari, J.R.; Andersen, L.B.; Blair, S.N.; Brownson, R.C.; et al. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Kerr, J.; Rosenberg, D.; Frank, L. The Role of the Built Environment in Healthy Aging. J. Plan. Lit. 2012, 27, 43–60. [Google Scholar] [CrossRef]
- Owen, N.; Humpel, N.; Leslie, E.; Bauman, A.; Sallis, J.F. Understanding environmental influences on walking: Review and research agenda. Am. J. Prev. Med. 2004, 27, 67–76. [Google Scholar] [CrossRef]
- Valenti, G.; Bonomi, A.G.; Westerterp, K.R. Walking as a Contributor to Physical Activity in Healthy Older Adults: 2 Week Longitudinal Study Using Accelerometry and the Doubly Labeled Water Method. JMIR mHealth uHealth 2016, 4, e56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwasnicka, D.; Dombrowski, S.U.; White, M.; Sniehotta, F. Theoretical explanations for maintenance of behaviour change: A systematic review of behaviour theories. Health Psychol. Rev. 2016, 10, 277–296. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar] [CrossRef]
- Cerin, E.; Nathan, A.; van Cauwenberg, J.; Barnett, D.W.; Barnett, A. The neighbourhood physical environment and active travel in older adults: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Cauwenberg, J.; Nathan, A.; Barnett, A.; Barnett, D.W.; Cerin, E. Relationships Between Neighbourhood Physical Environmental Attributes and Older Adults’ Leisure-Time Physical Activity: A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 1635–1660. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews. Int. J. Evid. Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Updated March 2011; Cochrane: London, UK, 2011. [Google Scholar]
- Guyatt, G.H.; Haynes, R.B.; Jaeschke, R.Z.; Cook, D.J.; Green, L.; Naylor, C.D.; Wilson, M.C.; Richardson, W.S. Users’ guides to the medical literature: XXV. Evidence-based medicine: Principles for applying the users’ guides to patient care. J. Am. Med. Assoc. 2000, 284, 1290–1296. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Chin. Integr. Med. 2009, 7, 889–896. [Google Scholar] [CrossRef]
- Health Evidence, Quality Assessment Tool—Review Articles. 2015. Available online: https://www.healthevidence.org/documents/our-appraisal-tools/quality-assessment-tool-dictionary-en.pdf (accessed on 11 April 2020).
- Foley, L.; Dumuid, D.; Atkin, A.J.; Olds, T.; Ogilvie, D. Patterns of health behaviour associated with active travel: A compositional data analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 26. [Google Scholar] [CrossRef]
- Cunningham, G.O.; Michael, Y.L. Concepts guiding the study of the impact of the built environment on physical activity for older adults: A review of the literature. Am. J. Health Promot. 2004, 18, 435–443. [Google Scholar] [CrossRef]
- Tuckett, A.G.; Banchoff, A.W.; Winter, S.J.; King, A.C. The built environment and older adults: A literature review and an applied approach to engaging older adults in built environment improvements for health. Int. J. Older People. Nurs. 2018, 13, e12171. [Google Scholar] [CrossRef]
- Levasseur, M.; Généreux, M.; Bruneau, J.-F.; Vanasse, A.; Chabot, É.; Beaulac, C.; Bédard, M. Importance of proximity to resources, social support, transportation and neighborhood security for mobility and social participation in older adults: Results from a scoping study. BMC Public Health 2015, 15, 503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadais, T.; Boulanger, M.; Trudeau, F.; Rivard, M.C. Environments favorable to healthy lifestyles: A systematic review of initiatives in Canada. J. Sport Health Sci. 2018, 7, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Won, J.; Lee, C.; Forjuoh, S.N.; Ory, M.G. Neighborhood safety factors associated with older adults’ health-related outcomes: A systematic literature review. Soc. Sci. Med. 2016, 165, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Yen, I.H.; Michael, Y.L.; Perdue, L. Neighborhood environment in studies of health of older adults: A systematic review. Am. J. Prev. Med. 2009, 37, 455–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, D.W.; Barnett, A.; Nathan, A.; van Cauwenberg, J.; Cerin, E. Built environmental correlates of older adults’ total physical activity and walking: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moran, M.; Van Cauwenberg, J.; Hercky-Linnewiel, R.; Cerin, E.; Deforche, B.; Plaut, P. Understanding the relationships between the physical environment and physical activity in older adults: A systematic review of qualitative studies. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Cauwenberg, J.; de Bourdeaudhuij, I.; de Meester, F.; van Dyck, D.; Salmon, J.; Clarys, P.; Deforche, B. Relationship Between The Physical Environment And Physical Activity In Older Adults: A Systematic Review. Health Place 2011, 17, 458–469. [Google Scholar] [CrossRef]
- Marzetti, E.; Calvani, R.; Tosato, M.; Cesari, M.; di Bari, M.; Cherubini, A.; Broccatelli, M.; Savera, G.; D’Elia, M.; Pahor, M.; et al. Physical activity and exercise as countermeasures to physical frailty and sarcopenia. Aging Clin. Exp. Res. 2017, 29, 35–42. [Google Scholar] [CrossRef]
- Blanchet, S.; Chikhi, S.; Maltais, D. The benefits of physical activities on cognitive and mental health in healthy and pathological aging. Geriatr. Psychol. Neuropsychiatr. Vieil. 2018, 16, 197–205. [Google Scholar] [CrossRef]
- Gianfredi, V.; Blandi, L.; Cacitti, S.; Minelli, M.; Signorelli, C.; Amerio, A.; Odone, A. Depression and Objectively Measured Physical Activity: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 3738. [Google Scholar] [CrossRef]
- Borchardt, J.L.; Paulitsch, R.G.; Dumith, S.C. The influence of built, natural and social environment on physical activity among adults and elderly in southern Brazil: A population-based study. Int. J. Public Health 2019, 64, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Lovasi, G.S.; Jacobson, J.S.; Quinn, J.W.; Neckerman, K.M.; Ashby-Thompson, M.N.; Rundle, A. Is the environment near home and school associated with physical activity and adiposity of urban preschool children? J. Urban. Health 2011, 88, 1143–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Parameter | Description |
|---|---|
| Population | Inclusion—Older adults, noninstitutionalized self-sufficient citizens Exclusion—Children, adolescents, young adults, institutionalized/hospitalized, housebound |
| Intervention | Features of built environment: street connectivity and grid pattern, road signs, easy access to the structures, parking for bicycles, street lights, presence of underpasses, walking trails, sidewalks, biking trails, structure and street security, reduction of road traffic, ad hoc structures (gyms, dancing halls), open spaces, benches, shaded areas, access to transport (bicycles), presence of handrails, presence of stairs and steps |
| Comparison | No intervention—Absence of the selected features of built environment |
| Outcome | Inclusion—Promotion of physical activity and movement Exclusion—Other health outcomes |
| Study design | Inclusion: review |
| Author(s) (Year) | Type of Study Population | Number and Type of Included Studies | Environmental Features/Factors | Environmental Features Measurement | Outcome (Physical Activity) | Physical Activity Measurement | Measure of Association | Conclusion | Qualitative Evaluation |
|---|---|---|---|---|---|---|---|---|---|
| Barnett et al. (2017) | Systematic review and meta-analysis Older adults ≥65 years old | 100 Cross-sectional, longitudinal and quasi-experimental | NEWS categories:
| Total environmental attributes: Objective: 48%, Perceived: 52% Specifically:
| Total physical activity (PA) and walking | Total PA outcomes: Objective: 27%, Self-reported: 74% Specifically:
| Meta-analytic approach + quality assessment | Positive association with total physical activity for:
| 10 |
| Cerin et al. (2017) | Systematic review and meta-analysis Older adults ≥65 years old | 42 Cross-sectional and longitudinal and quasi-experimental | NEWS categories:
| Total environmental attributes: Objective: 33%, Perceived: 68% Specifically:
| Active travel (AT*) categorized into:
| Self-reported: 100% | Meta-analytic approach + quality assessment | Positive associations with all active travel for:
| 10 |
| Cunningham and Michael (2004) | Literature review Older adults | 6 out of 27 NA | Safety Aesthetics Convenience or access to facilities Microscale urban design Land-use mix |
| Physical activity, walking | NA | NA | Associations with physical activity for:
| 5 |
| * Gadais et al. (2018) | Systematic review Elderly involved in 9% of the studies | 264 (19 about seniors) Quantitative, qualitative and mixed studies, situation and literature reviews |
| *—Survey: 45%
| Physical activity and active travel | NA | NA | * Recommendations for improving physical activity:
| 8 |
| Levasseur et al. (2015) | Scoping review Older adults | 39 out of 50 Cross-sectional, longitudinal and qualitative studies | Environment categories according to International Classification of Functioning, Disability and Health (ICF):
| Neighborhood measures: Objective: 14%, Subjective: 68%, Both: 18%. | Mobility | Objectively: 18%, Self-reported: 82%. | Sum of associations of single articles | Main positive association with mobility for:
| 9 |
| Moran et al. (2014) | Systematic reviewOlder adults ≥65 years old | 31 Qualitative and mix studies | Categorization done by authors:
| Indoor interviews (individual or focus groups): 68% Spatial qualitative methods: 32%
| Physical activity | NA | Sum of associations of single articles | Possible association with physical activity for: Pedestrian infrastructure:
| 10 |
| Tuckett et al. (2018) | Integrative literature review Older adults | NA NA | NA | NA | Physical activity | NA | NA | Physical activity associated with neighborhood walkability which relates to:
| 7 |
| Van Cauwenberg et al.(2011) | Systematic review Older adults ≥65 years old | 31 Cross-sectional and longitudinal | NEWS categories:
|
| Physical activity (PA):
| Objective: 6% Subjective: 94% | Sum of associations of single articles | Results were inconsistent but most of the studied environmental characteristics that were reported were not related to PA **. | 8 |
| Van Cauwenberg et al. (2018) | Systematic review and meta-analysis Older adults ≥65 years old | 72 Cross-sectional and longitudinal | NEWS categories:
| Total environmental attributes: Objective: 42%, Perceived: 63% Specifically:
| Physical activity during leisure-time (LTPA):
| Self-reported: 100% | Meta-analytic approach + quality assessment | Positive associations with leisure-time walking for:
| 10 |
| Won et al. (2016) | Systematic reviewOlder adults ≥50 years old | 16 out of 32 Cross-sectional and longitudinal | Four domains of neighborhood safety:
| Total environmental attributes: Objective: 6%, Subjective: 69%, Both: 25% Specifically:
| Physical activity and walking |
| NA | Associations of traffic-related safety consistently significant for physical activity =Associations of crime-related safety consistently significant for walking | 9 |
| Yen et al. (2009) | Systematic reviewOlder adults ≥55 years old | 7 out of 33 Cross-sectional and longitudinal |
|
| Physical activity, walking | NA | NA | Associations with PA ** for:
| 8 |
| Health Behaviors | Built Environment Factors | Reference of Associations (+) | Reference of Associations (−) |
|---|---|---|---|
| Overall physical activity | Walkability | Barnett et al. (2017) Tuckett et al. (2018) | |
| Land-use mix | Cunningham and Michael (2004) Tuckett et al. (2018) | ||
| Street connectivity | Tuckett et al. (2018) | ||
| Overall access to facilities | Barnett et al. (2017) Cunningham and Michael (2004) Levasseur et al. (2015) Moran et al. (2014) Tuckett et al. (2018) Yen et al. (2009) | ||
| Access to shops/commercial | Barnett et al. (2017) Tuckett et al. (2018) | ||
| Poor pedestrian access to shopping centers | Tuckett et al. (2018) | ||
| Access to public transport | Barnett et al. (2017) Levasseur et al. (2015) Moran et al. (2014) Tuckett et al. (2018) | ||
| Access to nature/parks/open space | Barnett et al. (2017) Levasseur et al. (2015) Moran et al. (2014) Yen et al. (2009) | ||
| Access to recreational facilities | Barnett et al. (2017) Levasseur et al. (2015) Moran et al. (2014) Tuckett et al. (2018) | ||
| Access to places for social interaction | Levasseur et al. (2015) Tuckett et al. (2018) | ||
| Access to exercise opportunities (senior oriented group activities) | Moran et al. (2014) | ||
| Access to rest areas —Seating Benches, public washrooms | Tuckett et al. (2018) —Levasseur et al. (2015) Moran et al. (2014) | ||
| Pedestrian-friendly infrastructure —Footpath quality, lack of hills Footpath quality ■ Sidewalk characteristics: presence and continuity, quality and maintenance, slopes and curbs, temporary obstacles on sidewalks ■ Separation between pedestrians and other nonmotorized transport | Barnett et al. (2017) Gadais et al. (2018) —Cunningham and Michael (2004) Levasseur et al. (2015) Tuckett et al. (2018) ■ Moran et al. (2014) | ||
| Poor pedestrian-friendly infrastructure —Footpath quality | Levasseur et al. (2015) —Yen et al. (2009) | ||
| Pedestrian/cycling facilities | Levasseur et al. (2015) | ||
| Aesthetics —Greenery/Aesthetically pleasing scenery Buildings and streetscape/Natural scenery | Levasseur et al. (2015) —Barnett et al. (2017) —Tuckett et al. (2018) Moran et al. (2014) | ||
| Lack of aesthetically pleasing scenery | Cunningham and Michael (2004) | ||
| Crime-related safety —Street lighting | Barnett et al. (2017) Tuckett et al. (2018) —Levasseur et al. (2015) | ||
| Crime-related safety —Unattended dogs, inadequate lighting Lack of street lighting and upkeep | Levasseur et al. (2015) —Cunningham and Michael (2004) Moran et al. (2014) | ||
| Traffic-related safety —Zebra-crossing characteristics Signaled crosswalks | Won et al. (2016) —Moran et al. (2014) Tuckett et al. (2018) | ||
| Traffic | Levasseur et al. (2015) | ||
| High environmental quality | Moran et al. (2014) | ||
| Pollution | Moran et al. (2014) | ||
| Noise | Cunningham and Michael (2004) | ||
| Leisure time walking, Leisure time physical activity | Walkability | Van Cauwenberg et al. (2018) | |
| Land-use mix—access | Van Cauwenberg et al. (2018) | ||
| Aesthetically pleasing scenery | Van Cauwenberg et al. (2018) | ||
| Access to public transit | Van Cauwenberg et al. (2018) | ||
| Access to recreational facilities | Van Cauwenberg et al. (2018) | ||
| Access to park/open space | Van Cauwenberg et al. (2018) | ||
| Barriers to walking/cycling | Van Cauwenberg et al. (2018) | ||
| Active travel | Walkability | Cerin et al. (2017) | |
| Residential density/urbanization | Cerin et al. (2017) | ||
| Street connectivity | Cerin et al. (2017) | ||
| Overall access to facilities, destinations and services | Cerin et al. (2017) Gadais et al. (2018) | ||
| Land-use mix—destination diversity | Cerin et al. (2017) | ||
| Access to shops/commercial | Cerin et al. (2017) | ||
| Access to food outlets | Cerin et al. (2017) | ||
| Access to business/institutional/industrial destinations | Cerin et al. (2017) | ||
| Access to public transport | Cerin et al. (2017) | ||
| Access to parks/open space/recreation | Cerin et al. (2017) Gadais et al. (2018) | ||
| Pedestrian-friendly infrastructure —Footpath quality, pedestrian crossing | Cerin et al. (2017) —Gadais et al. (2018) | ||
| Pedestrian/cycling facilities | Gadais et al. (2018) | ||
| Availability of benches/sitting facilities | Cerin et al. (2017) | ||
| Street lighting | Cerin et al. (2017) Gadais et al. (2018) | ||
| Easy access to building entrance Wheelchair access, walking access | Cerin et al. (2017) Gadais et al. (2018) | ||
| Human and motorized traffic volume | Cerin et al. (2017) | ||
| Littering/vandalism/decay | Cerin et al. (2017) | ||
| Walking | Walkability | Barnett et al. (2017) Yen et al. (2009) | |
| Residential density/urbanization —Density of physical activity facilities | Barnett et al. (2017) Yen et al. (2009) | ||
| Street connectivity | Yen et al. (2009) | ||
| Overall access to facilities, destinations and services | Barnett et al. (2017) Cunningham and Michael (2004) Yen et al. (2009) | ||
| Access to shops/commercial | Barnett et al. (2017) | ||
| Access to public transport | Barnett et al. (2017) | ||
| Access to nature/parks/open space | Barnett et al. (2017) Yen et al. (2009) | ||
| Pedestrian-friendly infrastructure | Barnett et al. (2017) Yen et al. (2009) | ||
| Greenery/aesthetically pleasing scenery | Barnett et al. (2017) | ||
| Street lighting | Barnett et al. (2017) | ||
| Crime-related safety | Barnett et al. (2017) Cunningham and Michael (2004) Won et al. (2016) Yen et al. (2009) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonaccorsi, G.; Manzi, F.; Del Riccio, M.; Setola, N.; Naldi, E.; Milani, C.; Giorgetti, D.; Dellisanti, C.; Lorini, C. Impact of the Built Environment and the Neighborhood in Promoting the Physical Activity and the Healthy Aging in Older People: An Umbrella Review. Int. J. Environ. Res. Public Health 2020, 17, 6127. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176127
Bonaccorsi G, Manzi F, Del Riccio M, Setola N, Naldi E, Milani C, Giorgetti D, Dellisanti C, Lorini C. Impact of the Built Environment and the Neighborhood in Promoting the Physical Activity and the Healthy Aging in Older People: An Umbrella Review. International Journal of Environmental Research and Public Health. 2020; 17(17):6127. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176127
Chicago/Turabian StyleBonaccorsi, Guglielmo, Federico Manzi, Marco Del Riccio, Nicoletta Setola, Eletta Naldi, Chiara Milani, Duccio Giorgetti, Claudia Dellisanti, and Chiara Lorini. 2020. "Impact of the Built Environment and the Neighborhood in Promoting the Physical Activity and the Healthy Aging in Older People: An Umbrella Review" International Journal of Environmental Research and Public Health 17, no. 17: 6127. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176127