Association of Blood Cadmium with Cardiovascular Disease in Korea: From the Korea National Health and Nutrition Examination Survey 2008–2013 and 2016


Abstract
:1. Introduction
2. Subjects and Methods
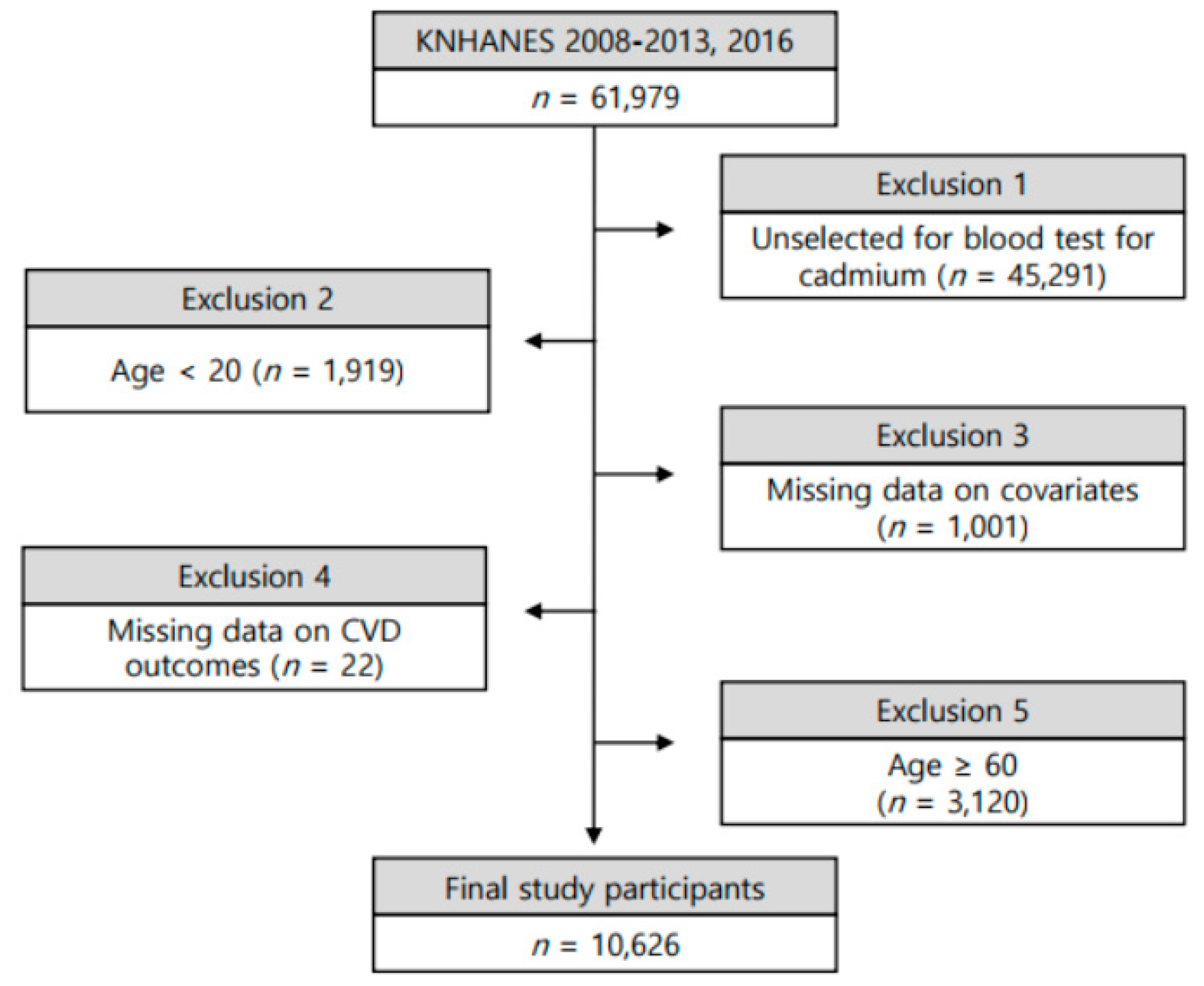
2.1. Study Population
2.2. Covariate Variables and CVD Outcomes
2.3. Determination of BCd Levels
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics and BCd Concentrations
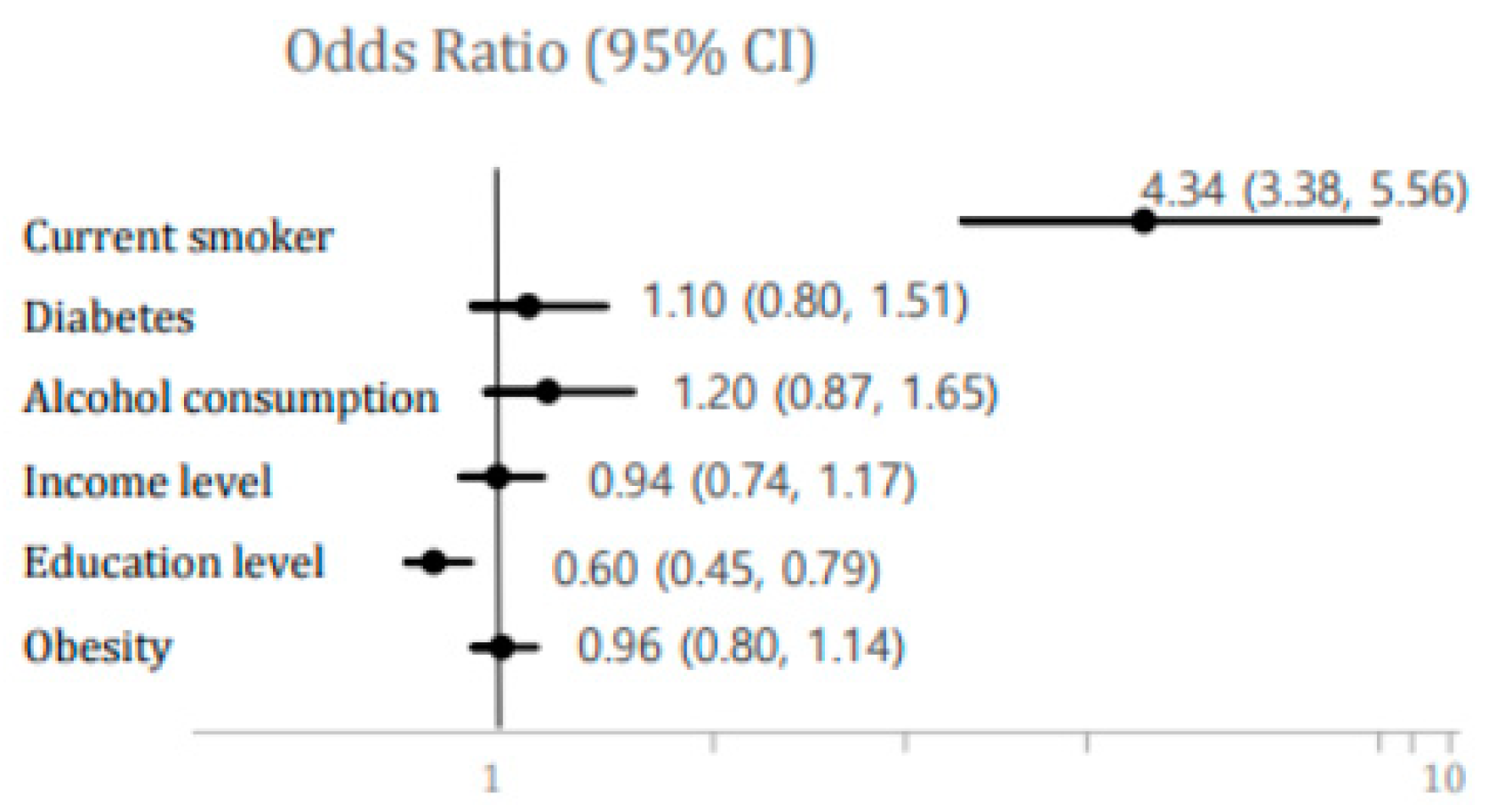
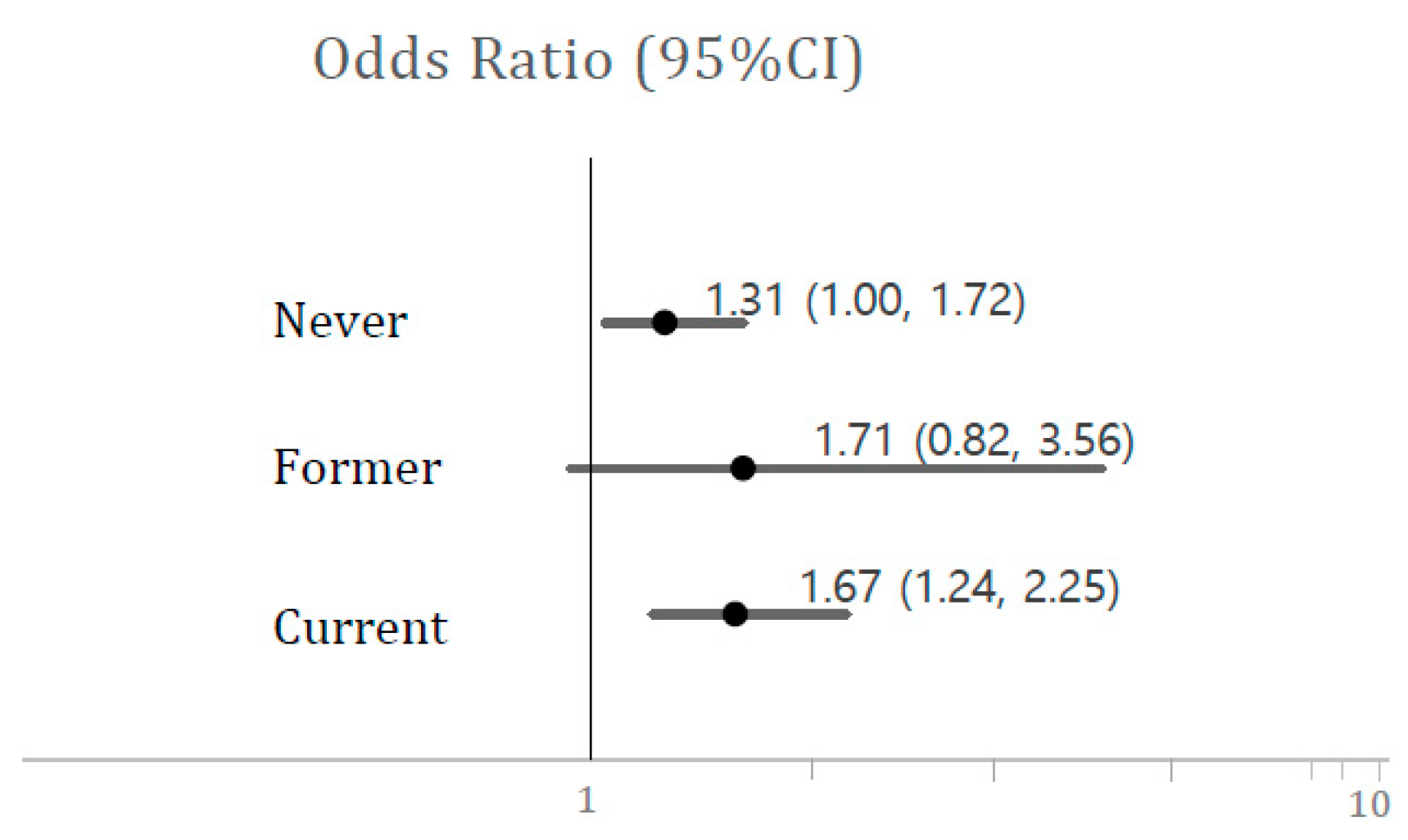
3.2. Related Factor with High Blood Cadmium
3.3. Associations between High BCd Level and Risks of Stroke, IHD, and Hypertension
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). About Cardiovascular Disease. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases (accessed on 1 July 2020).
- Murray, J.L.C.; Phil, D.; Lopez, A.D. Measuring the Global Burden of Disease. N. Engl. J. Med. 2013, 369, 448–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mensah, G.A.; Wei, G.S.; Sorlie, P.D.; Fine, L.J.; Rosenberg, Y.; Kaufmann, P.G.; Mussolino, M.E.; Hsu, L.L.; Addou, E.; Engelgau, M.M.; et al. Decline in cardiovascular mortality: Possible causes and implications. Circ. Res. 2017, 120, 366–380. [Google Scholar] [CrossRef]
- Feigin, V.V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and regional burden of stroke during 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2014, 383, 245–255. [Google Scholar] [CrossRef]
- Rosengren, A.; Giang, K.W.; Lappas, G.; Jern, C.; Torén, K.; Björck, L. Twenty-four-year trends in the incidence of ischemic stroke in Sweden from 1987 to 2010. Stroke 2013, 44, 2388–2393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kissela, B.M.; Khoury, J.C.; Alwell, K.; Moomaw, C.J.; Woo, D.; Adeoye, O.; Flaherty, M.L.; Khatri, P.; Ferioli, S.; la Rosa, F.D.; et al. Age at stroke: Temporal trends in stroke incidence in a large, biracial population. Neurology 2012, 79, 1781–1787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Venecia, T.; Lu, M.; Figueredo, V.M. Hypertension in young adults. Postgrad. Med. 2016, 128, 201–207. [Google Scholar] [CrossRef]
- Association American Heart and Stroke Association. Older Americans & Cardiovascular Disease. Statistical Fact Sheet 2016 Update; American Heart Association: Dallas, TX, USA, 2016. [Google Scholar]
- Chen, R.L.; Joyce, S.B.; Esiri, M.M.; Chen, L.-K.; Buchan, A.M. Ischemic stroke in the elderly: An overview of evidence. Nat. Rev. Neurol. 2010, 6, 256–265. [Google Scholar] [CrossRef]
- Chen, Y.; Lin, Y.; Po, H.L. Comparison of the risk factor profile, stroke subtypes, and outcomes between stroke patients aged 65 years or younger and elderly stroke patients: A hospital-based study. Int. J. Gerontol. 2013, 7, 205–208. [Google Scholar] [CrossRef] [Green Version]
- Poisson, S.N.; Schardt, T.Q.; Dingman, A.; Bernard, T.J. Etiology and treatment of arterial ischemic stroke in children and young adults. Curr. Treat. Options Neurol. 2014, 16, 315. [Google Scholar] [CrossRef]
- Fu, G.-U.; Yuan, W.-E.; Du, W.-A.; Yang, Z.-H.; Fu, N.; Zheng, H.-U.; Li, Z.-I.; Huang, Y.-U.; Zhang, Y.-U.; Dai, G.-U.; et al. Risk factors associated with recurrent strokes in young and elderly patients: A hospital-based study. Int. J. Gerontol. 2015, 9, 63–66. [Google Scholar] [CrossRef] [Green Version]
- Lei, L.; Bin, Z. Risk Factor Differences in Acute Myocardial Infarction between young and older people: A systematic review and meta-analysis. Int. J. Cardiovasc. Sci. 2019, 32, 163–176. [Google Scholar] [CrossRef]
- Putaala, J.; Metso, A.J.; Metso, T.M.; Konkola, N.; Kraemer, Y.; Haapaniemi, E.; Kaste, M.; Tatlisumak, T. Analysis of 1008 consecutive patients aged 15 to 49 with first-ever ischemic stroke the helsinki young stroke registry. Stroke 2009, 40, 1195–1203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, W.-O.; Kim, E.-U.; Kim, J.G.; Kim, J.-E.; Kim, J.Y.; Kang, K.; Kang, J.; Koo, J.; Kim, D.; Kim, B.J.; et al. Executive summary of stroke statistics in Korea 2018: A Report from the epidemiology research council of the Korean stroke society. J. Stroke 2019, 21, 42–59. [Google Scholar] [CrossRef] [PubMed]
- Caine, E.D. Health risks from toxic pollution. Lancet 2012, 380, 1532. [Google Scholar] [CrossRef]
- Blacksmith Institute Green Cross. The World’s Worst Pollution Problems: Assessing Health Risks at Hazarous Waste Sites; Blacksmith Institute: New York, NY, USA, 2012. [Google Scholar]
- Järup, L. Hazards of heavy metal contamination. Br. Med. Bull. 2003, 68, 167–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhury, R.; Ramond, A.; O’Keeffe, L.M.; Shahzad, S.; Kunutsor, S.K.; Muka, T.; Gregson, J.; Willeit, P.; Warnakula, S.; Khan, H.; et al. Environmental toxic metal contaminants and risk of cardiovascular disease; systematic review and meta-analysis. BMJ 2018, 362, k3310. [Google Scholar] [CrossRef] [Green Version]
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Cadmium. 2012. Available online: http://www.atsdr.cdc.gov/toxprofiles/tp5.pdf (accessed on 6 July 2020).
- Jarup, L.; Berglund, M.; Elinder, C.G.; Nordberg, G.; Vahter, M. Health effects of cadmium exposure—A review of the literature and a risk estimate. Scand. J Work Environ Health. 1998, 24, 1–51. [Google Scholar]
- Satarug, S.; Moore, M.R. Adverse health effects of chronic exposure to low-level cadmium in foodstuffs and cigarette smoke. Environ. Health Perspect. 2004, 112, 1099–1103. [Google Scholar] [CrossRef]
- Schoeters, G.; den Hond, E.; Zuurbier, M.; Naginiene, R.; van den Hazel, P.; Stilianakis, N.; Ronchetti, R.; Koppe, J.G. Cadmium and children: Exposure and health effects. Acta Pædiatr. 2006, 95 (Suppl. 453), 50–54. [Google Scholar] [CrossRef]
- Mortada, W.I.; Sobh, M.A.; El-Defrawy, M.M. The exposure to cadmium, lead and mercury from smoking and its impact on renal integrity. Med. Sci. Monit. 2004, 10, CR112–CR116. [Google Scholar]
- Agency for Toxic Substanced and Disease Registry (ATSDR). Public Health Statement for Cadmium; ATSDR: Atlanta, GA, USA, 2008. [Google Scholar]
- Korean Statistical Information Service (KOSIS). Daily Cigarette Smoking: ≥19 Years, by Sex (Period: Annual 1998~2018). Available online: https://kosis.kr/eng/statisticsList/statisticsListIndex.do?menuId=M_01_01&vwcd=MT_ETITLE&parmTabId=M_01_01&parentId=F.1;F_17.2;117_11702_A01.3;117_11702_A01_011.4;#SelectStatsBoxDiv (accessed on 2 July 2020).
- Messner, B.; Bernhard, D. Cadmium and cardiovascular diseases: Cell biology, pathophysiology, and epidemiological relevance. Biometals 2010, 23, 811–822. [Google Scholar] [CrossRef]
- Olszowski, T.; Baranowska-Bosiacka, I.; Gutowska, I.; Piotrowska, K.; Mierzejewska, K.; Korbecki, J.; Kurzawski, M.; Tarnowski, M.; Chlubek, D. The Effects of Cadmium at Low Environmental Concentrations on THP-1 Macrophage Apoptosis. Int. J. Mol. Sci. 2015, 16, 21410–21427. [Google Scholar] [CrossRef] [Green Version]
- Tellez-Plaza, M.; Jones, M.R.; Dominguez-Lucas, A.; Guallar, E.; Navas-Acien, A. Cadmium exposure and clinical cardiovascular disease: A systematic review. Curr. Atheroscler. Rep. 2013, 15, 356. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Park, S.K.; Hu, H.; Lee, S. Cadmium exposure and cardiovascular disease in the 2005 Korea National Health and Nutrition Examination Survey. Environ. Res. 2011, 111, 171–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, J.-Y.; Kim, J.-M.; Kim, Y. The association of heavy metals in blood, fish consumption frequency, and risk of cardiovascular diseases among Korean adults: The Korean National Health and Nutrition Examination Survey (2008–2010). Korean J. Nutr. 2012, 45, 347–361. [Google Scholar] [CrossRef] [Green Version]
- Eum, K.D.; Lee, M.S.; Paek, D. Cadmium in blood and hypertension. Sci. Total Environ. 2008, 407, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.K.; Kim, Y. Association of blood cadmium with hypertension in the Korean general population: Analysis of the 2008–2010 Korean National Health and Nutrition Examination Survey data. Am. J. Ind. Med. 2012, 55, 1060–1067. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.-Y.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-O.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Han, S.-U.; Bae, K.-W.; Lee, H.-Y.; Kim, S.-E.; Cho, H.-Y. Association between regular walking and periodontitis according to socioeconomic status: A cross-sectional study. Sci. Rep. 2019, 9, 12969. [Google Scholar] [CrossRef]
- Shin, J.-Y. Trends in the prevalence and management of diabetes in Korea: 2007–2017. Epidemiol. Health 2019, 41, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.-I.; Kim, S.-U.; Cho, J.H.; Yoon, C.-H.; Hwang, S.-E.; Lee, H.-A.; Youn, T.-A.; Chae, I.-N.; Kim, C.-H. Prevalence, awareness, treatment, and control of hypertension in Korea. Sci. Rep. 2019, 9, 10970. [Google Scholar] [CrossRef] [Green Version]
- Ahn, J.; Kim, N.; Lee, B.; Park, J.; Kim, Y. Association of blood pressure with blood lead and cadmium levels in Korean adolescents: Analysis of data from the 2010–2016 Korean National Health and Nutrition Examination Survey. J. Korean Med. Sci. 2018, 33, e278. [Google Scholar] [CrossRef] [PubMed]
- Ahn, B.; Kim, S.H.; Park, M.J. Blood cadmium concentrations in Korean adolescents: From the Korea ational Health and Nutrition Examination Survey 2010–2013. Int. J. Hyg. Environ. Health 2017, 220, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Kang, G.H.; Uhm, J.Y.; Choi, Y.G.; Kang, E.K.; Kim, S.Y.; Choo, W.O.; Chang, S.S. Environmental exposure of heavy metal (lead and cadmium) and hearing loss: Data from the Korea National Health and Nutrition Examination Survey (KNHANES 2010–2013). Ann. Occup. Environ. Med. 2018, 30, 22. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.-Y.; Kim, Y. Iron deficiency is associated with increased levels of blood cadmium in the Korean general population: Analysis of 2008–2009 Korean National Health and Nutrition Examination Survey data. Environ. Res. 2012, 112, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Lee, S.; Roh, J.; Won, J.-O.; Yoon, J.-I. The association between involuntary smoking exposure with urine cotinine level and blood cadmium level in general non-smoking populations. J. Korean Med. Sci. 2017, 32, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Johri, N.; Jacquillet, G.; Unwin, R. Heavy metal poisoning: The effects of cadmium on the kidney. Biometals 2010, 23, 783–792. [Google Scholar] [CrossRef]
- Järup, L.; Åkesson, A. Current status of cadmium as an environmental health problem. Toxicol. Appl. Pharmacol. 2009, 238, 201–208. [Google Scholar] [CrossRef]
- Tinkov, A.A.; Filippini, T.; Ajsuvakova, O.P.; Skalnaya, M.G.; Aaseth, J.; Bjørklund, G.; Gatiatulina, E.R.; Popova, E.V.; Nemereshina, O.N.; Huang, P.-A.; et al. Cadmium and atherosclerosis: A review of toxicological mechanisms and a meta-analysis of epidemiologic studies. Environ. Res. 2018, 162, 240–260. [Google Scholar] [CrossRef]
- Borne, Y.; Fagerberg, B.; Persson, M.; Ostling, G.; Soderholm, M.; Hedblad, B.; Sallsten, G.; Barregard, L.; Engstrom, G. Cadmium, carotid atherosclerosis, and incidence of ischemic stroke. J. Am. Heart Assoc. 2017, 6, e006415. [Google Scholar] [CrossRef] [Green Version]
- Wen, Y.; Huang, S.; Zhang, Y.; Zhang, H.; Zhou, L.; Li, D.-Y.; Xie, C.; Lv, Z.; Guo, Y.; Ke, Y.; et al. Associations of multiple plasma metals with the risk of ischemic stroke: A case-control study. Environ. Int. 2019, 125, 125–134. [Google Scholar] [CrossRef]
- Tellez-Plaza, M.; Navas-Acien, A.; Crainiceanu, C.M.; Guallar, E. Cadmium exposure and hypertension in the 1999–2004 National Health and Nutrition Examination Survey (NHANES). Environ. Health Perspect. 2008, 116, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Nordberg, G.F.; Nogawa, K.; Nordberg, M.; Friberg, L. Cadmium. In Handbook on the Toxicology of Metals; Nordberg, G.F., Fowler, B.A., Nordberg, M., Friberg, L., Eds.; Elsevier: Amsterdam, The Netherlands, 2007; pp. 445–486. [Google Scholar]
- Nordberg, M.; Jin, T.; Nordberg, G.F. Cadmium, metallothionein and renal tubular toxicity. IARC Sci. Publ. 1992, 118, 293–297. [Google Scholar]
- Valko, M.; Morris, H.; Cronin, M.T. Metals, toxicity and oxidative stress. Curr. Med. Chem. 2005, 12, 1161–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lall, S.B.; Das, N.; Rama, R.; Peshin, S.S.; Khattar, S.; Gulati, K.; Seth, S.D. Cadmium induced nephrotoxicity in rats. Indian J. Exp. Biol. 1997, 35, 151–154. [Google Scholar]
- S-enes, M.; Kazan, N.; Cos-kun, O.; Zengi, O.; I˙nan, L.; Yu, D. Oxidative and nitrosative stress in acute ischaemic stroke. Ann. Clin. Biochem. 2007, 44, 43–47. [Google Scholar] [CrossRef]
- Angeli, J.K.; Pereira, C.A.C.; Faria, T.D.; Stefanon, I.; Padilha, A.S.; Vassallo, D.V. Cadmium exposure induces vascular injury due to endothelial oxidative stress: The role of local angiotensin II and COX-2. Free Rad. Biol. Med. 2013, 65, 838–848. [Google Scholar] [CrossRef] [Green Version]
- Mijal, R.S.; Holzman, C.B. Blood Cadmium Levels in Women of Childbearing Age Vary by Race/Ethnicity. Environ. Res. 2010, 110, 505–512. [Google Scholar] [CrossRef] [Green Version]
- United Stated Environmental Protection Agency (USEPA). Integrated Risk Information System (IRIS) Assessment for Cadmium. 1994. Available online: https://cfpub.epa.gov/ncea/iris/iris_documents/documents/subst/0141_summary.pdf (accessed on 5 August 2020).
- Kurihara, I.; Kobayashi, E.; Suwazono, Y.; Uetani, M.; Inaba, T.; Oishiz, M.; Kido, T.; Nakagawa, H.; Nogawa, K. Association between exposure to cadmium and blood pressure in Japanese peoples. Arch. Environ. Health 2004, 59, 711–716. [Google Scholar] [CrossRef]
- Borne, Y.; Barregard, L.; Persson, M.; Hedblad, B.; Fagerberg, B.; Engstrom, G. Cadmium exposure and incidence of heart failure and atrial fibrillation: A population-based prospective cohort study. BMJ Open 2015, 5, e007366. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (US). How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2010; ISBN 978-0-16-084078-4. [Google Scholar]
- Muthusamy, S.; Peng, C.; Ng, J.C. Effects of binary mixtures of benzo[a]pyrene, arsenic, cadmium, and lead on oxidative stress and toxicity in HepG2 cells. Chemosphere 2016, 165, 41–51. [Google Scholar] [CrossRef]
- Pappas, R.S. Toxic elements in tobacco and in cigarette smoke; inflammation and sensitization. Metallomics 2011, 3, 1181–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willerson, J.T.; Ridker, P.M. Inflammation as a Cardiovascular Risk Factor. Circulation 2004, 109 (Suppl. II), II-2–II-10. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.J.; Park, J.H.; Jo, C.; Yoon, K.; Koh, Y.H. Cigarette smoke extracts and cadmium induce COX-2 expression through γ-secretase mediated p38 MAPK activation in C6 astroglia cells. PLoS ONE 2019, 14, e0212749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conolly, R.B.; Lutz, W.K. Nonmonotonic dose-response relationships: Mechanistic basis, kinetic modeling, and implications for risk assessment. Toxicol. Sci. 2004, 77, 151–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarup, L.; Rogenfelt, A.; Elinder, C.G.; Nogawa, K.; Kjellstrom, T. Biological half-time of cadmium in the blood of workers after cessation of exposure. Scand. J. Work Environ. Health 1983, 9, 327–331. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 10,626) | Non-High BCd (n = 9565) | High BCd (n = 1061) | p-Value b | ||||
|---|---|---|---|---|---|---|---|
| Variables | Mean ± SD | Mean ± SD | Mean ± SD | ||||
| Age (years) | 40.14 ± 11.19 | 39.37 ± 11.17 | 47.12 ± 8.74 | <0.0001 | |||
| Age | n | weighted % (SE) | n | weighted % (SE) | n | weighted % (SE) | |
| 20–29 | 2426 | 22.81 (0.43) | 2369 | 24.66 (0.47) | 57 | 5.83 (0.89) | <0.0001 |
| 30–39 | 2711 | 26.27 (0.43) | 2564 | 27.54 (0.47) | 147 | 14.62 (1.29) | |
| 40–49 | 2740 | 27.66 (0.39) | 2370 | 26.51 (0.43) | 370 | 38.22 (1.68) | |
| 50–59 | 2749 | 23.26 (0.37) | 2262 | 21.29 (0.39) | 487 | 41.33 (1.69) | |
| Sex | |||||||
| Male | 5081 | 50.37 (0.38) | 4702 | 51.71 (0.42) | 379 | 38.10 (1.69) | <0.0001 |
| Female | 5545 | 49.63 (0.38) | 4863 | 48.29 (0.42) | 682 | 61.90 (1.69) | |
| Smoking status | |||||||
| Never | 5947 | 54.41 (0.49) | 5365 | 54.56 (0.52) | 582 | 53.11 (1.82) | <0.0001 |
| Former | 1914 | 18.36 (0.43) | 1841 | 19.61 (0.47) | 73 | 6.87 (0.90) | |
| Current | 2765 | 27.23 (0.50) | 2359 | 25.83 (0.52) | 406 | 40.03 (1.79) | |
| Daily smoking amount (the number of cigarettes) | 3.93 ± 7.90 | 3.60 ± 7.48 | 6.94 ± 10.54 | <0.0001 | |||
| Education | |||||||
| Less than high school diploma | 1848 | 17.11 (0.44) | 1471 | 15.31 (0.43) | 377 | 33.59 (1.74) | <0.0001 |
| High school diploma | 4386 | 43.21 (0.61) | 3944 | 42.99 (0.64) | 442 | 45.21 (1.88) | |
| College diploma or higher | 4392 | 39.68 (0.63) | 4150 | 41.70 (0.66) | 242 | 21.20 (1.51) | |
| Household income | |||||||
| Quartile 1 | 2668 | 26.21 (0.59) | 2337 | 25.64 (0.60) | 331 | 31.51 (1.67) | 0.0003 |
| Quartile 2 | 2672 | 25.00 (0.53) | 2392 | 24.88 (0.55) | 280 | 26.04 (1.52) | |
| Quartile 3 | 2607 | 24.62 (0.53) | 2375 | 24.82 (0.56) | 232 | 22.86 (1.47) | |
| Quartile 4 | 2679 | 24.17 (0.60) | 2461 | 24.67 (0.63) | 218 | 19.60 (1.43) | |
| Frequency of alcohol drinks per week | |||||||
| 0 | 1994 | 18.13 (0.44) | 1725 | 17.44 (0.45) | 269 | 24.49 (1.58) | <0.0001 |
| 1 | 6094 | 57.47 (0.57) | 5619 | 58.85 (0.59) | 475 | 44.86 (1.85) | |
| 2 or 3 | 1845 | 17.57 (0.42) | 1650 | 17.53 (0.44) | 195 | 17.94 (1.46) | |
| ≥4 | 693 | 6.82 (0.30) | 571 | 6.18 (0.30) | 122 | 12.71 (1.25) | |
| LDL cholesterol (mg/dL) | 113.26 ± 31.54 | 112.99 ± 31.15 | 115.62 ± 34.89 | 0.2330 | |||
| Fasting glucose level (mg/dL) | 95.58 ± 20.58 | 95.24 ± 20.28 | 98.70 ± 22.86 | <0.0001 | |||
| Estimated glomerular filtration rate (eGFR, mL/min/1.73 m2) | 97.67 ± 17.27 | 97.91 ± 17.14 | 95.50 ± 18.20 | 0.0149 | |||
| SBP (mmHg) | 114.66 ± 15.06 | 114.06 ± 14.71 | 120.02 ± 16.98 | <0.0001 | |||
| DBP (mmHg) | 76.24 ± 10.81 | 75.91 ± 10.69 | 79.19 ± 11.48 | <0.0001 | |||
| BMI (kg/m2) | 23.63 ± 3.45 | 23.59 ± 3.46 | 23.95 ± 3.36 | 0.0028 | |||
| Obesity c | |||||||
| No | 7278 | 67.94 (0.56) | 6569 | 68.18 (0.58) | 709 | 65.81 (1.76) | 0.1887 |
| Yes | 3348 | 32.06 (0.56) | 2996 | 31.82 (0.58) | 352 | 34.19 (1.76) | |
| Regular walking d | |||||||
| No | 6271 | 58.64 (0.57) | 5607 | 58.11 (0.60) | 664 | 63.45 (1.77) | 0.0049 |
| Yes | 4355 | 41.36 (0.57) | 3958 | 41.89 (0.60) | 397 | 36.55 (1.77) | |
| Diabetes mellitus | |||||||
| No | 8151 | 76.83 (0.51) | 7435 | 77.93 (0.53) | 716 | 66.71 (1.69) | <0.0001 |
| Impaired fasting glucose | 1877 | 17.62 (0.45) | 1613 | 16.80 (0.47) | 264 | 25.17 (1.61) | |
| Yes | 598 | 5.55 (0.25) | 517 | 5.27 (0.26) | 81 | 8.12 (1.00) | |
| Stroke | |||||||
| No | 10,566 | 99.54 (0.07) | 9517 | 99.60 (0.07) | 1049 | 98.99 (0.36) | 0.0141 |
| Yes | 60 | 0.46 (0.07) | 48 | 0.40 (0.07) | 12 | 1.01 (0.36) | |
| Hypertension | |||||||
| No | 6108 | 57.30 (0.62) | 5640 | 58.72 (0.62) | 468 | 44.23 (1.84) | <0.0001 |
| Pre-hypertension | 2588 | 24.41 (0.50) | 2318 | 24.31 (0.53) | 270 | 25.31 (1.67) | |
| Yes | 1930 | 18.30 (0.46) | 1607 | 16.97 (0.46) | 323 | 30.46 (1.64) | |
| Ischemic heart disease | |||||||
| No | 10,546 | 99.25 (0.10) | 9501 | 99.31 (0.10) | 1045 | 98.73 (0.39) | 0.0766 |
| Yes | 80 | 0.75 (0.09) | 64 | 0.69 (0.10) | 16 | 1.27 (0.39) | |
| Total (n = 10,626) | Non-High BCd (n = 9565) | High BCd (n = 1061) | |
|---|---|---|---|
| Variables | Geometric mean (SE) | Geometric mean (SE) | Geometric mean (SE) |
| Total | 0.89 (0.01) | 0.80 (0.01) | 2.40 (0.02) ** |
| Age (years) | |||
| 20–29 | 0.57 (0.01) | 0.55 (0.01) | 2.34 (0.09) |
| 30–39 | 0.83 (0.01) | 0.78 (0.01) | 2.35 (0.03) |
| 40–49 | 1.06 (0.01) | 0.93 (0.01) | 2.41 (0.03) |
| 50–59 | 1.20 (0.01) | 1.04 (0.01) | 2.42 (0.03) |
| P for trend b | <0.0001 | <0.0001 | 0.7767 |
| Sex | |||
| Male | 0.82 (0.01) | 0.75 (0.01) | 2.37 (0.03) |
| Female | 0.97 (0.01) ** | 0.85 (0.01) ** | 2.42 (0.02) |
| Smoking status | |||
| Never | 0.85 (0.01) | 0.76 (0.01) | 2.43 (0.03) |
| Former | 0.75 (0.01) | 0.72 (0.01) * | 2.22 (0.04) * |
| Current | 1.09 (0.01) ** | 0.96 (0.01) ** | 2.39 (0.03) |
| Daily smoking amount (the number of cigarettes) | |||
| <10 | 0.83 (0.01) | 0.75 (0.01) | 2.41 (0.02) |
| 10–14 | 1.00 (0.02) | 0.91 (0.02) | 2.33 (0.02) |
| 15–19 | 1.10 (0.03) | 0.98 (0.02) | 2.46 (0.10) |
| 20–70 | 1.30 (0.02) | 1.11 (0.02) | 2.39 (0.04) |
| P for trend b | <0.0001 | <0.0001 | 0.2773 |
| Education | |||
| Less than high school diploma | 1.24 (0.02) | 1.06 (0.01) | 2.40 (0.04) |
| High school diploma | 0.89 (0.01) | 0.79 (0.01) | 2.43 (0.03) |
| College diploma or higher | 0.77 (0.01) | 0.72 (0.01) | 2.34 (0.03) |
| P for trend | <0.0001 | <0.0001 | 0.0694 |
| Household income | |||
| Quartile 1 | 0.95 (0.01) | 0.83 (0.01) | 2.43 (0.03) |
| Quartile 2 | 0.91 (0.01) | 0.81 (0.01) | 2.38 (0.04) |
| Quartile 3 | 0.87 (0.01) | 0.79 (0.01) | 2.39 (0.04) |
| Quartile 4 | 0.83 (0.01) | 0.76 (0.01) | 2.40 (0.04) |
| P for trend | 0.5947 | 0.7332 | 0.6763 |
| Frequency of alcohol consumption per week | |||
| 0 | 0.96 (0.02) | 0.83 (0.01) | 2.42 (0.04) |
| 1 | 0.83 (0.01) | 0.76 (0.01) | 2.37 (0.03) |
| 2 or 3 | 0.94 (0.02) | 0.85 (0.01) | 2.39 (0.04) |
| ≥4 | 1.19 (0.03) | 1.01 (0.02) | 2.48 (0.07) |
| P for trend | <0.0001 | <0.0001 | 0.4335 |
| Obesity c | |||
| No | 0.88 (0.01) | 0.79 (0.01) | 2.41 (0.02) |
| Yes | 0.92 (0.01) | 0.82 (0.01) | 2.39 (0.03) |
| Regular walking d (n, weighted %) | |||
| No | 0.93 (0.01) | 0.83 (0.01) | 2.40 (0.02) |
| Yes | 0.84 (0.01) | 0.76 (0.01) | 2.40 (0.03) |
| P for trend | 0.0003 | 0.0007 | 0.6745 |
| Diabetes mellitus | |||
| No | 0.85 (0.01) | 0.77 (0.01) | 2.40 (0.02) |
| Impaired fasting glucose | 1.02 (0.02) | 0.89 (0.01) | 2.41 (0.04) |
| Yes | 1.05 (0.03) | 0.92 (0.02) | 2.40 (0.08) |
| Stroke | |||
| No | 0.89 (0.01) | 0.80 (0.01) | 2.40 (0.02) |
| Yes | 0.94 (0.07) | 0.74 (0.04) * | 2.28 (0.04) |
| Hypertension | |||
| No | 0.83 (0.01) | 0.76 (0.01) | 2.33 (0.02) |
| Pre-hypertension | 0.90 (0.01) * | 0.80 (0.01) * | 2.46 (0.04) * |
| Yes | 1.10 (0.02) ** | 0.94 (0.01) * | 2.46 (0.04) * |
| Ischemic heart disease | |||
| No | 0.89 (0.01) | 0.80 (0.01) | 2.40 (0.02) |
| Yes | 1.10 (0.06) | 0.94 (0.04) | 2.41 (0.09) |
| Total (n = 10,626) | |||||
|---|---|---|---|---|---|
| Cases/Non-Cases | Crude OR (95% CI) | Model 1 b OR (95% CI) | Model 2 c OR (95% CI) | Model 3 d OR (95% CI) | |
| Stroke | |||||
| Non-high BCd | 48/9517 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| High BCd | 12/1049 | 2.55 (1.18, 5.51) | 2.37 (1.02, 5.49) | 2.39 (1.03, 5.56) | 2.50 (1.01, 6.18) |
| Hypertension | |||||
| Non-high BCd | 1607/7958 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| High BCd | 323/738 | 2.14 (1.83, 2.51) | 1.45 (1.20, 1.76) | 1.46 (1.20, 1.76) | 1.48 (1.22, 1.79) |
| Ischemic heart disease | |||||
| Non-high BCd | 64/9501 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| High BCd | 16/1045 | 1.84 (0.93, 3.66) | 1.11 (0.55, 2.24) | 1.12 (0.56, 2.26) | 1.08 (0.54, 2.15) |
| Systolic Blood Pressure (mmHg) | Diastolic Blood Pressure (mmHg) | ||||
|---|---|---|---|---|---|
| BCd level | n | Crude | Adjusted b | Crude | Adjusted b |
| BCd (μg/L) | 10,626 | 4.35 (3.83, 4.87) ** | 2.08 (1.50, 2.66) * | 2.67 (2.28, 3.05) ** | 1.39 (0.97, 1.81) * |
| Non-high BCd a | 9565 | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) |
| High BCd a | 1,061 | 5.85 (4.61, 7.10) | 3.00 (1.82, 4.17) | 3.33 (2.50, 4.16) | 1.92 (1.14, 2.70) |
| P for trend c | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, J.; Yun, S.-m.; Kim, M.; Koh, Y.H. Association of Blood Cadmium with Cardiovascular Disease in Korea: From the Korea National Health and Nutrition Examination Survey 2008–2013 and 2016. Int. J. Environ. Res. Public Health 2020, 17, 6288. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176288
Jeong J, Yun S-m, Kim M, Koh YH. Association of Blood Cadmium with Cardiovascular Disease in Korea: From the Korea National Health and Nutrition Examination Survey 2008–2013 and 2016. International Journal of Environmental Research and Public Health. 2020; 17(17):6288. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176288
Chicago/Turabian StyleJeong, Jihyun, Sang-moon Yun, Minkyeong Kim, and Young Ho Koh. 2020. "Association of Blood Cadmium with Cardiovascular Disease in Korea: From the Korea National Health and Nutrition Examination Survey 2008–2013 and 2016" International Journal of Environmental Research and Public Health 17, no. 17: 6288. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176288