Physical Activity, Sedentary Behaviour and Sleep, and Their Association with BMI in a Sample of Adolescent Females in New Zealand



Abstract
:1. Introduction
2. Materials and Methods
3. Results
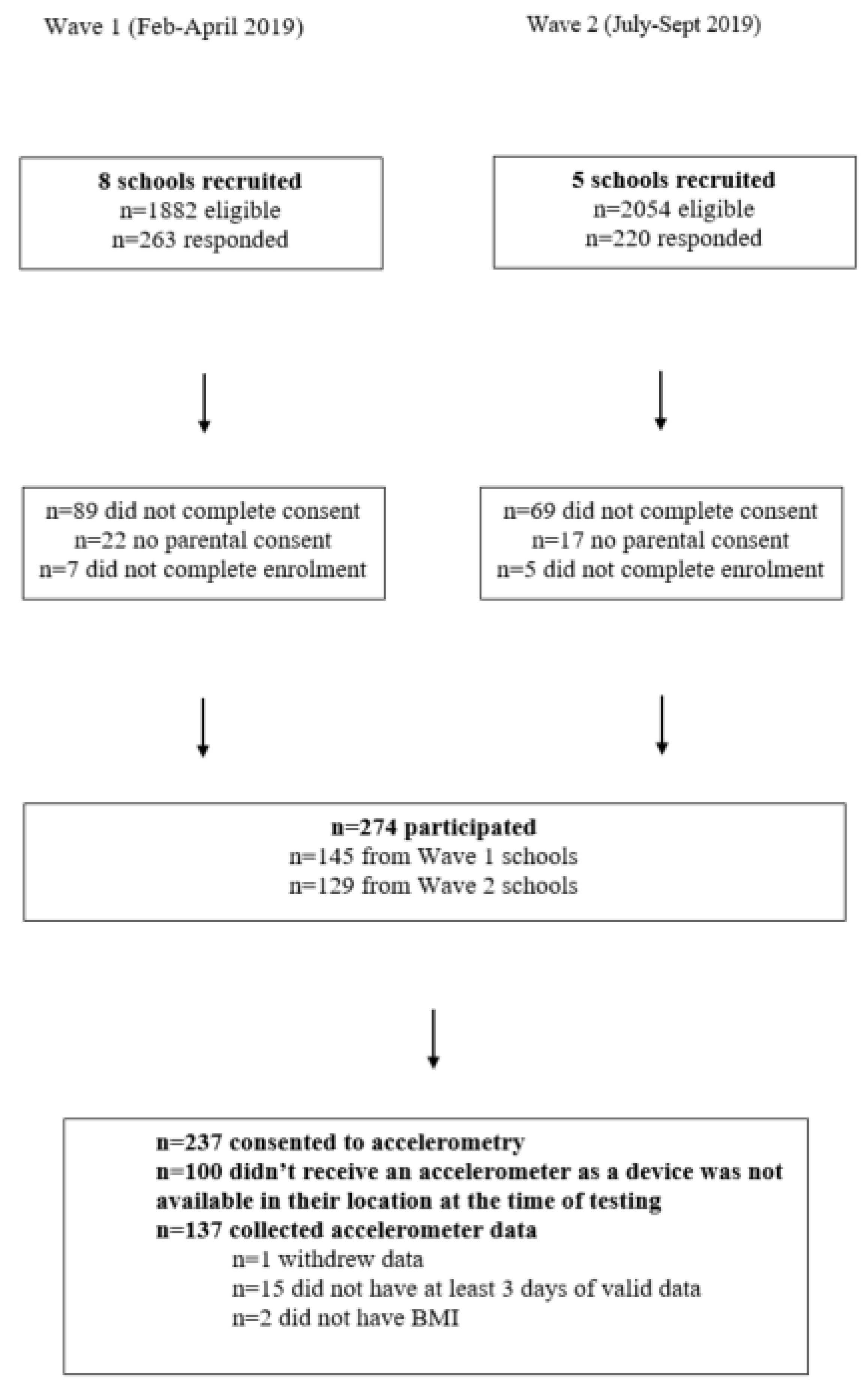
3.1. Participants
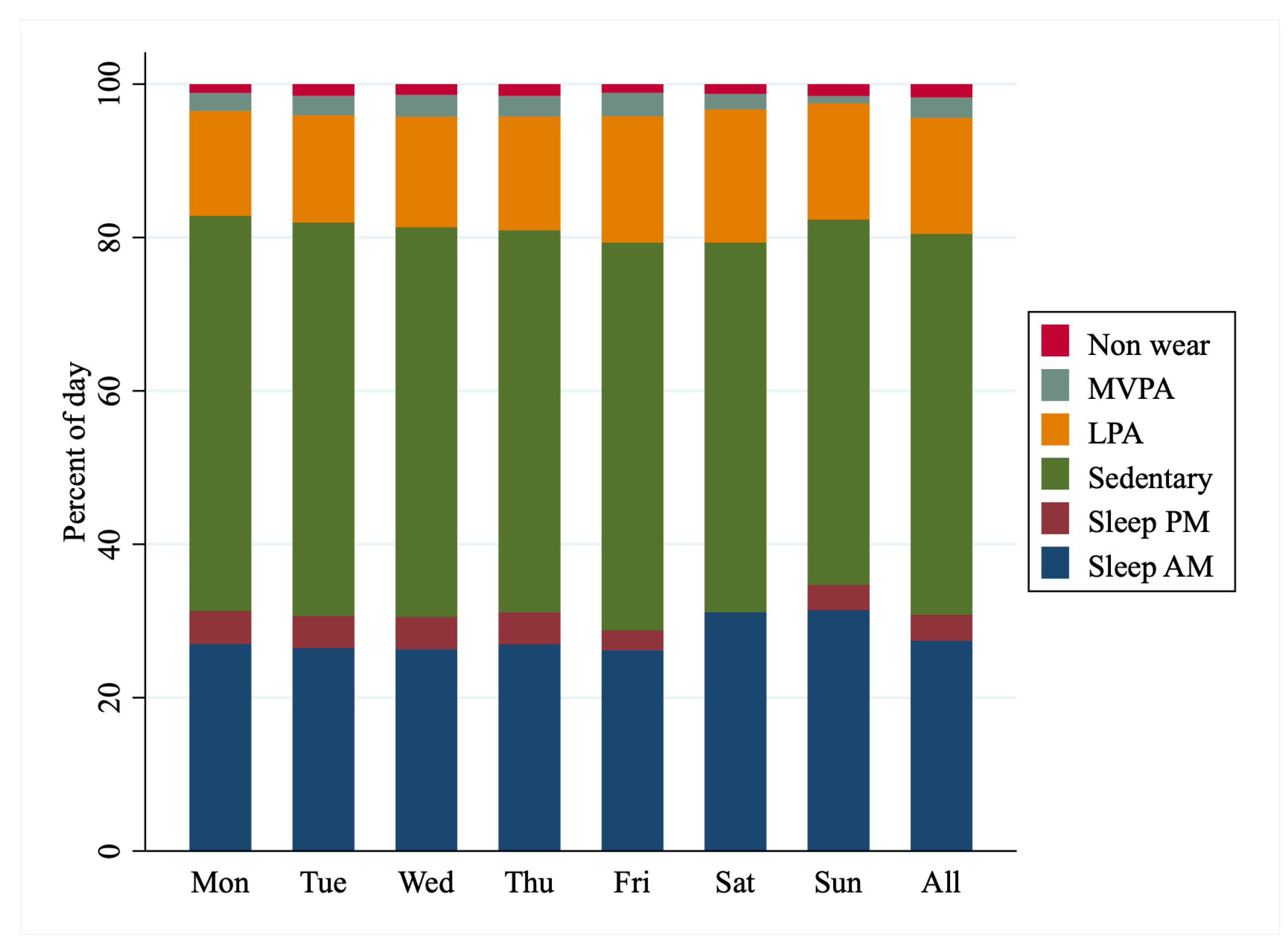
3.2. 24-h Activity Patterns
3.3. Associations Between 24-h Components and BMI
3.4. Adherance to Guidelines
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chaput, J.-P.; Carson, V.; Gray, C.; Tremblay, M. Importance of all movement behaviors in a 24 hour period for overall health. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 12575–12581. [Google Scholar] [CrossRef]
- Warburton, D.E.; Charlesworth, S.; Ivey, A.; Nettlefold, L.; Bredin, S.S.D. A systematic review of the evidence for Canada’s physical activity guidelines for adults. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 39. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, M.S.; Carson, V.; Chaput, J.-P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef]
- Ministry of Health. Children and Young People (5–17 years) ‘Sit Less, Move More, Sleep Well’. Available online: https://www.health.govt.nz/our-work/preventative-health-wellness/physical-activity#kids (accessed on 17 August 2020).
- Australian Government Department of Health. Australian Government Department of Health. Australian 24-Hour Movement Guidelines for Children and Young People (5–17 Years). In An Integration of Physical Activity, Sedentary Behaviour and Sleep; Australian Government Department of Health: Canberra, Australia, 2018. [Google Scholar]
- Ministry of Health. Annual Data Explorer 2017/18: New Zealand Health Survey. Available online: https://www.health.govt.nz/publication/annual-update-key-results-2017-18-new-zealand-health-survey (accessed on 17 August 2020).
- Australian Bureau of Statistics. Australian Health Survey 2011–2013. Available online: https://www.abs.gov.au/australianhealthsurvey (accessed on 17 August 2020).
- C.O.D.C.A. Childhood Obesity Facts. Available online: https://www.cdc.gov/obesity/data/childhood.html (accessed on 16 August 2020).
- H.O.C. Obesity Statistics. Available online: https://commonslibrary.parliament.uk/research-briefings/sn03336/ (accessed on 16 August 2020).
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.-J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Masse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef]
- Matricciani, L.; Olds, T.; Petkov, J. In search of lost sleep: Secular trends in the sleep time of school-aged children and adolescents. Sleep Med. Rev. 2012, 16, 203–211. [Google Scholar] [CrossRef]
- Haskell, W.L.; Lee, I.-M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 116, 1081. [Google Scholar] [CrossRef] [Green Version]
- Hinckson, E.A.; Duncan, S.; Oliver, M.; Mavoa, S.; Cerin, E.; Badland, H.; Stewart, T.; Ivory, V.; McPhee, J.; Schofield, G. Built environment and physical activity in New Zealand adolescents: A protocol for a cross-sectional study. BMJ Open 2014, 4. [Google Scholar] [CrossRef] [Green Version]
- Mota, J.; Santos, P.; Guerra, S.; Ribeiro, J.C.; Duarte, J.A. Patterns of daily physical activity during school days in children and adolescents. Am. J. Hum. Biol 2003, 15, 547–553. [Google Scholar] [CrossRef]
- Peddie, M.; Ranasinghe, C.; Scott, T.; Heath, A.-L.; Horwath, C.; Gibson, R.; Brown, R.; Houghton, L.; Haszard, J. Dietary Intake Nutritional Status and Lifestyle of Adolescent Vegetarian and Nonvegetarian Girls in New Zealand (The SuNDiAL Project): Protocol for a Clustered, Cross-Sectional Survey. JMIR Res. Protoc. 2020, 9, e17310. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)-a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Cain, K.L.; Sallis, J.F.; Conway, T.L.; Van Dyck, D.; Calhoon, L. Using accelerometers in youth physical activity studies: A review of methods. J. Phys. Act. Health 2013, 10, 437–450. [Google Scholar] [CrossRef]
- Kozey-Keadle, S.; Libertine, A.; Lyden, K.; Staudenmayer, J.; Freedson, P.S. Validation of wearable monitors for assessing sedentary behavior. Med. Sci. Sports Exerc. 2011, 43, 1561–1567. [Google Scholar] [CrossRef] [Green Version]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the computer science and applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Sadeh, A.; Sharkey, K.M.; Carskadon, M.A. Activity-based sleep-wake identification: An empirical test of methodological issues. Sleep Med. Rev. 1994, 17, 201–207. [Google Scholar] [CrossRef] [Green Version]
- Kinder, J.R.; Lee, K.A.; Thompson, H.; Hicks, K.; Topp, K.; Madsen, K.A. Validation of a Hip-Worn Accelerometer in Measuring Sleep Time in Children. J. Pediatric Nurs. 2012, 27, 127–133. [Google Scholar] [CrossRef] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1.6 million participants. Lancet Child. Adolesc. Health 2019. [Google Scholar] [CrossRef]
- Carson, V.; Chaput, J.-P.; Janssen, I.; Tremblay, M.S. Health associations with meeting new 24-hour movement guidelines for Canadian children and youth. Prev. Med. 2017, 95, 7–13. [Google Scholar] [CrossRef]
- Chastin, S.F.M.; Palarea-Albaladejo, J.; Dontje, M.L.; Skelton, D.A. Combined effects of time spent in physical activity, sedentary behaviors and sleep on obesity and cardio-metabolic health markers: A novel compositional data analysis approach. PLoS ONE 2015, 10, e0139984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, E.A.; Salmon, J.; McNaughton, S.A.; Orellana, L.; Wadley, G.D.; Bruce, C.; Dempsey, P.C.; Lacy, K.E.; Dunstan, D.W. Effects of breaking up sitting on adolescents’ postprandial glucose after consuming meals varying in energy: A cross-over randomised trial. J. Sci. Med. Sport 2018, 21, 280–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, R.W.; Haszard, J.J.; Meredith-Jones, K.A.; Galland, B.C.; Heath, A.M.; Lawrence, J.; Gray, A.R.; Sayers, R.; Hanna, M.; Taylor, B.J. 24-h movement behaviors from infancy to preschool: Cross-sectional and longitudinal relationships with body composition and bone health. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamer, M.; Stamatakis, E.; Steptoe, A. Effects of substituting sedentary time with physical activity on metabolic risk. Med. Sci. Sports Exerc. 2014, 46, 1946–1950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, J.A. Nonexercise activity thermogenesis (NEAT): Environment and biology. Am. J. Physiol. Endocrinol. Metab. 2004, 286, E675–E685. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Tanabe, K.; Yokoyama, N.; Zempo, H.; Kuno, S. Objectively measured light-intensity lifestyle activity and sedentary time are independently associated with metabolic syndrome: A cross-sectional study of Japanese adults. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 30. [Google Scholar] [CrossRef] [Green Version]
- Laurson, K.R.; Lee, J.A.; Gentile, D.A.; Walsh, D.A.; Eisenmann, J.C. Concurrent associations between physical activity, screen time, and sleep duration with childhood obesity. ISRN Obes. 2014, 2014. [Google Scholar] [CrossRef]
- Janssen, I.; Roberts, K.C.; Thompson, W. Adherence to the 24-hour movement guidelines among 10- to 17-year-old Canadians. Health Promot. Chronic. Dis. Prev. Can. 2017, 37, 369–375. [Google Scholar] [CrossRef]
- Ying, L.; Zhu, X.; Haegele, J.; Wen, Y. Movement in high school: Proportion of Chinese adolescents meeting 24-hour movement guidelines. Int. J. Environ. Res. Public Health 2020, 17, 2395. [Google Scholar] [CrossRef] [Green Version]
- Knell, G.; Durand, C.P.; Kohl, H.W., III; Wu, I.H.C.; Pettee Gabriel, K. Prevalence and likelihood of meeting sleep, physical activity, and screen-time guidelines among US youth. JAMA Pediatr. 2019, 173, 387–389. [Google Scholar] [CrossRef]
- Roberts, K.C.; Yao, X.; Carson, V.; Chaput, J.P.; Janssen, I.; Tremblay, M.S. Meeting the Canadian 24-Hour Movement Guidelines for Children and Youth. Health Rep. 2017, 28, 3–7. [Google Scholar] [PubMed]
- Bronikowski, M.; Bronikowska, M.; Maciaszek, J.; Glapa, A. Maybe it is not a goal that matters: A report from a physical activity intervention in youth. J. Sports Med. Phys. Fit. 2018, 58, 348–355. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; Altenburg, T.M.; et al. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Mean Difference (95% CI) for each z-Score Higher BMI | Mean Difference (95% CI) for Overweight Compared to Healthy Weight | Mean Difference (95% CI) for Obese Compared to Healthy Weight | |
|---|---|---|---|
| 24 h components | |||
| Sleep (minutes) | −11 (−23, 2) | −16 (−42, 10) | −28 (−72, 16) |
| Sedentary time (minutes) | −3 (−22, 16) | −7 (−47, 34) | 4 (−64, 71) |
| LPA (minutes) | −16 (3, 29) | 24 (−4, 52) | 34 (−13, 81) |
| MVPA (minutes) | −4 (−8, 1) | −7 (−16, 2) | −11 (−27, 4) |
| Breaks in sedentary time | |||
| Number of breaks | 2 (−3, 6) | 5 (−4, 13) | −2 (−16, 12) |
| Mean duration of breaks (minutes) | −0.3 (−1.0, 0.4) a | −0.6 (−2.0, 0.9) a | 0.1 (−2.3, 2.6) a |
| Mean intensity of breaks (counts per min) | 5 (−29, 40) | −48 (−121, 26) | −2 (−124, 120) |
| Mean duration of uninterrupted sedentary time (minutes) | −6 (−23, 11) | −14 (−51, 23) | 8 (−53, 70) |
| Bouts of MVPA | |||
| Number of bouts | 0 (−1, 1) | −1 (−4, 2) | −1 (−5, 4) |
| Mean duration of bouts (minutes) | −0.1 (−0.3, 0.05) | −0.2 (−0.6, 0.2) | −0.5 (−1.1, 0.2) |
| Mean intensity of bouts (counts per min) | −156 (−301, −10) | −188 (−494, 118) | −517 (−1027, −6) |
| N (%) Meeting Sleep Recommendation (8–10 h a Night) | N (%) Meeting Physical Activity Recommendation (60+ min of MVPA a Day) | N (%) Meeting Both Sleep and Physical Activity Recommendations | |
|---|---|---|---|
| Whole sample | 23 (19.3) | 27 (22.7) | 8 (6.7) |
| Healthy weight (n = 78) | 18 (23.1) | 21 (26.9) | 6 (7.7) |
| Overweight (n = 32) | 5 (15.6) | 5 (15.6) | 2 (6.3) |
| Obese (n = 9) | 0 | 1 (11.1) | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tye, L.S.; Scott, T.; Haszard, J.J.; Peddie, M.C. Physical Activity, Sedentary Behaviour and Sleep, and Their Association with BMI in a Sample of Adolescent Females in New Zealand. Int. J. Environ. Res. Public Health 2020, 17, 6346. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176346
Tye LS, Scott T, Haszard JJ, Peddie MC. Physical Activity, Sedentary Behaviour and Sleep, and Their Association with BMI in a Sample of Adolescent Females in New Zealand. International Journal of Environmental Research and Public Health. 2020; 17(17):6346. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176346
Chicago/Turabian StyleTye, Lauren S., Tessa Scott, Jillian J. Haszard, and Meredith C. Peddie. 2020. "Physical Activity, Sedentary Behaviour and Sleep, and Their Association with BMI in a Sample of Adolescent Females in New Zealand" International Journal of Environmental Research and Public Health 17, no. 17: 6346. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176346