Impacts of Thresholds of Gray Value for Cone-Beam Computed Tomography 3D Reconstruction on the Accuracy of Image Matching with Optical Scan

 , ,
, ,
Abstract
:1. Introduction
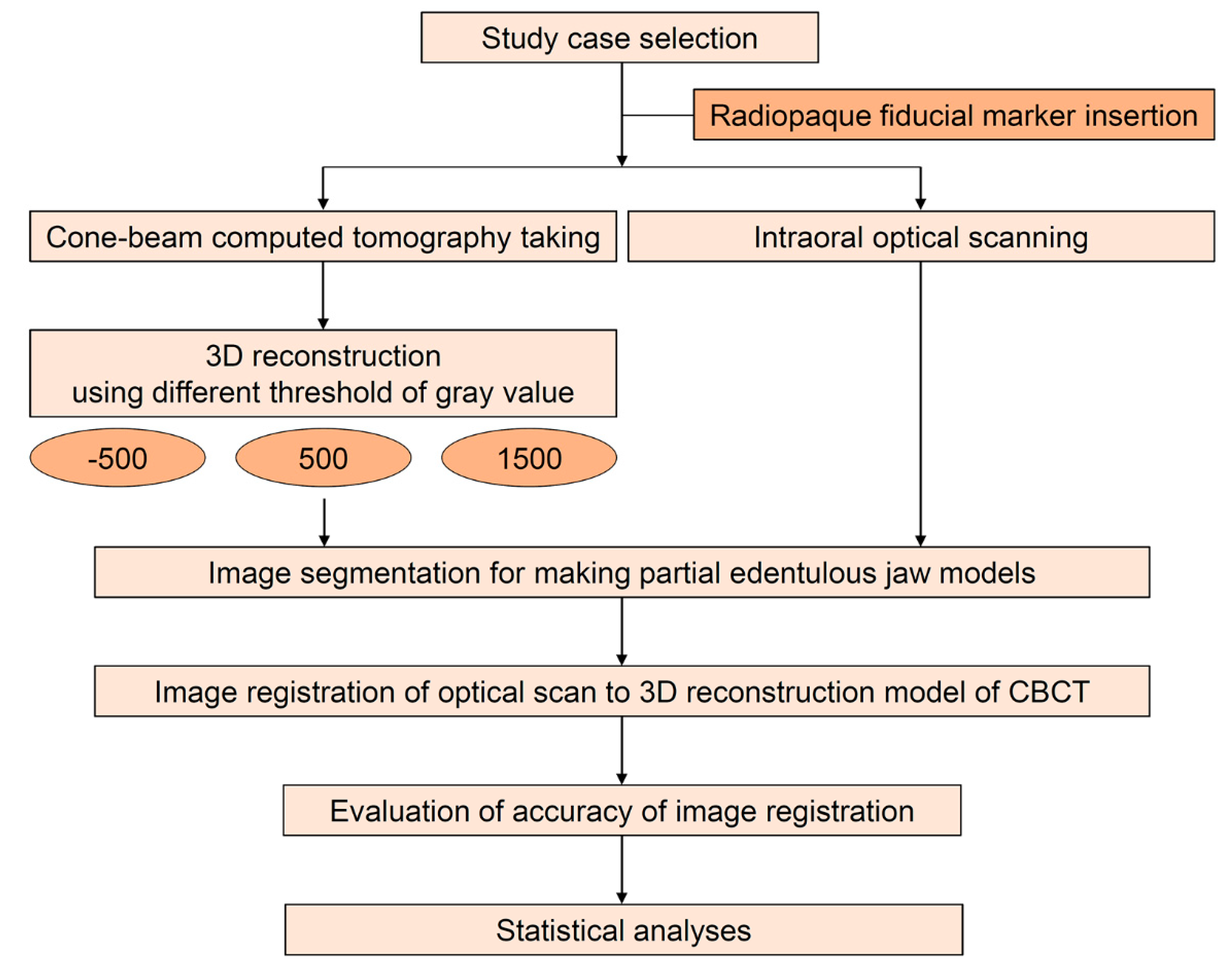
2. Materials and Methods
2.1. Image Acquisition via Cone-Beam Computed Tomography and Optical Scan
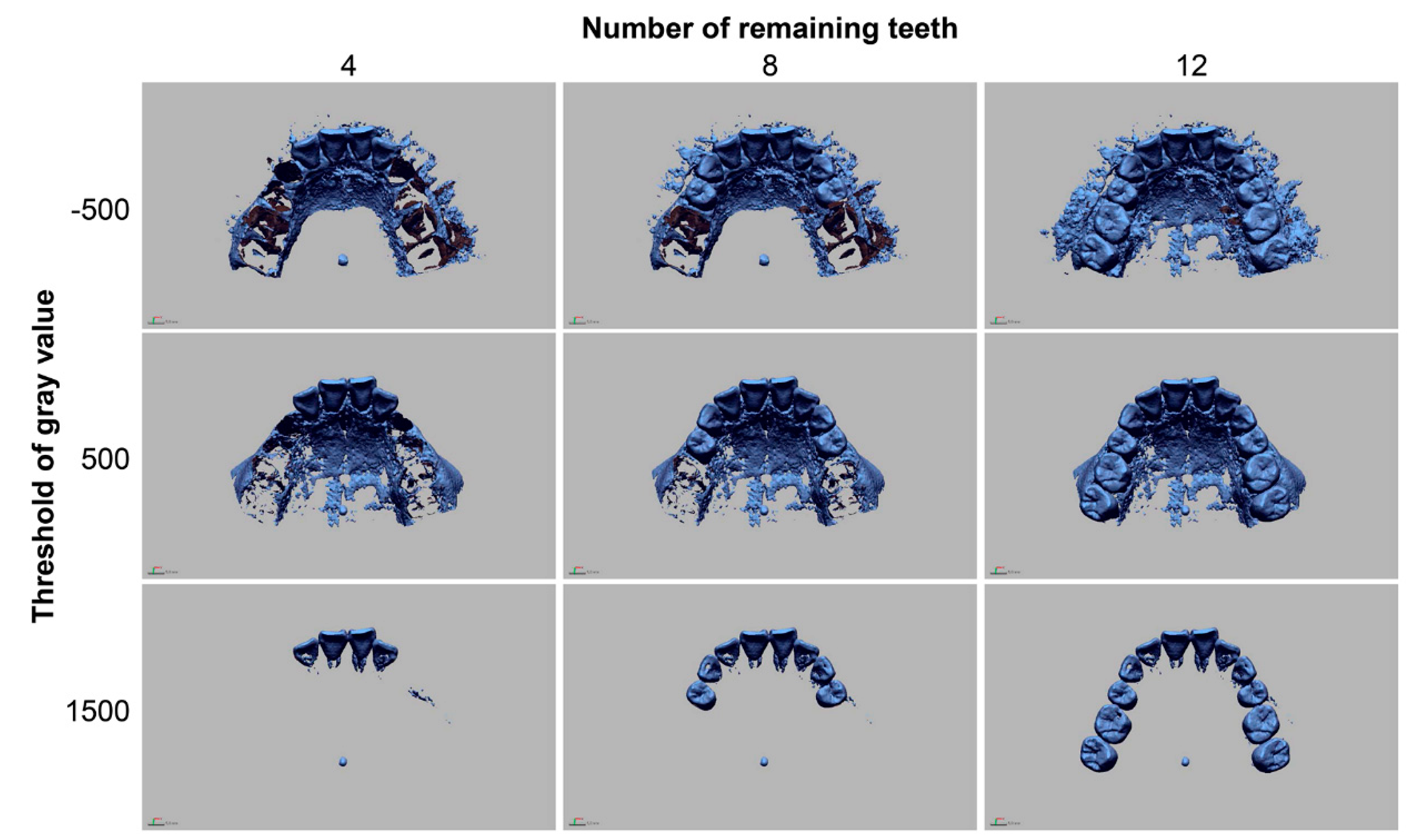
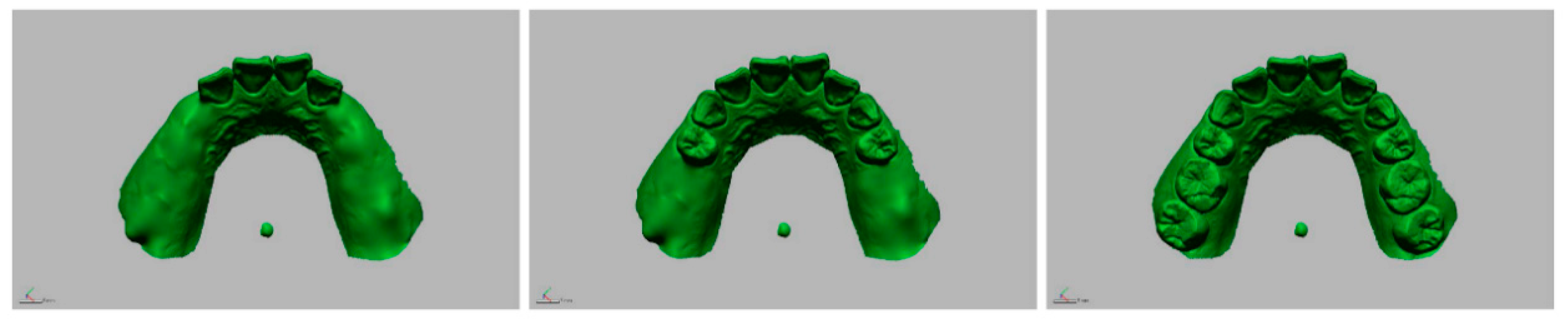
2.2. Image Conversion and Segmentation
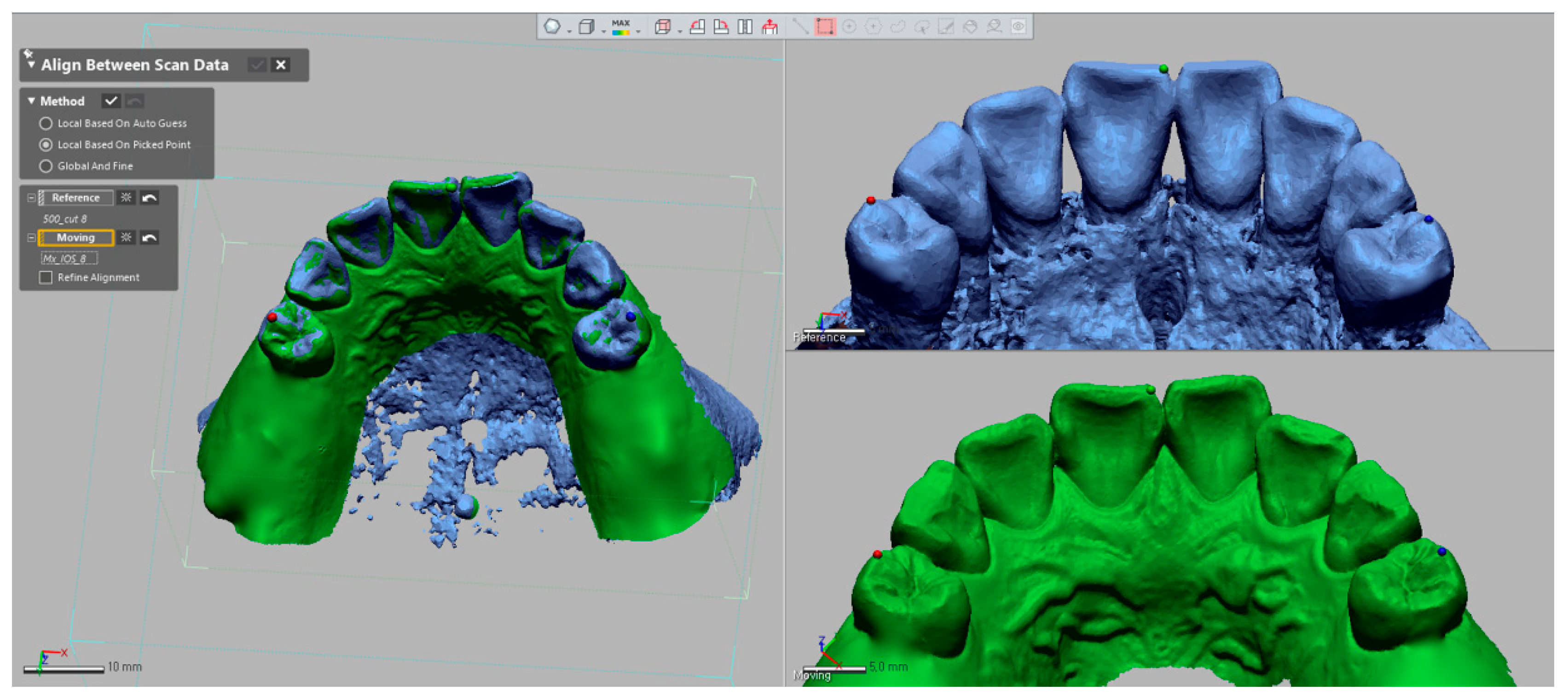
2.3. Image Registration of Optical Scan to 3D Reconstruction Model of CBCT
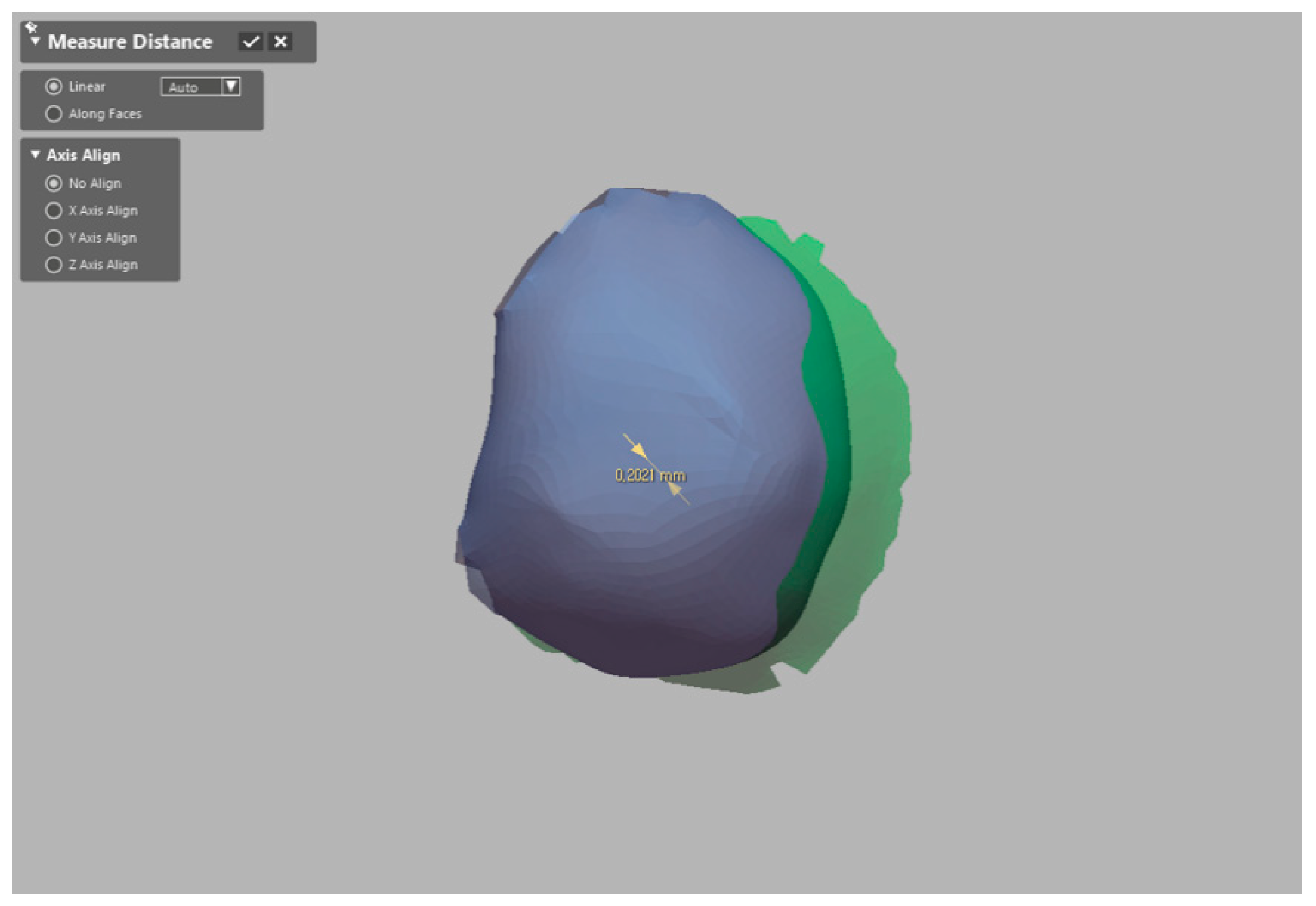
2.4. Evaluation of Accuracy of Image Registration
2.5. Statistical Analysis
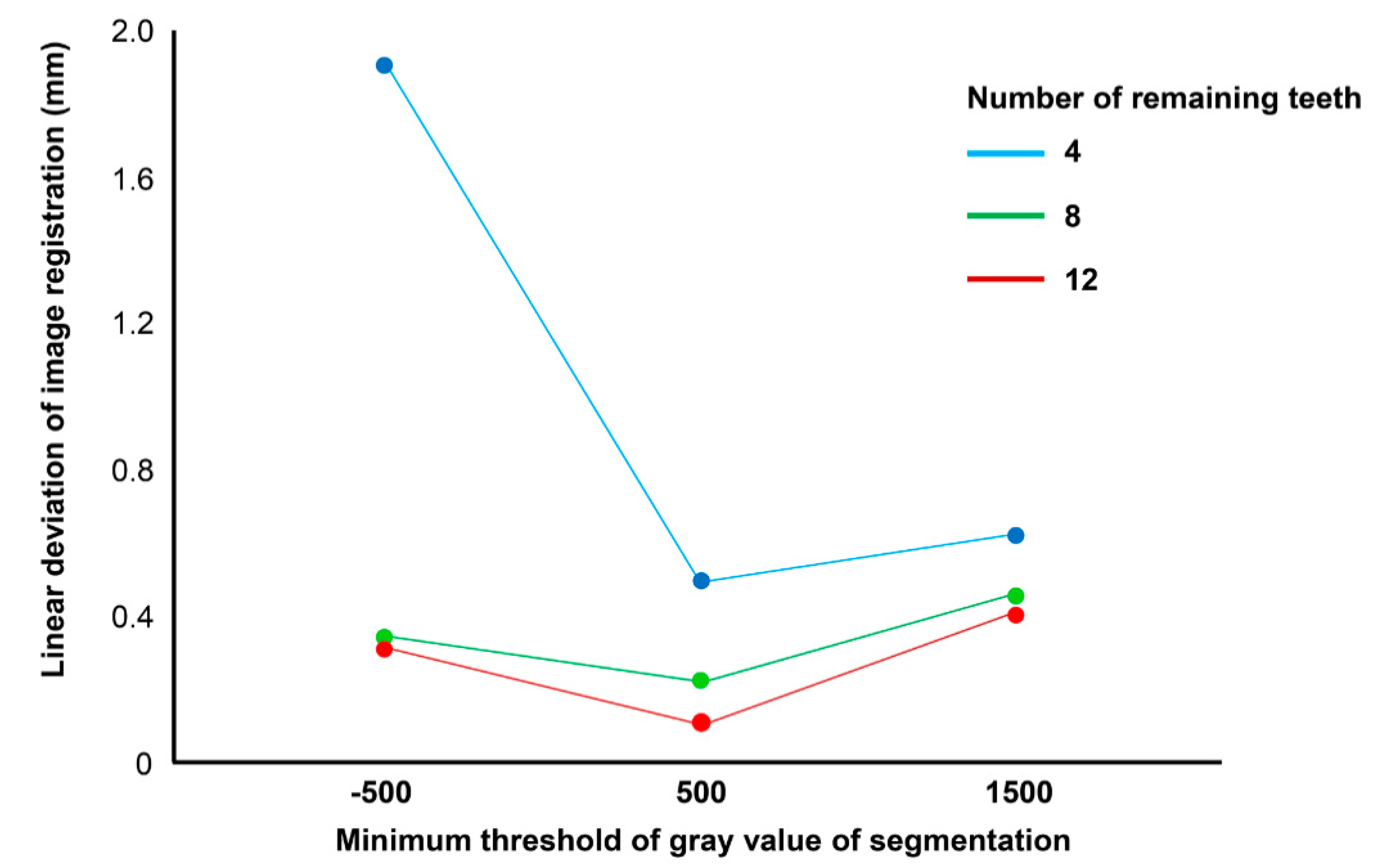
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Maspero, C.; Farronato, M.; Bellincioni, F.; Cavagnetto, D.; Abate, A. Assessing mandibular body changes in growing subjects: A comparison of CBCT and reconstructed lateral cephalogram measurements. Sci. Rep. 2020, 10, 11722. [Google Scholar] [CrossRef] [PubMed]
- Maspero, C.; Abate, A.; Cavagnetto, D.; El Morsi, M.; Fama, A.; Farronato, M. Available technologies, applications and benefits of teleorthodontics. A literature review and possible applications during the COVID-19 Pandemic. J. Clin. Med. 2020, 9, 1891. [Google Scholar] [CrossRef] [PubMed]
- Almaqrami, B.S.; Alhammadi, M.S.; Cao, B. Three dimensional reliability analyses of currently used methods for assessment of sagittal jaw discrepancy. J. Clin. Exp. Dent. 2018, 10, e352–e360. [Google Scholar] [CrossRef] [PubMed]
- Marchack, C.B. CAD/CAM-guided implant surgery and fabrication of an immediately loaded prosthesis for a partially edentulous patient. J. Prosthet. Dent. 2007, 97, 389–394. [Google Scholar] [CrossRef]
- Scarfe, W.C.; Farman, A.G. What is Cone-Beam CT and how does it work? Dent. Clin. N. Am. 2008, 52, 707–730. [Google Scholar] [CrossRef]
- Bryant, J.; Drage, N.A.; Richmond, S. Study of the scan uniformity from an i-CAT cone beam computed tomography dental imaging system. Dentomaxillofac. Radiol. 2008, 37, 365–374. [Google Scholar] [CrossRef]
- Pellegrino, G.; Bellini, P.; Cavallini, P.F.; Ferri, A.; Zacchino, A.; Taraschi, V.; Marchetti, C.; Consolo, U. Dynamic navigation in dental implantology: The influence of surgical experience on implant placement accuracy and operating time. an in vitro study. Int. J. Environ. Res. Public Health 2020, 17, 2153. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.W.; Yang, B.-E.; Cheon, K.J.; Jang, W.S.; Kim, J.W.; Byun, S.H. A simple and safe approach for maxillary sinus augmentation with the advanced surgical guide. Int. J. Environ. Res. Public Health 2020, 17, 3785. [Google Scholar] [CrossRef]
- Ferrini, F.; Sannino, G.; Chiola, C.; Capparé, P.; Gastaldi, G.; Gherlone, E.F. Influence of intra-oral scanner (I.O.S.) on the marginal accuracy of CAD/CAM single crowns. Int. J. Environ. Res. Public Health 2019, 16, 544. [Google Scholar] [CrossRef] [Green Version]
- Cattoni, F.; Teté, G.; Calloni, A.M.; Manazza, F.; Gastaldi, G.; Capparé, P. Milled versus moulded mock-ups based on the superimposition of 3D meshes from digital oral impressions: A comparative in vitro study in the aesthetic area. BMC Oral Health 2019, 19, 230. [Google Scholar] [CrossRef]
- Capparé, P.; Sannino, G.; Minoli, M.; Montemezzi, P.; Ferrini, F. Conventional versus digital impressions for full arch screw-retained maxillary rehabilitations: A randomized clinical trial. Int. J. Environ. Res. Public Health 2019, 16, 829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gherlone, E.; Ferrini, F.; Crespi, R.; Gastaldi, G.; Capparé, P. Digital impressions for fabrication of definitive “all-on-four” restorations. Implant. Dent. 2015, 24, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Gherlone, E.; Mandelli, F.; Capparé, P.; Pantaleo, G.; Traini, T.; Ferrini, F. A 3 years retrospective study of survival for zirconia-based single crowns fabricated from intraoral digital impressions. J. Dent. 2014, 42, 1151–1155. [Google Scholar] [CrossRef] [PubMed]
- Holst, S.; Blatz, M.B.; Eitner, S. Precision for computer-guided implant placement: Using 3D planning software and fixed intraoral reference points. J. Oral Maxillofac. Surg. 2007, 65, 393–399. [Google Scholar] [CrossRef]
- Flügge, T.V.; Derksen, W.; Poel, J.T.; Hassan, B.; Nelson, K.; Wismeijer, D. Registration of cone beam computed tomography data and intraoral surface scans—A prerequisite for guided implant surgery with CAD/CAM drilling guides. Clin. Oral Implant. Res. 2016, 28, 1113–1118. [Google Scholar] [CrossRef]
- Jamjoom, F.; Kim, D.G.; Lee, D.J.; McGlumphy, E.; Yilmaz, B. Effect of length and location of edentulous area on the accuracy of prosthetic treatment plan incorporation into cone-beam computed tomography scans. Clin. Implant. Dent. Relat. Res. 2018, 20, 300–307. [Google Scholar] [CrossRef]
- Almukhtar, A.; Ju, X.; Khambay, B.S.; McDonald, J.; Ayoub, A. Comparison of the accuracy of voxel based registration and surface based registration for 3D assessment of surgical change following orthognathic surgery. PLoS ONE 2014, 9, e93402. [Google Scholar] [CrossRef] [Green Version]
- Shokri, A.; Ramezani, L.; Bidgoli, M.; Akbarzadeh, M.; Ghazikhanlu-Sani, K.; Fallahi-Sichani, H. Effect of field-of-view size on gray values derived from cone-beam computed tomography compared with the Hounsfield unit values from multidetector computed tomography scans. Imaging Sci. Dent. 2018, 48, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Norton, M.R.; Gamble, C. Bone classification: An objective scale of bone density using the computerized tomography scan. Clin. Oral Implant. Res. 2001, 12, 79–84. [Google Scholar] [CrossRef]
- Nkenke, E.; Zachow, S.; Benz, M.; Maier, T.; Veit, K.; Kramer, M.; Benz, S.; Häusler, G.; Neukam, F.W.; Lell, M. Fusion of computed tomography data and optical 3D images of the dentition for streak artefact correction in the simulation of orthognathic surgery. Dentomaxillofac. Radiol. 2004, 33, 226–232. [Google Scholar] [CrossRef]
- Di Giacomo, G.; Cury, P.R.; De Araújo, N.S.; Sendyk, W.R.; Sendyk, C.L. Clinical application of stereolithographic surgical guides for implant placement: Preliminary results. J. Periodontol. 2005, 76, 503–507. [Google Scholar] [CrossRef]
- Mai, H.Y.; Lee, D.H. Impact of matching point selections on image registration accuracy between optical scan and computed tomography. BioMed Res. Int. 2020, 2020, 3285431. [Google Scholar] [CrossRef] [PubMed]
- Ye, N.; Jian, F.; Xue, J.; Wang, S.; Liao, L.; Huang, W.; Yang, X.; Zhou, Y.; Lai, W.; Li, J.; et al. Accuracy of in-vitro tooth volumetric measurements from cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 879–887. [Google Scholar] [CrossRef] [PubMed]
- Baumgaertel, S.; Palomo, J.M.; Palomo, L.; Hans, M.G. Reliability and accuracy of cone-beam computed tomography dental measurements. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 19–25, discussion 25–18. [Google Scholar] [CrossRef] [PubMed]
- Schulze, R.; Heil, U.; Gross, D.; Bruellmann, D.; Dranischnikow, E.; Schwanecke, U.; Schoemer, E. Artefacts in CBCT: A review. Dentomaxillofac. Radiol. 2011, 40, 265–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schafer, S.; Stayman, J.W.; Zbijewski, W.; Schmidgunst, C.; Kleinszig, G.; Siewerdsen, J.H. Antiscatter grids in mobile C-arm cone-beam CT: Effect on image quality and dose. Med. Phys. 2012, 39, 153–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.; Bai, T.; Yan, H.; Ouyang, L.; Pompos, A.; Wang, J.; Zhou, L.; Jiang, S.; Jia, X. A practical cone-beam CT scatter correction method with optimized Monte Carlo simulations for image-guided radiation therapy. Phys. Med. Biol. 2015, 60, 3567–3587. [Google Scholar] [CrossRef] [Green Version]
- Giacometti, V.; King, R.B.; Agnew, C.E.; Irvine, D.M.; Jain, S.; Hounsell, A.R.; McGarry, C.K. An evaluation of techniques for dose calculation on cone beam computed tomography. Br. J. Radiol. 2019, 92, 20180383. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, O.; Boldt, S.; Nadaes, M.; DeVito, K.L. Evaluating the scattered radiation intensity in CBCT. Radiat. Phys. Chem. 2018, 144, 159–164. [Google Scholar] [CrossRef]
- Dong, T.; Yuan, L.; Liu, L.; Qian, Y.; Xia, L.; Ye, N.; Fang, B. Detection of alveolar bone defects with three different voxel sizes of cone-beam computed tomography: An in vitro study. Sci. Rep. 2019, 9, 8146. [Google Scholar] [CrossRef]
- Dwivedi, N.; Nagarajappa, A.K.; Tiwari, R. Artifacts: The downturn of CBCT image. J. Int. Soc. Prev. Community Dent. 2015, 5, 440–445. [Google Scholar] [CrossRef] [Green Version]
- Rangel, F.A.; Maal, T.J.J.; De Koning, M.J.J.; Bronkhorst, E.M.; Bergé, S.J.; Kuijpers-Jagtman, A.M. Integration of digital dental casts in cone beam computed tomography scans-a clinical validation study. Clin. Oral Investig. 2018, 22, 1215–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, Y.D.; Mai, H.N.; Mai, H.Y.; Ha, J.H.; Li, L.J.; Lee, D.H. The effects of distribution of image matched fiducial markers on accuracy of computer-guided implant surgery. J. Prosthodont. 2020, 29, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Maspero, C.; Farronato, M.; Bellincioni, F.; Annibale, A.; Machetti, J.; Abate, A.; Cavagnetto, D.; Maspero, C. Three-dimensional evaluation of maxillary sinus changes in growing subjects: A retrospective cross-sectional study. Materials 2020, 13, 1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farronato, M.; Cavagnetto, D.; Abate, A.; Cressoni, P.; Fama, A.; Maspero, C. Assessment of condylar volume and ramus height in JIA patients with unilateral and bilateral TMJ involvement: Retrospective case-control study. Clin. Oral Investig. 2020, 24, 2635–2643. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N of Teeth | Minimum Threshold of Gray Value of Segmentation | p | ||
|---|---|---|---|---|
| −500 | 500 | 1500 | ||
| 4 | 1.89 ± 0.32 | 0.52 ± 0.17 | 0.65 ± 0.10 | 0.005 |
| 8 | 0.36 ± 0.07 | 0.21 ± 0.07 | 0.49 ± 0.05 | 0.002 |
| 12 | 0.30 ± 0.05 | 0.13 ± 0.02 | 0.42 ± 0.03 | 0.002 |
| P | 0.006 | 0.002 | 0.003 | |
| N of Teeth | Threshold | Mean Difference | p |
|---|---|---|---|
| 4 | −500 versus 500 | 1.37 | 0.008 * |
| 500 versus 1500 | 0.12 | 0.151 | |
| −500 versus 1500 | 1.24 | 0.008 * | |
| 8 | −500 versus 500 | 0.15 | 0.016 * |
| 500 versus 1500 | 0.28 | 0.008 * | |
| −500 versus 1500 | 0.13 | 0.008 * | |
| 12 | −500 versus 500 | 0.27 | 0.008 * |
| 500 versus 1500 | 0.29 | 0.008 * | |
| −500 versus 1500 | 0.12 | 0.008 * |
| Threshold | N of Teeth | Mean Difference | p |
|---|---|---|---|
| −500 | 4 versus 8 | 1.53 | 0.008 * |
| 8 versus 12 | 0.06 | 0.222 | |
| 4 versus 12 | 1.59 | 0.008 * | |
| 500 | 4 versus 8 | 0.31 | 0.008 * |
| 8 versus 12 | 0.08 | 0.008 * | |
| 4 versus 12 | 0.39 | 0.008 * | |
| 1500 | 4 versus 8 | 0.16 | 0.008 * |
| 8 versus 12 | 0.07 | 0.032 | |
| 4 versus 12 | 0.23 | 0.008 * |
| Source | Sum of Squares | D.F. | Mean Square | F | p |
|---|---|---|---|---|---|
| Threshold | 2,395,357.7 | 2 | 1,197,678.9 | 68.6 | <0.001 |
| Remaining teeth | 4,935,876.4 | 2 | 2,467,938.2 | 141.4 | <0.001 |
| Threshold × Remaining teeth | 3,740,647.5 | 4 | 935,161.9 | 53.6 | <0.001 |
| Error | 628,135.2 | 36 | 17,448.2 | ||
| Total | 25,448,153.0 | 45 | |||
| Corrected total | 11,700,016.8 | 44 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.-W.; Yoon, R.G.; Lee, H.; Lee, H.-J.; Choi, Y.-D.; Lee, D.-H. Impacts of Thresholds of Gray Value for Cone-Beam Computed Tomography 3D Reconstruction on the Accuracy of Image Matching with Optical Scan. Int. J. Environ. Res. Public Health 2020, 17, 6375. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176375
Park S-W, Yoon RG, Lee H, Lee H-J, Choi Y-D, Lee D-H. Impacts of Thresholds of Gray Value for Cone-Beam Computed Tomography 3D Reconstruction on the Accuracy of Image Matching with Optical Scan. International Journal of Environmental Research and Public Health. 2020; 17(17):6375. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176375
Chicago/Turabian StylePark, Se-Won, Ra Gyoung Yoon, Hyunwoo Lee, Heon-Jin Lee, Yong-Do Choi, and Du-Hyeong Lee. 2020. "Impacts of Thresholds of Gray Value for Cone-Beam Computed Tomography 3D Reconstruction on the Accuracy of Image Matching with Optical Scan" International Journal of Environmental Research and Public Health 17, no. 17: 6375. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176375