Knowledge, Attitude, and Practices of Healthcare Professionals on COVID-19 and Risk Assessment to Prevent the Epidemic Spread: A Multicenter Cross-Sectional Study from Punjab, Pakistan

 ,
,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Methodology
2.1. Study Design
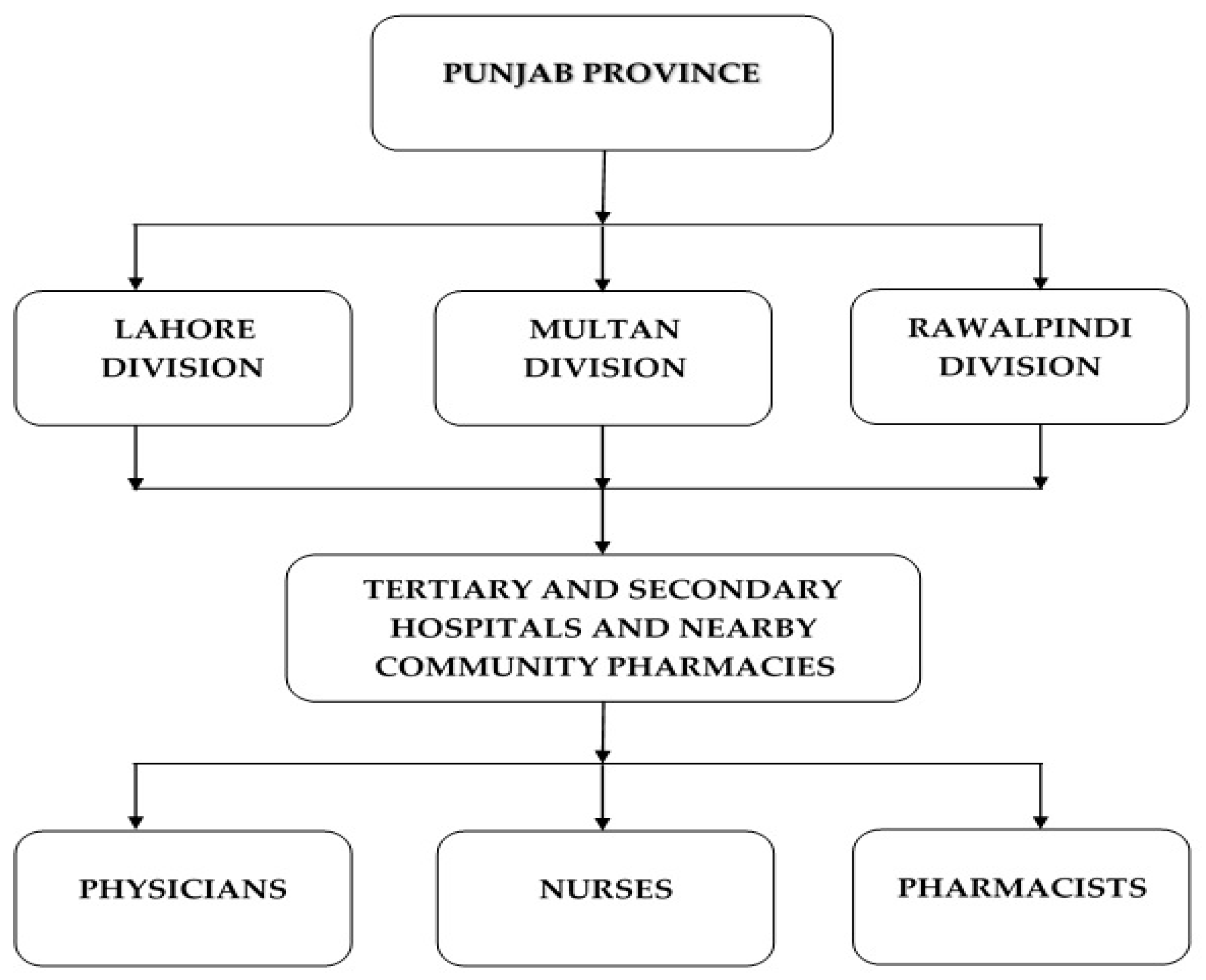
2.2. Study Setting
2.3. Study Participants
2.4. Sampling Strategy
2.5. Study Instrument
2.6. Data Collection
2.7. Ethical Approval
2.8. Statistical Analysis
3. Results
3.1. Demographics of Participants
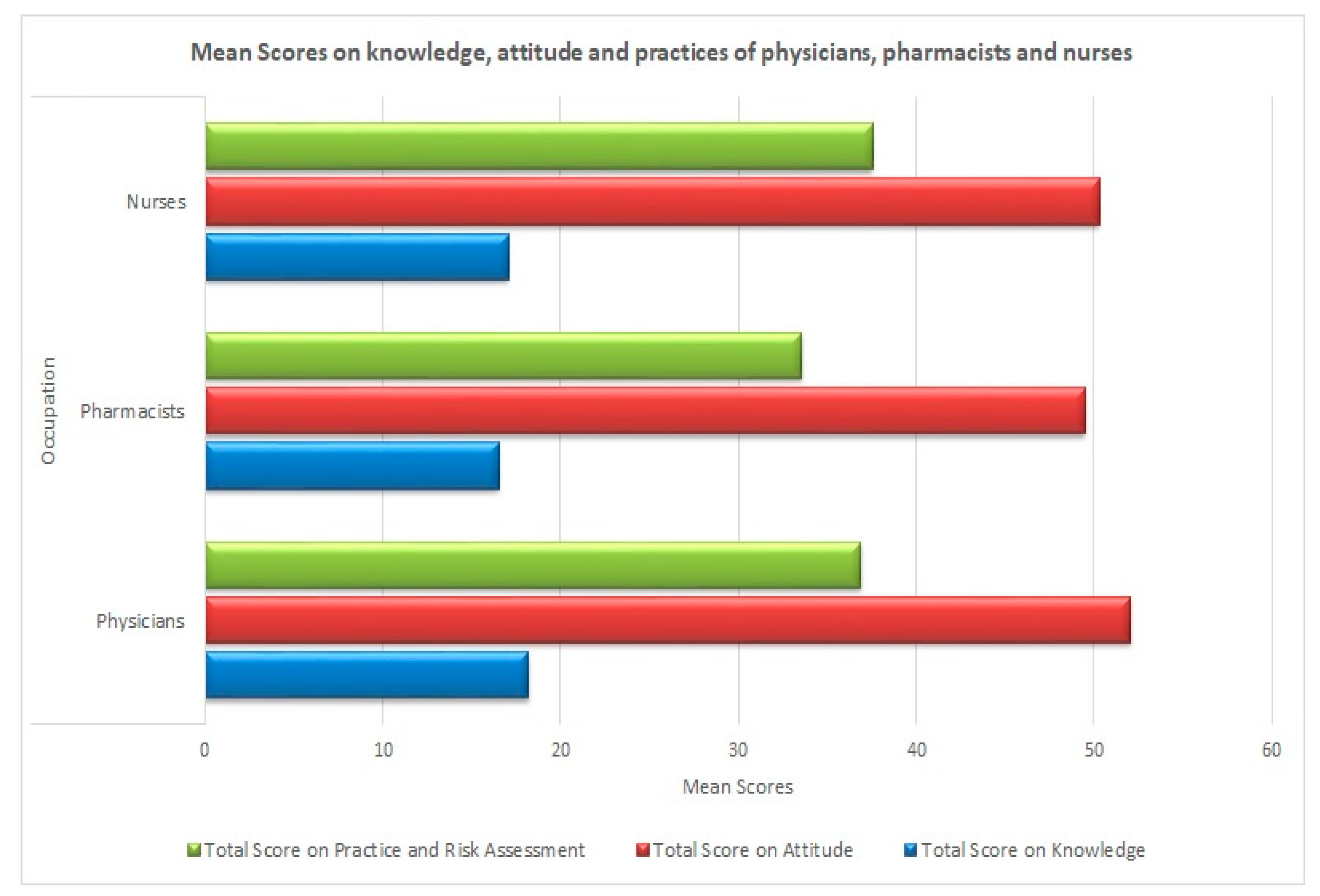
3.2. Knowledge of Healthcare Professionals
3.3. Attitude of Healthcare Professionals
3.4. Practices and Risk Assessment of Healthcare Professionals
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Paules, C.I.; Marston, H.D.; Fauci, A.S. Coronavirus Infections—More Than Just the Common Cold. JAMA 2020, 323, 707–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Naming the Coronavirus Disease. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 15 August 2020).
- World Health Organization (WHO). Novel Coronavirus Situation Report-1. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 15 August 2020).
- WHO Director General. Media Briefing 11 March 2020 Covid-19 a Pandemic. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020 (accessed on 22 March 2020).
- World Health Organization (WHO). Novel Coronavirus Situation Report-181. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 19 July 2020).
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus—Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available online: https://www.who.int/publications-detail/report-of-the-who-china-joint-mission-on-coronavirus-disease-2019-(covid-19) (accessed on 15 August 2020).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China. Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Cases in Pakistan. Available online: https://www.pakistantoday.com.pk/2020/02/26/sindh-health-two-coronavirus-cases-confirmed-in-pakistan-confirms-first-coronavirus-case-in-karachi/ (accessed on 23 March 2020).
- Ministry of National Health Services Regulation and Coordination, G.O.P. COVID-19 Pakistan. Available online: http://covid.gov.pk (accessed on 28 April 2020).
- Zhan, M.; Qin, Y.; Xue, X.; Zhu, S. Death from Covid-19 of 23 Health Care Workers in China. N. Engl. J. Med. 2020, 382, 2267–2268. [Google Scholar] [CrossRef]
- Anelli, F.; Leoni, G.; Monaco, R.; Nume, C.; Rossi, R.C.; Marinoni, G.; Spata, G.; De Giorgi, D.; Peccarisi, L.; Miani, A.; et al. Italian doctors call for protecting healthcare workers and boosting community surveillance during covid-19 outbreak. BMJ 2020, 368, m1254. [Google Scholar] [CrossRef]
- Khan, S.; Khan, M.; Maqsood, K.; Hussain, T.; Huda, N.-U.; Zeeshan, M. Is Pakistan prepared for the COVID-19 epidemic? A questionnaire-based survey. J. Med. Virol. 2020, 92, 824–832. [Google Scholar] [CrossRef] [Green Version]
- Bureau of Statistics, Government of Pakistan Census 2017. Available online: http://www.pbs.gov.pk/content/provisional-summary-results-6th-population-and-housing-census-2017-0 (accessed on 19 March 2020).
- Pakistan Medical and Dental Council. Registered Physicians in Punjab, Pakistan. Available online: http://www.pmdc.org.pk/Statistics/tabid/103/Default.aspx (accessed on 18 April 2020).
- Punjab Public Health Agency. Nurses and Midwifery in Punjab, Pakistan. Available online: http://www.ppha.punjab.gov.pk/news-and-highlights/nursing-and-midwifery.html (accessed on 18 April 2020).
- Punjab Pharmacy Council. Registered Pharmacists in Punjab, Pakistan. Available online: https://punjabpharmacycouncil.com/index_files/Page528.htm (accessed on 18 April 2020).
- World Health Organization (WHO). Risk Assessment and Management of Exposure of Health Care Workers in the Context of COVID-19. 2020. Available online: https://www.who.int/publications/m/item/risk-assessment-and-management-of-exposure-of-health-care-workers-in-the-context-of-covid-19-data-template (accessed on 15 August 2020).
- Asaad, A.M.; El-Sokkary, R.H.; Alzamanan, M.A.; El-Shafei, M. Knowledge and attitudes towards Middle East respiratory syndrome-coronavirus (MERS-CoV) among health care workers in south-western Saudi Arabia. East. Mediterr. Health J. 2019, 25. [Google Scholar] [CrossRef]
- Al-Hazmi, A.; Gosadi, I.; Somily, A.; Alsubaie, S.; Bin Saeed, A. Knowledge, attitude and practice of secondary schools and university students toward Middle East Respiratory Syndrome epidemic in Saudi Arabia: A cross-sectional study. Saudi J. Boil. Sci. 2016, 25, 572–577. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Wahed, W.Y.; Hefzy, E.M.; Ahmed, M.I.; Hamed, N.S. Assessment of Knowledge, Attitudes, and Perception of Health Care Workers Regarding COVID-19, A Cross-Sectional Study from Egypt. J. Commun. Health 2020, 1–10. [Google Scholar] [CrossRef]
- Papagiannis, D.; Malli, F.; Raptis, D.G.; Papathanasiou, I.V.; Fradelos, E.C.; Daniil, Z.; Rachiotis, G.; Gourgoulianis, K. Assessment of Knowledge, Attitudes, and Practices towards New Coronavirus (SARS-CoV-2) of Health Care Professionals in Greece before the Outbreak Period. Int. J. Environ. Res. Public Health 2020, 17, 4925. [Google Scholar] [CrossRef] [PubMed]
- Taghrir, M.H.; Borazjani, R.; Shiraly, R. COVID-19 and Iranian Medical Students; A Survey on Their Related-Knowledge, Preventive Behaviors and Risk Perception. Arch. Iran. Med. 2020, 23, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Rio, C.; Malani, P.N. COVID-19—New Insights on a Rapidly Changing Epidemic. JAMA 2020, 323, 1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Del Rio, C.; Malani, P.N. 2019 Novel Coronavirus—Important Information for Clinicians. JAMA 2020, 323, 1039. [Google Scholar] [CrossRef] [PubMed]
- Mitjà, O.; Clotet, B. Use of antiviral drugs to reduce COVID-19 transmission. Lancet Glob. Health 2020, 8, e639–e640. [Google Scholar] [CrossRef] [Green Version]
- Saqlain, M.; Munir, M.M.; Rehman, S.U.; Gulzar, A.; Naz, S.; Ahmed, Z.; Tahir, A.H.; Mashhood, M. Knowledge, attitude, practice and perceived barriers among healthcare workers regarding COVID-19: A cross-sectional survey from Pakistan. J. Hosp. Infect. 2020, 105, 419–423. [Google Scholar] [CrossRef]
- USA Food and Drug Administration. Food Safety and Coronavirus Disease 2019. Available online: https://www.fda.gov/food/food-safety-during-emergencies/food-safety-and-coronavirus-disease-2019-covid-19 (accessed on 10 April 2020).
- World Health Organization (WHO). COVID-19 and Food Safety: Guidance for Food Businesses; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Jiang, F.; Deng, L.; Zhang, L.; Cai, Y.; Cheung, C.W.; Xia, Z. Review of the Clinical Characteristics of Coronavirus Disease 2019 (COVID-19). J. Gen. Int. Med. 2020, 4, 1–5. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Coronavirus Disease 2019, Advice for Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/myth-busters (accessed on 10 April 2020).
- Million, M.; Lagier, J.-C.; Gautret, P.; Colson, P.; Fournier, P.-E.; Amrane, S.; Hocquart, M.; Mailhe, M.; Esteves-Vieira, V.; Doudier, B.; et al. Early treatment of COVID-19 patients with hydroxychloroquine and azithromycin: A retrospective analysis of 1061 cases in Marseille, France. Travel Med. Infect. Dis. 2020, 35, 101738. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.-C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 2020, 105949. [Google Scholar] [CrossRef]
- Molina, J.-M.; Delaugerre, C.; Le Goff, J.; Mela-Lima, B.; Ponscarme, D.; Goldwirt, L.; De Castro, N. No evidence of rapid antiviral clearance or clinical benefit with the combination of hydroxychloroquine and azithromycin in patients with severe COVID-19 infection. Med. Mal. Infect. 2020, 50. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Frequency (n) | Percentage (%) |
|---|---|---|
| Age Groups (Mean Age = 28.73 ± 6.31 years) | ||
| <=25 | 142 | 36.9 |
| 26–29 | 125 | 32.5 |
| 30+ | 118 | 30.6 |
| Gender | ||
| Male | 181 | 47.0 |
| Female | 204 | 53.0 |
| Marital Status | ||
| Married | 195 | 50.6 |
| Unmarried | 190 | 49.4 |
| Highest Level of Education | ||
| Bachelor | 181 | 47.0 |
| Masters | 170 | 44.2 |
| Doctorate | 34 | 8.8 |
| Occupation | ||
| Physician | 144 | 37.4 |
| Pharmacist | 128 | 33.2 |
| Nurse | 113 | 29.4 |
| Workplace Organization Type | ||
| Public | 196 | 50.9 |
| Private | 189 | 49.1 |
| Locality | ||
| Urban | 340 | 88.3 |
| Rural | 45 | 11.7 |
| Items | Yes n (%) | No n (%) | Do Not Know n (%) |
|---|---|---|---|
| Have you heard about the novel corona virus and the related terms COVID-19 or 2019-nCoV? | 385 (100%) | 0 (0%) | 0 (0%) |
| COVID-19 disease is a viral infection. | 385 (100%) | 0 (0%) | 0 (0%) |
| COVID-19 can be transmitted through close contact with infected people and infected animals. | 381 (99%) | 4 (1%) | 0 (0%) |
| COVID-19 virus can be transmitted through contaminated food and water. | 162 (42.1%) | 198 (51.4%) | 25 (6.5%) |
| Fever, sore throat, cough, and shortness of breath are possible symptoms of COVID-19 infection. | 385 (100%) | 0 (0%) | 0 (0%) |
| The novel coronavirus is a similar virus as SARS-CoV and MERS-CoV. | 308 (80.0%) | 31 (8.1%) | 46 (11.9%) |
| Does the virus survive on surfaces of doors, tables and other objects? | 371 (96.4%) | 9 (2.3%) | 5 (1.3%) |
| Is the COVID-19 infection the same illness as flu or cold? | 69 (17.9%) | 309 (80.3%) | 7 (1.8%) |
| Is there any laboratory test to confirm the presence of COVID-19 infection? | 369 (95.8%) | 12 (3.1%) | 4 (1.0%) |
| The incubation period of COVID-19 infection is 1–2 weeks. | 375 (97.4%) | 3 (0.8%) | 7 (1.8%) |
| Can COVID-19 infection be caught from a person who presents no symptoms and has recently visited the affected area? | 369 (95.8%) | 10 (2.6%) | 6 (1.6%) |
| A vaccine for the COVID-19 virus is now available in the market. | 14 (3.6%) | 361 (93.8%) | 10 (2.6%) |
| Antibiotics are useful for the treatment of COVID-19 infection. | 142 (36.9%) | 233 (60.5%) | 10 (2.6%) |
| People with a compromised immune system and old age people are at more risk of developing the infection. | 384 (99.7%) | 1 (0.3%) | 0 (0%) |
| Patients with comorbidities are at more risk of developing the infection. | 373 (96.9%) | 7 (1.8%) | 5 (1.3%) |
| Health care workers and hospitalized patients who are near to infected patients are at more risk of developing the infection. | 384 (99.7%) | 1 (0.3%) | 0 (0%) |
| People in crowded places are at increased risk of getting affected by the disease. | 385 (100%) | 0 (0%) | 0 (0%) |
| Patients of COVID-19 infection should be immediately isolated to avoid the transfer of infection to other people. | 384 (99.7%) | 1 (0.3%) | 0 (0%) |
| Healthcare professionals are well prepared to cater to the people in case there is a spread of COVID-19 disease. | 326 (84.7%) | 50 (13.0%) | 9 (2.3%) |
| Items | SD n (%) | D n (%) | N n (%) | A n (%) | SA n (%) |
|---|---|---|---|---|---|
| The disease can be transmitted by coughing and sneezing. | 4 (1.0%) | 2 (0.5%) | 3 (0.8%) | 106 (27.5%) | 270 (70.1%) |
| Transmission of COVID-19 infection can be prevented through wearing masks. | 0 (0%) | 6 (1.6%) | 18 (4.7%) | 182 (47.3%) | 179 (46.5%) |
| Transmission of COVID-19 infection can be prevented through washing hands and face regularly with antiseptics and sanitizers. | 2 (0.5%) | 0 (0%) | 8 (2.1%) | 146 (37.9%) | 229 (59.5%) |
| Transmission of COVID-19 infection can be prevented through the isolation of COVID-19-infected patients. | 0 (0%) | 0 (0%) | 9 (2.3%) | 141 (36.6%) | 235 (61.0%) |
| Transmission of COVID-19 infection can be prevented by taking antibiotics. | 114 (29.6%) | 92 (23.9%) | 29 (7.5%) | 64 (16.6%) | 86 (22.3%) |
| Restricting the travel of COVID-19-infected people to other areas of the world and of people in other areas to affected areas can be beneficial to prevent the spread of the infection. | 1 (0.3%) | 1 (0.3%) | 12 (3.1%) | 158 (41.0%) | 213 (55.3%) |
| Having a healthy and well-cooked diet can be helpful in reducing the risk of getting the novel coronavirus disease. | 1 (0.3%) | 13 (3.4%) | 36 (9.4%) | 189 (49.1%) | 146 (37.9%) |
| Avoiding touching the nose, mouth, and eyes can reduce the risk of infection. | 0 (0%) | 0 (0%) | 7 (1.8%) | 180 (46.8%) | 198 (51.4%) |
| Avoiding touching the surface of doors, furniture, or other things can be helpful in preventing the disease. | 1 (0.3%) | 3 (0.8%) | 26 (6.8%) | 195 (50.6%) | 160 (41.6%) |
| If a vaccine is developed against the novel coronavirus, it can significantly reduce the epidemic spread. | 1 (0.3%) | 2 (0.5%) | 26 (6.8%) | 183 (47.5%) | 173 (44.9%) |
| The available information about COVID-19 disease is sufficient in Pakistani society. | 18 (4.7%) | 58 (15.1%) | 43 (11.2%) | 138 (35.8%) | 128 (33.2%) |
| The government in our country has all the necessary healthcare facilities and is able to control the epidemic situation. | 35 (9.1%) | 63 (16.4%) | 36 (9.4%) | 138 (35.8%) | 113 (29.4%) |
| Items | Always n (%) | Mostly n (%) | Sometimes n (%) | Rarely n (%) | Never n (%) |
|---|---|---|---|---|---|
| I advise the general public to eat thoroughly cooked food, especially meat products. | 247 (64.2%) | 111 (28.8%) | 21 (5.5%) | 5 (1.3%) | 1 (0.3%) |
| I advise the public to keep themselves warm and hydrated. | 207 (53.8%) | 152 (39.5%) | 23 (6.0%) | 2 (0.5%) | 1 (0.3%) |
| I advise people to use soap or sanitizer regularly to wash their hands and face. | 276 (71.7%) | 97 (25.2%) | 11 (2.9%) | 1 (0.3%) | 0 (0%) |
| I advise the general public to avoid close contact with people with cough and flu-like symptoms. | 234 (60.8%) | 111 (28.8%) | 21 (5.5%) | 11 (2.9%) | 8 (2.1%) |
| During interaction with a COVID-19 patient, I wear the necessary personal protective equipment (PPE) such as masks, gloves, gown, etc. | 238 (61.8%) | 117 (30.4%) | 24 (6.2%) | 4 (1.0%) | 2 (0.5%) |
| I perform hand hygiene before and after touching COVID-19 patients or before and after performing an aseptic procedure. | 252 (65.5%) | 101 (26.2%) | 24 (6.2%) | 6 (1.6%) | 2 (0.5%) |
| I perform hand hygiene after touching a patient’s surroundings such as beds, tables, doors, etc. | 219 (56.9%) | 125 (32.5%) | 28 (7.3%) | 9 (2.3%) | 4 (1.0%) |
| I avoid unnecessary close contact, practice social distancing, and keep at least 1 meter distance from patients and other healthcare workers. | 233 (60.5%) | 98 (25.5%) | 27 (7.0%) | 13 (3.4%) | 14 (3.6%) |
| Characteristics | Study Group | p-Value |
|---|---|---|
| Total Score on Knowledge | Pharmacist–Nurse | 0.162 |
| Pharmacist–Physician | 0.000 * | |
| Nurse–Physician | 0.000 * | |
| Total Score on Attitude | Pharmacist–Nurse | 0.310 |
| Pharmacist–Physician | 0.000 * | |
| Nurse–Physician | 0.001 * | |
| Total Score on Practices and Risk Assessment | Pharmacist–Nurse | 0.000 * |
| Pharmacist–Physician | 0.000 * | |
| Nurse–Physician | 0.092 |
| Study Group | p-Values * | ||
|---|---|---|---|
| Knowledge | Attitude | Practice | |
| Physicians + Nurses + Pharmacists | <0.001 | <0.001 | 0.221 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malik, U.R.; Atif, N.; Hashmi, F.K.; Saleem, F.; Saeed, H.; Islam, M.; Jiang, M.; Zhao, M.; Yang, C.; Fang, Y. Knowledge, Attitude, and Practices of Healthcare Professionals on COVID-19 and Risk Assessment to Prevent the Epidemic Spread: A Multicenter Cross-Sectional Study from Punjab, Pakistan. Int. J. Environ. Res. Public Health 2020, 17, 6395. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176395
Malik UR, Atif N, Hashmi FK, Saleem F, Saeed H, Islam M, Jiang M, Zhao M, Yang C, Fang Y. Knowledge, Attitude, and Practices of Healthcare Professionals on COVID-19 and Risk Assessment to Prevent the Epidemic Spread: A Multicenter Cross-Sectional Study from Punjab, Pakistan. International Journal of Environmental Research and Public Health. 2020; 17(17):6395. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176395
Chicago/Turabian StyleMalik, Usman Rashid, Naveel Atif, Furqan Khurshid Hashmi, Fahad Saleem, Hamid Saeed, Muhammad Islam, Minghuan Jiang, Mingyue Zhao, Caijun Yang, and Yu Fang. 2020. "Knowledge, Attitude, and Practices of Healthcare Professionals on COVID-19 and Risk Assessment to Prevent the Epidemic Spread: A Multicenter Cross-Sectional Study from Punjab, Pakistan" International Journal of Environmental Research and Public Health 17, no. 17: 6395. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176395