Neighborhood Socioeconomic Deprivation Associated with Fat Mass and Weight Status in Youth

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Weight-Related Outcomes
2.2. Neighborhood Socioeconomic Deprivation (SED)
2.3. Physical Activity
2.4. Diet Quality
2.5. Student Characteristics
2.6. Statistical Analyses
3. Results
3.1. Descriptives
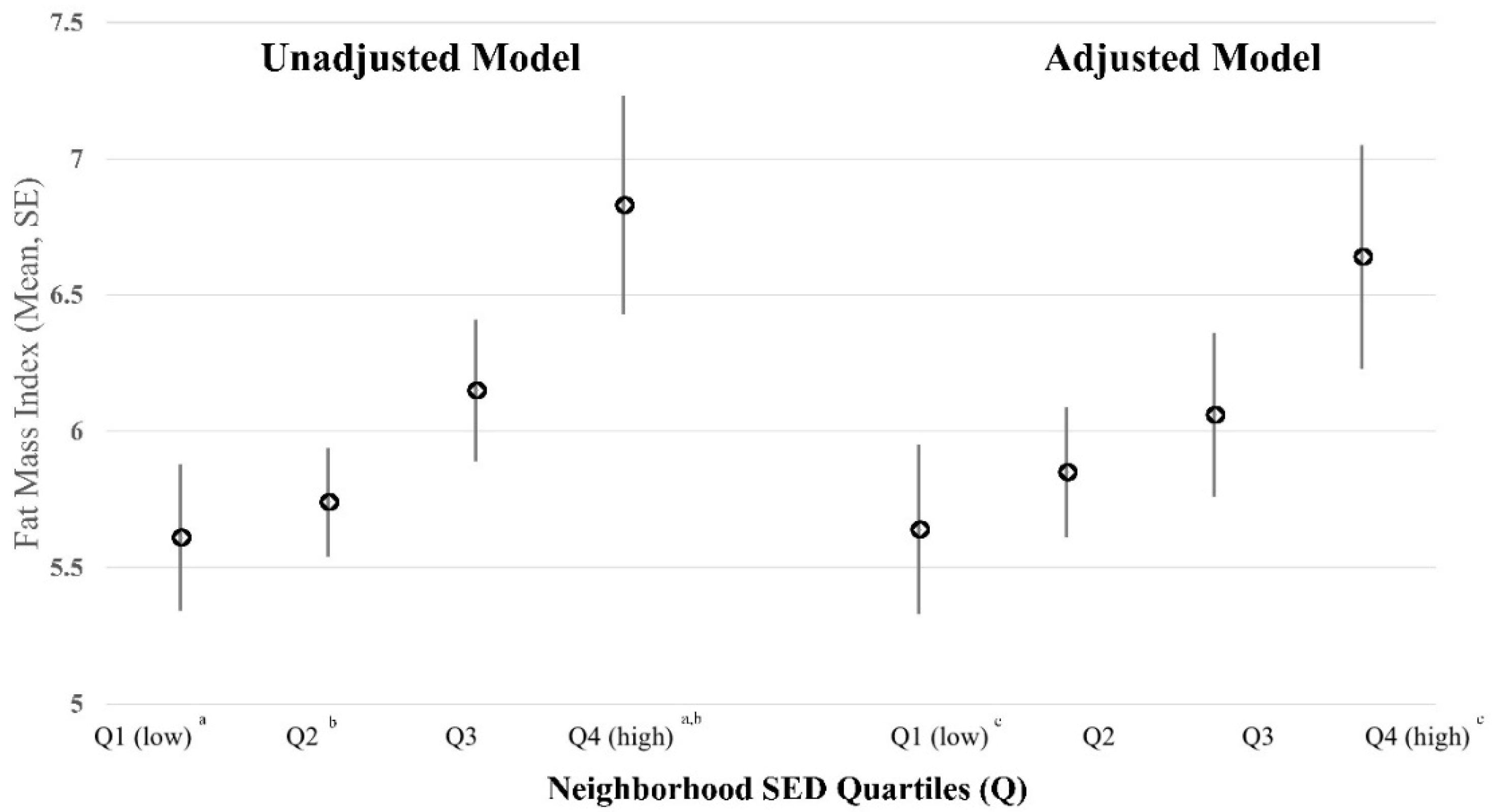
3.2. Multilevel Linear Regression Results
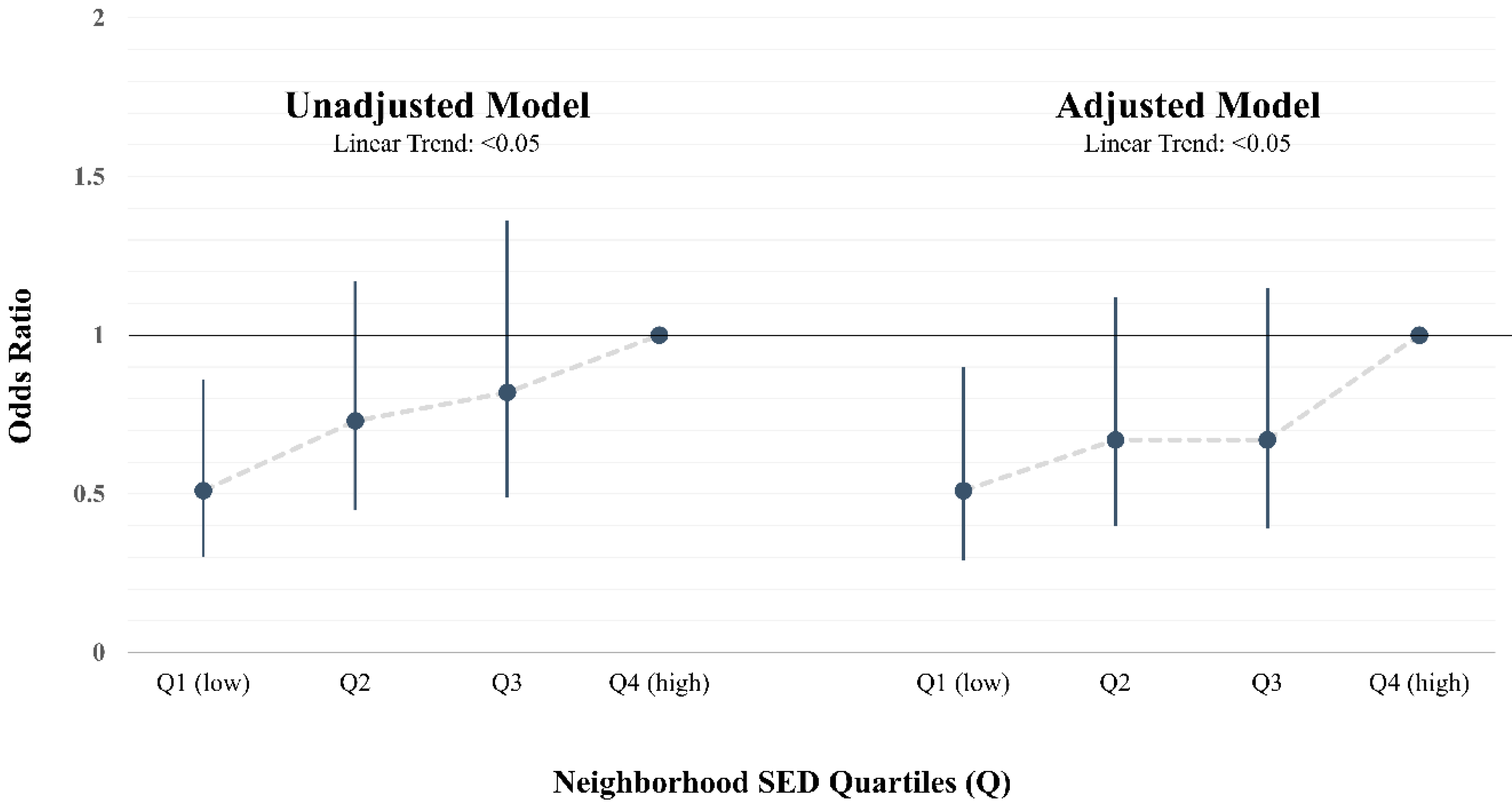
3.3. Multilevel Logistic Regression Results
3.4. Adjusted Least Square Means
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Center for Health Statistics. Special Feature on Socioeconomic Status and Health; National Center for Health: Hyattsville, MD, USA, 2012. [Google Scholar]
- Ogden, C.L.; Carroll, M.D.; Lawman, H.G.; Fryar, C.D.; Kruszon-Moran, D.; Kit, B.K.; Flegal, K.M. Trends in obesity prevalence among children and adolescents in the United States, 1988–1994 through 2013–2014. Jama 2016, 315, 2292–2299. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of obesity among adults and youth: United States, 2015–2016. In NCHS Data Brief; National Center for Health Statistics: Hyattsville, MD, USA, 2017. [Google Scholar]
- Cote, A.T.; Harris, K.C.; Panagiotopoulos, C.; Sandor, G.G.; Devlin, A.M. Childhood obesity and cardiovascular dysfunction. J. Am. Coll. Cardiol. 2013, 62, 1309–1319. [Google Scholar] [CrossRef] [Green Version]
- Bacha, F.; Gidding, S.S. Cardiac abnormalities in youth with obesity and type 2 diabetes. Curr. Diab. Rep. 2016, 16, 62. [Google Scholar] [CrossRef] [PubMed]
- Anderssen, S.A.; Cooper, A.R.; Riddoch, C.; Sardinha, L.B.; Harro, M.; Brage, S.; Andersen, L.B. Low cardiorespiratory fitness is a strong predictor for clustering of cardiovascular disease risk factors in children independent of country, age and sex. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Berenson, G.S.; Srinivasan, S.R.; Bao, W.; Newman, W.P.; Tracy, R.E.; Wattigney, W.A. Association between multiple cardiovascular risk factors and atherosclerosis in children and young adults. N. Engl. J. Med. 1998, 338, 1650–1656. [Google Scholar] [CrossRef] [PubMed]
- Frederick, C.B.; Snellman, K.; Putnam, R.D. Increasing socioeconomic disparities in adolescent obesity. Proc. Natl. Acad. Sci. USA 2014, 111, 1338–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvarado, S.E. Neighborhood disadvantage and obesity across childhood and adolescence: Evidence from the NLSY children and young adults cohort (1986–2010). Soc. Sci. Res. 2016, 57, 80–98. [Google Scholar] [CrossRef] [Green Version]
- Cubbin, C.; Sundquist, K.; Ahlén, H.; Johansson, S.E.; Winkleby, M.A.; Sundquist, J. Neighborhood deprivation and cardiovascular disease risk factors: Protective and harmful effects. Scand. J. Public Health 2006, 34, 228–237. [Google Scholar] [CrossRef]
- Gustafsson, P.E.; San Sebastian, M.; Janlert, U.; Theorell, T.; Westerlund, H.; Hammarström, A. Life-course accumulation of neighborhood disadvantage and allostatic load: Empirical integration of three social determinants of health frameworks. Am. J. Public Health 2014, 104, 904–910. [Google Scholar] [CrossRef]
- Leal, C.; Bean, K.; Thomas, F.; Chaix, B. Are associations between neighborhood socioeconomic characteristics and body mass index or waist circumference based on model extrapolations? Epidemiology 2011, 22, 694–703. [Google Scholar] [CrossRef] [Green Version]
- Meijer, M.; Röhl, J.; Bloomfield, K.; Grittner, U. Do neighborhoods affect individual mortality? A systematic review and meta-analysis of multilevel studies. Soc. Sci. Med. 2012, 74, 1204–1212. [Google Scholar] [CrossRef] [PubMed]
- Shishehbor, M.H.; Gordon-Larsen, P.; Kiefe, C.I.; Litaker, D. Association of neighborhood socioeconomic status with physical fitness in healthy young adults: The Coronary Artery Risk Development in Young Adults (CARDIA) study. Am. Heart J. 2008, 155, 699–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theall, K.P.; Drury, S.S.; Shirtcliff, E.A. Cumulative neighborhood risk of psychosocial stress and allostatic load in adolescents. Am. J. Epidemiol. 2012, 176, S164–S174. [Google Scholar] [CrossRef] [Green Version]
- Vartanian, T.P.; Houser, L. The effects of childhood neighborhood conditions on self-reports of adult health. J. Health Soc. Behav. 2010, 51, 291–306. [Google Scholar] [CrossRef] [PubMed]
- Schüle, S.A.; Bolte, G. Interactive and independent associations between the socioeconomic and objective built environment on the neighbourhood level and individual health: A systematic review of multilevel studies. PLoS ONE 2015, 10, e0123456. [Google Scholar] [CrossRef]
- Nau, C.; Schwartz, B.S.; Bandeen-Roche, K.; Liu, A.; Pollak, J.; Hirsch, A.; Bailey-Davis, L.; Glass, T.A. Community socioeconomic deprivation and obesity trajectories in children using electronic health records. Obesity 2015, 23, 207–212. [Google Scholar] [CrossRef] [Green Version]
- Voorhees, C.C.; Catellier, D.J.; Ashwood, J.S.; Cohen, D.A.; Rung, A.; Lytle, L.; Conway, T.L.; Dowda, M. Neighborhood socioeconomic status and non school physical activity and body mass index in adolescent girls. J. Phys. Act. Health 2009, 6, 731–740. [Google Scholar] [CrossRef]
- Janssen, I.; Boyce, W.F.; Simpson, K.; Pickett, W. Influence of individual-and area-level measures of socioeconomic status on obesity, unhealthy eating, and physical inactivity in Canadian adolescents. Am. J. Clin. Nutr. 2006, 83, 139–145. [Google Scholar] [CrossRef]
- Wardle, J.; Jarvis, M.J.; Steggles, N.; Sutton, S.; Williamson, S.; Farrimond, H.; Cartwright, M.; Simon, A.E. Socioeconomic disparities in cancer-risk behaviors in adolescence: Baseline results from the Health and Behaviour in Teenagers Study (HABITS). Prev. Med. 2003, 36, 721–730. [Google Scholar] [CrossRef]
- Oliver, L.N.; Hayes, M.V. Effects of neighbourhood income on reported body mass index: An eight year longitudinal study of Canadian children. BMC Public Health 2008, 8, 1. [Google Scholar] [CrossRef] [Green Version]
- Rossen, L.M. Neighbourhood economic deprivation explains racial/ethnic disparities in overweight and obesity among children and adolescents in the USA. J. Epidemiol. Community Health 2014, 68, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Grow, H.M.; Cook, A.J.; Arterburn, D.E.; Saelens, B.E.; Drewnowski, A.; Lozano, P. Child obesity associated with social disadvantage of children’s neighborhoods. Soc. Sci. Med. 2010, 71, 584–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nevill, A.M.; Duncan, M.J.; Lahart, I.; Sandercock, G. Modelling the association between weight status and social deprivation in English school children: Can physical activity and fitness affect the relationship? Ann. Hum. Biol. 2016, 43, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Colabianchi, N.; Griffin, J.L.; McIver, K.L.; Dowda, M.; Pate, R.R. Where are children active and does it matter for physical activity? A latent transition analysis. J. Phys. Act. Health 2016, 13, 1294–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M. 2000 CDC Growth Charts for the United States: Methods and development. Vital Health Stat. 2002, 246, 1–190. [Google Scholar]
- Horlick, M.; Arpadi, S.M.; Bethel, J.; Wang, J.; Moye, J., Jr.; Cuff, P.; Pierson, R.N., Jr.; Kotler, D. Bioelectrical impedance analysis models for prediction of total body water and fat-free mass in healthy and HIV-infected children and adolescents. Am. J. Clin. Nutr. 2002, 76, 991–999. [Google Scholar] [CrossRef]
- Lian, M.; Struthers, J.; Liu, Y. Statistical Assessment of Neighborhood Socioeconomic Deprivation Environment in Spatial Epidemiologic Studies. Open J. Stat. 2016, 6, 436. [Google Scholar] [CrossRef] [Green Version]
- Puyau, M.R.; Adolph, A.L.; Vohra, F.A.; Butte, N.F. Validation and calibration of physical activity monitors in children. Obesity 2002, 10, 150–157. [Google Scholar] [CrossRef]
- Trost, S.G.; Ward, D.S.; Moorehead, S.M.; Watson, P.D.; Riner, W.; Burke, J.R. Validity of the computer science and applications (CSA) activity monitor in children. Med. Sci. Sports Exerc. 1998, 30, 629–633. [Google Scholar] [CrossRef]
- Freedson, P.; Pober, D.; Janz, K.F. Calibration of accelerometer output for children. Med. Sci. Sports Exerc. 2005, 37, S523. [Google Scholar] [CrossRef]
- Dishman, R.K.; McIver, K.L.; Dowda, M.; Saunders, R.P.; Pate, R.R. Motivation and Behavioral Regulation of Physical Activity in Middle School Students. Med. Sci. Sports Exerc. 2015, 47, 1913–1921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunsberger, M.; O’Malley, J.; Block, T.; Norris, J.C. Relative validation of B lock K ids F ood S creener for dietary assessment in children and adolescents. Matern. Child Nutr. 2015, 11, 260–270. [Google Scholar] [CrossRef]
- Guenther, P.M.; Casavale, K.O.; Reedy, J.; Kirkpatrick, S.I.; Hiza, H.A.; Kuczynski, K.J.; Kahle, L.L.; Krebs-Smith, S.M. Update of the healthy eating index: HEI-2010. J. Acad. Nutr. Diet. 2013, 113, 569–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freedman, D.S.; Sherry, B. The validity of BMI as an indicator of body fatness and risk among children. Pediatrics 2009, 124, S23–S34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slater, S.J.; Ewing, R.; Powell, L.M.; Chaloupka, F.J.; Johnston, L.D.; O’Malley, P.M. The association between community physical activity settings and youth physical activity, obesity, and body mass index. J. Adolesc. Health 2010, 47, 496–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, S.M.; van Horn, M.L.; Lawman, H.G.; Wilson, D.K. Reliability of 24-hour dietary recalls as a measure of diet in African-American youth. J. Acad. Nutr. Diet. 2016, 116, 1551–1559. [Google Scholar] [CrossRef]
- Peart, T.; Velasco Mondragon, H.E.; Rohm-Young, D.; Bronner, Y.; Hossain, M.B. Weight status in US youth: The role of activity, diet, and sedentary behaviors. Am. J. Health Behav. 2011, 35, 756–764. [Google Scholar] [CrossRef]
- Carroll-Scott, A.; Gilstad-Hayden, K.; Rosenthal, L.; Peters, S.M.; McCaslin, C.; Joyce, R.; Ickovics, J.R. Disentangling neighborhood contextual associations with child body mass index, diet, and physical activity: The role of built, socioeconomic, and social environments. Soc. Sci. Med. 2013, 95, 106–114. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Participant Characteristics a | Total Sample (n = 828) |
|---|---|
| Age (years) | 10.6 (0.5) |
| Sex | |
| Male | 45.3% |
| Female | 54.7% |
| Race/Ethnicity | |
| Non-Hispanic White | 39.1% |
| Non-Hispanic Black | 33.6% |
| Hispanic | 10.4% |
| Other | 16.9% |
| Parent Education | |
| ≤High School Education | 42.3% |
| >High School Education | 57.7% |
| Weight-Related Outcomes | |
| Fat Mass Index | 5.9 (3.7) |
| Body Mass Index (BMI) | 21.0 (4.7) |
| BMI Percentile | 72.8 (26.9) |
| Weight Status | |
| Normal Weight/Underweight | 53.1% |
| Overweight/Obese | 46.9% |
| Physical Activity (PA) | |
| Moderate-to-Vigorous PA (Minutes/Hour) b | 2.8 (1.8) |
| Sedentary Behavior (Minutes/Hour) c | 32.1 (4.4) |
| Diet Quality | |
| Healthy Eating Index d | 30.1 (5.38) |
| Neighborhood Socioeconomic Deprivation e | −0.19 (0.65) |
| Variable | Model 1. Unadjusted | Model 2. Adjusted a | Model 3. + MVPA a | Model 4. + Sedentary a | Model 5. + Diet a | Model 6. Fully Adjusted a | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Estimate (SE) | Estimate (SE) | Estimate (SE) | Estimate (SE) | Estimate (SE) | Estimate (SE) | |||||||
| Neighborhood SED | 0.54 (0.19) | ** | 0.41 (0.20) | * | 0.39 (0.21) | 0.42 (0.21) | * | 0.45 (0.20) | * | 0.45 (0.21) | * | |
| MVPA | −0.61 (0.08) | *** | −0.45 (0.09) | *** | ||||||||
| Sedentary | 0.20 (0.03) | *** | 0.12 (0.03) | *** | ||||||||
| Diet Quality | 0.04 (0.02) | 0.04 (0.02) | ||||||||||
| Goodness of Fit | ||||||||||||
| −2 LL | 4488.2 | 4449.1 | 4392.1 | 4407.6 | 4452.1 | 4388.3 | ||||||
| AIC | 4492.2 | 4451.1 | 4396.1 | 4411.6 | 4454.1 | 4392.3 | ||||||
| Variable | Model 1. Unadjusted | Model 2. Adjusted a | Model 3. + MVPA a | Model 4. + Sedentary a | Model 5. + Diet a | Model 6: Fully Adjusted a |
|---|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Neighborhood SED | 1.36 (1.10, 1.69) | 1.29 (1.03, 1.61) | 1.28 (1.01, 1.60) | 1.29 (1.02, 1.62) | 1.31 (1.05, 1.65) | 1.30 (1.03, 1.65) |
| MVPA | 0.75 (0.68, 0.83) | 0.80 (0.71, 0.90) | ||||
| Sedentary | 1.09 (1.05, 1.12) | 1.04 (0.99, 1.08) | ||||
| Diet Quality | 1.02 (0.99, 1.05) | 1.02 (0.99, 1.05) | ||||
| Goodness of Fit | ||||||
| −2 LL | 1136.2 | 1132.3 | 1096.1 | 1108.4 | 1130.4 | 1090.9 |
| AIC | 1140.2 | 1148.3 | 1114.1 | 1126.4 | 1148.4 | 1114.9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clennin, M.; Brown, A.; Lian, M.; Dowda, M.; Colabianchi, N.; Pate, R.R. Neighborhood Socioeconomic Deprivation Associated with Fat Mass and Weight Status in Youth. Int. J. Environ. Res. Public Health 2020, 17, 6421. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176421
Clennin M, Brown A, Lian M, Dowda M, Colabianchi N, Pate RR. Neighborhood Socioeconomic Deprivation Associated with Fat Mass and Weight Status in Youth. International Journal of Environmental Research and Public Health. 2020; 17(17):6421. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176421
Chicago/Turabian StyleClennin, Morgan, Asia Brown, Min Lian, Marsha Dowda, Natalie Colabianchi, and Russell R. Pate. 2020. "Neighborhood Socioeconomic Deprivation Associated with Fat Mass and Weight Status in Youth" International Journal of Environmental Research and Public Health 17, no. 17: 6421. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176421