The Effect of Wearing a Customized Mouthguard on Body Alignment and Balance Performance in Professional Basketball Players


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Procedure
2.3. Mouthguard
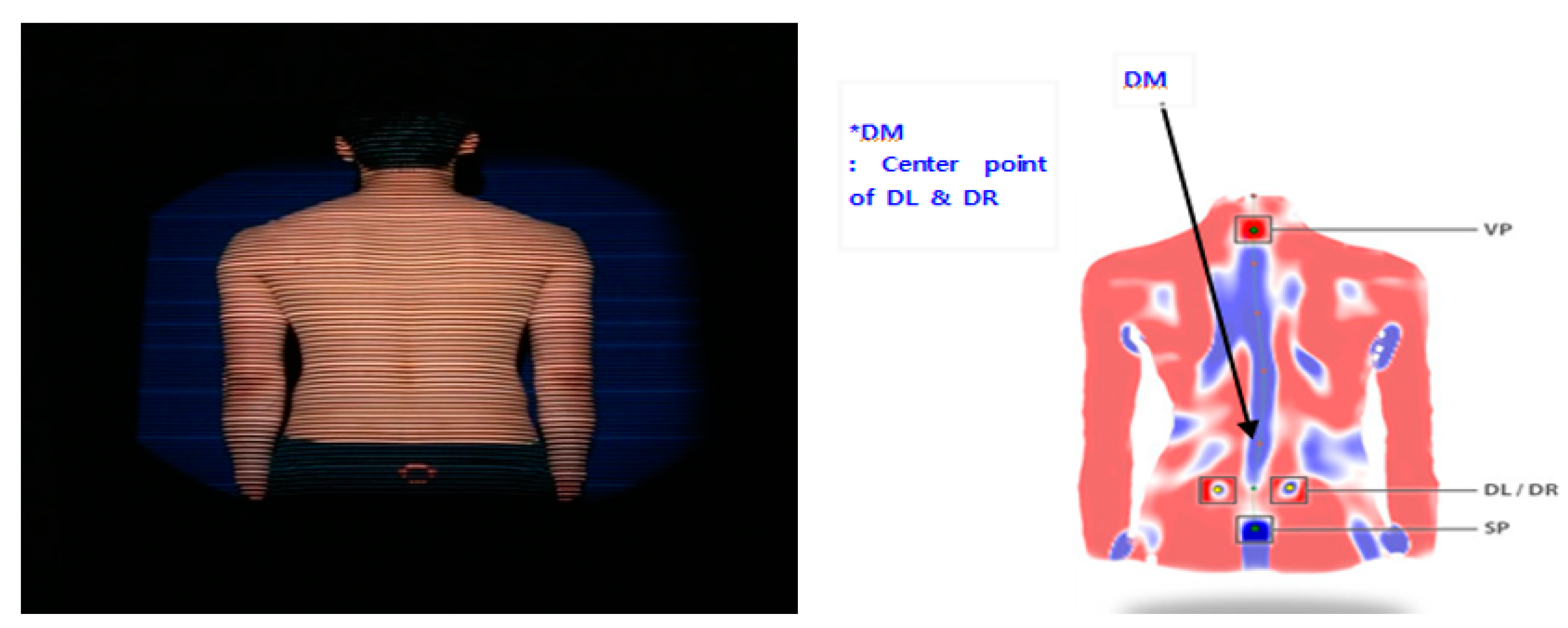
2.4. Measurement of Body Alignment
2.5. Measurement of Balance Performance
2.6. Statistical Analysis
3. Results
3.1. Changes in Body Alignment
3.2. Changes in Balance Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jeon, K.; Kim, S. Effect of unilateral exercise on spinal and pelvic deformities, and isokinetic trunk muscle strength. J. Phys. Ther. Sci. 2016, 28, 844–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, J.C.; Suh, S.W.; Jung, B.J.; Hur, C.Y.; Chae, I.J.; Kang, C.S.; Wang, J.H.; Moon, W.N.; Cheon, E.M. Asymmetric Exercise and Scoliosis-A Study on Volleyball Athletes. Kor. J. Orthop. Assoc. 2001, 36, 455–460. [Google Scholar] [CrossRef]
- Omey, M.L.; Micheli, L.J.; Gerbino, P.G. Idiopathic scoliosis and spondylosis in the female athlete. Clin. Orthop. 2000, 372, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Sadat-Ali, M.; Al-Othman, A.; Bubshait, D.; Al-Dakheel, D. Does scoliosis causes low bone mass? A comparative study between siblings. Eur. J. Spine. 2008, 17, 944–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nault, M.L.; Allard, P.; Hinse, S.; Le Blanc, R.; Caron, O.; Labelle, H.; Sadeghi, H. Relations between standing stability and body posture parameters in adolescent idiopathic scoliosis. Spine 2002, 27, 1911–1917. [Google Scholar] [CrossRef] [PubMed]
- Yagi, M.; Kaneko, S.; Yato, Y.; Asazuma, T. Standing balance and compensatory mechanisms in patients with adult spinal deformity. Spine 2017, 42, 584–591. [Google Scholar] [CrossRef]
- Modi, H.; Srinivasalu, S.; Mehta, S.; Yang, J.H.; Song, H.R.; Suh, S.W. Muscle imbalance in volleyball players initiates scoliosis in immature spines: A screening analysis. Asian Spine J. 2008, 2, 38. [Google Scholar] [CrossRef] [Green Version]
- Gravara, M.; Hadzik, A. Postural variables in girls practicing volleyball. Biomed. Hum. Kinet. 2009, 1, 67–71. [Google Scholar]
- Hawrylak, A.; Skolimowski, T.; Barczyk, K.; Biec, E. Asymetry of trunk in athletes of different kind of sports. Pol. J. Sports Med. 2001, 17, 232–235. [Google Scholar]
- Scanlan, A.T.; Fox, J.L.; Borges, N.R.; Tucker, P.S.; Dalbo, V.J. Temporal changes in physiological and performance responses across game-specific simulated basketball activity. J. Sport Health Sci. 2018, 7, 176–182. [Google Scholar] [CrossRef]
- Drakos, M.C.; Domb, B.; Starkey, C.; Callahan, L.; Allen, A.A. Injury in the National Basketball Association: A 17-year overview. Sports Health 2010, 2, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Neumann, D.A. Kinesiology of the Musculoskeletal System: Foundations for Physical Rehabilitation, 1st ed.; St. Mosby: Michigan, MI, USA, 2002. [Google Scholar]
- Morimoto, T.; Sonohata, M.; Kitajima, M.; Yoshihara, T.; Hirata, H.; Mawatari, M. Hip-Spine Syndrome: The Coronal Alignment of the Lumbar Spine and Pelvis in Patients with Ankylosed Hips. Spine Surg. Relat. Res. 2019, 4, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Baldini, A.; Beraldi, A.; Nota, A.; Danelon, F.; Ballanti, F.; Longoni, S. Gnathological postural treatment in a professional basketball player: A case report and an overview of the role of dental occlusion on performance. Ann. Stomatol. 2012, 3, 51. [Google Scholar]
- Mannheimer, J.S.; Rosenthal, R.M. Acute and chronic postural abnormalities as related to craniofacial pain and temporomandibular disorders. Dent. Clin. N. Am. 1991, 35, 185–208. [Google Scholar] [PubMed]
- Gelb, H.; Mehta, N.R.; Forgiane, A.G. The relationship between jaw posture and muscular strength in sports dentistry: A reappraisal. J. Craniomandib. Pract. 1996, 14, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Cetin, C.; Kececi, A.D.; Erdogan, A.; Baydar, M.L. Influence of custom-made mouth guards on strength, speed and anaerobic performance of teakwondo athletes. Dent. Traumatol. 2009, 25, 272–276. [Google Scholar] [CrossRef]
- Queiroz, A.F.; de Brito, R.B.; Ramacciato, J.C.; Motta, R.H.; Florio, F.M. Influence of mouthguards on the physical performance of soccer players. Dent. Traumatol. 2013, 26, 450–454. [Google Scholar] [CrossRef]
- Allen, C.R.; Dabbs, N.C.; Zachary, C.S.; Garmer, J.C. The acute effect of a commercial bite-aligning mouth-piece on strength and power in recreationally trained men. J. Strength Cond. Res. 2014, 28, 499–503. [Google Scholar] [CrossRef]
- Gravara, M.; Hadzik, A. The body posture in young athletes compared to their peers. Med. Sport. 2009, 25, 115–124. [Google Scholar]
- Grabara, M. Body posture of young female basketball players. Biomed. Hum. Kinet. 2012, 4, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Rocha, C.P.; Croci, C.S.; Caria, P.H. Is there relationship between temporomandibular disorders and head and cervical posture? A systematic review. J. Oral Rehabil. 2013, 40, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Martins, R.S.; Girouard, P.; Elliott, E.; Mekary, S. Physiological responses of a jaw-repositioning custom-made mouthguard on airway and their effects on athletic performance. J. Strength Cond. Res. 2020, 34, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Wojtys, E.; Ashton-Miller, J.; Huston, L.; Moga, P. The assocation between athletic training time and the sagittal curvature of the immature spine. Am. J. Sports Med. 2000, 28, 490–498. [Google Scholar] [CrossRef]
- Boldori, L.; Da Solda, M.; Marelli, A. Anomalies of the trunk. An analysis of their prevalence in young athletes. Minerva. Pediatr. 1999, 51, 259–264. [Google Scholar] [PubMed]
- Kantor, E.; Poupard, L.; Le Bozec, S.; Bouisset, S. Does body stability depend on postural chain mobility or stability area? Neurosci. Lett. 2001, 308, 128–132. [Google Scholar] [CrossRef]
- Gangloff, P.; Louis, J.P.; Perrin, P.P. Dental occlusion modifies gaze postural stabilization in human subjects. Neurosci. Lett. 2000, 293, 203–206. [Google Scholar] [CrossRef]
- Milani, R.S.; De Pierre, D.D.; Lapeyre, L.; Pourreyron, L. Relationship between dental occlusion and posture. J. Craniomandib. Pract. 2000, 18, 127–134. [Google Scholar] [CrossRef]
- Sakaguchi, K.; Mehta, N.R.; Abdallah, E.F.; Forgione, A.G.; Hirayama, H.; Kawasaki, T.; Yokoyama, A. Examination of the relationship between mandibular position and body posture. Cranio. Oct. 2007, 25, 237–249. [Google Scholar] [CrossRef]
- Blum, C.A. Chiropractic perspective of dental occlusion’s affect on posture. J. Chiroprac. Edu. 2004, 18, 38. [Google Scholar]
- Guskiewicz, K.M.; Ross, S.E.; Marshall, S.W. Postural stability and neuropsychological deficits after concussion in collegiate athletes. J. Athl. Train. 2001, 36, 263–273. [Google Scholar]
- Huang, M.H.; Brown, S.H. Age differences in the control of postural stability during reaching tasks. Gait Posture 2013, 38, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Hertel, J.; Plisky, P. Using the Star Excursion Balance Test to assess dynamic postural-control deficits and outcomes in lower extremity injury: A literature and systematic review. J. Athl. Train. 2012, 47, 339–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hrysomallis, C. Balance ability and athletic performance. Sports Med. 2011, 41, 221–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scanian, A.; Dascombe, B.; Reabum, P. A comparison of the activity demands of elite and sub-elite Australian men’s basketball competition. J. Sports Sci. 2011, 29, 1153–1160. [Google Scholar] [CrossRef]
- Ben Abdelkrim, N.; El Fazaa, S.; El Ati, J. Time-motion analysis and physiological data of elite under-19-year-old basketball players during competition. Br. J. Sports Med. 2007, 41, 69–75. [Google Scholar] [CrossRef]
- Ferrari, C.H.; de Medeiros, J.M.F. Dental trauma and level of information: Mouth-guard use in different contact sports. Dent. Traumatol. 2002, 18, 144–147. [Google Scholar] [CrossRef]
- Duddy, F.A.; Weissman, J.; Lee, R.A.S.; Paranjpe, A.; Di Paolo, C. Influence of different types of mouth guards on strength and performance of collegiate athletes: A controlled-randomized trial. Dent. Traumatol. 2012, 28, 263–267. [Google Scholar] [CrossRef]
- Dumm-Lewis, C.; Luk, H.Y.; Comstock, B.A.; Szivak, T.K.; Hooper, D.R.; Kupchak, B.R.; Watts, A.M.; Putney, B.J.; Volek, H.J.S.; Denegar, C.R.; et al. The effects of a customized over-counter mouth guard on neuromuscular force and power production in trained men and women. J. Strength Cond. Res. 2012, 26, 1085–1093. [Google Scholar] [CrossRef]
- Morales, J.; Solana-Tramunt, M.; Miró, A.; García, M. Effects of jaw clenching while wearing a customized bite-aligning mouthpiece on strength in healthy young men. J. Strength Cond. Res. 2016, 30, 1102–1110. [Google Scholar]
- Tardieu, C.; Dumitrescu, M.; Giraudeau, A.; Blanc, J.L.; Cheynet, F.; Borel, L. Dental occlusion and postural control in adults. Neurosci. Lett. 2009, 450, 221–224. [Google Scholar] [CrossRef]
- Maeda, Y.; Emura, I.; Nakamura, K.; Nishida, K.; Nokubi, T. Study on the role of occlusal support for the body equilibrium function among elderly people -Examination with static and dynamic configuration-. J. Jpn. Prosthodont. Soc. 1995, 39, 900–905. [Google Scholar] [CrossRef] [Green Version]
- Golem, D.L.; Arent, S.M. Effects of over-the-counter jaw-repositioning mouth guards on dynamic balance, flexibility, agility, strength, and power in college-aged male athletes. J. Strength Cond. Res. 2015, 29, 500–512. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Definition | Unit |
|---|---|---|
| Torsion Trunk | Left and right rotation of trunk | [°] |
| Trunk Imbalance | From the VP to vertical line and angle of connect line from VP to DM | [°] |
| Trunk Inclination | Anterior and posterior inclination of trunk in the side position | [°] |
| Pelvic Tilt | Length of both pelvic tilts | [mm] |
| Pelvic Torsion | Contrary anterior and posterior torsion of both pelvic sides | [°] |
| Pelvic Rotation | Left and right rotation of both pelvic sides | [°] |
| Kyphotic Angle | Maximum kyphotic angle in the thoracic vertebrae part | [°] |
| Lordotic Angle | Maximum lordotic angle in the lumbar vertebrae part | [°] |
| Lateral Deviation | Lateral deviation length to connection line of VP and DM | [mm] |
| Surface Rotation | Surface rotation angle to connection line of VP and DM | [°] |
| Variables | NT | AT | RT | F-Value | p-Value |
|---|---|---|---|---|---|
| Trunk torsion [°] | 2.0 ± 6.81 | 1.6 ± 4.11 | 3.0 ± 4.43 | 0.782 | 0.451 |
| Trunk inclination [°] | 2.4 ± 2.92 | 1.8 ± 2.38 | 1.5 ± 1.83 | 2.928 | 0.075 |
| Trunk imbalance [°] | −0.3 ± 1.17 | −0.3 ± 0.77 | 0.04 ± 0.67 | 2.628 | 0.098 |
| Pelvic tilt [mm] | −0.7 ± 7.96 | 0.1 ± 6.62 | 0.3 ± 4.33 | 0.423 | 0.580 |
| Pelvic torsion [°] | 4.3 ± 2.93a | 2.9 ± 2.38b | 2.1 ± 2.01b | 9.569 | <0.001 |
| Pelvis rotation [°] | −1.8 ± 4.36 | −0.5 ± 2.96 | −0.3 ± 2.09 | 3.094 | 0.063 |
| Kyphotic angle [°] | 37.3 ± 6.37a | 38.6 ± 6.36a | 41.9 ± 5.99b | 13.197 | <0.001 |
| Lordotic angle [°] | 31.7 ± 8.84 | 33.4 ± 8.56 | 34.3 ± 9.12 | 3.223 | 0.072 |
| Surface rotation max [°] | 0.2 ± 7.60 | −2.0 ± 5.00 | −1.0 ± 4.07 | 1.979 | 0.169 |
| Lateral deviation max [mm] | 2.4 ± 9.22 | 1.9 ± 7.52 | 2.8 ± 6.30 | 0.314 | 0.675 |
| Variables | NT | AT | RT | F-Value | p-Value | |
|---|---|---|---|---|---|---|
| Static | RF X axis | 1368.4 ± 812.93a | 592.2 ± 477.59b | 327.0 ± 211.19c | 33.817 | <0.001 |
| RF Y axis | 425.1 ± 339.77a | 190.3 ± 168.24b | 327.0 ± 211.19a | 7.665 | 0.004 | |
| Sum of RF X + Y axis | 1502.4 ± 887.03a | 660.3 ± 525.93b | 374.8 ± 224.90c | 33.044 | <0.001 | |
| LF X axis | 1619.9 ± 1137.99a | 504.0 ± 355.42b | 258.4 ± 191.59c | 31.606 | <0.001 | |
| LF Y axis | 390.3 ± 305.74a | 155.7 ± 94.36b | 99.3 ± 52.53c | 20.193 | <0.001 | |
| Sum of LF X + Y axis | 1738.8 ± 1179.47a | 563.2 ± 370.38b | 300.2 ± 199.55c | 33.046 | <0.001 | |
| Dynamic | RF X axis | 1164.6 ± 508.36a | 660.0 ± 285.47b | 327.0 ± 211.19c | 42.657 | <0.001 |
| RF Y axis | 446.8 ± 172.96a | 363.8 ± 163.83a | 272.0 ± 122.69b | 16.306 | <0.001 | |
| Sum of RF X + Y axis | 1400.2 ± 549.12a | 847.0 ± 352.71b | 595.6 ± 208.65c | 40.962 | <0.001 | |
| LF X axis | 1280.0 ± 680.85a | 669.6 ± 363.73b | 412.0 ± 214.88c | 34.069 | <0.001 | |
| LF Y axis | 409.5 ± 180.06a | 306.0 ± 128.76a | 261.8 ± 106.02b | 10.670 | 0.001 | |
| Sum of LF X + Y axis | 1449.3 ± 710.18a | 819.6 ± 398.35b | 562.8 ± 251.46c | 32.918 | <0.001 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, H.J.; Lee, J.-H.; Hong, D.-S.; Jung, H.C. The Effect of Wearing a Customized Mouthguard on Body Alignment and Balance Performance in Professional Basketball Players. Int. J. Environ. Res. Public Health 2020, 17, 6431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176431
Nam HJ, Lee J-H, Hong D-S, Jung HC. The Effect of Wearing a Customized Mouthguard on Body Alignment and Balance Performance in Professional Basketball Players. International Journal of Environmental Research and Public Health. 2020; 17(17):6431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176431
Chicago/Turabian StyleNam, Hae Joo, Joon-Hee Lee, Dae-Seok Hong, and Hyun Chul Jung. 2020. "The Effect of Wearing a Customized Mouthguard on Body Alignment and Balance Performance in Professional Basketball Players" International Journal of Environmental Research and Public Health 17, no. 17: 6431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176431