Communicating Evidence about the Causes of Obesity and Support for Obesity Policies: Two Population-Based Survey Experiments

 , ,
, ,  ,
,
Abstract
:1. Background
2. Study 1
2.1. Method
2.1.1. Participants
2.1.2. Design
2.1.3. The Interventions
2.1.4. Measures
Policy Support
Causal Beliefs (Manipulation Checks)
Comprehension
Other Variables
2.1.5. Analyses
2.2. Results
2.2.1. Policy Support
2.2.2. Causal Beliefs (Manipulation Checks)
2.2.3. Subjective Comprehension
2.3. Discussion
3. Study 2
- I
- Communicating messages that attribute obesity to the environment will (a) increase support for obesity prevention policies and (b) strengthen the belief that the environment causes obesity
- II
- These effects will be greater amongst:
- participants from the USA
- participants who are obese or overweight
- III
- Participants from England will report greater levels of support for obesity prevention policies and will be more likely to believe that the environment causes obesity.
3.1. Method
3.1.1. Participants
3.1.2. Design
3.1.3. The Interventions
3.1.4. Measures
Primary Outcome(s)
Causal Beliefs (Manipulation Checks)
Other Variables
3.1.5. Analyses
3.2. Results
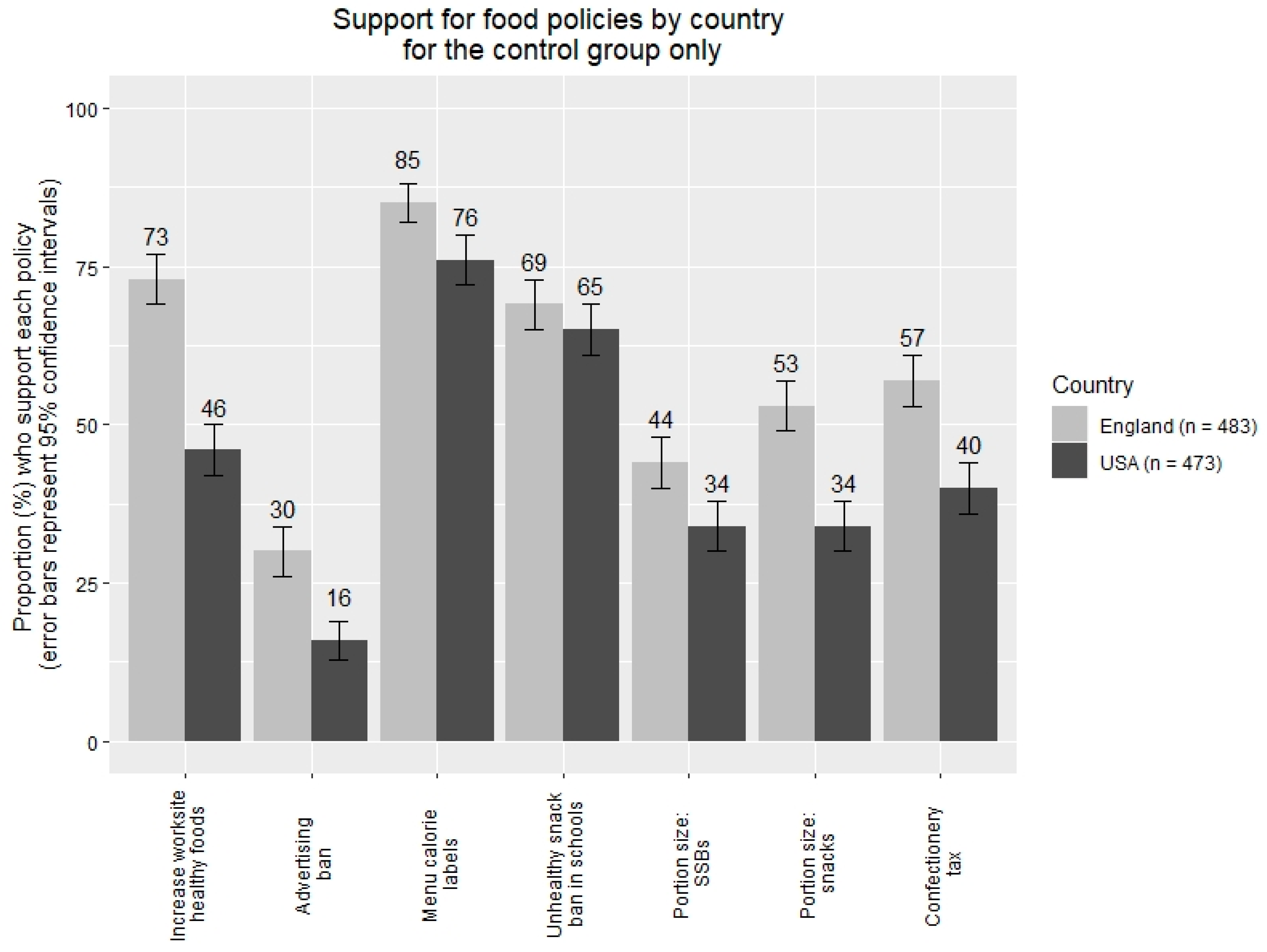
3.2.1. Policy Support
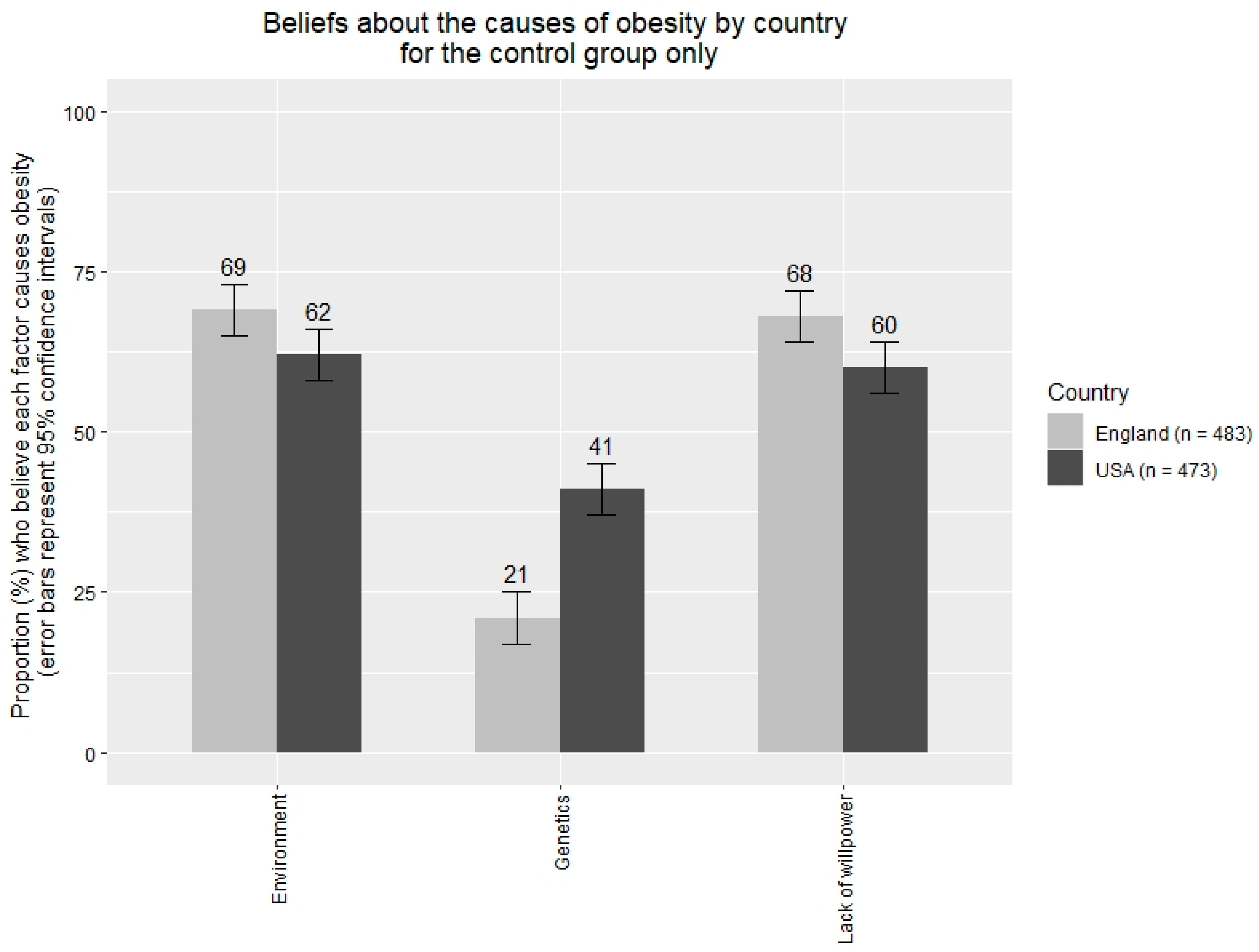
3.2.2. Beliefs about the Causes of Obesity (Manipulation Checks)
3.3. Discussion
4. General Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- GBD Obesity Collaborators. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Steel, N.; Ford, J.A.; Newton, J.N.; Davis, A.C.; Vos, T.; Naghavi, M.; Glenn, S.; Hughes, A.; Dalton, A.M.; Stockton, D. Changes in health in the countries of the UK and 150 English Local Authority areas 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018, 1647–1661. [Google Scholar] [CrossRef] [Green Version]
- Swinburn, B.A.; Kraak, V.I.; Allender, S.; Atkins, V.J.; Baker, P.I.; Bogard, J.R.; Brinsden, H.; Calvillo, A.; De Schutter, O.; Devarajan, R. The global syndemic of obesity, undernutrition, and climate change: The Lancet Commission report. Lancet 2019, 393, 791–846. [Google Scholar] [CrossRef]
- Hilbert, A.; Rief, W.; Braehler, E. What determines public support of obesity prevention? J. Epidemiol. Community Health 2007, 61, 585–590. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, J.P.; Pilling, M.; Marteau, T.M. Communicating quantitative evidence of policy effectiveness and support for the policy: Three experimental studies. Soc. Sci. Med. 2018, 218, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, J.P.; Archer, S.; Pilling, M.; Kenny, M.; Hollands, G.J.; Marteau, T. Public acceptability of nudging and taxing to reduce consumption of alcohol, tobacco, and food: A population-based survey experiment. Soc. Sci. Med. 2019, 236, 112395. [Google Scholar] [CrossRef]
- Diepeveen, S.; Ling, T.; Suhrcke, M.; Roland, M.; Marteau, T.M. Public acceptability of government intervention to change health-related behaviours: A systematic review and narrative synthesis. BMC Public Health 2013, 13, 756. [Google Scholar] [CrossRef] [Green Version]
- Heider, F. The Psychology of Interpersonal Relations; Wiley: New York, NY, USA, 1958. [Google Scholar]
- Kelley, H.H. The processes of causal attribution. Am. Psychol. 1973, 28, 107–128. [Google Scholar] [CrossRef]
- Weiner, B. “Spontaneous” causal thinking. Psychol. Bull. 1985, 97, 74. [Google Scholar] [CrossRef]
- Gendolla, G.H.; Koller, M. Surprise and motivation of causal search: How are they affected by outcome valence and importance? Motiv. Emot. 2001, 25, 327–349. [Google Scholar] [CrossRef]
- Ross, L. The intuitive psychologist and his shortcomings: Distortions in the attribution process. In Advances in Experimental Social Psychology; Elsevier: Amsterdam, The Netherlands, 1977; Volume 10, pp. 173–220. [Google Scholar]
- Gilbert, D.T.; Malone, P.S. The correspondence bias. Psychol. Bull. 1995, 117, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malle, B.F. The actor-observer asymmetry in attribution: A (surprising) meta-analysis. Psychol. Bull. 2006, 132, 895. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, A.L. Politics, religion, attribution theory, and attitudes toward same-sex unions. Soc. Sci. Q. 2014, 95, 701–718. [Google Scholar] [CrossRef] [Green Version]
- Haider-Markel, D.P.; Joslyn, M.R. Beliefs About the Origins of Homosexuality and Support For Gay RightsAn Empirical Test of Attribution Theory. Public Opin. Q. 2008, 72, 291–310. [Google Scholar] [CrossRef] [Green Version]
- Sakalli, N. Application of the attribution-value model of prejudice to homosexuality. J. Soc. Psychol. 2002, 142, 264–271. [Google Scholar] [CrossRef]
- Zucker, G.S.; Weiner, B. Conservatism and perceptions of poverty: An attributional analysis. J. Appl. Soc. Psychol. 1993, 23, 925–943. [Google Scholar] [CrossRef]
- Linos, K.; West, M. Self-interest, social beliefs, and attitudes to redistribution. Re-addressing the issue of cross-national variation. Eur. Sociol. Rev. 2003, 19, 393–409. [Google Scholar] [CrossRef]
- Genschow, O.; Rigoni, D.; Brass, M. Belief in free will affects causal attributions when judging others’ behavior. Proc. Natl. Acad. Sci. USA 2017, 114, 10071–10076. [Google Scholar] [CrossRef] [Green Version]
- Elischberger, H.B.; Glazier, J.J.; Hill, E.D.; Verduzco-Baker, L. “Boys don’t cry”—Or do they? Adult attitudes toward and beliefs about transgender youth. Sex Roles 2016, 75, 197–214. [Google Scholar] [CrossRef]
- Martin, J.K.; Pescosolido, B.A.; Tuch, S.A. Of fear and loathing: The role of’disturbing behavior,’labels, and causal attributions in shaping public attitudes toward people with mental illness. J. Health Soc. Behav. 2000, 208–223. [Google Scholar] [CrossRef]
- Crandall, C.; D’Anello, S.; Sakalli, N.; Lazarus, E.; Nejtardt, G.W.; Feather, N. An attribution-value model of prejudice: Anti-fat attitudes in six nations. Personal. Soc. Psychol. Bull. 2001, 27, 30–37. [Google Scholar] [CrossRef]
- Mazzocchi, M.; Cagnone, S.; Bech-Larsen, T.; Niedzwiedzka, B.; Saba, A.; Shankar, B.; Verbeke, W.; Traill, W.B. What is the public appetite for healthy eating policies? Evidence from a cross-European survey. Health Econ. Policy Law 2015, 10, 267–292. [Google Scholar] [CrossRef] [PubMed]
- Barry, C.L.; Brescoll, V.L.; Brownell, K.D.; Schlesinger, M. How beliefs about the causes of obesity affect support for public policy. Milbank Q. 2009, 87, 7–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joslyn, M.R.; Haider-Markel, D.P. Perceived causes of obesity, emotions, and attitudes about Discrimination Policy. Soc. Sci. Med. 2019, 223, 97–103. [Google Scholar] [CrossRef]
- Nimegeer, A.; Patterson, C.; Hilton, S. Media framing of childhood obesity: A content analysis of UK newspapers from 1996 to 2014. BMJ Open 2019, 9, e025646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barry, C.L.; Jarlenski, M.; Grob, R.; Schlesinger, M.; Gollust, S.E. News media framing of childhood obesity in the United States from 2000 to 2009. Pediatrics 2011, 128, 132–145. [Google Scholar] [CrossRef]
- Chiang, J.; Arons, A.; Pomeranz, J.L.; Siddiqi, A.; Hamad, R. Geographic and Longitudinal Trends in Media Framing of Obesity in the United States. Obesity 2020. [Google Scholar] [CrossRef]
- Beeken, R.J.; Wardle, J. Public beliefs about the causes of obesity and attitudes towards policy initiatives in Great Britain. Public Health Nutr. 2013, 16, 2132–2137. [Google Scholar] [CrossRef] [Green Version]
- Pearl, R.L.; Lebowitz, M.S. Beyond personal responsibility: Effects of causal attributions for overweight and obesity on weight-related beliefs, stigma, and policy support. Psychol. Health 2014, 29, 1176–1191. [Google Scholar] [CrossRef]
- Ortiz, S.E.; Zimmerman, F.J.; Adler, G.J., Jr. Increasing public support for food-industry related, obesity prevention policies: The role of a taste-engineering frame and contextualized values. Soc. Sci. Med. 2016, 156, 142–153. [Google Scholar] [CrossRef] [Green Version]
- Young, R.; Hinnant, A.; Leshner, G. Individual and social determinants of obesity in strategic health messages: Interaction with political ideology. Health Commun. 2016, 31, 903–910. [Google Scholar] [CrossRef]
- McGlynn, J.; McGlone, M.S. Desire or Disease? Framing Obesity to Influence Attributions of Responsibility and Policy Support. Health Commun. 2018, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Niederdeppe, J.; Kim, H.K.; Lundell, H.; Fazili, F.; Frazier, B. Beyond counterarguing: Simple elaboration, complex integration, and counterelaboration in response to variations in narrative focus and sidedness. J. Commun. 2012, 62, 758–777. [Google Scholar] [CrossRef]
- Garbarino, E.; Henry, P.; Kerfoot, S. Using attribution to foster public support for alternative policies to combat obesity. Eur. J. Mark. 2018, 52, 418–438. [Google Scholar] [CrossRef]
- Open Science Collaboration. Estimating the reproducibility of psychological science. Science 2015, 349, aac4716. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, J.P.; Vasiljevic, M.; Pilling, M.; Hall, M.G.; Ribisl, K.M.; Marteau, T.M. Communicating Evidence about the Causes of Obesity and Support for Obesity Policies in British and US populations: Two Population-Based Survey Experiments. 2020. Available online: https://www.researchsquare.com/article/rs-34854/v1 (accessed on 24 June 2020).
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Houts, P.S.; Doak, C.C.; Doak, L.G.; Loscalzo, M.J. The role of pictures in improving health communication: A review of research on attention, comprehension, recall, and adherence. Patient Educ. Couns. 2006, 61, 173–190. [Google Scholar] [CrossRef]
- Kirk, S.F.; Penney, T.L.; McHugh, T.L. Characterizing the obesogenic environment: The state of the evidence with directions for future research. Obes. Rev. 2010, 11, 109–117. [Google Scholar] [CrossRef]
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Allen, M.; Preiss, R.W. Comparing the persuasiveness of narrative and statistical evidence using meta-analysis. Commun. Res. Rep. 1997, 14, 125–131. [Google Scholar] [CrossRef]
- Reynolds, J.P.; Stautz, K.; Pilling, M.; van der Linden, S.; Marteau, T. Communicating the effectiveness and ineffectiveness of government policies and their impact on public support: A systematic review with meta-analysis. R. Soc. Open Sci. 2020, 7, 190522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pornpitakpan, C. The persuasiveness of source credibility: A critical review of five decades’ evidence. J. Appl. Soc. Psychol. 2004, 34, 243–281. [Google Scholar] [CrossRef]
- Smith, R.D.; Cornelsen, L.; Quirmbach, D.; Jebb, S.A.; Marteau, T.M. Are sweet snacks more sensitive to price increases than sugar-sweetened beverages: Analysis of British food purchase data. BMJ Open 2018, 8, e019788. [Google Scholar] [CrossRef]
- Hollands, G.J.; Shemilt, I.; Marteau, T.M.; Jebb, S.A.; Lewis, H.B.; Wei, Y.; Higgins, J.P.T.; Ogilvie, D. Portion, package or tableware size for changing selection and consumption of food, alcohol and tobacco. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhar, T.; Baylis, K. Fast-food consumption and the ban on advertising targeting children: The Quebec experience. J. Mark. Res. 2011, 48, 799–813. [Google Scholar] [CrossRef]
- Lambert, H.; Moy, C. Social grade allocation to the 2011 census. Retrieved Novemb. 2013, 29, 2017. [Google Scholar]
- Clarke, H.; Sanders, D.; Stewart, M.; Whiteley, P. British General Election Study, 2001; Cross-Section Survey [computer file]; UK Data Archive [distributor]: Colchester, UK, 2003. [Google Scholar]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. J. Clin. Epidemiol. 2010, 63, e1–e37. [Google Scholar] [CrossRef] [Green Version]
- Petrescu, D.C.; Hollands, G.J.; Couturier, D.L.; Ng, Y.L.; Marteau, T.M. Public Acceptability in the UK and USA of Nudging to Reduce Obesity: The Example of Reducing Sugar-Sweetened Beverages Consumption. PLoS ONE 2016, 11, e0155995. [Google Scholar] [CrossRef] [Green Version]
- Ipsos MORI. Acceptable Behaviour? Public Opinion on Behaviour Change Policy; Ipsos MORI: London, UK, 2012. [Google Scholar]
- Ejlerskov, K.T.; Sharp, S.J.; Stead, M.; Adamson, A.J.; White, M.; Adams, J. Supermarket policies on less-healthy food at checkouts: Natural experimental evaluation using interrupted time series analyses of purchases. PLoS Med. 2018, 15, e1002712. [Google Scholar] [CrossRef] [Green Version]
- Field, A. Discovering Statistics Using IBM SPSS Statistics; SAGE: London, UK, 2014. [Google Scholar]
- Lakens, D.; Scheel, A.M.; Isager, P.M. Equivalence testing for psychological research: A tutorial. Adv. Methods Pract. Psychol. Sci. 2018, 1, 259–269. [Google Scholar] [CrossRef] [Green Version]
- Lakens, D. Equivalence tests: A practical primer for t tests, correlations, and meta-analyses. Soc. Psychol. Personal. Sci. 2017, 8, 355–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, M.H.; van der Linden, S.; Ballew, M.T.; Rosenthal, S.A.; Gustafson, A.; Leiserowitz, A. The Experience of Consensus: Video as an Effective Medium to Communicate Scientific Agreement on Climate Change. Sci. Commun. 2019, 41, 659–673. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Support for Obesity Prevention Policies (n = 1680) | Causal Beliefs (Obesity): Environment (n = 1680) | Causal Beliefs (Human Behaviour): Environment (n = 1680) | |||
|---|---|---|---|---|---|---|
| B [95% CIs] | p | B [95% CIs] | p | B [95% CIs] | p | |
| Age | 0.01 [0.00, 0.01] | 0.003 * | 0.00 [−0.01, 0.00] | 0.465 | 0.00 [−0.01, 0.00] | < 0.001 * |
| Gender | ||||||
| Male (ref.) | ||||||
| Female | 0.44 [0.27, 0.61] | < 0.001 * | 0.08 [−0.05, 0.20] | 0.236 | 0.10 [0.01, 0.18] | 0.023 |
| SES | ||||||
| DE (ref.) | ||||||
| C1C2 | 0.37 [0.15, 0.59] | 0.001 * | 0.23 [0.07, 0.39] | 0.006 * | 0.20 [0.09, 0.31] | < 0.001 * |
| AB | 0.51 [0.26, 0.76] | < 0.001 * | 0.26 [0.07, 0.44] | 0.007 * | 0.27 [0.15, 0.39] | < 0.001 * |
| Education | ||||||
| Low (ref) | ||||||
| Medium | 0.06 [−0.15, 0.27] | 0.571 | −0.03 [−0.19, 0.13] | 0.704 | 0.21 [0.10, 0.31] | < 0.001 * |
| High | 0.17 [−0.07, 0.41] | 0.161 | 0.07 [−0.11, 0.25] | 0.432 | 0.35 [0.23, 0.46] | < 0.001 * |
| Region | ||||||
| London (ref) | ||||||
| North East | 0.04 [−0.44, 0.51] | 0.883 | −0.08 [−0.43, 0.27] | 0.667 | 0.11 [−0.12, 0.35] | 0.346 |
| North West | −0.14 [−0.49, 0.22] | 0.451 | −0.14 [−0.41, 0.12] | 0.282 | −0.08 [−0.25, 0.09] | 0.376 |
| Yorkshire & Humb. | 0.16 [−0.20, 0.52] | 0.376 | −0.23 [−0.49, 0.04] | 0.094 | −0.01 [−0.19, 0.16] | 0.874 |
| East Midlands | −0.04 [−0.43, 0.36] | 0.852 | −0.01 [−0.30, 0.28] | 0.938 | 0.05 [−0.14, 0.24] | 0.604 |
| West Midlands | 0.01 [−0.35, 0.37] | 0.964 | −0.18 [−0.45, 0.09] | 0.183 | −0.13 [−0.30, 0.05] | 0.160 |
| East of England | 0.13 [−0.25, 0.50] | 0.510 | −0.15 [−0.42, 0.13] | 0.294 | −0.10 [−0.29, 0.08] | 0.261 |
| South East | −0.10 [−0.43, 0.24] | 0.564 | −0.15 [−0.39, 0.10] | 0.248 | −0.12 [−0.28, 0.05] | 0.165 |
| South West | −0.03 [−0.38, 0.32] | 0.856 | −0.18 [−0.44, 0.08] | 0.167 | 0.13 [−0.04, 0.31] | 0.121 |
| Wales | −0.06 [−0.51, 0.39] | 0.785 | −0.18 [−0.51, 0.15] | 0.288 | −0.12 [−0.34, 0.10] | 0.294 |
| Scotland | −0.33 [−0.70, 0.04] | 0.079 | −0.47 [−0.75, −0.20] | 0.001 * | −0.21 [−0.39, −0.02] | 0.028 |
| Group | ||||||
| Control (ref) | ||||||
| Obesity message (a) | 0.08 [−0.19, 0.35] | 0.559 | −0.01 [−0.21, 0.19] | 0.922 | 0.18 [0.04, 0.31] | 0.009 * |
| Obesity message (b) | −0.14 [−0.41, 0.13] | 0.314 | −0.27 [−0.47, −0.07] | 0.007 * | −0.03 [−0.16, 0.10] | 0.669 |
| Behavioural message (a) | −0.04 [−0.31, 0.22] | 0.756 | −0.09 [−0.29, 0.10] | 0.345 | 0.05 [−0.08, 0.18] | 0.482 |
| Behavioural message (b) | 0.04 [−0.23, 0.30] | 0.783 | −0.02 [−0.21, 0.17] | 0.829 | 0.10 [−0.03, 0.22] | 0.138 |
| Group | Study 1 | Study 2 |
|---|---|---|
| Group 1 | Control (no message) | Control (no message) |
| Group 2 | Obesity message (a) + images | Obesity message (a) (no image) |
| Group 3 | Obesity message (b) + images | Obesity message (c) (no image) |
| Group 4 | Behaviour message (a) + images | |
| Group 5 | Behaviour message (b) + images |
| Variables | Support for Encouraging Policies (n = 2544) | Support for Discouraging Policies (n = 2586) | ||
|---|---|---|---|---|
| B [95% CIs] | p | B [95% CIs] | p | |
| Age | 0.00 [0.00, 0.00] | 0.728 | 0.00 [0.00, 0.00] | 0.590 |
| Gender | ||||
| Male (ref) | ||||
| Female | 0.23 [0.16, 0.30] | < 0.001 * | 0.26 [0.19, 0.34] | < 0.001 * |
| Group | ||||
| Control (ref) | ||||
| Obesity (a) | 0.05 [−0.03, 0.14] | 0.215 | −0.01 [−0.10, 0.08] | 0.823 |
| Obesity (c) | 0.06 [−0.03, 0.14] | 0.171 | −0.02 [−0.10, 0.07] | 0.723 |
| Country | ||||
| England (ref) | ||||
| USA | −0.15 [−0.22, −0.08] | < 0.001 * | −0.46 [−0.54, −0.39] | < 0.001 * |
| Variables | Causal Beliefs: Environment (n = 2711) | Causal Beliefs: Genetics (n = 2711) | Causal Beliefs: Willpower (n = 2711) | |||
|---|---|---|---|---|---|---|
| B [95% CI] | p | B [95% CI] | p | B [95% CI] | p | |
| Age | −0.01 [−0.01, −0.01] | < 0.001 * | 0.00 [0.00, 0.00] | 0.317 | 0.00 [0.00, 0.01] | 0.143 |
| Gender | ||||||
| Male (ref) | ||||||
| Female | 0.27 [0.15, 0.38] | < 0.001 * | 0.11 [0.01, 0.21] | 0.034 | −0.33 [−0.45, −0.22] | < 0.001 * |
| Group | ||||||
| Control (ref) | ||||||
| Obesity (a) | −0.12 [−0.26, 0.02] | 0.087 | −0.04 [−0.16, 0.08] | 0.519 | 0.11 [−0.03, 0.24] | 0.120 |
| Obesity (c) | −0.14 [−0.28, 0.00] | 0.053 | 0.00 [−0.12, 0.13] | 0.956 | 0.07 [−0.07, 0.20] | 0.331 |
| Country | ||||||
| England (ref) | ||||||
| USA | −0.15 [−0.26, −0.03] | 0.011 | 0.61 [0.51, 0.71] | < 0.001 * | −0.22 [−0.33, −0.11] | < 0.001 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reynolds, J.P.; Vasiljevic, M.; Pilling, M.; Hall, M.G.; Ribisl, K.M.; Marteau, T.M. Communicating Evidence about the Causes of Obesity and Support for Obesity Policies: Two Population-Based Survey Experiments. Int. J. Environ. Res. Public Health 2020, 17, 6539. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186539
Reynolds JP, Vasiljevic M, Pilling M, Hall MG, Ribisl KM, Marteau TM. Communicating Evidence about the Causes of Obesity and Support for Obesity Policies: Two Population-Based Survey Experiments. International Journal of Environmental Research and Public Health. 2020; 17(18):6539. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186539
Chicago/Turabian StyleReynolds, James P., Milica Vasiljevic, Mark Pilling, Marissa G. Hall, Kurt M. Ribisl, and Theresa M. Marteau. 2020. "Communicating Evidence about the Causes of Obesity and Support for Obesity Policies: Two Population-Based Survey Experiments" International Journal of Environmental Research and Public Health 17, no. 18: 6539. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186539