Pregnancy in Patients with Type One Diabetes Mellitus Treated with Continuous Subcutaneous Insulin Infusion—Preconception Basal Insulin Dose as a Potential Risk Factor for Fetal Overgrowth?


Abstract
:1. Introduction
2. Patients and Methods
3. Statistical Analysis
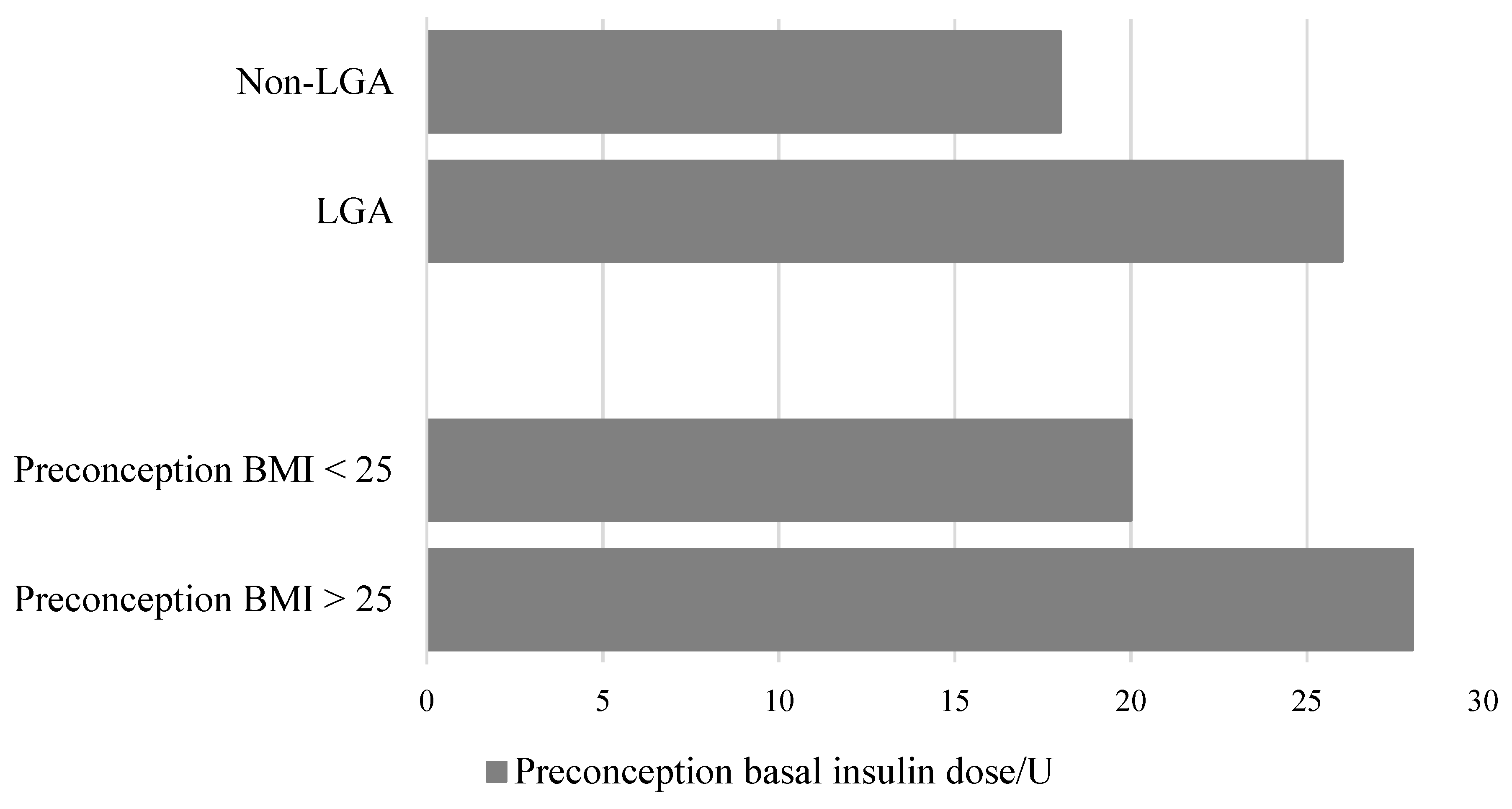
4. Results
5. Discussion
6. Conclusions
7. Ethics Statements
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Feldman, A.Z.; Brown, F.M. Management of Type I Diabetes in Pregnancy. Curr. Diab. Rep. 2016, 16, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baack, M.L.; Wang, C.; Hu, S.; Segar, J.L.; Norris, A.W. Hyperglycemia Induces Embryopathy, Even in the Absence of Systemic Maternal Diabetes: An in Vivo Test of the Fuel Mediated Teratogenesis Hypothesis. Reprod. Toxicol. 2014, 46, 129–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polsky, S.; Wu, M.; Bode, B.W.; DuBose, S.N.; Goland, R.S.; Maahs, D.M.; Foster, N.C.; Peters, A.L.; Levy, C.J.; Shah, V.N.; et al. Diabetes Technology Use Among Pregnant and Nonpregnant Women with T1D in the T1D Exchange. Diabetes Technol. Ther. 2018, 20, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Beck, R.W.; Bergenstal, R.M.; Laffel, L.M.; Pickup, J.C. Advances in technology for management of type 1 diabetes. Lancet 2019, 394, 1265–1273. [Google Scholar] [CrossRef]
- Roeder, H.A.; Moore, T.R.; Ramos, G.A. Insulin pump dosing across gestation in women with well-controlled type 1 diabetes mellitus. Am. J. Obstet. Gynecol. 2012, 207, 324. [Google Scholar] [CrossRef] [PubMed]
- Jensen, D.M.; Damm, P.; Moelsted-Pedersen, L.; Ovesen, P.; Westergaard, J.G.; Moeller, M.; Beck-Nielsen, H. Outcomes in Type 1 Diabetic Pregnancies. A nationwide, population-based study. Diabetes Care 2004, 27, 2819–2823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owens, L.A.; Egan, A.M.; Carmody, L.; Dunne, F. Ten years of optimizing outcomes for women with type 1 and type 2 diabetes in pregnancy-the Atlantic DIP experience. J. Clin. Endocrinol. Metab. 2016, 101, 1598–1605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, Y.; Xu, Q.; Yang, H.; Yang, Y.; Wang, L.; Chen, H.; Anderson, C.; Liu, X.; Song, G.; Li, Q.; et al. Preconception diabetes mellitus and adverse pregnancy outcomes in over 6.4 million women: A population-based cohort study in China. PLoS Med. 2019, 16, e1002926. [Google Scholar] [CrossRef] [PubMed]
- Colstrup, M.; Mathiesen, E.R.; Damm, P.; Jensen, D.M.; Ringholm, L. Pregnancy in women with type 1 diabetes: Have the goals of st. Vincent declaration been met concerning foetal and neonatal complications? J. Matern. Fetal Neonatal Med. 2013, 26, 1682–1686. [Google Scholar] [CrossRef] [PubMed]
- Morrens, A.; Verhaeghe, J.; Vanhole, C.; Devlieger, R.; Mathieu, C.; Benhalima, K. Risk factors for large-for-gestational age infants in pregnant women with type 1 diabetes. BMC Pregnancy Childbirth 2016, 16, 162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulla, B.M.; Noor, N.; James-Todd, T.; Isganaitis, E.; Takoudes, T.C.; Curan, A.; Warren, C.E.; O’Brien, K.E.; Brown, F.M. Continuous Glucose Monitoring, Glycemic Variability, and Excessive Fetal Growth in Pregnancies Complicated by Type 1 Diabetes. Diabetes Technol. Ther. 2018, 20, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Sacks, D.A.; Liu, A.I.; Wolde-Tsadik, G.; Amini, S.B.; Huston-Presley, L.; Catalano, P.M. What proportion of birth weight is attributable to maternal glucose among infants of diabetic woman? Am. J. Obstet. Gynecol. 2006, 194, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Desove, G.; Nolan, C.J. The fetal glucose steal: An underappreciated phenomenon in diabetic pregnancy. Diabetologia 2016, 59, 1089–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, N.; Robker, R.L. Developmental programming of obesity and insulin resistance: Does mitochondrial dysfunction in oocytes play a role? Mol. Hum. Reprod. 2015, 21, 23–30. [Google Scholar] [CrossRef] [PubMed]
- McGrath, R.T.; Glastras, S.J.; Hocking, S.L.; Fulcher, G.R. Large-for-Gestational-Age Neonates in Type 1 Diabetes and Pregnancy: Contribution of Factors Beyond Hyperglycemia. Diabetes Care 2018, 41, 1821–1828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuroda, A.; Kaneto, H.; Yasuda, T.; Matsuhisa, M.; Miyashita, K.; Fujiki, N.; Fujisawa, K.; Yamamoto, T.; Takahara, M.; Sakamoto, F.; et al. Basal Insulin Requirement is ~30% of the Total daily Insulin Dose in Type 1 Diabetic Patients Who Use the Insulin Pump. Diabetes Care 2011, 34, 1089–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, A.B. How much do I give? Reevaluation of insulin dosing estimation formulas using continuous glucose monitoring. Endocr. Pract. 2010, 16, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Deeb, A.; Abu-Awad, S.; Tomy, M.; Suliman, S.; Mustafa, H. Relationship Between Basal Insulin Requirement and Body Mass Index in Children and Adults with Type 1 Diabetes on Insulin Pump Therapy. J. Diabetes Sci. Technol. 2015, 9, 711–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musulin, J.; Baretic, M.; Simegi-Dekic, V. Assesment of body composition of patients with type 1 diabetes by bioelectrical impendance analysis. Lijec. Vjesn. 2017, 139, 280–285. [Google Scholar]
- Jensen, D.M.; Damm, P.; Sørensen, B.; Molsted-Pedersen, L.; Westergaard, J.G.; Beck-Nielsen, H. Pregnancy outcome and prepregnancy body mass index in 2459 glucose-tolerant Danish women. Am. J. Obstet. Gynecol. 2003, 189, 239–244. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Preconception Characteristics | |
|---|---|
| A1C/% | 6.3 ± 0.8 |
| A1C/mmol/mol | 45 ± 0.8 |
| TDD/units | 40.3 ± 16.4 |
| Basal insulin/IU | 21.9 ± 9.4 |
| Bolus insulin/IU | 18.3 ± 8.6 |
| Basal insulin/percentage | 55 ± 9 |
| Bolus insulin/percentage | 45 ± 9 |
| Body weight/kg | 65.4 ± 8.1 |
| BMI/kg/m2 | 24 ± 3 |
| Pregnancy Outcomes | |
|---|---|
| Gestational weight gain/kg | 12 ± 3 |
| Birth weight/g, birth length/cm | 3571 ± 695, 50 ± 2 |
| Week of delivery and Apgar score | 38 ± 1, 10 ± 1 |
| LGA prevalence/% | 46 (16/35) |
| Macrosomia prevalence/% | 28 (10/35) |
| Neonatal hypoglycaemia/% | 6 (2/35) |
| Preconception | p | r |
|---|---|---|
| A1C | 0.04 | 0.3 |
| Basal insulin dose/IU | 0.01 | 0.4 |
| Bolus insulin dose/IU | 0.08 | 0.3 |
| BMI/kg/m2 | 0.60 | 0.1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lekšić, G.; Baretić, M.; Ivanišević, M.; Jurišić-Eržen, D. Pregnancy in Patients with Type One Diabetes Mellitus Treated with Continuous Subcutaneous Insulin Infusion—Preconception Basal Insulin Dose as a Potential Risk Factor for Fetal Overgrowth? Int. J. Environ. Res. Public Health 2020, 17, 6566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186566
Lekšić G, Baretić M, Ivanišević M, Jurišić-Eržen D. Pregnancy in Patients with Type One Diabetes Mellitus Treated with Continuous Subcutaneous Insulin Infusion—Preconception Basal Insulin Dose as a Potential Risk Factor for Fetal Overgrowth? International Journal of Environmental Research and Public Health. 2020; 17(18):6566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186566
Chicago/Turabian StyleLekšić, Gloria, Maja Baretić, Marina Ivanišević, and Dubravka Jurišić-Eržen. 2020. "Pregnancy in Patients with Type One Diabetes Mellitus Treated with Continuous Subcutaneous Insulin Infusion—Preconception Basal Insulin Dose as a Potential Risk Factor for Fetal Overgrowth?" International Journal of Environmental Research and Public Health 17, no. 18: 6566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186566