Positive and Negative Impacts of Caring among Adolescents Caring for Grandparents. Results from an Online Survey in Six European Countries and Implications for Future Research, Policy and Practice

 , ,
, ,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
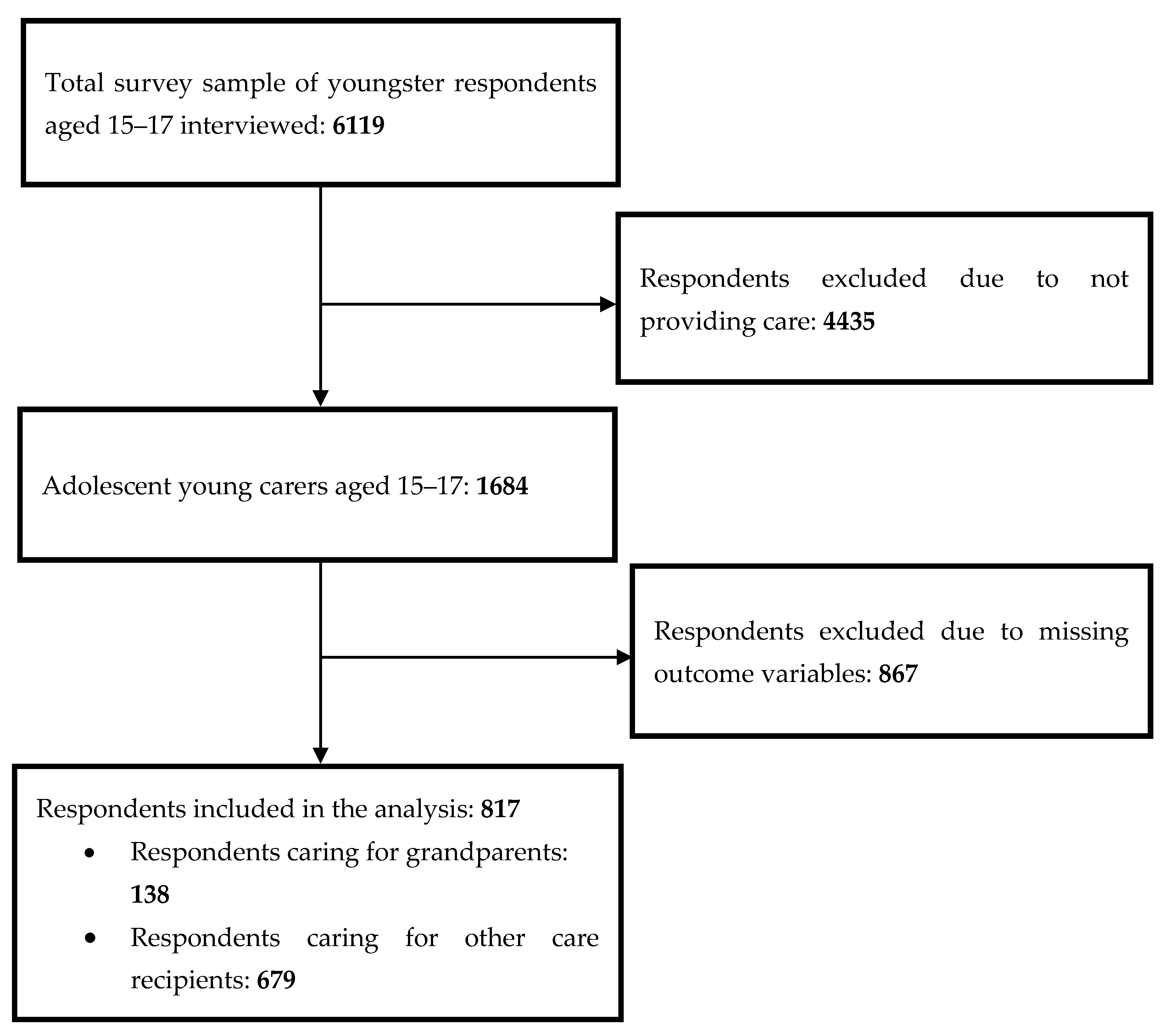
2.1. Participants’ Inclusion Criteria and Recruitment Strategies
2.2. Data Collection Procedure
2.3. Ethics
2.4. Measures
2.5. Data Analysis
3. Results
3.1. Is There Any Difference in Positive and Negative Outcomes of Caregiving between AYCs of GrPs and AYCs of OCRs?
3.2. Which Are the Exposure Factors to Positive and Negative Caregiving Outcomes and Health Problems among AYCs of GrPs, in Comparison to AYCs of OCRs?
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Triantafillou, J.; Naiditch, M.; Repkova, K.; Stiehr, K.; Carretero, S.; Emilsson, T.; Di Santo, P.; Bednarik, R.; Brichtova, L.; Ceruzzi, F.; et al. Informal Care in the Long-Term Care System. European Overview Paper. 2010. Available online: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.572.1803&rep=rep1&type=pdf (accessed on 5 March 2020).
- Verbakel, E.; Metzelthin, S.F.; Kempen, G.I. Caregiving to older adults: Determinants of informal caregivers’ subjective well-being and formal and informal support as alleviating conditions. J. Gerontol. B Psychol. Sci. Soc. Sci. 2018, 73, 1099–1111. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Informal Care in Europe. Exploring Formalization, Availability and Quality; Report, 2018; European Commission: Brussels, Belgium, 2018; Available online: https://ec.europa.eu/social/main.jsp?catId=738&langId=en&pubId=8106&furtherPubs=yes (accessed on 27 October 2019).
- Ferrant, G.; Pesando, M.C.; Nowacka, K. Unpaid Care Work: The Missing Link in the Analysis of Gender Gaps in Labour Outcomes; OECD Development Centre: Paris, France, 2014; Available online: https://www.oecd.org/dev/development-gender/Unpaid_care_work.pdf (accessed on 8 April 2020).
- Aldridge, J.; Becker, S. Children Who Care: Inside the World of Young Carers; Loughborough University: Loughborough, UK, 1993. [Google Scholar]
- Becker, S. Young carers. In The Blackwell Encyclopedia of Social Work; Davies, M., Ed.; Blackwell: Oxford, UK, 2000; p. 378. [Google Scholar]
- Joseph, S.; Sempik, J.; Leu, A.; Becker, S. Young carers research, practice and policy: An overview and critical perspective on possible future directions. Adolesc. Res. Rev. 2020, 5, 77–89. [Google Scholar] [CrossRef] [Green Version]
- Teipel, K. Understanding Adolescence Seeing Through a Developmental Lens; University of Minnesota, Konopka Institute, State Adolescent Health Resource Center: Minneapolis, MN, USA, 2013. [Google Scholar]
- Brimblecombe, N.; Pickard, L.; King, D.; Knapp, M. Perceptions of unmet needs for community social care services in England. A comparison of working carers and the people they care for. Health Soc. Care Community 2017, 25, 435–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutherford, A.; Bu, F. Issues with the measurement of informal care in social surveys: Evidence from the English longitudinal study of ageing. Ageing Soc. 2018, 38, 2541–2559. [Google Scholar] [CrossRef] [Green Version]
- Aldridge, J. Where are we now? Twenty-five years of research, policy and practice on young carers. Crit. Soc. Policy 2018, 38, 155–165. [Google Scholar] [CrossRef] [Green Version]
- Leu, A.; Becker, S. Young carers. In Oxford Bibliographies in Childhood Studies; Montgomery, H., Ed.; Oxford University Press: New York, NY, USA, 2019; Available online: https://www.oxfordbibliographies.com/view/document/obo-9780199791231/obo-9780199791231-0120.xml (accessed on 22 April 2020).
- Leu, A.; Becker, S. A cross-national and comparative classification of in-country awareness and policy responses to ‘young carers’. J. Youth Stud. 2017, 20, 750–762. [Google Scholar] [CrossRef] [Green Version]
- Leu, A.; Frech, M.; Wepf, H.; Sempik, J.; Joseph, S.; Helbling, L.; Moser, U.; Becker, S.; Jung, C. Counting young carers in Switzerland: A study of prevalence. Child. Soc. 2019, 33, 53–67. [Google Scholar] [CrossRef]
- Evans, R.; Becker, S. Children Caring for Parents with HIV and AIDS: Global Issues and Policy Responses; Policy Press: Bristol, UK, 2009. [Google Scholar]
- Nagl-Cupal, M.; Daniel, M.; Koller, M.M.; Mayer, H. Prevalence and effects of caregiving on children. J. Adv. Nurs. 2014, 70, 2314–2325. [Google Scholar] [CrossRef]
- Dellmann-Jenkins, M.; Brittain, L. Young adults’ attitudes toward filial responsibility and actual assistance to elderly family members. J. Appl. Gerontol. 2003, 22, 214–229. [Google Scholar] [CrossRef]
- Orel, N.A.; Dupuy, P. Grandchildren as auxiliary caregivers for grandparents with cognitive and/or physical limitations: Coping strategies and ramifications. Child. Study J. 2002, 32, 193–213. [Google Scholar]
- Piercy, K.W.; Chapman, J.G. Adopting the caregiver role: A family legacy. Fam. Relat. 2001, 50, 386–393. [Google Scholar] [CrossRef]
- Brody, E. Women in the Middle: Their Parent-Care Years; Springer: New York, NY, USA, 1990. [Google Scholar]
- Townsend, A.L.; Franks, M.M. Quality of the relationship between elderly spouses: Influence on spouse caregivers’ subjective effectiveness. Fam. Relat. 1997, 46, 33–39. [Google Scholar] [CrossRef]
- Dilworth-Anderson, P.; Williams, S.W.; Cooper, T. Family caregivers to elderly African Americans: Caregiver types and structures. J. Gerontol. B Psychol. Sci. Soc. Sci. 1999, 54, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Dellmann-Jenkins, M.; Blankemeyer, M.; Pinkard, O. Incorporating the elder caregiving role into the developmental tasks of young adulthood. Int. J. Aging Hum. Dev. 2001, 52, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Hamill, S.B. Caring for grandparent with Alzheimer’s disease: Help from “forgotten” generation. J. Fam. Issues 2012, 33, 1195–1217. [Google Scholar] [CrossRef]
- Orel, N.A.; Dupuy, P.; Wright, J. Auxiliary Caregivers: The perception of grandchildren within multigenerational caregiving environments. J. Intergener. Relatsh. 2004, 2, 67–92. [Google Scholar] [CrossRef]
- Schumacher, A.; Willems, H. Caring for the elderly. Effects on family and adolescents. In Cultures of Care; Boll, T., Ferring, D., Valsiner, J., Eds.; Information Age Publishing Inc.: Charlotte, NC, USA, 2018; Chapter 5; pp. 99–122. [Google Scholar]
- Szinovacz, M.E. Caring for a demented relative at home: Effects on parent-adolescent relationship and family dynamics. J. Aging Stud. 2003, 17, 445–472. [Google Scholar] [CrossRef]
- Goodnow, J.J.; Lawrence, J.A. Work contribution to the family: Developing a conceptual and research framework. In Family Obligation and Assistance During Adolescence; Fuligni, A.J., Ed.; Jossey-Bass: San Francisco, CA, USA, 2001; pp. 5–22. [Google Scholar]
- Blanton, P.W. Family caregiving to frail elders: Experiences of young adult grandchildren a as auxiliary caregivers. J. Intergener. Relatsh. 2013, 11, 18–31. [Google Scholar] [CrossRef]
- Joseph, S.; Becker, S.; Becker, F. Manual for Measures of Caring Activities and Outcomes for Children and Young People; Princess Royal Trust for Carers: London, UK, 2009. [Google Scholar]
- Svanberg, E.; Stott, J.; Spector, A. ‘Just helping’: Children living with a parent with young onset dementia. Aging Ment. Health 2010, 14, 740–751. [Google Scholar] [CrossRef]
- Cassidy, T.; Giles, M.; McLaughlin, M. Benefit finding and resilience in child caregivers. Br. J. Health Psychol. 2014, 19, 606–618. [Google Scholar] [CrossRef]
- Fives, A.; Kennan, D.; Canavan, J.; Brady, B. Why we still need the term ‘young carer’: Findings from an exploratory study of young carers in Ireland. Crit. Soc. Work 2013, 14, 49–61. [Google Scholar]
- Stamatopoulos, V. The young carer penalty: Exploring the costs of caregiving among a sample of Canadian youth. Child. Youth Serv. 2018, 39, 180–205. [Google Scholar] [CrossRef]
- Fruhauf, C.A.; Orel, N.A. Developmental issues of grandchildren who provide care to grandparents. Int. J. Aging Hum. Dev. 2008, 67, 209–230. [Google Scholar] [CrossRef]
- Fruhauf, C.A.; Jarrott, S.E.; Allen, K.R. Grandchildren’s perceptions of caring for grandparents. J. Fam. Issues 2006, 27, 887–911. [Google Scholar] [CrossRef] [Green Version]
- Hooper, L.M.; L’Abate, L.; Sweeney, L.G.; Gianesini, G.; Jankowski, P.J. (Eds.) Parentification. In Models of Psychopathology; Springer: New York, NY, USA, 2014; pp. 37–54. [Google Scholar]
- Carers Trust. Invisible and in Distress: Prioritising the Mental Health of England’s Young Carers; Report; Carers Trust: London, UK, 2016; Available online: https://carers.org/sites/default/files/invisibleandindistress_report.pdf (accessed on 15 February 2020).
- Aldridge, J.; Becker, S. Children Caring for Parents with Mental Illness: Perspectives of Young Carers, Parents and Professionals; Policy Press: Bristol, UK, 2003. [Google Scholar]
- Hamilton, M.G.; Adamson, E. Bounded agency in young carers’ lifecourse-stage domains and transitions. J. Youth Stud. 2013, 16, 101–117. [Google Scholar] [CrossRef]
- Cohen, C.; Greene, J.; Toyinbo, P.; Siskowsky, R.N. Impact of family caregiving by youth on their psychological well-being: A latent trait analysis. J. Behav. Health Serv. Res. 2012, 39, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Doran, T.; Drever, T.; Whitehead, M. Health of young and elderly carers: An analysis of UK census data. BMJ 2003, 327, 1388. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, S.; Schulze, G.C. Between inclusion and participation: Young carers who are absent from school. JCEP 2015, 14, 314–328. [Google Scholar] [CrossRef]
- Kettell, L. Young adult carers in higher education: The motivations, barriers and challenges involved—A UK study. JFHE 2018, 44, 100–112. [Google Scholar] [CrossRef]
- Bolas, H.; Wersch, A.V.; Flynn, D. The well-being of young people who care for a dependent relative: An interpretative phenomenological analysis. Psychol. Health 2007, 22, 829–850. [Google Scholar] [CrossRef]
- Phillips, D.; Paul, G.; Fahy, M.; Dowling-Hetherington, L.; Kroll, T.; Moloney, B.; Duffy, C.; Fealy, G.; Lafferty, A. The invisible workforce during the COVID-19 pandemic: Family carers at the frontline. HRB Open Res. 2020, 3, 24. [Google Scholar] [CrossRef]
- Carers Trust Scotland. 2020 Vision: Hear Me, See Me, Support Me and Don’t Forget Me; Report; Carers Trust Scotland: Glasgow, UK, 2020; Available online: https://carers.org/downloads/scotland-pdfs/2020-vision.pdf (accessed on 23 July 2020).
- Kavanaugh, M.S.; Stamatopoulos, V.; Cohen, D.; Zhang, L. Unacknowledged caregivers: A scoping review of research on caregiving youth in the United States. Adolesc. Res. Rev. 2016, 1, 29–49. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. World medical association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regulation, G.D.P. Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data, and repealing Directive 95/46/EC (General Data Protection Regulation). Off. J. Eur. Union 2016, 59, 294. [Google Scholar]
- Ravens-Sieberer, U.; Erhart, M.; Rajmil, L.; Herdman, M.; Auquier, P.; Bruil, J.; Power, M.; Duer, W.; Abel, T.; Czemy, L.; et al. Reliability, construct and criterion validity of the KIDSCREEN-10 score: A short measure for children and adolescents’ well-being and health-related quality of life. Qual. Life Res. 2010, 19, 1487–1500. [Google Scholar] [CrossRef] [Green Version]
- Ravens-Sieberer, U.; Herdman, M.; Devine, J.; Otto, C.; Bullinger, M.; Rose, M.; Klasen, F. The European KIDSCREEN approach to measure quality of life and well-being in children: Development, current application, and future advances. Qual. Life Res. 2014, 23, 791–803. [Google Scholar] [CrossRef] [Green Version]
- León, M.; Pavolini, E. ‘Social investment’ or back to ‘familism’: The impact of the economic crisis on family and care policies in Italy and Spain. South. Eur. Soc. Polit. 2014, 19, 353–369. [Google Scholar] [CrossRef]
- Hlebec, V.; Rakar, T. Ageing policies in Slovenia: Before and after austerity. In Selected Contemporary Challenges of Ageing Policy; Tomczyk, Ł., Klimczuk, A., Eds.; Uniwersytet pedagogiczny w Krakowie: Krakow, Poland, 2017; pp. 27–51. [Google Scholar]
- Boehmer, U.; Clark, M.A.; Heeren, T.C.; Showalter, E.A.; Fredman, L. Differences in caregiving outcomes and experiences by sexual orientation and gender identity. LGBT Health 2018, 5, 112–120. [Google Scholar] [CrossRef]
- Thomas, N.; Stainton, T.; Jackson, S.; Cheung, W.Y.; Doubtfire, S.; Webb, A. ‘Your friends don’t understand’: Invisibility and unmet need in the lives of ‘young carers’. Child. Fam. Soc. Work 2003, 8, 35–46. [Google Scholar] [CrossRef]
- Pelle, J. Young carers from black and minority ethnic community. In Child and Adolescent Mental Health: Theory and Practice; Hooper, C., Thompson, M., Laver-Bradbury, C., Gale, C., Eds.; Taylor&Francis: Boca Raton, FL, USA, 2012; pp. 351–356. [Google Scholar]
- James, E. Caring Alone. Why Black, Asia and Minority Ethnic Continue to Struggle to Access Support. Report. 2019. Available online: https://www.batod.org.uk/wp-content/uploads/2019/05/caring_alone_report.pdf (accessed on 15 March 2020).
- Becker, S. Defining young carers in different national contexts. In Young Carers in Europe. An Exploratory Cross-National Study in Britain, France, Sweden and Germany; Becker, S., Ed.; Department of Social Sciences Loughborough University: Loughborough, UK, 1995; Available online: http://www.ycrg.org.uk/youngCarersDownload/Young%20Carers%20in%20Europe1.pdf (accessed on 12 May 2020).
- Evans, B.C.; Coon, D.W.; Belyea, M.J.; Ume, E. Collective care: Multiple caregivers and multiple care recipients in Mexican American families. J. Transcult. Nur. 2017, 28, 398–407. [Google Scholar] [CrossRef]
- Quinn, C.; Jones, I.R.; Clare, L. Illness representations in caregivers of people with dementia. Aging Ment. Health 2017, 21, 553–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del-Pino-Casado, R.; Millán-Cobo, M.D.; Palomino-Moral, P.A.; Frías-Osuna, A. Cultural correlates of burden in primary caregivers of older relatives: A cross-sectional study. J. Nurs. Sch. 2014, 46, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Regnier, F.; Le Bihan, E.; Tichit, C.; Baumann, M. Adolescent body dissatisfaction in contrasting socioeconomic milieus, coming from a French and Luxembourgish context. Int. J. Environ. Res. Public Health 2019, 17, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Roit, B.; van Bochove, M. Migrant care work going Dutch? The emergence of a live-in migrant care market and the restructuring of the Dutch long-term care system. Soc. Policy. Adm 2017, 51, 76–94. [Google Scholar] [CrossRef]
- Di Rosa, M.; Barbabella, F.; Poli, A.; Santini, S.; Lamura, G. Migrant care workers in Italian households: Recent trends and future perspectives. In The Routledge Handbook of Social Care Work Around the World; Christensen, K., Pilling, D., Eds.; Routledge: Oxford, UK, 2018; pp. 142–155. [Google Scholar]
- Van Hooren, F. Varieties of migrant care work: Comparing patterns of migrant labour in social care. J. Eur. Soc. Policy 2012, 22, 133–147. [Google Scholar] [CrossRef]
- Williams, F. Converging variations in migrant care work in Europe. J. Eur. Soc. Policy 2012, 22, 363–373. [Google Scholar] [CrossRef]
- Fellmeth, G.; Rose-Clarke, K.; Zhao, C.; Busert, L.K.; Zheng, Y.; Massazza, A.; Sonmez, H.; Eder, B.; Blewitt, A.; Lertgrai, W.; et al. Health impacts of parental migration on left-behind children and adolescents: A systematic review and meta-analysis. Lancet 2018, 392, 2567–2582. [Google Scholar] [CrossRef] [Green Version]
- UN General Assembly. Convention on the Rights of the Child; Treaty Series; United Nation: New York, NY, USA, 1989; Volume 1577, p. 3. Available online: https://www.refworld.org/docid/3ae6b38f0.html (accessed on 27 July 2020).
- European Commission. Active Ageing Report. Special Eurobarometer 378; Report; European Commission: Brussels, Belgium, 2012; Available online: https://ec.europa.eu/commfrontoffice/publicopinion/archives/ebs/ebs_378_en.pdf (accessed on 8 April 2020).
- Santini, S.; Tombolesi, V.; Baschiera, B.; Lamura, G. Intergenerational programs involving adolescents, institutionalized elderly, and older volunteers: Results from a pilot research-action in Italy. Biomed. Res. Int. 2018, 2018, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Fast, J.; Keating, N.; Eales, J.; Kim, C.; Lee, Y. Trajectories of family care over the lifecourse: Evidence from Canada. Ageing Soc. 2020, 1–18, Published online on 8 January 2020. Available online: https://www.researchgate.net/publication/338457889_Trajectories_of_family_care_over_the_lifecourse_evidence_from_Canada (accessed on 25 April 2020). [CrossRef] [Green Version]


{kind=link}
| AYCs | p | |||
|---|---|---|---|---|
| Total | OCRs | GrPs | ||
| 817 (100%) | 679 (83.1%) | 138 (16.9%) | ||
| Gender | 0.536 | |||
| Male | 202 (24.7%) | 173 (25.5%) | 29 (21.0%) | |
| Female | 591 (72.4%) | 486 (71.5%) | 105 (76.1%) | |
| Transgender/non-binary | 24 (2.9%) | 20 (3.0%) | 4 (2.9%) | |
| Age | 0.104 | |||
| 15 | 104 (12.7%) | 94 (13.8%) | 10 (7.2%) | |
| 16 | 361 (44.2%) | 297 (43.8%) | 64 (46.4%) | |
| 17 | 352 (43.1%) | 288 (42.4%) | 64 (46.4%) | |
| Country of birth % | 0.631 | |||
| National | 752 (92.5%) | 623 (92.3%) | 129 (93.5%) | |
| Abroad | 61 (7.5%) | 52 (7.7%) | 9 (6.5%) | |
| Formal support services received by AYCs’ family | 0.005 | |||
| No | 394 (49.1%) | 310 (46.6%) | 84 (61.8%) | |
| Yes | 296 (36.9%) | 260 (39.0%) | 36 (26.5%) | |
| I do not know | 112 (14.0%) | 96 (14.4%) | 16 (11.8%) | |
| Hours a day spent providing care | 3.9 ± 5.0 | 4.0 ± 5.2 | 2.9 ± 3.6 | 0.014 |
| Country of residence | ||||
| CH | 40 (4.9%) | 31 (4.6%) | 9 (6.5%) | <0.001 |
| IT | 116 (14.2%) | 66 (9.7%) | 50 (36.3%) | |
| NL | 79 (9.7%) | 66 (9.7%) | 13 (9.4%) | |
| SE | 280 (34.3%) | 266 (39.2%) | 14 (10.1%) | |
| SL | 135 (16.5%) | 96 (14.1%) | 39 (28.3%) | |
| UK | 167 (20.4%) | 154 (22.7%) | 13 (9.4%) | |
| Range | AYCs | p | |||
|---|---|---|---|---|---|
| Total | OCRs | GrPs | |||
| 817 (100%) | 679 (83.1 %) | 138 (16.9%) | |||
| MACA-YC18 | 1–36 | 13.2 ± 5.7 | 13.3 ± 5.7 | 12.8 ± 5.6 | 0.326 |
| PANOC-YC20 Negative Outcomes | 0–20 | 5.6 ± 5.2 | 5.8 ± 5.2 | 4.2 ± 4.9 | 0.001 |
| PANOC-YC20 Positive Outcomes | 0–20 | 12.7 ± 47 | 12.5 ± 4.6 | 13.8 ± 4.8 | 0.003 |
| KIDSCREEN-10 General health status | 10–50 | 32.9 ± 7.3 | 32.9 ± 73 | 33.2 ± 7.2 | 0.603 |
| Health problems in connection with caring role, n (%) | <0.001 | ||||
| No | 468 (57.3%) | 384 (56.6%) | 84 (60.9%) | ||
| Yes | 349 (42.7%) | 295 (43.4%) | 54 (39.1%) | ||
| PANOC-YC20 Negative Outcomes | PANOC-YC20 Positive Outcomes | Health Problems in Connection to Care Role | ||||
|---|---|---|---|---|---|---|
| Β | p | β | p | OR | p | |
| Caring for GrPs (ref. No) | −1.09 | 0.010 | 1.20 | 0.008 | 0.94 | 0.765 |
| Age (ref.15) | ||||||
| 16 | −0.76 | 0.159 | 0.49 | 0.330 | 0.76 | 0.245 |
| 17 | −0.75 | 0.157 | 0.68 | 0.179 | 0.77 | 0.278 |
| Gender (ref. Male) | ||||||
| Female | 0.90 | 0.021 | 0.41 | 0.275 | 1.53 | 0.016 |
| Transgender/non-binary | 3.50 | 0.006 | −1.76 | 0.127 | 4.71 | 0.002 |
| Hours a day spent providing care | 0.22 | <0.001 | 0.01 | 0.721 | 1.07 | <0.001 |
| Country of birth (ref. National) | ||||||
| Abroad | 2.49 | <0.001 | 0.36 | 0.560 | 1.30 | 0.382 |
| Formal services (ref. No) | ||||||
| Yes | 1.86 | <0.001 | −0.38 | 0.292 | 1.79 | <0.001 |
| Don’t know | 1.38 | 0.007 | −0.58 | 0.256 | 0.84 | 0.457 |
| Constant | 3.71 | <0.001 | 11.89 | <0.001 | 0.43 | 0.003 |
| R2 | 0.139 | 0.025 | 0.059 | |||
| PANOC-YC20 Negative Outcomes | PANOC-YC20 Positive Outcomes | Health Problems in Connection with Caring Role | ||||
|---|---|---|---|---|---|---|
| Β | p | β | p | OR | p | |
| Caring for GrPs (ref. No) | 0.21 | 0.619 | 0.24 | 0.604 | 0.95 | 0.786 |
| Age (ref.15) | ||||||
| 16 | −0.33 | 0.520 | −0.15 | 0.769 | 0.71 | 0.158 |
| 17 | −0.41 | 0.422 | 0.10 | 0.837 | 0.71 | 0.160 |
| Gender (ref. Male) | ||||||
| Female | 1.19 | 0.002 | 0.14 | 0.708 | 1.51 | 0.022 |
| Transgender/non-binary | 3.58 | 0.003 | −1.68 | 0.128 | 5.02 | 0.002 |
| Hours a day spent providing care | 0.20 | <0.000 | 0.01 | 0.829 | 1.06 | 0.002 |
| Country of birth (ref. National) | ||||||
| Abroad | 2.13 | 0.001 | 0.53 | 0.382 | 1.28 | 0.407 |
| Formal services (ref. No) | ||||||
| Yes | 1.16 | 0.002 | 0.25 | 0.487 | 1.71 | 0.002 |
| Don’t know | 0.39 | 0.472 | 0.01 | 0.989 | 0.94 | 0.801 |
| Country (ref. CH) | ||||||
| IT | −3.75 | <0.001 | 1.64 | 0.069 | 0.56 | 0.153 |
| NL | −3.40 | 0.001 | −1.23 | 0.224 | 0.37 | 0.024 |
| SE | −0.14 | 0.895 | −0.89 | 0.303 | 0.52 | 0.092 |
| SL | −3.87 | <0.001 | 2.04 | 0.022 | 0.59 | 0.184 |
| UK | −0.05 | 0.963 | −0.88 | 0.331 | 0.83 | 0.646 |
| Constant | 4.99 | <0.001 | 12.50 | <0.001 | 0.82 | 0.654 |
| R2 | 0.237 | 0.085 | 0.068 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santini, S.; Socci, M.; D’Amen, B.; Di Rosa, M.; Casu, G.; Hlebec, V.; Lewis, F.; Leu, A.; Hoefman, R.; Brolin, R.; et al. Positive and Negative Impacts of Caring among Adolescents Caring for Grandparents. Results from an Online Survey in Six European Countries and Implications for Future Research, Policy and Practice. Int. J. Environ. Res. Public Health 2020, 17, 6593. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186593
Santini S, Socci M, D’Amen B, Di Rosa M, Casu G, Hlebec V, Lewis F, Leu A, Hoefman R, Brolin R, et al. Positive and Negative Impacts of Caring among Adolescents Caring for Grandparents. Results from an Online Survey in Six European Countries and Implications for Future Research, Policy and Practice. International Journal of Environmental Research and Public Health. 2020; 17(18):6593. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186593
Chicago/Turabian StyleSantini, Sara, Marco Socci, Barbara D’Amen, Mirko Di Rosa, Giulia Casu, Valentina Hlebec, Feylyn Lewis, Agnes Leu, Renske Hoefman, Rosita Brolin, and et al. 2020. "Positive and Negative Impacts of Caring among Adolescents Caring for Grandparents. Results from an Online Survey in Six European Countries and Implications for Future Research, Policy and Practice" International Journal of Environmental Research and Public Health 17, no. 18: 6593. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186593