1. Introduction
By 2050, Portugal is projected to be one of the oldest countries in Europe, with persons aged 55 years or more representing almost half (47.1%) of the total population [
1]. This increasing population aging raises many questions at socioeconomic, health, scientific and ethics levels. It is fundamental to consider in which conditions and with what quality of life (QoL) older adults are and will be living. This important question has led to international interest in the enhancement, and measurement, of quality of life in old age, attracting increasing research and policy interest [
2]. Specifically, in Portugal, the advancement in aging research is noteworthy, with some studies approaching conceptualization and assessment of QoL and related concepts, such as well-being, successful and active aging.
The World Health Organization Quality of Life (WHOQOL) group has developed outstanding work in this area. This group has proposed a definition and operationalized the construct from a cross-cultural perspective, resulting in three instruments: WHOQOL-100, WHOQOL-BREF and WHOQOL-OLD [
3,
4]. This last one was specifically created to study older adults’ QoL and already has a European Portuguese version, with the same categories of the original version (sensory abilities; autonomy; past, present and future activities; social participation; death and dying; and intimacy) and with a seventh one regarding family/family life, which is an important dimension for understanding Portuguese older adults’ QoL [
5]. Despite the common use of WHOQOL instruments in research and the availability of several measures to assess health-related QoL in Portugal (e.g., SF-36, EQ-5D), the extent of available generic QoL instruments applicable to the older population is still limited.
The Control, Autonomy, Self-realization, and Pleasure (CASP)-19 scale is one of most frequently used measures of QoL in older age [
6]. Based on a psycho-sociological conceptualization of QoL that draws on the “theory of human need”, scale includes 19 Likert-type items that reflect four different dimensions of QoL: control (four items), autonomy (five items), self-realization (five items), and pleasure (five items) [
6,
7,
8]. Taken together, the items can be combined into a measure of overall QoL, as they present the degree to which the respondents have their needs covered. Due to the questionable psychometric properties of CASP-19 presented by several researchers who highlighted that the factor structure of the scale did not follow what was predicted by the theory [
9,
10], a shorter version of the scale has been proposed (CASP-12) [
9]. This version leaves out the items that only weakly reflect a given dimension [
9].
To date, both the original version and the shorter version of CASP have been increasingly used internationally. The scale has been included in many national and cross-national studies in countries from North and South America, as well as from Africa and Australasia [
11]. In Europe, it has been used in countries like United Kingdom, France, Sweden and Ireland, being also included in two well-known cross-national projects: the Health, Alcohol and Psychosocial factors in Eastern Europe (HAPIEE) and the Survey of Health, Aging and Retirement in Europe (SHARE) [
12]. This last project in particular constitutes a longitudinal survey conducted every two years since 2004 that collects information on medical, social and economic status of the population aged 50+ from more than 20 countries in Europe [
13].
In a recent and thorough examination of the psychometric properties of the SHARE version of the CASP-12 scale that included internal consistency analyses, factor structure analyses, item-total Spearman correlations, and cross country invariance, Borrat-Besson et al. showed that the structure postulated by the authors of the CASP-12 scale could not be replicated, and suggested a revised scale with ten items instead of twelve [
14]. In addition, when exploring the cross-cultural robustness of the results, they showed that Portugal and Italy presented different results. Both countries stand out against the general results pattern with respect to the pleasure dimension since item 10 (“I look forward to each day”) correlated negatively with all dimensions. This result was associated to aspects of translation and interpretation, reinforcing the importance of cultural significance in validation processes. Other studies have found a 2 or 3-factor structure [
15,
16].
Presently, the number of studies advancing the available understanding of the underlying structure of the CASP scale has been rising [
11], including the evaluation of its dimensionality using Rasch analysis [
17]. Rasch analysis is a robust item response theory technique that provides information on the dimensionality of a scale, contributing thus to the construct validity testing, and also on item fit and item local dependency, differential item functioning (DIF), and disordered response categories. Scales that fit the Rasch model provide an interval linear measure that establishes equal intervals between the values, and that could be used in parametric analysis. Despite these advances, there are no full validation studies of the Portuguese version of the CASP scale used in the SHARE project.
The purpose of this study is to analyze the psychometric properties of the European Portuguese version of the CASP-12 scale used in the SHARE project in a sample of people aged 50 years of older.
3. Results
The sample was composed of 55% women, had an overall mean age of 67.81 (SD: 9.01; range: 50–94), and presented an average of 6.28 years of education (SD: 4.16; range: 0–25), with most of the sample (61.8%) having primary level education. Most of the participants were married or lived with a spouse (75.9%), were retired (62.4%), and lived in urban settings (72.5%). A description of the sample is presented in
Table 1.
The CASP-12 total score was computable for 1468 (88.1%) participants, thus, missing data represented 11.9% of the sample. The mean CASP-12 was 26.68 (SD: 5.80, range: 12–48). Skewness for the total score was 0.311, and floor and ceiling effects were less than 0.5% (
Table 2). For domains, pleasure presented the highest percentage of missing data (11.3%) and floor effect (12.1%). All domain scores covered the full score range (3 to 12 points). No domain showed a ceiling effect. Some items presented marked floor or ceiling effects, particularly in the autonomy and pleasure domains.
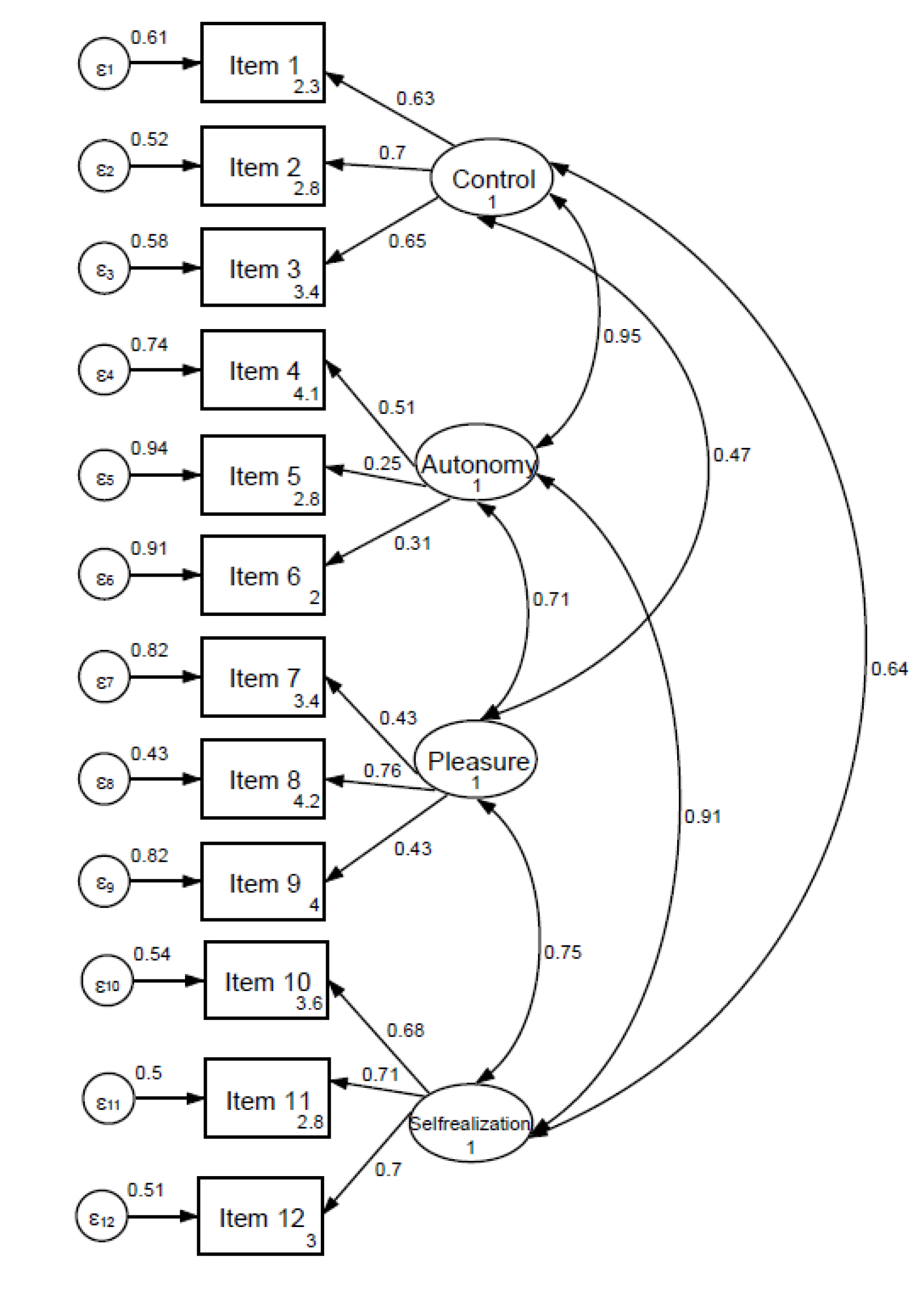
Figure 1 shows the path diagram of the CASP-12 scale performed through CFA. The 4-factor model obtained a RMSEA of 0.07 and a CFI of 0.90, χ
2 (48) = 444.59,
p < 0.001). Details are provided in the
Supplementary Material, including models for one and three factors.
Item–total corrected correlation was 0.25–0.59 for total scale. By domains, the lowest values corresponded to autonomy (0.13–0.26) and the highest to self-realization (0.48–0.61). The inter-domain correlation coefficients (internal validity) are shown in
Table 3. CASP-12 domains correlated from 0.22 (autonomy and pleasure) to 0.46 (pleasure and self-realization). Regarding convergent validity (
Table 3), CASP-12 total score correlated −0.57 with Euro-D, 0.52 with life satisfaction, −0.47 with self-perceived health and 0.41 with GALI. For domains, control (r
S = 0.49) and self-realization (r
S = 0.46) reached the highest correlation coefficients with Euro-D. Self-realization also showed the highest correlation coefficients with life satisfaction (r
S = −0.46) and self-perceived health (r
S = 0.45). The pleasure domain displayed the lowest correlation coefficients with the other applied measures.
CASP-12 total and domains showed significant differences in scores by sex (women showed lower mean scores than men,
p < 0.01), by age groups (lower mean scores in older participants in all domains except in autonomy,
p < 0.01), by activity limitation assessed with GALI (higher mean scores for those participants without limitations,
p < 0.001), by self-perceived health (lower mean scores for participants with poor health,
p < 0.001), and by presence of multimorbidity (lower mean scores for participants with two or more chronic conditions,
p < 0.001) (
Table 4).
Regarding internal consistency (
Table 5), Cronbach’s alpha for the total score of CASP-12 was 0.78, with a range from 0.37 (autonomy) to 0.73 (self-realization) for domains. Inter-item correlation and item homogeneity indexes were lower for autonomy and higher for self-realization.
Finally, a Rasch analysis was performed with the 12 items, showing a lack of fit to the Rasch model. Therefore, each domain was analyzed separately, and all showed unidimensionality, ordered thresholds, item local independency and lack of DIF by gender.
Table 6 presents the person and item fit parameters for the CASP-12 domains. The control domain presented a good fit to the Rasch model, PSI = 0.617. Item 1 (“My age prevents me from doing the things I would like to do”) displayed DIF by age, with adults aged 75 or more underestimating scores. Similarly to control, the autonomy domain, showed a good fit to the Rasch model with a low PSI of 0.312 and DIF by age for item 4 (“I can do the things I want to do”). The pleasure domain displayed an adequate fit to the Rasch model after splitting items 8 (“I feel that my life has meaning”) and 9 (“On balance, I look back on my life with a sense of happiness”) due to DIF by age (underestimation of scores by older adults), with low PSI (0.372). Finally, the self-realization section had a good fit to the Rasch model, PSI = 0.71, and no DIF by age groups. When super items were created for each domain, a good fit to the Rasch model was observed, with χ
2 (36) = 10.089,
p = 0.745, PSI = 0.722.
4. Discussion
This is the first complete validation study with the European Portuguese version of the CASP-12 scale used in the SHARE study. This version is slightly different to that originally proposed by Wiggins et al. [
9].
Regarding data quality and acceptability, missing data and skewness of domains and total score were within the standard limits. Most items showed a marked ceiling effect, particularly in the control and pleasure domains, and two items showed a floor effect. This is in line with the other studies reporting the distribution of items scores in CASP-12 [
15]. However, domains and total score did not show floor or ceiling effects.
Internal consistency of CASP-12 was satisfactory in the self-realization domain and when combining all items. The autonomy domain presented the lowest values of internal consistency, as reported in previous studies [
14,
15]. The autonomy and pleasure domains also showed low reliability indices in Rasch analysis. This should be considered when using these two domains individually.
The autonomy domain also showed the weakest results for internal, construct and structural validity. This domain showed low correlation coefficients with other domains (0.22 with pleasure and 0.36 with self-realization). In Rasch analysis, the autonomy domain presented a low reliability and one item with bias by age. Some authors have proposed dropping the items on “family responsibilities” and on “shortage of money”, as they could be measuring something different to QoL [
9], or forming a domain with control in a bi- or tri-factorial model [
15,
16]. However, despite the problems with the item on “family responsibilities”, family life is an important dimension for Portuguese older adults’ QoL, as commented in the Introduction, and this prevent us from deleting this item [
5].
Moreover, the CFA supported the 4-factor model proposed by CASP-12 original developers [
42]. However, the factor intercorrelations found in the CFA were much higher than the scale intercorrelations for internal validity. In addition, items 5 and 6 items loaded weakly on the “autonomy” scale, and the same was observed for item 7 on the “pleasure” scale. This suggests the need for further research to elucidate on the advantages and disadvantages of using different factor structures of the CASP-12 scale in Portugal. Even though the first 12-item model did provide a good fit to the Rasch model, an adequate fit was found for each of the individual domains, as well as the model with one super item per domain. Thus, results from Rasch analysis point to a hierarchical scale structure of the CASP-12 scale with a higher-order construct, QoL, formed by four lower-order unidimensional sections. A previous Rasch analysis found evidence for a unidimensional 15-item version of the CASP scale [
17].
Regarding convergent validity, the total score of CASP-12 showed the highest correlation coefficients with the item on satisfaction with life and with the Euro-D, as hypothesized. Depression is a main determinant of QoL deterioration, and this relationship has been previously reported in other studies applying CASP-12 in older samples [
43].
Women, participants aged 76 year or older, with limitations of activity, with poor self-perceived health and with two or more chronic diseases scored significantly lower in CASP-12, as in other studies [
43,
44]. Portugal has a high old age–dependency ratio, reaching 65.8% [
1]; thus, these results suggest the need of intervention in the most vulnerable population to improve their QoL and achieve healthy and active aging. Gender differences are not due to an item bias by gender, as indicated in our DIF analyses and in previous studies [
17]. However, a bias by age was found in four items, and further research is needed to confirm our findings. If confirmed, differences by age in the autonomy and pleasure dimensions should be interpreted cautiously, as they might be due to item bias.
Several limitations to this study must be acknowledged. A heterogeneous, diverse sample is usually advised for validation studies. In this case, the SHARE project does not include individuals living in nursing homes. Furthermore, because of the cross-sectional design, it is not possible to evaluate the temporal stability of the structure presented. Therefore, further studies should assess CASP-12 validity with other Portuguese samples (i.e., institutionalized older adults) and analyze responses for test-retest reliability.
In explicitly resisting a conflation of QoL with health status that often happens in old age, the CASP scale was developed to focus on favorable and advantageous features of aging and on older people’s positive characteristics [
42]. Despite some limitations, it is an instrument with adequate psychometric features, and its use is encouraged as it may contribute to furthering the study of older adults’ needs and strengths and therefore improve the well-being of the older population in Portugal. The CASP-12 scale is a QoL instrument that might be useful for clinical practice, as well as to assess public health interventions and aging policies in Portugal. In addition, this study underscores the past and future research studies performed with data from the SHARE project and that use the CASP-12 scale as a QoL measure.
5. Conclusions
In conclusion, the European Portuguese version of the CASP-12 scale, when applied to people aged 50 years or older, presented some inadequacies in terms of acceptability, internal consistency and structural and construct validity of two of the four domains that compose it. Therefore, the total score could be preferred over the use of individual domains scores. The European Portuguese version of the CASP-12 scale used in the SHARE project presents some strengths, such as good acceptability, unbiased scores by gender, fit to the Rasch model, and adequate reliability of the pleasure and self-realization domains. Nevertheless, future research should present more evidence on the scale’s psychometric properties, including its factor structure in different samples, namely, old–old and institutionalized individuals.

 ,
, 


{kind=link}