Evaluation of Salivary Matrix Metalloproteinase (MMP-8) in Periodontal Patients Undergoing Non-Surgical Periodontal Therapy and Mouthwash Based on Ozonated Olive Oil: A Randomized Clinical Trial


 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population and Setting
2.3. Sample Size Calculation
2.4. Inclusion Criteria
- Male or female, 30–60 years old;
- With diagnosis of periodontal disease;
- Plaque index (PI) ≥ 35%, Gingival index (GI) ≥ 35%;
- No diabetes and cardiovascular diseases;
- No pharmacological therapies;
- No smoking, alcohol and/or drug consumption;
- No pregnancy or breastfeeding;
- No allergy.
2.5. Randomized Allocation
2.6. Blinding
2.7. Periodontal Charting
2.8. Salivary MMP-8 Assessment
2.9. Description of the Mouthwash
2.10. Clinical Procedure
2.11. Co-Intervention
2.12. Duration of the Study and Times of Follow-Up
2.13. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Birkedal-Hansen, H.; Moore, W.; Bodden, M.; Windsor, L.; Birkedal-Hansen, B.; Decarlo, A.; Engler, J. Matrix Metalloproteinases: A Review. Crit. Rev. Oral Biol. Med. 1993, 4, 197–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birkedal-Hansen, H. Role of matrix metalloproteinases in human periodontal diseases. J. Periodontol. 1993, 64, 474–484. [Google Scholar] [PubMed]
- Reynolds, J.J.; Meikle, M.C. Mechanisms of connective tissue matrix destruction in periodontitis. Periodontol 2000 1997, 14, 144–157. [Google Scholar] [CrossRef] [PubMed]
- Sorsa, T.; Tjäderhane, L.; Salo, T. Matrix metalloproteinases (MMPs) in oral diseases. Oral Dis. 2004, 10, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.Y.; Cox, S.W.; Eley, B.M.; Mäntylä, P.; Rönkä, H.; Sorsa, T. Matrix metalloproteinase-8 levels and elastase activities in gingival crevicular fluid from chronic adult periodontitis patients. J. Clin. Periodontol. 2000, 27, 366–369. [Google Scholar] [CrossRef]
- Cole, A.A.; Chubinskaya, S.; Schumacher, B.; Huch, K.; Cs-Szabo, G.; Yao, J.; Mikecz, K.; Hasty, K.A.; Kuettner, K.E. Chondrocyte Matrix Metalloproteinase. J. Biol. Chem. 1996, 271, 11023–11026. [Google Scholar] [CrossRef] [Green Version]
- Kiili, M.; Cox, S.W.; Chen, H.W.; Wahlgren, J.; Maisi, P.; Eley, B.M.; Salo, T.; Sorsa, T.; Chen, H.W. Collagenase-2 (MMP-8) and collagenase-3 (MMP-13) in adult periodontitis: Molecular forms and levels in gingival crevicular fluid and immunolocalisation in gingival tissue. J. Clin. Periodontol. 2002, 29, 224–232. [Google Scholar] [CrossRef]
- Kinney, J.S.; Ramseier, C.A.; Giannobile, W.V. Oral fluid-based biomarkers of alveolar bone loss in periodontitis. Ann. N.Y. Acad. Sci. 2007, 1098, 230–251. [Google Scholar] [CrossRef] [Green Version]
- Özmeriç, N. Advances in periodontal disease markers. Clin. Chim. Acta 2004, 343, 1–16. [Google Scholar] [CrossRef]
- Ingman, T.; Sorsa, T.; Michaelis, J.; Konttinen, Y.T. Immunohistochemical study of neutrophil- and fibroblast-type collegenase and stromelysin-1 in adult periodontitis. Scand. J. Dent Res. 1994, 102, 342–349. [Google Scholar]
- Golub, L.M.; Lee, H.M.; Greenwald, R.A.; Ryan, M.E.; Sorsa, T.; Salo, T.; Giannobile, W.V. A matrix metalloproteinase inhibitor reduces bone-type collagen degradation fragments and specific collagenases in gingival crevicular fluid during adult periodontitis. Inflamm. Res. 1997, 46, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Prasanna, V.; Lakshmanan, R. Characteristics, uses and side effects of chlorhexidine—A review. IOSR JDMS 2016, 15, 57–59. [Google Scholar]
- Plantinga, N.L.; Wittekamp, B.H.J.; Leleu, K.; Depuydt, P.; Abeele, A.-M.V.D.; Brun-Buisson, C.; Bonten, M.J.M. Oral mucosal adverse events with chlorhexidine 2% mouthwash in ICU. Intensive Care Med. 2016, 42, 620–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hidalgo, E.; Dominguez, C. Mechanisms underlying chlorhexidine-induced cytotoxicity. Toxicol. Vitr. 2001, 15, 271–276. [Google Scholar] [CrossRef]
- Megha Gupta; Abhishek. Ozone: An emerging prospect in dentistry. Indian J. Dent. Sci. 2012, 1, 47–50. [Google Scholar]
- Nardi, G.M.; Sabatini, S.; Guerra, F.; Tatullo, M.; Ottolenghi, L. Tailored Brushing Method (TBM): An Innovative Simple Protocol to Improve the Oral Care. J. Biomed. 2016, 1, 26–31. [Google Scholar] [CrossRef] [Green Version]
- Brauner, A. Periodontology: New Methods. Ozone Sci. Eng. 1992, 14, 165–176. [Google Scholar] [CrossRef]
- Menabde, G.T.; Natroshvili, N.D.; Natroshvili, T.D. Ozonotherapy for the treatment of periodontitis. Georgian Med. News 2006, 134, 43–46. [Google Scholar]
- Ingman, T.; Tervahartiala, T.; Ding, Y.; Tschesche, H.; Haerian, A.; Kinane, D.F.; Konttinen, Y.T.; Sorsa, T. Matrix metalloproteinases and their inhibitors in gingival crevicular fluid and saliva of periodontitis patients. J. Clin. Periodontol. 1996, 23, 1127–1132. [Google Scholar] [CrossRef]
- Holmes, J. Clinical reversal of root caries using ozone, double-blind, randomised, controlled 18-month trial. Gerodontology 2003, 20, 106–114. [Google Scholar] [CrossRef]
- Christodoulides, N.; Floriano, P.N.; Miller, C.S.; Ebersole, J.L.; Mohanty, S.; Dharshan, P.; Griffin, M.; Lennart, A.; Ballard, K.L.M.; King, C.P.; et al. Lab-on-a-Chip Methods for Point-of-Care Measurements of Salivary Biomarkers of Periodontitis. Ann. N.Y. Acad. Sci. 2007, 1098, 411–428. [Google Scholar] [CrossRef]
- Miller, C.S.; King, C.P.; Langub, M.C.; Kryscio, R.J.; Thomas, M.V. Salivary biomarkers of existing periodontal disease. J. Am. Dent. Assoc. 2006, 137, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Agan, S.; Sönmez, S.; Serdar, M. The effect of topical doxycycline usage on gingival crevicular fluid MMP-8 levels of chronic and aggressive periodontitis patients: A pilot study. Int. J. Dent. Hyg. 2006, 4, 114–121. [Google Scholar] [CrossRef]
- Kinane, D.F.; Darby, I.B.; Said, S.; Luoto, H.; Sorsa, T.; Tikanoja, S.; Mäntylä, P. Changes in gingival crevicular fluid matrix metalloproteinase-8 levels during periodontal treatment and maintenance. J. Periodontal Res. 2003, 38, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Pozo, P.; Valenzuela, M.A.; Melej, C.; Zaldivar, M.; Puente, J.; Martinez, B.; Gamonal, J. Longitudinal analysis of metalloproteinases, tissue inhibitors of metalloproteinases and clinical parameters in gingival crevicular fluid from periodontitis-affected patients. J. Periodontal Res. 2005, 40, 199–207. [Google Scholar] [CrossRef]
- Nicolini, A.C.; Rotta, I.D.S.; Langa, G.P.J.; Friedrich, S.A.; Arroyo-Bonilla, D.A.; Wagner, M.C.; Weidlich, P.; Rösing, C.K.; Cavagni, J. Efficacy of ozonated water mouthwash on early plaque formation and gingival inflammation: A randomized controlled crossover clinical trial. Clin. Oral Investig. 2020, 6, 1–8. [Google Scholar] [CrossRef]
- Verma, R.; Indurkar, M.S. Effect of ozonated oil and chlorhexidine gel on plaque induced gingivitis: A randomized control clinical trial. J. Indian Soc. Periodontol. 2016, 20, 32–35. [Google Scholar] [CrossRef]
- Nogales, C.G.; Ferrari, P.H.; Kantorovich, E.O.; Lage-Marques, J.L. Ozone Therapy in Medicine and Dentistry. J. Contemp. Dent. Pr. 2008, 9, 75–84. [Google Scholar] [CrossRef]
- Mohanty, S.; Panigrahi, A. Ozone-Boon in Dentistry. Indian J. Public Health Res. Dev. 2019, 10, 780. [Google Scholar] [CrossRef]
- Sivalingam, V.P.; Panneerselvam, E.; Raja, K.V.; Gopi, G. Does Topical Ozone Therapy Improve Patient Comfort After Surgical Removal of Impacted Mandibular Third Molar? A Randomized Controlled Trial. J. Oral Maxillofac. Surg. 2017, 75, 51. [Google Scholar] [CrossRef]
- Uitto, V.J.; Suomalainen, K.; Sorsa, T. Salivary collagenase. Origin, characteristics and relationship to periodontal health. J. Periodontal Res. 1990, 25, 135–142. [Google Scholar] [PubMed]
- Isola, G.; Matarese, G.; Ramaglia, L.; Pedullà, E.; Rapisarda, E.; Iorio-Siciliano, V. Association between periodontitis and glycosylated haemoglobin before diabetes onset: A cross-sectional study. Clin. Oral Investig. 2019, 24, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Korostoff, J.M.; Wang, J.F.; Sarment, D.P.; Stewart, J.C.; Feldman, R.S.; Billings, P.C. Analysis ofIn SituProtease Activity in Chronic Adult Periodontitis Patients: Expression of Activated MMP-2 and a 40 kDa Serine Protease. J. Periodontol. 2000, 71, 353–360. [Google Scholar] [CrossRef]
- Lynch, E. Leczenie prochnicy za pomocą ozonu. Quintessence Lek. Stomatol. 2003, 11, 198–200. [Google Scholar]
- Bocci, V. Ozone: A New Medical Drug; Springer: Berlin/Heidelberg, Germany, 2005; p. 162. [Google Scholar]
- Górnicki, A.; Gutsze, A. In vitro effects of ozone on human erythrocyte membranes: An EPR study. Acta Biochim. Pol. 2000, 47, 963–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Measurement | Index | Study Group | Control Group | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
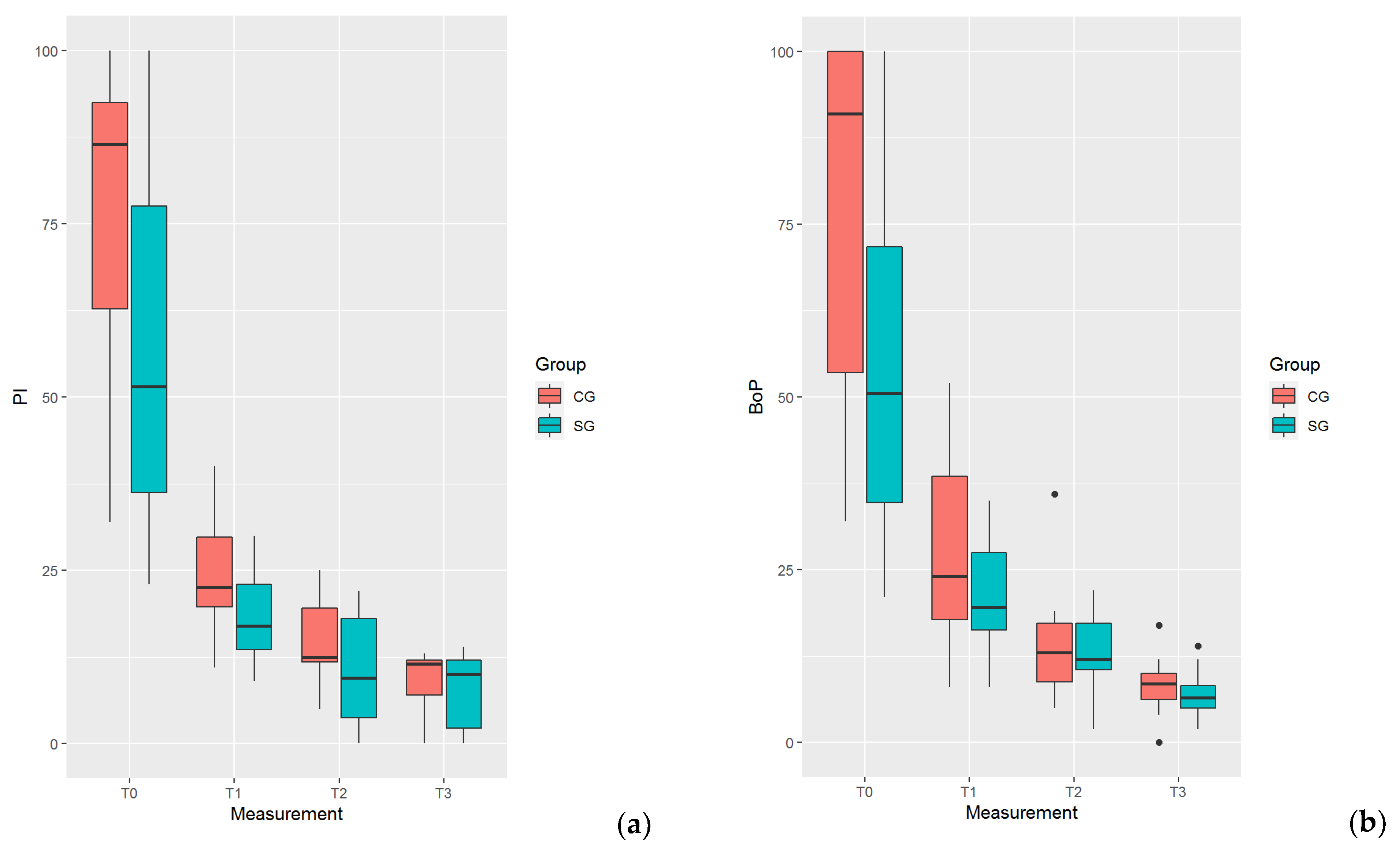
| T0 | PI | 56.75 | 25.95 | 77.33 | 21.10 |
| BoP | 54.67 | 27.07 | 76.08 | 27.27 | |
| PPD | 4.426 | 1.391 | 4.394 | 0.781 | |
| MMP | 82.26 | 54.41 | 128.75 | 30.74 | |
| T1 | PI | 18.58 | 6.503 | 23.75 | 8.456 |
| BoP | 20.83 | 8.270 | 27.50 | 13.31 | |
| PPD | 2.351 | 0.899 | 2.884 | 0.785 | |
| MMP-8 | 63.12 | 48.82 | 115.9 | 30.04 | |
| T2 | PI | 10.25 | 8.170 | 14.83 | 5.684 |
| BoP | 12.67 | 5.926 | 14.25 | 7.930 | |
| PPD | 2.15 | 0.922 | 2.206 | 0.781 | |
| MMP-8 | 45.48 | 37.96 | 106.0 | 29.18 | |
| T3 | PI | 7.417 | 5.242 | 9.250 | 3.917 |
| BoP | 7.000 | 3.377 | 8.250 | 4.190 | |
| PPD | 2.083 | 0.814 | 2.451 | 0.746 | |
| MMP-8 | 32.33 | 27.76 | 94.32 | 26.91 | |
| Measurement | Outcome | Study Group | Control Group | Difference SG–CG | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | Std. Error | Mean | Std. Error | Mean | Std. Error | p-Value | ||
| T1 | PI | 0.6864 | 0.013 | 0.6313 | 0.019 | −0.0551 | 0.024 | 0.022 |
| BoP | 0.6221 | 0.023 | 0.5503 | 0.034 | -0.0718 | 0.041 | 0.085 | |
| PPD | 0.3354 | 0.023 | 0.4181 | 0.037 | 0.0828 | 0.044 | 0.065 | |
| MMP-8 | 0.1038 | 0.005 | 0.2867 | 0.015 | 0.1829 | 0.016 | <0.001 | |
| T2 | PI | 0.8074 | 0.008 | 0.8115 | 0.022 | 0.0041 | 0.024 | 0.863 |
| BoP | 0.7994 | 0.013 | 0.7342 | 0.022 | −0.0652 | 0.026 | 0.014 | |
| PPD | 0.4853 | 0.028 | 0.4600 | 0.041 | −0.0253 | 0.050 | 0.616 | |
| MMP-8 | 0.1841 | 0.008 | 0.4992 | 0.016 | 0.3151 | 0.018 | <0.001 | |
| T3 | PI | 0.8777 | 0.008 | 0.8692 | 0.016 | −0.0084 | 0.018 | 0.640 |
| BoP | 0.8868 | 0.010 | 0.8536 | 0.012 | −0.0331 | 0.016 | 0.040 | |
| PPD | 0.4326 | 0.023 | 0.4652 | 0.040 | 0.0327 | 0.046 | 0.483 | |
| MMP-8 | 0.2755 | 0.009 | 0.6509 | 0.014 | 0.3755 | 0.016 | <0.001 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nardi, G.M.; Cesarano, F.; Papa, G.; Chiavistelli, L.; Ardan, R.; Jedlinski, M.; Mazur, M.; Grassi, R.; Grassi, F.R. Evaluation of Salivary Matrix Metalloproteinase (MMP-8) in Periodontal Patients Undergoing Non-Surgical Periodontal Therapy and Mouthwash Based on Ozonated Olive Oil: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 6619. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186619
Nardi GM, Cesarano F, Papa G, Chiavistelli L, Ardan R, Jedlinski M, Mazur M, Grassi R, Grassi FR. Evaluation of Salivary Matrix Metalloproteinase (MMP-8) in Periodontal Patients Undergoing Non-Surgical Periodontal Therapy and Mouthwash Based on Ozonated Olive Oil: A Randomized Clinical Trial. International Journal of Environmental Research and Public Health. 2020; 17(18):6619. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186619
Chicago/Turabian StyleNardi, Gianna Maria, Francesca Cesarano, Giulio Papa, Lorella Chiavistelli, Roman Ardan, Maciej Jedlinski, Marta Mazur, Roberta Grassi, and Felice Roberto Grassi. 2020. "Evaluation of Salivary Matrix Metalloproteinase (MMP-8) in Periodontal Patients Undergoing Non-Surgical Periodontal Therapy and Mouthwash Based on Ozonated Olive Oil: A Randomized Clinical Trial" International Journal of Environmental Research and Public Health 17, no. 18: 6619. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186619