Reliability of the Resonance Frequency Analysis Values in New Prototype Transepithelial Abutments: A Prospective Clinical Study


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
- Patients with age equal to or greater than 18 years.
- Patients whose wishes and needs were rehabilitation with dental implants.
- Collaborative patients with unremarkable medical histories (ASA 1)
- Healthy, non-smoking, no or minimal alcohol use [24] and not known diagnosed allergies.
- Implants that were placed in areas in which extractions were performed at least 4 months before the implant surgery, thus the ridge was fully healed.
- Implants placed in areas with no bone regeneration needed.
- Implants with absence of clinical mobility or painful symptoms.
- -
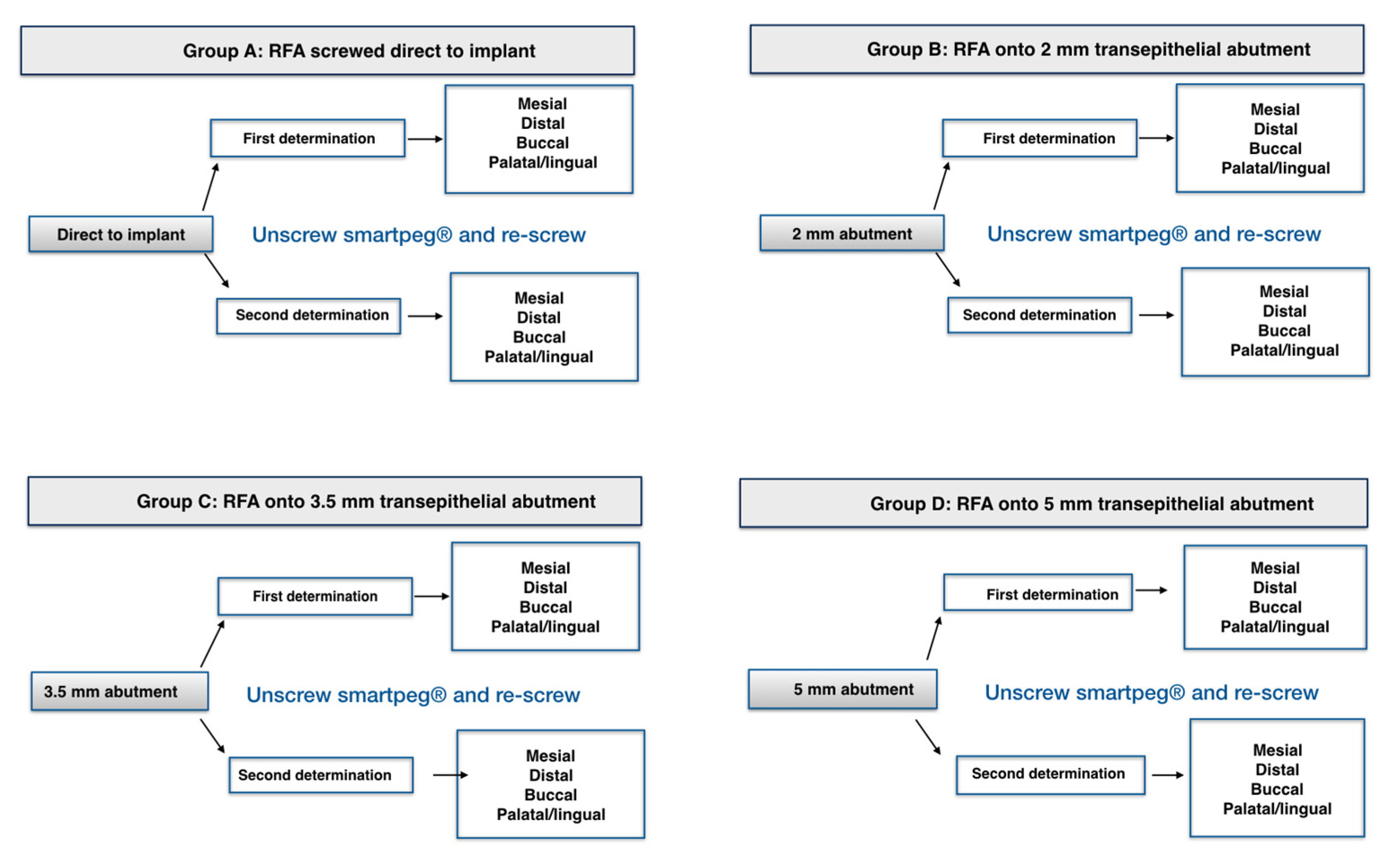
- A prototype transepithelial abutment was screwed at 10 N to avoid loosening by mechanical torque control as recommended by the manufacturer.
- -
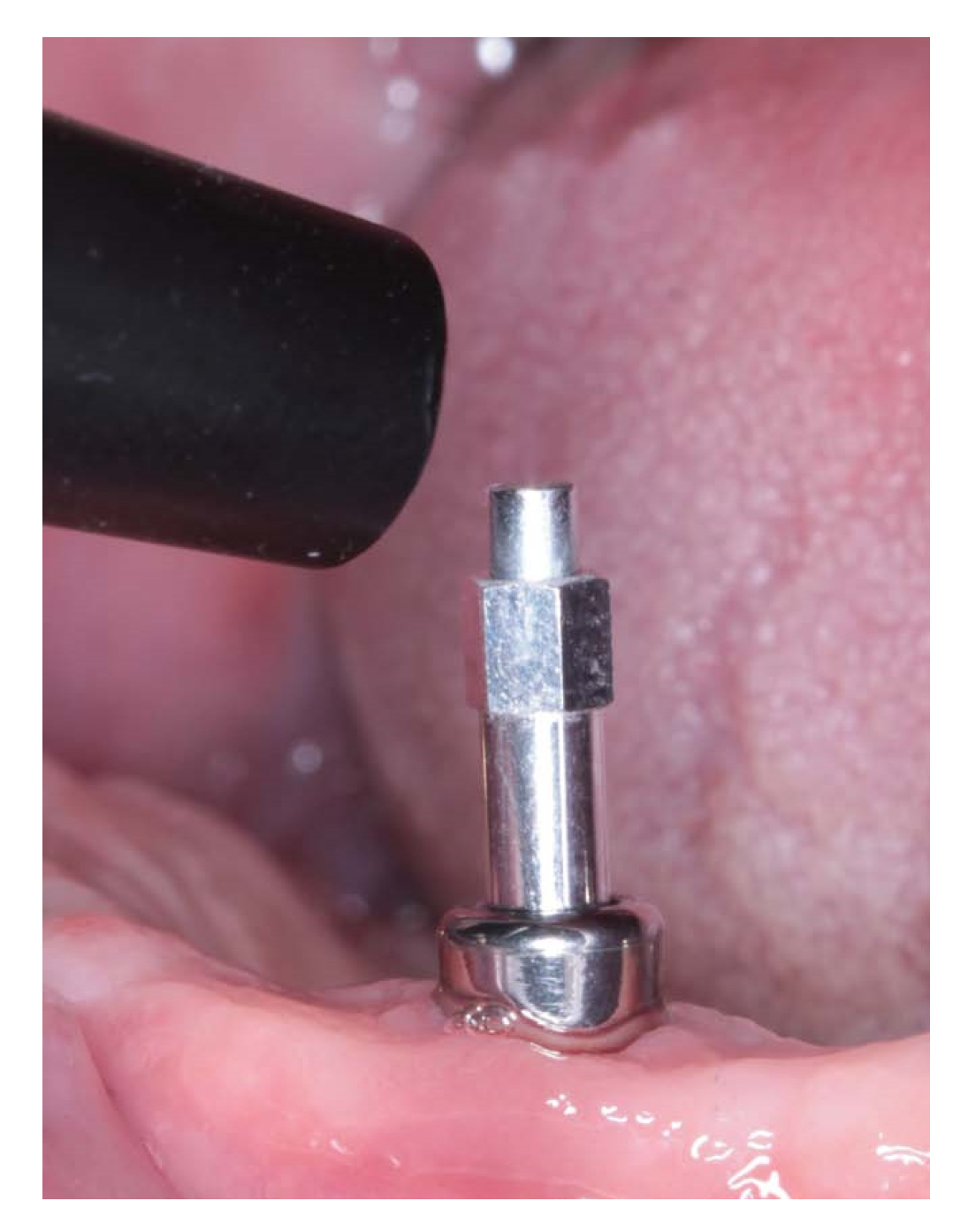
- Smartpeg placement was carried out strictly following manufacturer’s guidelines.
- -
- No tissue interposition between implant and SmartPeg.
- -
- Digital tightening (4–5 N/cm) with the plastic screwdriver provided by the manufacturer [25].
- -
- The SmartPeg had no contact with the neighboring teeth.
Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Meredith, N. Assessment of implant stability as a prognostic determinant. Int. J. Prosthodont. 1998, 11, 491–501. [Google Scholar]
- Chang, P.C.; Lang, N.P.; Giannobile, W.V. Evaluation of functional dynamics during osseointegration and regeneration associated with oral implants. Clin. Oral Implant. Res. 2010, 21, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Meredith, N.; Alleyne, D.; Cawley, P. Quantitative determination of the stability of the implant-tissue interface using resonance frequency analysis. Clin. Oral Implant. Res. 1996, 7, 261–267. [Google Scholar] [CrossRef]
- Meredith, N.; Shagaldi, F.; Alleyne, D.; Sennerby, L.; Cawley, P. The application of resonance frecuency measurements to study the stability of titanium implants during healing in the rabbit tibia. Clin. Oral Implant. Res. 1997, 8, 234–243. [Google Scholar] [CrossRef]
- Veltri, M.; Balleri, P.; Ferrari, M. Influence of transducer orientation on Osstell stability measurements of osseointegrated implants. Clin. Implant. Dent. Relat. Res. 2007, 9, 60–64. [Google Scholar] [CrossRef]
- Herrero-Climent, M.; Albertini, M.; Rios-Santos, J.V.; Lázaro-Calvo, P.; Fernández-Palacín, A.; Bullon, P. Resonance frequency analysis-reliability in third generation instruments: Osstell mentor. Med. Oral Patol. Oral Cir. Bucal 2012, 17, 801–806. [Google Scholar] [CrossRef] [Green Version]
- Herrero-Climent, M.; Santos-García, R.; Jaramillo-Santos, R.; Romero-Ruiz, M.M.; Fernández-Palacin, A.; Lázaro-Calvo, P.; Bullón, P.; Ríos-Santos, J.V. Assessment of Osstell ISQ’s reliability for implant stability measurement: A cross-sectional clinical study. Med. Oral Patol. Oral Cir. Bucal 2013, 18, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Lages, F.S.; Douglas-de Oliveira, D.W.; Costa, F.O. Relationship between implant stability measurements obtained by insertion torque and resonance frequency analysis: A systematic review. Clin. Implant. Dent. Relat. Res. 2018, 20, 26–33. [Google Scholar] [CrossRef]
- Sennerby, L.; Meredith, N. Implant stability measurements using resonance frequency analysis: Biological and biomechanical aspects and clinical implications. Periodontology 2000 2008, 47, 51–66. [Google Scholar] [CrossRef]
- Friberg, B.; Sennerby, L.; Linden, B.; Gröndahl, K.; Lekholm, U. Stability measurements of one-stage Brånemark implants during healing in mandibles. A clinical resonance frequency analysis study. Int. J. Oral Maxillofac. Surg. 1999, 28, 266–272. [Google Scholar] [CrossRef]
- Friberg, B.; Sennerby, L.; Meredith, N.; Lekholm, U. A comparison between cutting torque and resonance frecuency measurements of maxillary implants. A 20 month clinical study. Int. J. Oral Maxillofac. Surg. 1999, 28, 297–303. [Google Scholar] [CrossRef]
- Bischof, M.; Nedir, R.; Szmukler-Moncler, S.; Bernard, J.P.; Samson, J. Implant stability measurement of delayed and immediately loaded implants during healing. Clin. Oral Implants Res. 2004, 15, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Romanos, G.E.; Bastardi, D.J.; Kakar, A.; Moore, R.; Delgado-Ruiz, R.A.; Javed, F. In vitro comparison of resonance frequency analysis devices to evaluate implant stability of narrow diameter implants at varying drilling speeds in dense artificial bone blocks. Clin. Implant Dent. Relat. Res. 2019, 21, 1023–1027. [Google Scholar] [CrossRef] [PubMed]
- Sim, C.P.; Lang, N.P. Factors influencing resonance frequency analysis assessed by Osstell mentor during implant tissue integration: Instrument positioning, bone structure, implant length. Clin. Oral Implant. Res. 2010, 21, 598–604. [Google Scholar] [CrossRef]
- Gallucci, G.O.; Benic, G.I.; Eckert, S.E.; Papaspyridakos, P.; Schimmel, M.; Schrott, A.; Weber, H.P. Consensus statements and clinical recommendations for implant loading protocols. Int. J. Oral Maxillofac. Implant. 2014, 29, 287–290. [Google Scholar] [CrossRef]
- Sanz, M.; Ivanoff, C.J.; Weingart, D.; Wiltfang, J.; Gahlert, M.; Cordaro, L.; Ganeles, J.; Bragger, U.; Jackowski, J.; Martin, W.C.; et al. Clinical and radiologic outcomes after submerged and transmucosal implant placement with two-piece implants in the anterior maxilla and mandible: 3-year results of a randomized controlled clinical trial. Clin. Implant. Dent. Relat. Res. 2015, 17, 234–246. [Google Scholar] [CrossRef]
- Baltayan, S.; Pi-Anfruns, J.; Aghaloo, T.; Moy, P.K. The Predictive Value of Resonance Frequency Analysis Measurements in the Surgical Placement and Loading of Endosseous Implants. J. Oral Maxillofac. Surg. 2016, 74, 1145–1152. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, C.M.; Carvalho, L.F.; Costa, L.J.; Sa, M.J.; Figueiredo, C.R.; Azevedo, A.S. Titanium implants: A removal torque study in osteopenic rabbits. Indian J. Dent. Res. 2010, 21, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Roccuzzo, M.; Bunino, M.; Prioglio, F.; Bianchi, S.D. Early loading of sandblasted and acid-etched (SLA) implants: A prospective split-mouth comparative study. Clin. Oral Implant. Res. 2001, 12, 572–578. [Google Scholar] [CrossRef]
- Praça, L.F.G.; Teixeira, R.C.; Rego, R.O. Influence of abutment disconnection on peri-implant marginal bone loss: A randomized clinical trial. Clin. Oral Implant. Res. 2020, 31, 341–351. [Google Scholar] [CrossRef]
- Bressan, E.; Grusovin, M.G.; D’Avenia, F.; Neumann, K.; Sbricoli, L.; Luongo, G.; Esposito, M. The influence of repeated abutment changes on peri-implant tissue stability: 3-year post-loading results from a multicentre randomised controlled trial. Eur. J. Oral Implantol. 2017, 10, 373–390. [Google Scholar]
- Canullo, L.; Bignozzi, I.; Cocchetto, R.; Cristalli, M.P.; Iannello, G. Immediate positioning of a definitive abutment versus repeated abutment replacements in post-extractive implants: 3-year follow-up of a randomised multicentre clinical trial. Eur. J. Oral Implantol. 2010, 3, 285–296. [Google Scholar] [PubMed]
- Herrero-Climent, M.; Díaz-Castro, C.M.; Fernández Chereguini, C.; Falcao, C.; Gil, F.J.; Ríos-Santos, J.V. Resonance frequency analysis by the Osstell system, using the transducer screwed to different healings abutments. Rev. Port. Estomatol. Med. Dent. Cir. Maxilofac. 2017, 58, 91–96. [Google Scholar]
- Hurwitz, E.E.; Simon, M.; Vinta, S.R.; Zehm, C.F.; Shabot, S.M.; Minhajuddin, A.; Abouleish, A.E. Adding examples to the ASA-Physical Status classification improves correct assignments to patients. Anesthesiology 2017, 126, 614–622. [Google Scholar] [CrossRef] [PubMed]
- Kästel, I.; de Quincey, G.; Neugebauer, J.; Sader, R.; Gehrke, P. Does the manual insertion torque of smartpegs affect the outcome of implant stability quotients (ISQ) during resonance frequency analysis (RFA)? Int. J. Implant. Dent. 2019, 5, 42. [Google Scholar] [CrossRef] [Green Version]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Jaramillo, R.; Santos, R.; Lázaro, P.; Romero, M.; Rios-Santos, J.V.; Bullón, P.; Fernández-Palacín, A.; Herrero-Climent, M. Comparative analysis of 2 resonance frequency measurement devices: Osstell Mentor and Osstell ISQ. Implant. Dent. 2014, 23, 351–356. [Google Scholar] [CrossRef] [Green Version]
- Gupta, R.K.; Padmanabhan, T.V. Resonance frequency analysis. Indian J. Dent. Res. 2011, 22, 567–573. [Google Scholar] [CrossRef]
- Lachmann, S.; Jäger, B.; Axmann, D.; Gomez-Roman, G.; Groten, M.; Weber, H. Resonance frequency analysis and damping capacity assessment. Part I: An in vitro study on measurement reliability and a method of comparison in the determination of primary dental implant stability. Clin. Oral Implant. Res. 2006, 17, 75–79. [Google Scholar] [CrossRef]
- Lages, F.S.; Willya Douglas-de-Oliveira, D.; Ibelli, G.S.; Assaf, F.; Queiroz, T.P.; Costa, F.O. Relationship between implant stability on the abutment and platform level by means of resonance frequency analysis: A cross-sectional study. PLoS ONE 2017, 24, e0181873. [Google Scholar] [CrossRef] [Green Version]
- Mandeville, P.B. El Coeficiente de Correlación de Intraclase (CCI). Cienc. UANL 2005, 3, 414–416. [Google Scholar]
- Tözum, T.F.; Turkyilmaz, I.; McGlumphy, E.A. Relationship between dental implant stability determined by resonance frequency analysis measurements and peri-implant vertical defects: An in vitro study. J. Oral Rehabil. 2008, 25, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Merheb, J.; Coucke, W.; Jacobs, R.; Naert, I.; Quirynen, M. Influence of bony defects on implant stability. Clin. Oral Implant. Res. 2010, 21, 919–923. [Google Scholar] [CrossRef]
- Lachmann, S.; Yves Laval, J.; Jäger, B.; Axmann, D.; Gomez-Roman, G.; Groten, M.; Weber, H. Resonance frequency analysis and damping capacity assessment. Part II: Peri-implant bone loss follow-up. An in vitro study with the Periotest and Ostell instruments. Clin. Oral Implant. Res. 2006, 17, 80–84. [Google Scholar] [CrossRef]
- Yang, S.M.; Shin, S.Y.; Kye, S.B. Relationship between implant stability measured by resonance frequency analysis (RFA) and bone loss during early healing period. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2008, 105, 12–19. [Google Scholar] [CrossRef]
- Monje, A.; Insua, A.; Monje, F.; Muñoz, F.; Salvi, G.E.; Buser, D.; Chappuis, V. Diagnostic accuracy of the implant stability quotient in monitoring progressive peri-implant bone loss: An experimental study in dogs. Clin. Oral Implant. Res. 2018, 29, 1016–1024. [Google Scholar] [CrossRef] [PubMed]
- Tözum, T.F.; Turkyilmaz, I.; Bal, B.T. Initial stability of two dental implants systems: Influence of buccolingual width and probe orientation on resonance frequency measurements. Clin. Implant. Dent. Relat. Res. 2010, 12, 194–201. [Google Scholar] [CrossRef]
- Gursoytrak, B.; Ataoglu, H. Use of resonance frequency analysis to evaluate the effects of surface properties on the stability of different implants. Clin. Oral Implant. Res. 2020, 31, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Ersanli, S.; Karabuda, C.; Beck, F.; Leblebicioglu, B. Resonance frequency analysis of one-stage dental implant stability during the osseointegration period. J. Periodontol. 2005, 76, 1066–1071. [Google Scholar] [CrossRef]
- Gallardo, Y.N.R.; da Silva-Olivio, I.R.; Gonzaga, L.; Sesma, N.; Martin, W. A Systematic Review of Clinical Outcomes on Patients Rehabilitated with Complete-Arch Fixed Implant-Supported Prostheses According to the Time of Loading. J. Prosthodont. 2019, 28, 958–968. [Google Scholar] [CrossRef]
- Raghavendra, S.; Wood, M.C.; Taylor, T.D. Early wound healing around endosseous implants: A review of the literature. Int. J. Oral Maxillofac. Implant. 2005, 20, 425–431. [Google Scholar]
- Barewal, R.M.; Oates, T.W.; Meredith, N.; Cochran, D.L. Resonance frequency measurement of implant stability in vivo on implants with a sandblasted and acid-etched surface. Int. J. Oral Maxillofac. Implant. 2003, 18, 641–651. [Google Scholar]
- Díaz-Castro, M.C.; Falcao, A.; López-Jarana, P.; Falcao, C.; Ríos-Santos, J.V.; Fernández-Palacín, A.; Herrero-Climent, M. Repeatability of the resonance frequency analysis values in implants with a new technology. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e636–e642. [Google Scholar] [CrossRef] [PubMed]
- García-Vives, N.; Andrés-García, R.; Rios-Santos, V.; Fernández-Palacín, A.; Bullón-Fernández, P.; Herrero-Climent, M.; Herrero-Climent, F. In vitro evaluation of the type of implant bed preparation with osteotomes in bone type IV and its influence on the stability of two implant systems. Med. Oral Patol. Oral Cir. Bucal 2009, 14, e455–e460. [Google Scholar] [PubMed]
- Maximiano Millán, A.; Bravo Álvarez, R.; Plana Montori, M.; Guerrero González, M.; Saura García-Martín, D.; Ríos-Carrasco, B.; Monticelli, F.; Ríos-Santos, J.V.; Fernández-Palacín, A. Assessment of the Simultaneous Use of Biomaterials in Transalveolar Sinus Floor Elevation: Prospective Randomized Clinical Trial in Humans. Int. J. Environ. Res. Public Health 2020, 17, 1888. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SmartPeg Screwed | Mesial | Distal | Buccal | Palatal/Lingual | ||||
|---|---|---|---|---|---|---|---|---|
| First | Repeated | First | Repeated | First | Repeated | First | Repeated | |
| Direct to implant | 7.147 ± 5.887 | 73.095 ± 5.866 | 72.914 ± 6.071 | 72.724 ± 6.278 | 71.698 ± 6.804 | 71.655 ± 6.836 | 72.138 ± 6.589 | 72.30138 ± 6.414 |
| To 2 mm abutment | 73.56 ± 6.57 | 73.483 ± 7.94 | 73.595 ± 6.542 | 73.24 ± 6.298 | 71.69 ± 8.205 | 72.112 ± 7.922 | 72.164 ± 7.097 | 72.793 ± 6.914 |
| To 3.5 mm abutment | 73.345 ± 6.409 | 73.207 ± 6.169 | 73.19 ± 6.482 | 72.845 ± 6.389 | 71.259 ± 8.02 | 71.362 ± 7.909 | 72.112 ± 6.995 | 71.802 ± 6.935 |
| To 5 mm abutment | 72.483 ± 6.239 | 72.345 ± 6.347 | 71.983 ± 6.911 | 72.103 ± 6.771 | 69.828 ± 9.651 | 69.819 ± 9.32 | 71.578 ± 6.966 | 71.526 ± 7.012 |
| Mesial | Distal | Buccal | Palatal/Lingual | |
|---|---|---|---|---|
| Direct to implant | 0.993 | 0.985 | 0.980 | 0.970 |
| (0.989–0.995) | (0.978–0.990) | (0.971–0.986) | (0.957–0.979) | |
| To 2 mm abutment | 0.841 | 0.982 | 0.973 | 0.972 |
| (0.771–0.890) | (0.975–0.998) | (0.962–0.982) | (0.959–0.980) | |
| To 3.5 mm abutment | 0.990 | 0.98 | 0.966 | 0.981 |
| (0.985–0.993) | (0.972–0.986) | (0.951–0.977) | (0.972–0.987) | |
| To 5 mm abutment | 0.993 | 0.993 | 0.986 | 0.979 |
| (0.990–0.995) | (0.990–0.995) | (0.980–0.991) | (0.970–0.986) |
| Mesial | Distal | Buccal | Palatal/Lingual | |
|---|---|---|---|---|
| 8 mm implant | 0.99 | 0.996 | 0.993 | 0.921 |
| (0.995–1.00) | (0.980–0.999) | (0.968–0.998) | (0.648–0.982) | |
| 10 mm implant | 0.992 | 0.979 | 0.968 | 0.965 |
| (0.986–0.995) | (0.996–0.987) | (0.948–0.980) | (0.943–0.979) | |
| 12 mm implant | 0.993 | 0.993 | 0.996 | 0.985 |
| (0.988–0.996) | (0.986–0.996) | (0.993–0.998) | (0.972–0.992) |
| Mesial | Distal | Buccal | Palatal/Lingual | |
|---|---|---|---|---|
| 3.5 mm | 0.995 | 0.970 | 0.949 | 0.958 |
| (0.992–0.997) | (0.947–0.983) | (0.909–0.971) | (0.926–0.977) | |
| 4 mm | 0.990 | 0.989 | 0.991 | 0.983 |
| (0.983–0.994) | (0.982–0.994) | (0.984–0.995) | (0.970–0.990) | |
| 4.5 mm | 0.996 | 0.995 | 0.994 | 0.941 |
| (0.989–0.999) | (0.986–0.998) | (0.984–0.998) | (0.831–0.979) |
| Mesial | Distal | Buccal | Palatal/lingual | |
|---|---|---|---|---|
| Direct to implant versus 2-mm abutment | 0.884 | 0.897 | 0.852 | 0.878 |
| (0.833–0.920) | (0.851–0.928) | (0.786–0.897) | (0.823–0.915) | |
| Direct to implant vs. 3.5-mm abutment | 0.924 | 0.921 | 0.845 | 0.906 |
| (0.891–0.948) | (0.885–0.945) | (0.776–0.892) | (0.865–0.935) | |
| Direct to implant vs. 5-mm abutment | 0.945 | 0.928 | 0.794 | 0.917 |
| (0.921–0.962) | (0.896–0.950) | (0.703–0.857) | (0.880–0.943) | |
| 2-mm versus 3.5-mm abutment | 0.945 | 0.977 | 0.983 | 0.962 |
| (0.921–0.962) | (0.967–0.984) | (0.976–0.988) | (0.945–0.974) | |
| 2-mm versus 5-mm abutment | 0.931 | 0.965 | 0.850 | 0.959 |
| (0.900–0.952) | (0.950–0.976) | (0.784–0.896) | (0.941–0.972) | |
| 3.5-mm versus 5-mm abutment | 0.976 | 0.972 | 0.863 | 0.972 |
| (0.966–0.984) | (0.959–0.980) | (0.803–0.905) | (0.960–0.981) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerrero-González, M.; Monticelli, F.; Saura García-Martín, D.; Herrero-Climent, M.; Ríos-Carrasco, B.; Ríos-Santos, J.-V.; Fernández-Palacín, A. Reliability of the Resonance Frequency Analysis Values in New Prototype Transepithelial Abutments: A Prospective Clinical Study. Int. J. Environ. Res. Public Health 2020, 17, 6733. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186733
Guerrero-González M, Monticelli F, Saura García-Martín D, Herrero-Climent M, Ríos-Carrasco B, Ríos-Santos J-V, Fernández-Palacín A. Reliability of the Resonance Frequency Analysis Values in New Prototype Transepithelial Abutments: A Prospective Clinical Study. International Journal of Environmental Research and Public Health. 2020; 17(18):6733. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186733
Chicago/Turabian StyleGuerrero-González, María, Francesca Monticelli, David Saura García-Martín, Mariano Herrero-Climent, Blanca Ríos-Carrasco, José-Vicente Ríos-Santos, and Ana Fernández-Palacín. 2020. "Reliability of the Resonance Frequency Analysis Values in New Prototype Transepithelial Abutments: A Prospective Clinical Study" International Journal of Environmental Research and Public Health 17, no. 18: 6733. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186733