Developing an Environmental Health Sciences COVID-19 Research Agenda: Results from the NIEHS Disaster Research Response (DR2) Work Group’s Modified Delphi Method

 ,
,
Abstract
:1. Introduction
The Need for Coordinated Disaster Research Response (DR2)
2. Materials and Methods
2.1. Step 1: Identify Diverse Experts
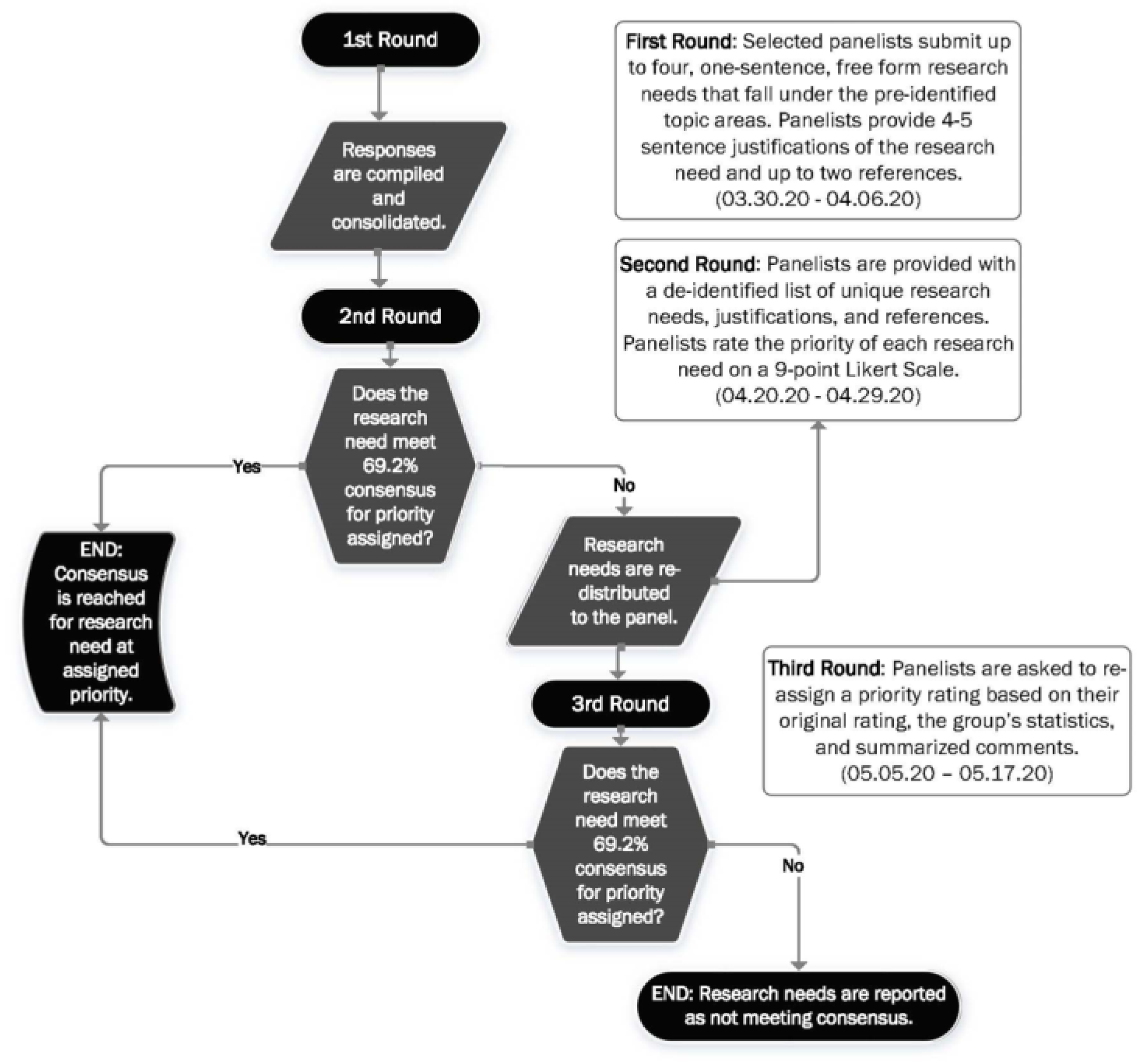
2.2. Step 2: Solicit Research Questions from Panelists
- Transmission and routes of exposure;
- Virus survival and infectivity;
- Personal protective equipment (PPE);
- Occupational health impacts and interventions;
- Environmental public health impacts and interventions;
- Environmental health risk communication;
- Cross-cutting areas.
2.3. Step 3: Panelists Rate Priority of Research Questions
2.4. Step 4: Panelists Re-rate Priority of Research Questions, Considering the Group’s Response
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 31 May 2020).
- Brainard, J. Scientists are Drowning in COVID-19 Papers. Can New Tools Keep Them Afloat? Available online: https://www.sciencemag.org/news/2020/05/scientists-are-drowning-covid-19-papers-can-new-tools-keep-them-afloat (accessed on 25 May 2020).
- Lurie, N.; Manolio, T.; Patterson, A.P.; Collins, F.; Frieden, T. Research as a Part of Public Health Emergency Response. N. Engl. J. Med. 2013, 368, 1251–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forum on Medical and Public Health Preparedness for Catastrophic Events; Board on Health Sciences Policy, Institute of Medicine. Science Preparedness: Conducting Research during Public Health Emergencies; National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Yeskey, K.; Miller, A. Science Unpreparedness. Disaster Med. Public Health Prep. 2015, 9, 444–445. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Sendai Framework for Disaster Risk Reduction 2015–2030; United Nations Office for Disaster Risk Reduction: Geneva, Switzerland, 2015. [Google Scholar]
- Japan and NIEHS Partner to Advance Disaster Research Response (Environmental Factor, October 2017). Available online: https://factor.niehs.nih.gov/2017/10/feature/feature-3-japan/index.htm (accessed on 31 May 2020).
- The CanDR2 Network: Improving Disaster Health Outcomes and Resilience through Data and Research|NCCEH. Available online: https://ncceh.ca/content/blog/candr2-network-improving-disaster-health-outcomes-and-resilience-through-data-and (accessed on 31 May 2020).
- Institute of Medicine. Preface; National Academies Press: Washington, DC, USA, 2010. [Google Scholar]
- Institute of Medicine, National Research Council. Research Priorities to Inform Public Health and Medical Practice for Ebola Virus Disease: Workshop in Brief; Reeve, M., Altevogt, B., Eds.; The National Academies Press: Washington, DC, USA, 2014. [Google Scholar]
- Institute of Medicine, National Academies of Sciences, Engineering; Medicine. Potential Research Priorities to Inform Public Health and Medical Practice for Domestic Zika Virus: Workshop in Brief; Snair, J., Hermann, J., Brown, L., Wollek, S., Balogh, E., Maxfield, K., Eds.; The National Academies Press: Washington, DC, USA, 2016. [Google Scholar]
- WHO. Blueprint; WHO R&D: 2020. Available online: https://www.who.int/research-observatory/analyses/rd_blueprint/en/ (accessed on 31 May 2020).
- A Coordinated Global Research Roadmap. Available online: https://www.who.int/publications/m/item/a-coordinated-global-research-roadmap (accessed on 6 July 2020).
- Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats. Research Topics Discussed; The National Academies of Science, Engineering, and Medicine: Washington, DC, USA, 2020. [Google Scholar]
- Keeney, S.; McKenna, H.; Hasson, F. The Delphi Technique in Nursing and Health Research; John Wiley & Sons, Incorporated: Hoboken, NJ, USA, 2011; ProQuest Ebook Central; Available online: https://0-ebookcentral-proquest-com.brum.beds.ac.uk/lib/washington/detail.action?docID=624638 (accessed on 5 September 2020).
- Dalkey, N.C. Delphi; Rand Corp: Santa Monica, CA, USA, 1967. [Google Scholar]
- RAND. Delphi Method. Available online: https://www.rand.org/topics/delphi-method.html (accessed on 8 May 2018).
- Environmental Health Sciences Core Centers. Available online: https://www.niehs.nih.gov/research/supported/centers/core/index.cfm (accessed on 31 May 2020).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNutt, M. A Community for Disaster Science. Science 2015, 348, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, D. How Swamped Preprint Servers Are Blocking Bad Coronavirus Research. Nature 2020, 581, 130–131. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Science, Engineering, and Medicine. Evidence-Based Practices for Public Health Emergency Preparedness and Response: Assessment of and Recommendations for the Field. Available online: https://www.nationalacademies.org/our-work/evidence-based-practices-for-public-health-emergency-preparedness-and-response-assessment-of-and-recommendations-for-the-field (accessed on 31 May 2020).
- National Academies of Science, Engineering, and Medicine. Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats. Rapid Expert Consultations on the COVID-19 Pandemic. Available online: https://www.nap.edu/read/25784/ (accessed on 31 May 2020).
- National Institutes of Health. Financial Conflict of Interest|grants.nih.gov. Available online: https://grants.nih.gov/grants/policy/coi/index.htm (accessed on 31 May 2020).
- Carbone, E.G.; Thomas, E.V. Science as the Basis of Public Health Emergency Preparedness and Response Practice: The Slow but Crucial Evolution. Am. J. Public Health 2018, 108, S383–S386. [Google Scholar] [CrossRef] [PubMed]
- Errett, N.A.; Haynes, E.N.; Wyland, N.; Everhart, A.; Pendergrast, C.; Parker, E.A. Assessing the National Capacity for Disaster Research Response (DR2) within the NIEHS Environmental Health Sciences Core Centers. Environ. Health 2019, 18, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Expertise | %(n) a |
|---|---|
| Environmental Toxicology | 23 (6) |
| Environmental Microbiology | 30.8 (8) |
| Exposure Sciences | 30.8 (8) |
| Environmental Epidemiology | 34.6 (9) |
| Environmental Public Health Practice | 19.4 (7) |
| Occupational Health | 42.3 (11) |
| Environmental Health Social Sciences | 8.7 (4) |
| Other b | 7.7 (2) |
| Questions that Reached Consensus in Round 2 | Ave Rating |
| What are the relative contributions of the different disease transmission routes for COVID-19 and how do they vary among exposure scenarios? | 7.62 |
| What environmental or occupational exposures might render an individual more susceptible to COVID-19 infection and/or progression of COVID-19-related illness? | 7.58 |
| What are the impacts on rates, severity, and outcomes of infection in environmental justice communities where concomitant exposure to contaminants may result in immunocompromised or otherwise increased sensitivity, and poverty and lack of infrastructure can limit ability to implement protective measures? | 7.42 |
| Where is SARS-CoV-2 in the environment, and how long does it remain infectious? | 7.35 |
| What is the particle size distribution for airborne particles carrying the virus? Does particle size (large droplet vs. small droplet nuclei) make a difference in probability of infection? | 7.31 |
| What is the role of HVAC/ventilation in the spread of virus? How can optimized airflow prevent the spread of airborne viruses at high occupancy places? | 7.19 |
| What are the real-world risks of infection via fomites on different types of surfaces? | 7.08 |
| What is the transmission potential during the initial incubation/asymptomatic phase? | 7.04 |
| What are the connections between air pollution, cardiorespiratory diseases, and SARS-CoV-2/COVID-19 severity? | 7.04 |
| What are the modes of transmission? Do the modes of transmission affect the severity of symptoms? | 6.85 |
| What are the effective public health measures to control the spread of COVID-19 and what has their impact on public health been? | 6.85 |
| What patient care activities put healthcare workers at risk of inhaling SARS-CoV-2? | 6.81 |
| What can be done to understand the communication needs for communities where education, culture, or language barriers make it difficult to implement effective control strategies to stop the spread of disease and reduce risk? | 6.73 |
| How do environmental exposures influence immune defenses and inflammation in the respiratory tract? | 6.69 |
| Questions that Reached Consensus in Round 3 | Ave Rating |
| What is the effect of the environment on transmission? | 7.73 |
| What are approaches that can be used to manage the epidemic in contexts where access to water, sanitation, and hygiene (WASH) is minimal (e.g., low-income countries, homeless populations)? | 7.69 |
| Droplet transmission of COVID-19 has been demonstrated. To what extent is aerosolization a mode of transmission, including (and especially) in the setting where an aerosolizing procedure is NOT being performed? | 7.62 |
| What are potential historical and/or concurrent environmental exposures modulating the severity of COVID-19 in different sub-populations? | 7.38 |
| How effective are face masks, and what are the risks of the general public using face masks in reducing community transmissions? | 7.31 |
| What are the impacts to those who were employed in minimum wage jobs thought to be extremely low risk, who became the front-line protectors in maintaining supply lines to a society in lockdown? | 7.19 |
| What are the co-factors for transmissibility and susceptibility, including role of spread by and to essential services workers? | 7.19 |
| How long does the airborne virus maintain infectivity? | 7.19 |
| Does air pollution (outdoor and indoor) increase the risk of morbidity and mortality in SARS-CoV-2/COVID-19? | 7.08 |
| How will meteorological variables (relative humidity, temperature, rainfall) and seasonality affect the epidemic? | 7.00 |
| What are the underlying risk factors for COVID-19? | 6.92 |
| What interventions could reduce the lung’s susceptibility to COVID-19 from such environmental or occupational exposures? | 6.88 |
| What is the interaction between chemical exposure and COVID-19 morbidity/mortality? | 6.81 |
| What are most effective models of risk communication for different segments of the population, given the divergent messages from various forms of media, the changing messages, and what are the expected outcomes of the messages? | 6.42 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Errett, N.A.; Howarth, M.; Shoaf, K.; Couture, M.; Ramsey, S.; Rosselli, R.; Webb, S.; Bennett, A.; Miller, A. Developing an Environmental Health Sciences COVID-19 Research Agenda: Results from the NIEHS Disaster Research Response (DR2) Work Group’s Modified Delphi Method. Int. J. Environ. Res. Public Health 2020, 17, 6842. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186842
Errett NA, Howarth M, Shoaf K, Couture M, Ramsey S, Rosselli R, Webb S, Bennett A, Miller A. Developing an Environmental Health Sciences COVID-19 Research Agenda: Results from the NIEHS Disaster Research Response (DR2) Work Group’s Modified Delphi Method. International Journal of Environmental Research and Public Health. 2020; 17(18):6842. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186842
Chicago/Turabian StyleErrett, Nicole A., Marilyn Howarth, Kimberley Shoaf, Megan Couture, Steven Ramsey, Richard Rosselli, Sara Webb, April Bennett, and Aubrey Miller. 2020. "Developing an Environmental Health Sciences COVID-19 Research Agenda: Results from the NIEHS Disaster Research Response (DR2) Work Group’s Modified Delphi Method" International Journal of Environmental Research and Public Health 17, no. 18: 6842. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186842