In Search of Concrete Outcomes—A Systematic Review on the Effectiveness of Educational Interventions on Reducing Acute Occupational Injuries


Abstract
:1. Introduction
2. Materials and Methods
2.1. Types of Studies
2.2. Types of Participants
2.3. Types of Interventions
2.4. Types of Outcome Measures
2.5. Exclusion Criteria
2.6. Information Sources
2.7. Selection of Studies
2.8. Data Extraction and Management
2.9. Assessment of Risk of Bias in Included Studies
2.10. Data Synthesis
3. Results
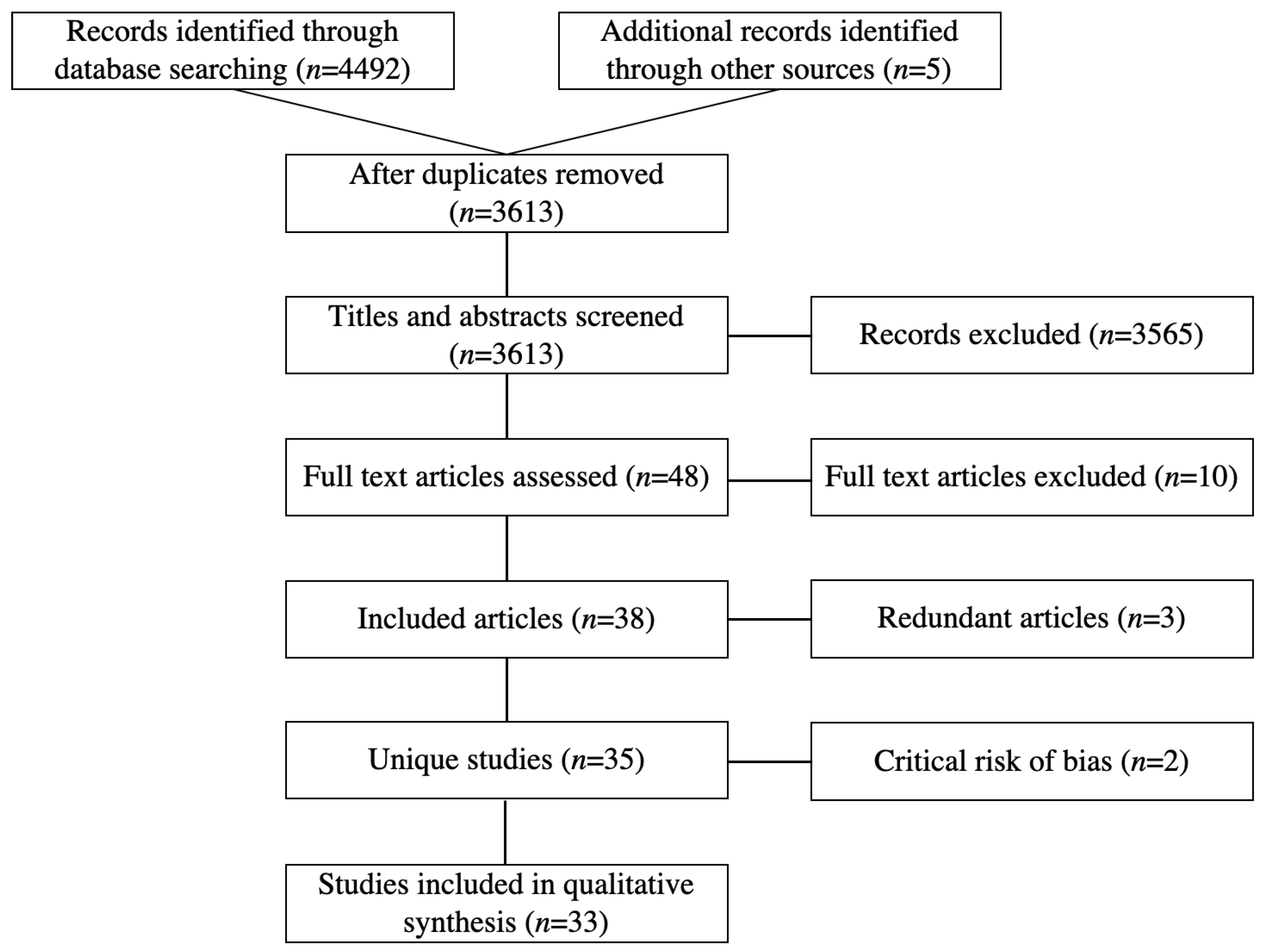
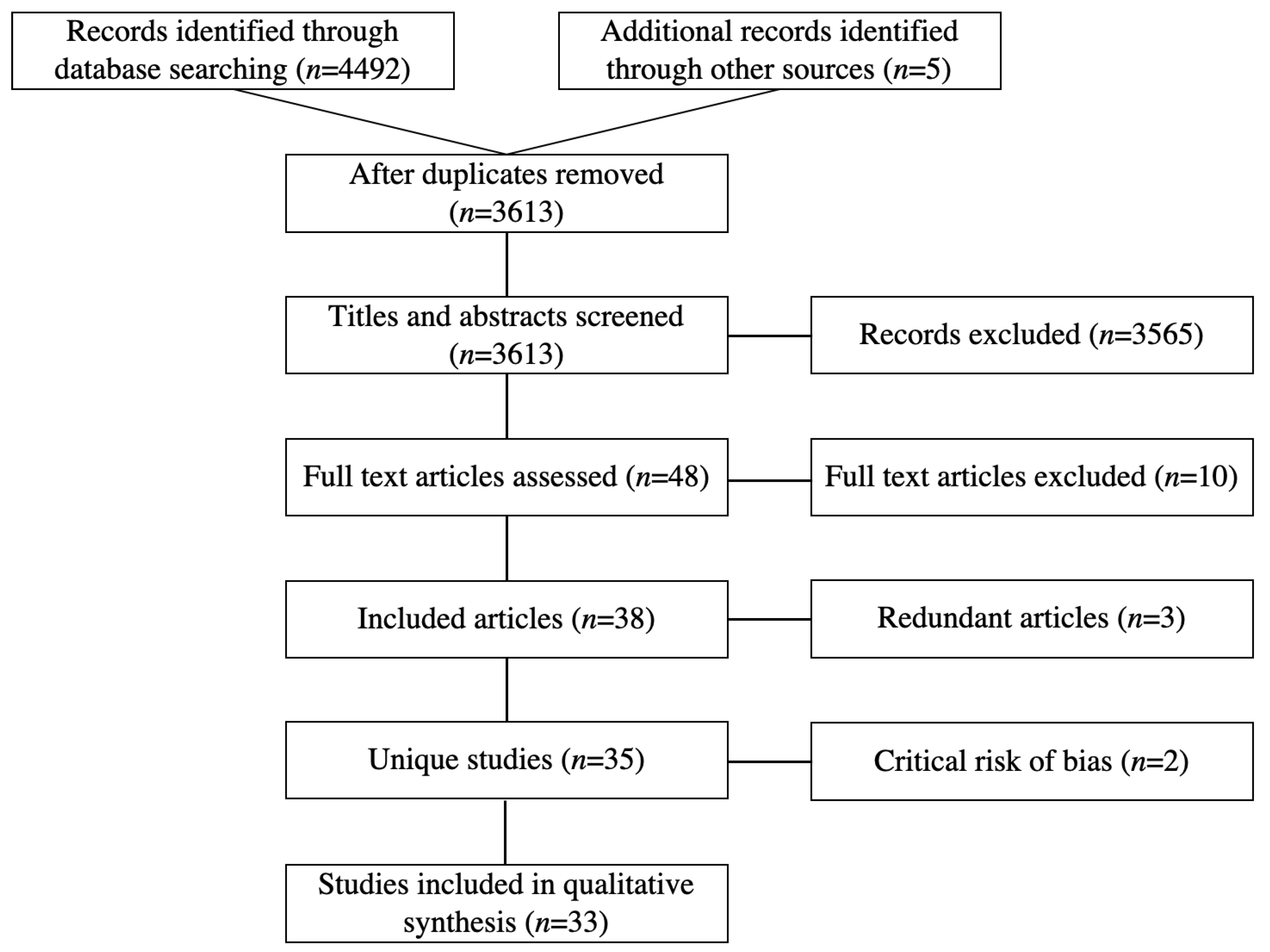
3.1. Results of the Search
3.2. Study Characteristics
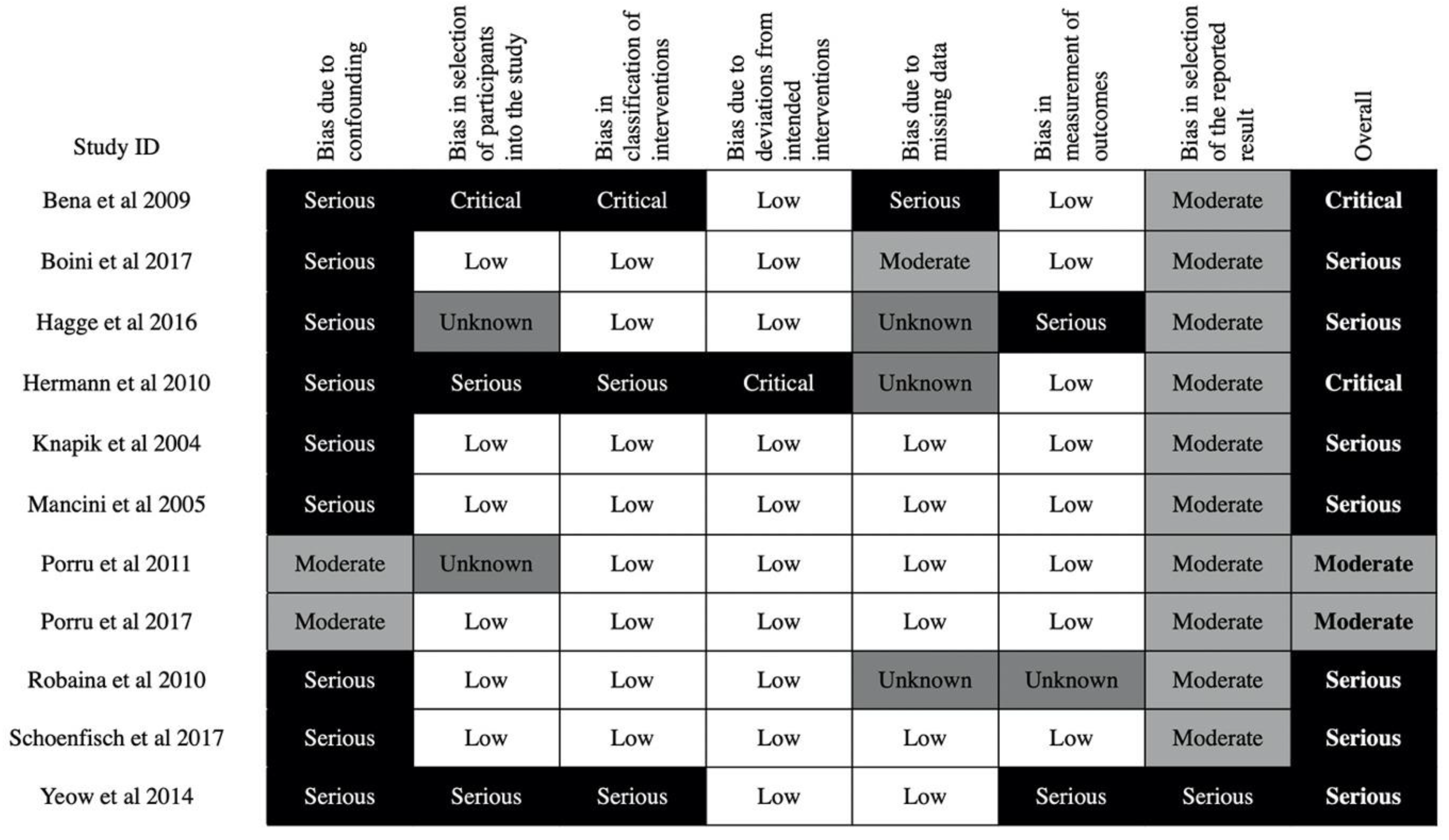
3.3. Risk of Bias in Included Studies
4. Discussion
4.1. Agriculture, Forestry, Fishing, and Hunting
4.2. Arts, Entertainment, and Recreation
4.3. Construction
4.4. Educational Services
4.5. Health Care and Social Assistance
4.6. Manufacturing
4.7. Mining, Quarrying, and Oil and Gas Extraction
4.8. Public Administration
4.9. Transportation and Warehousing
4.10. Utilities
4.11. Observations across Industries
4.12. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- #1. health education.mp. OR Health Education/OR primary prevention.mp. OR Primary Prevention/OR Health Promotion/OR social media.mp. OR Social Media/OR Marketing/OR Social Marketing/OR occupational health service.mp. OR Occupational Health Services/OR intervention.mp. OR educat*.mp. OR program*.mp.
- #2. work*.mp. OR occupation*.mp. OR employee.mp. OR industry.mp. OR Industry/OR agriculture.mp. OR Agriculture/OR farm*.mp. OR construction*.mp.
- #3. attitude*.mp. OR behavio*.mp. OR intention*.mp. OR belief*.mp. OR perception.mp. OR Perception/OR attitude to health.mp. OR Attitude to Health/OR Risk/OR Behavioral Risk Factor Surveillance System/OR Awareness/
- #4. occupational accident.mp. OR Accidents, Occupational/OR Insurance, Health/OR insurance claims.mp. OR absenteeism.mp. OR Absenteeism/OR Mortality/OR mortality risk.mp. OR (injur* adj3 reduction).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword, floating subheading word, candidate term word] OR (injur* adj3 prevention).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword, floating subheading word, candidate term word] OR (accident* adj3 reduction).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword, floating subheading word, candidate term word] OR (accident* adj3 prevention).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword, floating subheading word, candidate term word]
- #5. wounds.mp. OR “Wounds and Injuries”/OR hazard*.mp. OR fatality.mp. OR disability.mp. OR accident.mp. OR Accidents/OR death*.mp. OR injur*.mp.
- #6. #1 AND #2 AND #3 AND #4 AND #5
Appendix B

{kind=link}
{kind=link}
{kind=link}
| Study | Reason(s) for Exclusion |
|---|---|
| Bahn S, Barratt-Pugh L. Evaluation of the mandatory construction induction training program in Western Australia: unanticipated consequences. Eval Program Plann. 2012; 35(3): 337–43. [65] | Injury outcomes were not quantified |
| Sarma BP. Prevention of burns: 13 years’ experience in Northeastern India. Burns. 2011; 37(2): 265–72. [66] | Interventions and outcomes are not specific to the occupational setting |
| de Boer AGEM, Burdorf A, van Duivenbooden C, Frings-Dresen MHW. The effect of individual counselling and education on work ability and disability pension: a prospective intervention study in the construction industry. Occup Environ Med. 2007; 64(12): 792–7. [67] | The study measured disability as an outcome, but it didn’t specify if this referred to disability due to acute injuries, chronic exertion, or non-physical causes |
| Donham KJ, Lange JL, Kline A, Rautiainen RH, Grafft L. Prevention of occupational respiratory symptoms among certified safe farm intervention participants. J Agromedicine. 2010; 16(1): 40–51. [68] | The study only measured organic dust toxic syndrome, which should be classified as an occupational disease instead of occupational injury |
| Donham KJ, Rautiainen RH, Lange JL, Schneiders S. Injury and illness costs in the Certified Safe Farm study. J Rural Health. 2007; 23(4): 348–55. [69] | Same study as Rautiainen et al. 2004 [12] |
| Hagel LM, Pickett W, Pahwa P, Day L, Brison RJ, Marlenga B, et al. Prevention of agricultural injuries: an evaluation of an education-based intervention. Inj Prev. 2008 Oct 1; 14(5): 290–5. [70] | This was a cross-sectional survey, which was not one of the study types listed in our inclusion criteria |
| Melamed S, Oksenberg A. Excessive daytime sleepiness and risk of occupational injuries in non-shift daytime workers. Sleep. 2002; 25(3): 315–21. [71] | Did not provide sufficient injury outcome data |
| Taylor EL. Safety benefits of mandatory OSHA 10 h training. Saf Sci. 2015; 77: 66–71. [72] | Legislative intervention |
| Trinh MT. Developing Resilient Safety Culture for Construction Projects in Vietnam. Western Sydney University (Australia); 2018. [73] | Not an educational intervention |
| Vieira F. Importance of the sleepiness and fatigue prevention for reducing occupational accidents in a Brazilian mining company. Sleep Med. 2011; 12(Suppl 1): S21–2. [74] | The intervention has very few educational components, which are also vaguely defined. Moreover, the study only measured equipment downtime and unmet production due to drowsiness, which are not sufficiently reliable outcomes according to our inclusion criteria |
| Young S. From zero to hero. A case study of industrial injury reduction: New Zealand Aluminium Smelters Limited. Saf Sci. 2014; 64: 99–108. [75] | The behavioral component is a very small proportion of the intervention and it’s not consistently implemented |
| Yu W. Evaluating the Effectiveness of Participatory Training for Occupational Health and Safety Improvements—A Randomized Controlle Trial with One-year Follow-up in China. ProQuest Dissertations and Theses. The Chinese University of Hong Kong (Hong Kong); 2010. [76] | Same study as Yu et al. 2017 [30] |
| Yu I, Yu W, Li Z. The effectiveness of participatory training on reduction of occupational injuries: A randomised controlled trial. Occup Environ Med. 2011; 68(Suppl 1): S24–5. [77] | Same study as Yu et al. 2017 [30] |
Appendix C
| Study ID | Disclosures |
|---|---|
| Rasmussen et al., 2003 [26] | Funded by grants from the Danish Insurance Association, The Work Environment Fund, The Health Fund of the Danish Ministry of Health, and the Public Health Research Fund of the counties of Ribe and Ringkoebing, Denmark. COI information not provided |
| Vercruysse et al., 2016 [27] | Supported by Flemish Policy Research Centre on Sports; authors declared no COI |
| Sullivan et al., 2017 [28] | Funded by Federal Emergency Management Agency (FEMA) Assistance for Firefighters grants EMW-2007-FP-02197 and EMW-2008-FP-02566; National Institute of Occupational Safety and Health grant 1R01OH010300-02; National Institutes of Health National Heart, Lung, and Blood Institute grant R01NS054277; and an endowed professorship provided to Harvard Medical School by Cephalon, Inc. Some researchers had lecture fees, previous research support, association with various organizations, and consulting histories |
| Rautiainen et al., 2004 [29] | The Certified Safe Farm study was funded by NIOSH (Grant No. U06/CCU712913), the Iowa Wellmark Foundation, Pioneer Hi-Bred International, Inc., the Iowa Pork Producers Council, the National Pork Producer’s Council, and Iowa’s Injury Prevention Research Center. COI information not provided |
| Yu et al., 2017 [30] | Funded by the Chinese University of Hong Kong, the Hong Kong Workers’ Health Center and the Shenzhen Hospital for Occupational Disease Control and Prevention; authors declared no COI |
| Morgan et al., 2012 [31] | Supported by the Hunter Medical Research Institute and funded by Tomago Aluminium and the Hunter Medical Research Institute. Tomago had no involvement in study design, analysis, and interpretation of data, or the decision to submit the manuscript for publication. S.M. from Tomago Aluminium reviewed the drafted manuscript for accuracy and also organized the data collection at Tomago and assisted with recruitment |
| Adams et al., 2013 [32] | This trial was funded by an intra-mural research grant from the Fluid Research Fund of the Christian Medical College, Vellore, administered through the Office of Research. Protective eyewear was funded by a project grant from the Christoffel-Blindenmission (CBM) to the Department of Ophthalmology, Christian Medical College, Vellore. The funding sources had no role in the design, conduct, or reporting of this trial; authors declared no COI |
| Geller et al., 2001 [33] | Centers for Disease Control and Prevention, Grant U56-CCU 914658. No info on COI |
| Hagge et al., 2016 [34] | None provided |
| Robaina et al., 2010 [35] | “Drs. Robaina and Ávila are members of the Scientific Council of the National Institute of Workers’ Health, Cuba. Dr. Partanen declares no conflicts of interest.” |
| Hermann et al., 2010 [36] | None provided |
| Mancini et al., 2005 [37] | No information on funding, no competing interests |
| Yeow et al., 2014 [38] | None provided |
| Kidd et al., 2000 [39] | Grant-Number-R01-CCR-413067 |
| Borger et al., 2011 [40] | None provided |
| Bena et al., 2009 [41] | This work was supported by a grant from the Regione Piemonte. COI not provided |
| Porru et al., 2011 [42] | Authors declared no COI, no information about grants |
| Porru et al., 2017 [43] | Association of Italian Foundries (ASSOFOND) provided “assistance and support.” Otherwise no COI or grants mentioned. |
| Knapik et al., 2004 [44] | None provided |
| Boini et al., 2017 [45] | This research received no specific grant from any funding agency in the public, commercial or non-profit sectors; authors declared no COI |
| Schoenfisch et al., 2017 [46] | Funding by CPWR—The Center for Construction Research and Training-through cooperative agreement number U60-OH009762 from the National Institute of Occupational Safety and Health (NIOSH). Authors declared no COI. |
| Koblesky et al., 2015 [47] | Author declared no grants COI and no commercial COI |
| Gatti et al., 2013 [48] | None provided |
| Williams et al., 2010 [53] | Funded by the Center for Construction Research and Training – CPWR through a grant from NIOSH. The lead author was supported in part by the Center for Disease Control and Prevention (CDC), Training Program Grant # 5 T01 CD000189-05. |
| Shouman et al., 2002 [54] | None provided |
| Nunu et al., 2018 [55] | Authors declared no “significant financial support... that could have influenced its outcome” |
| Day 2002 [56] | None provided, except that the lead author worked at the mill of intervention |
| Howard et al., 2009 [57] | Funding: Worksafe Victoria, Transport Accident Commission. No information on conflicts of interest |
| Badmos et al., 2018 [58] | None provided |
| Johnson et al., 2002 [59] | None provided |
| Kowalski- Trakofler et al., 2003 [60] | None provided |
| Salminen 2008 [49] | None provided |
| Evanoff et al., 2016 [50] | Funding by the Center for Construction Research and Training through the National Institute of Occupational Safety and Health (U54 OH00830 and U60 OH009762) and the Washington University Institute of Clinical and Translational Sciences grant UL1 TR000448 from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH). Authors declared no financial COI |
| Darragh et al., 2004 [51] | Funding by the US Department of Labor, Occupational Safety and Health Administration (OSHA) through a cooperative agreement with the Technical Assistance and Training Corporation, Washington, DC. No info on COI |
| Spangenberg et al., 2002 [52] | Commissioned by the owner of the construction site (A/S Øresundsforbindelsen) |
References
- Hämäläinen, P.; Takala, J.; Kiat, T.B. Global Estimates of Occupational Accidents and Work-Related Illnesses 2017; Workplace Safety and Health Institute: Singapore, 2017. [Google Scholar]
- Takala, J.; Hämäläinen, P.; Saarela, K.L.; Yun, L.Y.; Manickam, K.; Jin, T.W.; Heng, P.; Tjong, C.; Kheng, L.G.; Lim, S. Global estimates of the burden of injury and illness at work in 2012. J. Occup. Environ. Hyg. 2014, 11, 326–337. [Google Scholar] [CrossRef] [PubMed]
- International Labour Organization Global Trends on Occupational Accidents and Diseases. Available online: https://www.ilo.org/legacy/english/osh/en/story_content/external_files/fs_st_1-ILO_5_en.pdf (accessed on 14 August 2019).
- Pike, I.; Richmond, S.; Rothman, L.; Macpherson, A. (Eds.) Canadian Injury Prevention Resource; Parachute: Toronto, ON, Canada, 2015. [Google Scholar]
- Lund, J.; Aarø, L.E. Accident prevention. Presentation of a model placing emphasis on human, structural and cultural factors. Saf. Sci. 2004, 42, 271–324. [Google Scholar] [CrossRef]
- Munro, J.; Coleman, P.; Nicholl, J.; Harper, R.; Kent, G.; Wild, D. Can we prevent accidental injury to adolescents? A systematic review of the evidence. Inj. Prev. 1995, 1, 249–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeRoo, L.A.; Rautiainen, R.H. A systematic review of farm safety interventions. Am. J. Prev. Med. 2000, 18, 51–62. [Google Scholar] [CrossRef]
- McCallum, D.M.; Murphy, S.; Reed, D.B.; Claunch, D.T.; Reynolds, S.J. What we know about the effectiveness of farm safety day programs and what we need to know. J. Rural Heal. 2013, 29, 20–29. [Google Scholar] [CrossRef]
- Ruotsalainen, J.H.; Verbeek, J.H.; Salmi, J.A.; Jauhiainen, M.; Laamanen, I.; Pasternack, I.; Husman, K. Evidence on the effectiveness of occupational health interventions. Am. J. Ind. Med. 2006, 49, 865–872. [Google Scholar] [CrossRef]
- Van der Molen, H.F.; Lehtola, M.M.; Lappalainen, J.; Hoonakker, P.L.T.; Hsiao, H.; Haslam, R.; Hale, A.R.; Frings-Dresen, M.H.W.; Verbeek, J.H. Interventions to prevent injuries in construction workers. Cochrane database Syst. Rev. 2012, 12, CD006251. [Google Scholar] [CrossRef]
- Rautiainen, R.; Lehtola, M.M.; Day, L.M.; Schonstein, E.; Suutarinen, J.; Salminen, S.; Verbeek, J.H. Interventions for preventing injuries in the agricultural industry. Cochrane Database Syst. Rev. 2008. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Non-randomised Controlled Study (NRS) Designs. Available online: https://childhoodcancer.cochrane.org/non-randomised-controlled-study-nrs-designs (accessed on 8 May 2019).
- Baker, S.P.; Ginsburg, M.J.; O’Neill, B.; Li, G. The Injury Fact Book; Oxford University Press: Oxford, UK, 1992; ISBN 0195061942. [Google Scholar]
- Peden, M.; McGee, K.; Sharma, G. The Injury Chart Book: A Graphical Overview of the Global Burden of Injuries; World Health Organization: Geneva, Switzerland, 2002; ISBN 924156220X. [Google Scholar]
- Katz, L.F.; Margo, R.A. Technical change and the relative demand for skilled labor: The united states in historical perspective. In Human Capital in History: The American Record; University of Chicago Press: Chicago, IL, USA, 2014; pp. 15–57. [Google Scholar]
- David, H. Why are there still so many jobs? The history and future of workplace automation. J. Econ. Perspect. 2015, 29, 3–30. [Google Scholar]
- Committee to Assess Training Needs for Occupational Safety and Health Personnel in the United States. Safe Work in the 21st Century: Education and Training Needs for the Next decade’s Occupational Safety and Health Personnel; National Academies Press: Washington, DC, USA, 2000; ISBN 0309070260. [Google Scholar]
- Cox, A.R.; Williamson, G.C. Job security for occupational health and safety professionals in the 21st century: What you need to know about the Institute of Medicine (2000) report. Aaohn J. 2001, 49, 169–170. [Google Scholar] [CrossRef] [PubMed]
- Scherer, R.W.; Langenberg, P.; Von Elm, E. Full publication of results initially presented in abstracts. Cochrane Database Syst. Rev. 2005. [Google Scholar] [CrossRef]
- North American Industry Classification System (NAICS) Canada 2017 Version 1.0. Available online: http://www23.statcan.gc.ca/imdb/p3VD.pl?Function=getVD&TVD=307532 (accessed on 9 May 2019).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, I4919. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- National Safety Council Industry Incidence and Rates—Industry Profiles. Available online: https://injuryfacts.nsc.org/work/industry-incidence-rates/industry-profiles/ (accessed on 28 July 2019).
- Rasmussen, K.; Carstensen, O.; Lauritsen, J.M.; Glasscock, D.J.; Hansen, O.N.; Jensen, U.F. Prevention of farm injuries in Denmark. Scand. J. Work. Environ. Heal. 2003, 29, 288–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vercruysse, S.; Haerens, L.; Verhagen, E.; Goossens, L.; De Clercq, D. Effects of a multifactorial injury prevention intervention in physical education teachers: A randomized controlled trial. Eur. J. Sport Sci. 2016, 16, 868–876. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.P.; O’Brien, C.S.; Barger, L.K.; Rajaratnam, S.M.W.; Czeisler, C.A.; Lockley, S.W.; Harvard Work Hours, Health and Safety Group. Randomized, prospective study of the impact of a sleep health program on firefighter injury and disability. Sleep 2017, 40, zsw001. [Google Scholar] [CrossRef] [Green Version]
- Rautiainen, R.H.; Lange, J.L.; Hodne, C.J.; Schneiders, S.; Donham, K.J. Injuries in the Iowa certified safe farm study. J. Agric. Saf. Health 2004, 10, 51–63. [Google Scholar] [CrossRef]
- Yu, I.T.S.; Yu, W.; Li, Z.; Qiu, H.; Wan, S.; Xie, S.; Wang, X. Effectiveness of participatory training in preventing accidental occupational injuries: A randomized-controlled trial in China. Scand. J. Work. Environ. Health 2017, 43, 226–233. [Google Scholar] [CrossRef]
- Morgan, P.J.; Collins, C.E.; Plotnikoff, R.C.; Cook, A.T.; Berthon, B.; Mitchell, S.; Callister, R. The impact of a workplace-based weight loss program on work-related outcomes in overweight male shift workers. J. Occup. Environ. Med. 2012, 54, 122–127. [Google Scholar] [CrossRef]
- Adams, J.S.K.; Raju, R.; Solomon, V.; Samuel, P.; Dutta, A.K.; Rose, J.S.; Tharyan, P. Increasing compliance with protective eyewear to reduce ocular injuries in stone-quarry workers in Tamil Nadu, India: A pragmatic, cluster randomised trial of a single education session versus an enhanced education package delivered over six months. Injury 2013, 44, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Geller, A.C.; Glanz, K.; Shigaki, D.; Isnec, M.R.; Sun, T.; Maddock, J. Impact of skin cancer prevention on outdoor aquatics staff: The Pool Cool program in Hawaii and Massachusetts. Prev Med 2001, 33, 155–161. [Google Scholar] [CrossRef]
- Hagge, M.; McGee, H.; Matthews, G.; Aberle, S. Behavior-based safety in a coal mine: The relationship between observations, participation, and injuries over a 14-year period. J. Organ. Behav. Manage. 2017, 37, 107–118. [Google Scholar] [CrossRef]
- Robaina, C.; Partanen, T.J.; Avila, I. A program for the reduction of occupational injuries and changes in safety culture among stevedores at Port of Havana, Cuba. Int. J. Occup. Environ. Health 2010, 16, 312–319. [Google Scholar] [CrossRef]
- Hermann, J.A.; Ibarra, G.V.; Hopkins, B.L. A safety program that integrated behavior-based safety and traditional safety methods and its effects on injury rates of manufacturing workers. J. Organ. Behav. Manage. 2010, 30, 6–25. [Google Scholar] [CrossRef]
- Mancini, G.; Baldasseroni, A.; Laffi, G.; Curti, S.; Mattioli, S.; Violante, F.S. Prevention of work related eye injuries: Long term assessment of the effectiveness of a multicomponent intervention among metal workers. Occup. Environ. Med. 2005, 62, 830–835. [Google Scholar] [CrossRef]
- Yeow, P.H.P.; Goomas, D.T. Outcome-and-behavior-based safety incentive program to reduce accidents: A case study of a fluid manufacturing plant. Saf. Sci. 2014, 70, 429–437. [Google Scholar] [CrossRef]
- Kidd, P.; Struttmann, T.; Parshall, M.; Wojcik, S. Loss Education to Reduce Construction–Related Injuries; Kentucky Injury Prevention and Research Center: Atlanta, GA, USA, 2000. [Google Scholar]
- Borger, J.; Sun, Y.; Bochmann, F.; Guldner, K.; Ponto, K. Reduction of occupational injuries by conduction of a preventive training programme - An epidemiological follow-up study in the German glass industry. Occup. Environ. Med. 2011, 68, S25. [Google Scholar] [CrossRef] [Green Version]
- Bena, A.; Berchialla, P.; Coffano, M.E.; Debernardi, M.L.; Icardi, L.G. Effectiveness of the training program for workers at construction sites of the high-speed railway line between Torino and Novara: Impact on injury rates. Am. J. Ind. Med. 2009, 52, 965–972. [Google Scholar] [CrossRef]
- Porru, S.; Calza, S.; Arici, C. An effectiveness evaluation of a multifaceted preventive intervention on occupational injuries in foundries: A 13-year follow-up study with interrupted time series analysis. Int. Arch. Occup. Environ. Health 2011, 84, 867–876. [Google Scholar] [CrossRef]
- Porru, S.; Calza, S.; Arici, C. Prevention of occupational injuries: Evidence for effective good practices in foundries. J. Safety Res. 2017, 60, 53–69. [Google Scholar] [CrossRef] [PubMed]
- Knapik, J.J.; Bullock, S.H.; Toney, E.; Wells, J.D.; Hoedebecke, E.; Jones, B.H. Influence of an injury reduction program on injury and fitness outcomes among soldiers. Inj. Prev. 2004, 10, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Boini, S.; Colin, R.; Grzebyk, M. Effect of occupational safety and health education received during schooling on the incidence of workplace injuries in the first 2 years of occupational life: A prospective study. BMJ Open 2017, 7, e015100. [Google Scholar] [CrossRef]
- Schoenfisch, A.L.; Lipscomb, H.; Sinyai, C.; Adams, D. Effectiveness of OSHA Outreach Training on carpenters’ work-related injury rates, Washington State 2000–2008. Am. J. Ind. Med. 2017, 60, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Koblesky, N. Workers compensation E-Mod factor improves through actionable measures. Transfusion 2015, 55, S228–S229. [Google Scholar]
- Gatti, M.; Valdina, A.; Tosolin, F.; Arezes, P.; Baptista, J.S.; Barroso, M.P.; Carneiro, P.; Costa, N.; Melo, R.; Miguel, A.S.; et al. The reduction of injuries due to the Behavior-Based Safety processes implemented in several plants and sites A collection of case studies reviews the results obtained from behavior analysis applied to industrial environment. In Proceedings of the Occupational Safety and Hygiene, Guimarães, Portugal, 12 February 2013; pp. 216–218. [Google Scholar]
- Salminen, S. Two interventions for the prevention of work-related road accidents. Saf. Sci. 2008, 46, 545–550. [Google Scholar] [CrossRef]
- Evanoff, B.; Dale, A.; Zeringue, A.; Fuchs, F.; Gaal, J.; Lipscomb, H.J. Results of a fall prevention educational intervention for residential construction. Saf. Sci. 2016, 89, 301–307. [Google Scholar] [CrossRef] [Green Version]
- Darragh, A.R.; Stallones, L.; Bigelow, P.L.; Keefe, T.J. Effectiveness of the HomeSafe Pilot Program in reducing injury rates among residential construction workers, 1994-1998. Am. J. Ind. Med. 2004, 45, 210–217. [Google Scholar] [CrossRef]
- Spangenberg, S.; Mikkelsen, K.L.; Kines, P.; Dyreborg, J. The construction of the Oresund link between Denmark and Sweden: The effect of a multi-faceted safety campaign. Saf. Sci. 2002, 40, 457–465. [Google Scholar] [CrossRef]
- Williams, Q., Jr.; Ochsner, M.; Marshall, E.; Kimmel, L.; Martino, C. The impact of a peer-led participatory health and safety training program for Latino day laborers in construction. J. Safety Res. 2010, 41, 253–261. [Google Scholar] [CrossRef]
- Shouman, A.E.; El-Damaty, S.I.; Bakr, I.; Mukhtar, A.; Kamal, A.M. Accident prevention program in a glass factory in Shoubra El Khema district. J. Egypt. Public Health Assoc. 2002, 77, 73–99. [Google Scholar] [PubMed]
- Nunu, W.; Tendai, k.; Phakamani, M. An evaluation of the effectiveness of the Behaviour Based Safety Initiative card system at a cement manufacturing company in Zimbabwe. Saf. Health Work 2018, 9, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Day, R.C. Changing a Corporate Culture: Implementing Safety Leadership at a Pulp and Paper mill; St. Francis Xavier University: Ann Arbor, MI, USA, 2002. [Google Scholar]
- Howard, M.; Wilson, J.; Hare, D.; Swann, P. Health break - Sleep disorders screening in road transport. Sleep Biol. Rhythms 2009, 7, S14. [Google Scholar] [CrossRef]
- Badmos, E. Accident prevention: From vision to action through “harm to zero” concept. Occup. Environ. Med. 2018, 75, S31. [Google Scholar] [CrossRef]
- Johnson, K.A.; Ruppe, J. A job safety program for construction workers designed to reduce the potential for occupational injury using tool box training sessions and computer-assisted biofeedback stress management techniques. Int. J. Occup. Saf. Ergon. 2002, 8, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Kowalski-Trakofler, K.M.; Barrett, E.A. The concept of degraded images applied to hazard recognition training in mining for reduction of lost-time injuries. J. Safety Res. 2003, 34, 515–525. [Google Scholar] [CrossRef] [PubMed]
- National Safety Council Work Safety Introduction. Available online: https://injuryfacts.nsc.org/work/work-overview/work-safety-introduction/ (accessed on 11 July 2019).
- The World Bank World Development Report 2008: Agriculture for Development. Available online: http://siteresources.worldbank.org/INTWDRS/Resources/477365-1327599046334/WDR_00_book.pdf (accessed on 11 July 2019).
- Lipscomb, H.J.; Li, L.; Dement, J. Work-related falls among union carpenters in Washington State before and after the Vertical Fall Arrest Standard. Am. J. Ind. Med. 2003, 44, 157–165. [Google Scholar] [CrossRef]
- Cagno, E.; Micheli, G.J.L.; Jacinto, C.; Masi, D. An interpretive model of occupational safety performance for Small-and Medium-sized Enterprises. Int. J. Ind. Ergon. 2014, 44, 60–74. [Google Scholar] [CrossRef]
- Bahn, S.; Barratt-Pugh, L. Evaluation of the mandatory construction induction training program in Western Australia: Unanticipated consequences. Eval. Program Plann. 2012, 35, 337–343. [Google Scholar] [CrossRef]
- Sarma, B.P. Prevention of burns: 13 years’ experience in Northeastern India. Burns 2011, 37, 265–272. [Google Scholar] [CrossRef]
- De Boer, A.G.E.M.; Burdorf, A.; van Duivenbooden, C.; Frings-Dresen, M.H.W. The effect of individual counselling and education on work ability and disability pension: A prospective intervention study in the construction industry. Occup. Environ. Med. 2007, 64, 792–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donham, K.J.; Lange, J.L.; Kline, A.; Rautiainen, R.H.; Grafft, L. Prevention of occupational respiratory symptoms among certified safe farm intervention participants. J. Agromedicine 2010, 16, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Donham, K.J.; Rautiainen, R.H.; Lange, J.L.; Schneiders, S. Injury and illness costs in the Certified Safe Farm study. J. Rural Health 2007, 23, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Hagel, L.M.; Pickett, W.; Pahwa, P.; Day, L.; Brison, R.J.; Marlenga, B.; Crowe, T.; Snodgrass, P.; Ulmer, K.; Dosman, J.A. Prevention of agricultural injuries: An evaluation of an education-based intervention. Inj. Prev. 2008, 14, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Melamed, S. Excessive daytime sleepiness and risk of occupational injuries in non-shift daytime workers. Sleep 2002, 25, 315–321. [Google Scholar] [CrossRef] [Green Version]
- Taylor, E.L. Safety benefits of mandatory OSHA 10 h training. Saf. Sci. 2015, 77, 66–71. [Google Scholar] [CrossRef] [Green Version]
- Trinh, M.T. Developing Resilient Safety Culture for Construction Projects in Vietnam; Western Sydney University (Australia): Sydney, NSW, Australia, 2018. [Google Scholar]
- Vieira, F. Importance of the sleepiness and fatigue prevention for reducing occupational accidents in a Brazilianmining company. Sleep Med. 2011, 12, S21–S22. [Google Scholar] [CrossRef]
- Young, S. From zero to hero. A case study of industrial injury reduction: New Zealand Aluminium Smelters Limited. Saf. Sci. 2014, 64, 99–108. [Google Scholar] [CrossRef]
- Yu, W. Evaluating the Effectiveness of Participatory Training for Occupational Health and Safety Improvements—A Randomized Controlle Trial with One-year Follow-up in China; The Chinese University of Hong Kong (Hong Kong): Hong Kong, China, 2010. [Google Scholar]
- Yu, I.; Yu, W.; Li, Z. The effectiveness of participatory training on reduction of occupational injuries: A randomised controlled trial. Occup. Environ. Med. 2011, 68, S24–S25. [Google Scholar] [CrossRef] [Green Version]

| Population/Problem | Intervention | Context | Outcome |
|---|---|---|---|
| Injury | Education | Work | Injury prevention |
| Wounds | Program | Occupation | Injury reduction |
| Fatality | Social Marketing | Employee | Insurance claims |
| Disability | Primary Prevention | Industry | Absenteeism |
| Agriculture, forestry, fishing and hunting. | Study ID | Type of Study | Participants | Timeframe | Intervention(s) and Control (If Applicable) | Outcomes |
| Rasmussen et al., 2003 [26] | RCT randomized at the farm level | Farmers in Denmark Intervention: 99 farms, n = 498 Control: 102 farms, n = 492 | Duration: November 1995 to July 1997 Extended follow up: N/A | Safety audits with feedback, and a 1-day safety course featuring didactic and participatory education; controls received no safety course | No significant effect in preventing injuries compared to control, even when adjusting for seasonal variation—30% reduction in injury rate (95% CI: 21% increase—60% reduction) | |
| Rautiainen et al., 2004 [29] | Matched pairs cluster RCT, randomized at the farm level | Farmers in the USA Intervention: n = 152 farms Control: n = 164 farms | Duration: 1998 to 2003 Extended follow up: N/A | Annual clinical screening, access to didactic materials, and a monetary incentive for farmers who received a safety audit score; controls received no intervention | No significant effect in preventing injuries compared to control, even when adjusting for confounding factors—rate ratio of injury rates (intervention vs. control) was 1.08 (96% CI: 0.86–1.37) | |
| Arts, Entertainment, & Recreation | Geller et al., 2001 [33] | Matched-pairs cluster RCT, randomized at the pool level | Pool staff in the USA Intervention: n = 142 Control: n = 78 | Duration: summer 1999 Extended follow up: N/A | Didactic education on sunburns and skin cancer, plus engineering and personal protective equipment support; the control group received placebo intervention on child injury prevention. | Significant effect in preventing sunburns compared to control—1.42 was the average number of sunburns among intervention participants, and 2.07 among control participants (p < 0.05) |
| Construction | Bena et al., 2009 [41] 1 | Interrupted time series | Construction workers in Italy Basic modules: n = 2320 or 2375 worker jobs Specific modules: n = 1158 or 1164 worker jobs | Duration: July 2002 to December 2005 Extended follow up: N/A | Didactic module-based education, basic modules for all workers and specific modules for specific jobs | No significant effect in preventing injuries—estimated 6% decrease in the frequency of injuries per 10,000 days of exposure (p = 0.08) |
| Kidd et al., 2007 (grant report) [39] | Controlled before and after | Construction workers in the USA Intervention: n = 260 Control: n = 95 | Duration: 1995 to 1999 Extended follow up: N/A | Participatory training for fall prevention and back injury prevention | No significant differences in the number or cost of injury claims compared to control | |
| Schoenfisch et al., 2017 [46] | Prospective cohort | Carpenters in the USA Exposed: n = 377 with OSHA-10 training, n = 76 with OSHA-30 training Unexposed: n = 17,106 | Duration: 2000 to 2008 Extended follow up: N/A | The Occupational Safety and Health Administration (OSHA) offered 10- and 30-h didactic injury prevention courses | No significant effect in preventing injuries—the rate ratio of injuries in trained vs. untrained workers was 0.87 (95% CI: 0.72–1.06) | |
| Evanoff et al., 2016 [50] | Uncontrolled Before and After | Carpenters in the USA, n = 2291 | Duration: 2007 to 2009 Extended follow up: N/A | Didactic and participatory education on fall prevention | No significant effect in preventing injuries, once covariates are accounted for—incidence rate of falls (95% CI) pre-intervention: 18.3 (15.5–21.1) vs. post-intervention: 14 (11.7–16.2) | |
| Darragh et al., 2004 [51] | Uncontrolled Before and After | Construction workers in the USA n = 97 companies | Duration: 1997 to 1998 Extended follow up: N/A | Three-hour safety training and orientation, plus access to optional 10-h OSHA training courses | No significant effect in preventing injuries—the risk ratio before and after intervention was 0.97 (95% CI: 0.5–2.0) | |
| Johnson & Ruppe 2002 [59] | Uncontrolled before and after | Construction workers in the USA, n = 55 | Duration: 1998 to 1999 Extended follow up: N/A | Didactic education, plus stress management and spirituality sessions | Although injury rates decreased, statistical significance was not stated | |
| Spangenberg et al., 2002 [52] | Uncontrolled before and after | Construction workers in Denmark, sample size not stated, but estimated 6.8 million person-hours worked | Duration: 1996 to 1998 Extended follow up: N/A | Didactic education, safety-based monetary incentives, and a social marketing campaign | Significant effect in preventing injuries, once concurrent changes in construction intensity are accounted for—25% reduction in injuries (95%CI: 1–43%) | |
| Williams et al., 2010 [53] | Uncontrolled before and after | Construction workers in the USA (all Latino males), n = 313 | Duration: 1 day Extended follow up: 2–6 months | Didactic education on topics pertinent to Latino immigrant workers | Although injury rates decreased by 24.0%, statistical significance was not stated | |
| Education Services | Vercruysse et al., 2016 [27] | Cluster RCT, randomized at the school level | Physical education teachers in Belgium Intervention: n = 29 teachers from 19 schools Control: n = 26 teachers from 20 schools | Duration: September 2013 to June 2014 Extended follow up: N/A | Didactic and participatory education, access to didactic videos; controls did not receive any intervention | No significant effect in preventing injuries compared to control—0.20 (95% CI: 0.06–0.61) work injuries per 1000 h in the intervention group; 0.54 (0.24–1.18) work injuries per 1000 h in the control group |
| Health Care & Social Assistance | Koblesky 2017 (abstract) [47] | Uncontrolled before and after | Blood center employees in the USA, 2010 to 2014 Sample size not stated | Duration: 2011 to 2014 Extended follow up: N/A | Didactic education and social marketing, plus administrative changes | Although the number of injuries, workers’ compensation claims, and days away from work decreased, statistical significance was not stated |
| Manufacturing | Yu et al., 2017 [30] | Paired cluster RCT | Factory workers in China Intervention: n = 966 from 30 experimental factories Control 1: n = 966 from the same 30 experimental factories Control 2: n = 1706 from 30 control factories | Duration: June 2008 to November 2009 Extended follow up: 12 months | Participatory education featuring a workplace inspection exercise followed by discussion on implementable actions; controls received didactic education only | Significant effect in preventing injuries compared to control and baseline. Compared to the experimental group, the odds ratio (95% CI) was 1.78 (1.04–3.04) for experimental factory controls, and 1.77 (1.13–2.79) for control factory controls |
| Morgan et al., 2012 [31] | Individually randomized RCT | Overweight/obese (BMI 25–40) male aluminum workers in Australia Intervention: n = 65 Control: n = 45 | Duration: October 2009 to March 2010 Extended follow up: 12 months | Didactic education, lifestyle feedback, free pedometers, and a monetary incentive to lose weight (although the stated goal was obesity reduction, injury prevention was an intended effect of intervention); controls were put on a waitlist | Significant effect in preventing injuries compared to control—the mean difference between groups was 0.3 fewer injuries per person for the intervention group (95% CI: 0.0–0.6) | |
| Hermann et al., 2010 [36] 1 | Controlled before and after | Automobile plant workers in Mexico Intervention: one plant (workforce 873–1350) Control: two plants (workforces 2990–3800 and 1291–1369 respectively) | Duration: January 1997 to January 2004 Extended follow up: N/A | Didactic education, a social marketing campaign, and behavioral feedback, plus administrative changes; controls received a basic safety campaign | Significant effect in preventing injuries compared to baseline—92% percent decrease of medical plus lost-time cases in the experimental plant, 3% in control plant A, and 6% in control plant B | |
| Mancini et al., 2005 [37] | Controlled before and after | Factory workers in Italy Intervention: n = 237 metal-ware factories (workforce not stated) Control: construction and wood/ceramics industries (workforce not stated) | Duration: December 1991 to June 1992 Extended follow up: 11 years | Didactic education and a social marketing campaign; controls received no intervention | Significant effect in preventing eye injuries compared to control—post-intervention incident rate ratios (95% CI) were 0.77 (0.61–0.97) after 1–4 years, 0.63 (0.50–0.79) after 5–8 years, and 0.58 (0.43–0.77) after 9–11 years | |
| Yeow & Goomas 2014 [38] | Controlled before and after study | Fluid plant workers in the USA Intervention: one fluid manufacturing plant, n = 362 Control: one fluid manufacturing plant, n = 338 | Duration: 26 months Extended follow up: N/A | A safety-based monetary incentive program, peer-based monitoring and safety discussions; controls received didactic lectures only | Significant effect in preventing injuries compared to control (48% reduction after 2 years) and baseline (33% reduction after 2 years) | |
| Porru et al., 2011 [42] | Interrupted Time Series | Foundry workers in Italy One ferrous foundry (n = 230 approximately) and one non-ferrous foundry (n = 50 approximately) | Duration: 2000–2002 Extended follow up: 7 years | Safety discussions, didactic and participatory education, technical and organizational support, and health surveillance | Significant effect in preventing injuries in the short, medium, and long term for foundry A, but only in the long term for foundry B | |
| Porru et al., 2017 [43] | Interrupted time series | Foundry workers in Italy 22 ferrous (total n = 2750 workers) and 7 non-ferrous foundries (total n = 710 workers) | Duration: 2008 to 2013 Extended follow up: N/A | Improved formalization and dissemination of safety instructions, didactic education, safety audits and administrative support, and health surveillance | Only significant 26% (95% CI: 5–43%) reduction in incidence rate (per worker) but not frequency rate (per hour) in ferrous foundries; no significant differences found in non-ferrous foundries | |
| Borger et al., 2011 (abstract) [40] | Interrupted time series | Glass factory workers in Germany 10 glass factories, n = 860 | Duration: 2002 to 2003 Extended follow up: 6 years | Training on job-specific safety behaviors and risk management | Significant effect in preventing injuries—ITS reveals a 37% decrease that can be attributed to intervention | |
| Shouman et al., 2002 [54] | Uncontrolled before and after | Glass factory workers in Egypt, n = 1229 | Duration: 2000 calendar year Extended follow up: N/A | Didactic education, social marketing, a safety-based monetary incentive, greater availability of PPE, and administrative support | Significant effect in preventing injuries—24% reduction in both incidence rate (per worker) and frequency rate (per hour) | |
| Nunu et al., 2018 [55] | Uncontrolled before and after | Cement manufacturing workers in Zimbabwe, n = 244 | Duration: 2007 to 2011 Extended follow up: N/A | Peer-based behavioral monitoring and reinforcement; rewards for safe behavior and reorientation for unsafe behavior | Significant effect in preventing injuries—37% reduction in the number of injuries | |
| Day 2002 (thesis) [56] | Uncontrolled before and after | Workers at a pulp and paper mill in Canada, n = 190 | Duration: February to March 2002 Extended follow up: 2 months | One-day safety leadership course, all workers were welcome to attend | Although medical and first-aid incidents increased, statistical significance was not stated | |
| Gatti et al., 2013 (abstract) [48] | Uncontrolled before and after | Workers in 2 factories in Italy, sample sizes not stated | Duration: both studies are 2010 to 2012 Extended follow up: N/A | Behavioral feedback, reinforcement, and problem solving | Although injury rates decreased by 52% in the first factory and 68% in the second factory, statistical significance was not stated in either | |
| Mining, Quarrying, and Oil and Gas Extraction | Adams et al., 2013 [32] | Cluster-randomized RCT at the quarry level | Stone quarry workers in India Intervention: n = 103 from three experimental quarries Control: n = 101 from three control quarries | Duration: September 2006 to March 2007 Extended follow up: N/A | Eleven sessions of didactic education, social marketing, group motivational sessions, and individual counselling; controls received one session of standard didactic education | Significant effect in preventing injuries compared to baseline—12% reduction (95% CI: 3–21%) |
| Hagge et al., 2016 [34] | Controlled before and after | Miners in the USA Intervention: n = approximately 400 Control: industry standard | Duration: 2007 to 2014 Extended follow up: N/A | Peer safety observation and feedback, and creation of a new safety plan, plus safety-oriented administrative changes | Although injury rates decreased by 50%, statistical significance was not stated | |
| Kowalski-Trakofler & Barrett 2016 [60] | Uncontrolled before and after | Miners in the USA Study B: 4 mines with >2300 workers total; Study C: 1 mine with 550 workers (Study A not included due to lack of injury outcomes) | Duration: 1995 to 1996 for Study B; 1995 for Study C Extended follow up: 12 months for Study C | Degraded images were used instead of highlighted images during safety training | Significant effect in preventing injuries in study B (9.06% decrease in the first year and a further 29.94% in the second year); although injury rates decreased by 27.1% in study C, significance was not stated | |
| Public Administration | Sullivan et al., 2017 [28] | Matched-pairs cluster RCT, randomized at the station level | Firefighters in the USA Intervention: 16 stations, n = 601 Control: 16 stations, n = 588 | Duration: last 2 weeks of August 2009 Extended follow up: 54 weeks | Didactic education on sleep health (although the stated goal was to improve sleep health, injury prevention was an intended effect of intervention); controls did not receive intervention | Significant effect in reducing the number of injury and disability days (1.4 per worker in the intervention group vs. 2.6 per worker in the control group), but not the number of injuries and motor vehicle crashes |
| Knapik et al., 2004 [44] | Historically controlled | Soldiers in the USA Intervention: n = 1283 (1122 men and 161 women) Historical control: n = 2559 (2303 men and 256 women) | Duration: 36 weeks Extended follow up: N/A | Modified physical training and didactic education, plus administrative injury surveillance support | Significant effect in preventing injuries for men only—adjusted risk ratio of control vs. intervention (95% CI) was 1.50 (1.06–2.12) for men and 1.37 (0.57–3.29) for women | |
| Transportation and Warehousing | Robaina et al., 2010 [35] | Controlled before and after | Stevedores in Cuba Intervention: n = 185 (from one terminal) Control: n = 105 (from another terminal) | Duration: January 2004 to April 2005 Extended follow up: until end of 2006 | Group safety discussions, didactic and participatory education for workers and supervisors; controls received no intervention. | Significant effect in preventing injuries compared to control (58.8% of injuries prevented) and baseline (2.8 fewer injuries per 100 person-years) |
| Howard et al., 2009 (abstract) [57] | Uncontrolled before and after | Road transport drivers, Australia, n = 800 | Duration: 3 years Extended follow up: 12 months | Sleep health education and individual health screening, (although the stated goal was to improve sleep health, injury prevention was an intended effect of intervention) | Significant effect in preventing injuries—lost time injuries per 100 drivers were reduced from 17.1 to 14.2 | |
| Utilities | Salminen 2008 [49] | Uncontrolled before and after | Electricians in Finland, 1998 to 2005 Study 1: n = 172 Study 2: n = 179 | Duration: 2001 to 2002 for Study 1; 2001 for Study 2 Extended follow up: 3 years for both studies | Study 1: group safety discussion followed by collaborative decision on solutions Study 2: Didactic and participatory education on driving safety | In Study 1, although work-related traffic incidents decreased by 72.2%, other occupational injuries increased by 15.1%. The proportion of traffic-related incidents decreased significantly. In Study 2, although the rate of injuries increased by 50%, statistical significance was not stated |
| Badmos 2018 (abstract) [58] | Uncontrolled before and after | Electricity distribution company employees in Nigeria, (sample size not stated) | Duration: 2015 to 2017 Extended follow up: N/A | Safety counselling and videos, safety huddles, and hazard identification competitions, plus administrative changes | Although injury rates decreased by 40% among staff, statistical significance was not stated. | |
| Mixed Industries | Boini et al., 2017 [45] | Prospective cohort | Young workers in France, 2009–2014 Exposed: students who received occupational safety and health (OSH) training in school, n = 687 Unexposed: students who did not receive training, n = 68 | Duration: variable Extended follow up: 2 years | Didactic education (varied based on type of diploma) | Significant effect in preventing injuries—the incident rate ratio of exposed to unexposed was 0.51 (95% CI: 0.00–0.98). |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Pang, M.; Smith, J.; Pawliuk, C.; Pike, I. In Search of Concrete Outcomes—A Systematic Review on the Effectiveness of Educational Interventions on Reducing Acute Occupational Injuries. Int. J. Environ. Res. Public Health 2020, 17, 6874. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186874
Li J, Pang M, Smith J, Pawliuk C, Pike I. In Search of Concrete Outcomes—A Systematic Review on the Effectiveness of Educational Interventions on Reducing Acute Occupational Injuries. International Journal of Environmental Research and Public Health. 2020; 17(18):6874. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186874
Chicago/Turabian StyleLi, Jim, Max Pang, Jennifer Smith, Colleen Pawliuk, and Ian Pike. 2020. "In Search of Concrete Outcomes—A Systematic Review on the Effectiveness of Educational Interventions on Reducing Acute Occupational Injuries" International Journal of Environmental Research and Public Health 17, no. 18: 6874. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186874