Healthcare at Your Fingertips: The Acceptance and Adoption of Mobile Medical Treatment Services among Chinese Users


Abstract
:1. Introduction
2. Literature Review and Hypothesis Development
2.1. TAM Constructs
2.2. Trust, Privacy Concerns, Personality, and Interactivity
3. Methods
3.1. Instrument Development
3.2. Participant Recruitment and Data Collection
3.3. Data Analysis
4. Results
4.1. Description of Respondents
4.2. Measurement Model
4.3. Structural Model
5. Discussion
5.1. Insights into Users’ Adoption Behavior toward MMT Services
5.2. Factors Influencing the Acceptance of MMT Applications
5.3. Implications
5.4. Limitations and Future Work
6. Conclusions
Supplementary Materials
Funding
Acknowledgments
Conflicts of Interest
References
- Ma, X.; Gui, X.; Fan, J.; Zhao, M.; Chen, Y.; Zheng, K. Professional Medical Advice at your Fingertips. In Proceedings of the ACM on Human-Computer Interaction; Association for Computing Machinery (ACM): New York, NY, USA, 2018; Volume 2, pp. 1–22. [Google Scholar]
- Chen, Y.; Cheng, K.; Tang, C.; Siek, K.A.; Bardram, J.E. Is My Doctor Listening to Me?: Impact of Health It Systems on Patient-Provider Interaction. In Proceedings of the CHI’13 Extended Abstracts on Human Factors in Computing Systems, Paris, France, 27 April–2 May 2013; Association for Computing Machinery (ACM): New York, NY, USA, 2013; Volume 2013, pp. 2419–2426. [Google Scholar]
- Unruh, K.T.; Skeels, M.M.; Hartzler, A.L.; Pratt, W. Transforming Clinic Environments into Information Workspaces for Patients. In Proceedings of the SIGCHI conference on human factors in computing systems, Atlanta, GA, USA, 10–15 April 2010; Association for Computing Machinery (ACM): New York, NY, USA, 2010; Volume 2010, pp. 183–192. [Google Scholar]
- Weinstein, R.S.; Lopez, A.M.; Joseph, B.; Erps, K.A.; Holcomb, M.; Barker, G.P.; Krupinski, E.A. Telemedicine, Telehealth, and Mobile Health Applications That Work: Opportunities and Barriers. Am. J. Med. 2014, 127, 183–187. [Google Scholar] [CrossRef]
- eHealth at WHO. Available online: https://www.who.int/ehealth/about/en/ (accessed on 15 June 2020).
- Craig, J.; Chua, R.; Russell, C.; Patterson, V.; Wootton, R. The cost-effectiveness of teleneurology consultations for patients admitted to hospitals without neurologists on site. 1: A retrospective comparison of the case-mix and management at two rural hospitals. J. Telemed. Telecare 2000, 6, 46–49. [Google Scholar] [CrossRef]
- Elford, R.; White, H.; Bowering, R.; Ghandi, A.; Maddiggan, B.; John, K.S. A randomized, controlled trial of child psychiatric assessments conducted using videoconferencing. J. Telemed. Telecare 2000, 6, 73–82. [Google Scholar] [CrossRef]
- Jung, C.; Padman, R.; Shevchik, G.; Paone, S. Who are Portal Users vs. Early E-Visit Adopters? A Preliminary Analysis. In AMIA. Annual Symposium Proceedings, Washington, DC, USA, 22–26 October 2011; AMIA Symposium: Bethesda, MD, USA, 2011; Volume 2011, pp. 1070–1079. [Google Scholar]
- Goel, M.S.; Brown, T.L.; Williams, A.; Cooper, A.J.; Hasnain-Wynia, R.; Baker, D.W. Patient reported barriers to enrolling in a patient portal. J. Am. Med. Inform. Assoc. 2011, 18, i8–i12. [Google Scholar] [CrossRef] [Green Version]
- Neuner, J.M.; Fedders, M.; Caravella, M.; Bradford, L.; Schapira, M.M. Meaningful Use and the Patient Portal. Am. J. Med. Qual. 2014, 30, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Guo, X.; Zhang, X.; Sun, Y. The privacy–personalization paradox in mHealth services acceptance of different age groups. Electron. Commer. Res. Appl. 2016, 16, 55–65. [Google Scholar] [CrossRef]
- MHealth Market by Type, Stakeholders, and Application: Global Opportunity Analysis and Industry Forecast, 2020–2027. Available online: https://www.researchandmarkets.com/reports/5118805/mhealth-market-by-type-stakeholders-and (accessed on 12 June 2020).
- Internet Penetration Rate Exceeds 60%, Mobile Internet Usage Continues to Deepen. Available online: http://www.cac.gov.cn/2019-08/30/c_1124939666.htm (accessed on 30 August 2019).
- Analysis of 40 mHealth Applications and Functions. Available online: http://www.woshipm.com/pd/861832.html (accessed on 6 December 2017).
- Cho, J. The impact of post-adoption beliefs on the continued use of health apps. Int. J. Med. Inform. 2016, 87, 75–83. [Google Scholar] [CrossRef]
- Hoque, R. An empirical study of mHealth adoption in a developing country: The moderating effect of gender concern. BMC Med. Inform. Decis. Mak. 2016, 16, 51. [Google Scholar] [CrossRef] [Green Version]
- Tao, D.; Wang, T.; Wang, T.; Zhang, T.; Zhang, X.; Qu, X. A systematic review and meta-analysis of user acceptance of consumer-oriented health information technologies. Comput. Hum. Behav. 2020, 104, 106147. [Google Scholar] [CrossRef]
- Deng, Z.; Mo, X.; Liu, S. Comparison of the middle-aged and older users’ adoption of mobile health services in China. Int. J. Med. Inform. 2014, 83, 210–224. [Google Scholar] [CrossRef]
- Akter, S.; Ray, P.; Ambra, J.D. Continuance of mHealth services at the bottom of the pyramid: The roles of service quality and trust. Electron. Mark. 2012, 23, 29–47. [Google Scholar] [CrossRef]
- Hoque, R.; Sorwar, G. Understanding factors influencing the adoption of mHealth by the elderly: An extension of the UTAUT model. Int. J. Med. Inform. 2017, 101, 75–84. [Google Scholar] [CrossRef]
- Alsswey, A.; Al-Samarraie, H. Elderly users’ acceptance of mHealth user interface (UI) design-based culture: The moderator role of age. J. Multimodal User Interfaces 2019, 14, 49–59. [Google Scholar] [CrossRef]
- Cui, D. Beyond “connected presence”: Multimedia mobile instant messaging in close relationship management. Mob. Media Commun. 2015, 4, 19–36. [Google Scholar] [CrossRef]
- Roettl, J.; Bidmon, S.; Terlutter, R.; Urquhart, C.; Spanakis, E. What Predicts Patients’ Willingness to Undergo Online Treatment and Pay for Online Treatment? Results from a Web-Based Survey to Investigate the Changing Patient-Physician Relationship. J. Med. Internet Res. 2016, 18, e32. [Google Scholar] [CrossRef]
- Labrique, A.; Vasudevan, L.; Chang, L.W.; Mehl, G. H_pe for MHealth: More “y” or “o” on the Horizon? Int. J. Med. Inform. 2013, 82, 467–469. [Google Scholar] [CrossRef] [Green Version]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User Acceptance of Computer Technology: A Comparison of Two Theoretical Models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Ni, Q.; Zhou, R. What factors influence the mobile health service adoption? A meta-analysis and the moderating role of age. Int. J. Inf. Manag. 2018, 43, 342–350. [Google Scholar] [CrossRef]
- Guo, X.; Sun, Y.; Wang, N.; Peng, Z.; Yan, Z. The dark side of elderly acceptance of preventive mobile health services in China. Electron. Mark. 2012, 23, 49–61. [Google Scholar] [CrossRef]
- Li, H.; Wu, J.; Gao, Y.; Shi, Y. Examining individuals’ adoption of healthcare wearable devices: An empirical study from privacy calculus perspective. Int. J. Med. Inform. 2016, 88, 8–17. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.D.D. User Acceptance of Information Technology: Toward a Unified View. MIS Q. 2003, 27, 425. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V. Determinants of Perceived Ease of Use: Integrating Control, Intrinsic Motivation, and Emotion into the Technology Acceptance Model. Inf. Syst. Res. 2000, 11, 342–365. [Google Scholar] [CrossRef] [Green Version]
- Nov, O.; Ye, C. Users’ personality and perceived ease of use of digital libraries: The case for resistance to change. J. Am. Soc. Inf. Sci. Technol. 2008, 59, 845–851. [Google Scholar] [CrossRef]
- Meuter, M.L.; Ostrom, A.L.; Bitner, M.J.; Roundtree, R. The influence of technology anxiety on consumer use and experiences with self-service technologies. J. Bus. Res. 2003, 56, 899–906. [Google Scholar] [CrossRef]
- Akter, S.; Ambra, J.D.; Ray, P. Trustworthiness in mHealth information services: An assessment of a hierarchical model with mediating and moderating effects using partial least squares (PLS). J. Am. Soc. Inf. Sci. Technol. 2010, 62, 100–116. [Google Scholar] [CrossRef] [Green Version]
- Chellappa, R.; Sin, R.G. Personalization versus Privacy: An Empirical Examination of the Online Consumer’s Dilemma. Inf. Technol. Manag. 2005, 6, 181–202. [Google Scholar] [CrossRef]
- Westin, A. Right to Privacy; American Medical Record Association: Chicago, IL, USA, 1967.
- Sutanto, J.; Palme, E.; Tan, C.-H.; Phang, C.W. Addressing the Personalization-Privacy Paradox: An Empirical Assessment from a Field Experiment on Smartphone Users. MIS Q. 2013, 37, 1141–1164. [Google Scholar] [CrossRef]
- Wu, K.-W.; Huang, S.Y.; Yen, D.C.; Popova, I. The effect of online privacy policy on consumer privacy concern and trust. Comput. Hum. Behav. 2012, 28, 889–897. [Google Scholar] [CrossRef]
- Milne, G.R.; Culnan, M.J. Strategies for reducing online privacy risks: Why consumers read (or don’t read) online privacy notices. J. Interact. Mark. 2004, 18, 15–29. [Google Scholar] [CrossRef]
- Joinson, A.N.; McKenna, K.Y.A.; Postmes, T.; Reips, U.D. Self-Disclosure, Privacy and the Internet. In Oxford Handbook of Internet Psychology; Oxford University Press: Oxford, UK, 2012; pp. 237–250. [Google Scholar]
- Lee, C.H.; Cranage, D.A. Personalisation–privacy paradox: The effects of personalisation and privacy assurance on customer responses to travel Web sites. Tour. Manag. 2011, 32, 987–994. [Google Scholar] [CrossRef]
- Benbasat, S.Y.X.K. The Effects of Personalization and Familiarity on Trust and Adoption of Recommendation Agents. MIS Q. 2006, 30, 941. [Google Scholar] [CrossRef]
- Guilabert, M.B. Attitudes toward Consumer-Customized High-Tech Products: The Role of Perceived Usefulness, Perceived Ease of Use, Technology Readiness, and Customer Customization Sensitivity. Ph.D. Thesis, Georgia State University, Atlanta, GA, USA, June 2005. [Google Scholar]
- Liang, T.P.; Chen, H.Y.; Du, T.; Turban, E.; Li, Y. Effect of Personalization on the Perceived Usefulness of Online Customer Services: A Dual-Core Theory. J. Electron. Commer. Res. 2012, 13, 275–288. [Google Scholar]
- Wu, G.M. The Role of Perceived Interactivity in Interactive Ad Processing. Ph.D. Thesis, The University of Texas at Austin, Austin, TX, USA, August 2000. [Google Scholar]
- Lee, T. The Impact of Perceptions of Interactivity on Customer Trust and Transaction Intentions in Mobile Commerce. J. Electron. Commer. Res. 2005, 6, 165. [Google Scholar]
- Chen, Q.; Chen, H.-M.; Kazman, R. Investigating antecedents of technology acceptance of initial eCRM users beyond generation X and the role of self-construal. Electron. Commer. Res. 2007, 7, 315–339. [Google Scholar] [CrossRef]
- Teo, H.-H.; Oh, L.-B.; Liu, C.; Wei, K.K. An empirical study of the effects of interactivity on web user attitude. Int. J. Hum. Comput. Stud. 2003, 58, 281–305. [Google Scholar] [CrossRef]
- Zhang, X.; Guo, X.; Lai, K.-H.; Guo, F.; Li, C. Understanding Gender Differences in m-Health Adoption: A Modified Theory of Reasoned Action Model. Telemed. e-Health 2014, 20, 39–46. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, N.; Guo, X.; Peng, Z. Understanding the Acceptance of Mobile Health Services: A Comparison and Integration of Alternative Models. J. Electron. Commer. Res. 2013, 14, 183–200. [Google Scholar]
- Thatcher, J.B.; Perrewé, P.L. An Empirical Examination of Individual Traits as Antecedentsto Computer Anxiety and Computer Self-Efficacy. MIS Q. 2002, 26, 381–396. [Google Scholar] [CrossRef] [Green Version]
- Xue, L.; Yen, C.C.; Chang, L.; Chan, H.C.; Tai, B.C.; Tan, S.B.; Duh, H.B.L.; Choolani, M. An exploratory study of ageing women’s perception on access to health informatics via a mobile phone-based intervention. Int. J. Med. Inform. 2012, 81, 637–648. [Google Scholar] [CrossRef]
- McKnight, D.H.; Choudhury, V.; Kacmar, C. Developing and Validating Trust Measures for e-Commerce: An Integrative Typology. Inf. Syst. Res. 2002, 13, 334–359. [Google Scholar] [CrossRef] [Green Version]
- Teo, T.S.; Liu, J. Consumer trust in e-commerce in the United States, Singapore and China. Omega 2007, 35, 22–38. [Google Scholar] [CrossRef]
- Jee, J.; Lee, W.-N. Antecedents and Consequences of Perceived Interactivity. J. Interact. Advert. 2002, 3, 34–45. [Google Scholar] [CrossRef]
- Hew, T.-S.; Kadir, S.L.S.A. Behavioural intention in cloud-based VLE: An extension to Channel Expansion Theory. Comput. Hum. Behav. 2016, 64, 9–20. [Google Scholar] [CrossRef]
- Featherman, M.S.; Pavlou, P.A. Predicting e-services adoption: A perceived risk facets perspective. Int. J. Hum. Comput. Stud. 2003, 59, 451–474. [Google Scholar] [CrossRef] [Green Version]
- Sun, S.; Zhou, X.; Denny, J.C.; Rosenbloom, T.S.; Xu, H. Messaging to your doctors: Understanding patient-provider communications via a portal system. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Paris, France, 27 April–2 May 2013; Association for Computing Machinery (ACM): New York, NY, USA, 2013; Volume 2013, p. 1739. [Google Scholar] [CrossRef]
- Will the Online Medical Services Rise Sharply with the Explosion of Online Consultations? Available online: https://www.iyiou.com/p/123584.html%0D (accessed on 17 February 2020).
- Product Analysis of Online Medical Apps: Ping an Good Doctor. Available online: http://www.woshipm.com/evaluating/1754515.html (accessed on 20 December 2018).
- Fornell, C.; Bookstein, F.L. Two Structural Equation Models: LISREL and PLS Applied to Consumer Exit-Voice Theory. J. Mark. Res. 1982, 19, 440–452. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F.; Ringle, C.M.; Sarstedt, M. PLS-SEM: Indeed a Silver Bullet. J. Mark. Theory Pr. 2011, 19, 139–152. [Google Scholar] [CrossRef]
- Report on Chinese Employers’ Demand and White-Collar Talent Supply in the Fall of 2019. Available online: https://reports.hrflag.com/Report/detail?fileid=f185948d8a4947dc8e85ee6e1707d216&msg=2019%E5%B9%B4%E7%A7%8B%E5%AD%A3%E4%B8%AD%E5%9B%BD%E9%9B%87%E4%B8%BB%E9%9C%80%E6%B1%82%E4%B8%8E%E7%99%BD%E9%A2%86%E4%BA%BA%E6%89%8D%E4%BE%9B%E7%BB%99%E6%8A%A5%E5%91%8A-%E6%99%BA%E8%81%94%E6%8B%9B%E8%81%98_HRflag%E4%BC%97%E6%97%97 (accessed on 18 August 2020).
- Larcker, D.F.; Fornell, C. Evaluating Structural Equation Models with Unobservable Variables and Measurement Error. J. Mark. Res. 1981, 18, 39. [Google Scholar] [CrossRef]
- Chin, W.W. Commentary: Issues and Opinion on Structural Equation Modeling. MIS Q. 1998, 22, 7–16. [Google Scholar]
- Hao, H. The Development of Online Doctor Reviews in China: An Analysis of the Largest Online Doctor Review Website in China. J. Med. Internet Res. 2015, 17, e134. [Google Scholar] [CrossRef]
- Hao, H.; Zhang, K.; Santana, S. The Voice of Chinese Health Consumers: A Text Mining Approach to Web-Based Physician Reviews. J. Med. Internet Res. 2016, 18, e108. [Google Scholar] [CrossRef]
- Becker, D. Acceptance of Mobile Mental Health Treatment Applications. Procedia Comput. Sci. 2016, 98, 220–227. [Google Scholar] [CrossRef] [Green Version]
- Chang, M.-Y.; Pang, C.; Tarn, J.M.; Liu, T.-S.; Yen, D.C. Exploring user acceptance of an e-hospital service: An empirical study in Taiwan. Comput. Stand. Interfaces 2015, 38, 35–43. [Google Scholar] [CrossRef]
- Esmaeilzadeh, P.; Sambasivan, M.; Kumar, N. The Challenges and Issues Regarding E-Health and Health Information Technology Trends in the Healthcare Sector. Databases Inf. Syst. 2010, 113, 23–37. [Google Scholar] [CrossRef]
- Chauhan, S.; Jaiswal, M. A meta-analysis of e-health applications acceptance. J. Enterp. Inf. Manag. 2017, 30, 295–319. [Google Scholar] [CrossRef]
- Kim, J.B. The Mediating Role of Presence on Consumer Intention to Participate in a Social Commerce Site. J. Internet Commer. 2015, 14, 425–454. [Google Scholar] [CrossRef]
- Hung, S.-Y.; Chang, C.-M.; Kuo, S.-R. User acceptance of mobile e-government services: An empirical study. Gov. Inf. Q. 2013, 30, 33–44. [Google Scholar] [CrossRef]
- Jiang, Z.; National University of Singapore; Chan, J.; Tan, B.; Chua, W. Effects of Interactivity on Website Involvement and Purchase Intention. J. Assoc. Inf. Syst. 2010, 11, 34–59. [Google Scholar] [CrossRef]
- Krishnan, N.F.A.S. The Personalization Privacy Paradox: An Empirical Evaluation of Information Transparency and the Willingness to Be Profiled Online for Personalization. MIS Q. 2006, 30, 13. [Google Scholar] [CrossRef] [Green Version]
- Roussos, G.; Koukara, L.; Kourouthanasis, P.; Giaglis, G.; Tuominen, J.; Seppala, O.; Frissaer, J. A Case Study in Pervasive Retail. In Proceedings of the 2nd International Workshop on Mobile Commerce, Atlanta, GA, USA, 23–28 September 2002; Association for Computing Machinery (ACM): New York, NY, USA, 2002; Volume 2010, pp. 90–94. [Google Scholar]
- Morosan, C.; DeFranco, A. Modeling guests’ intentions to use mobile apps in hotels. Int. J. Contemp. Hosp. Manag. 2016, 28, 1968–1991. [Google Scholar] [CrossRef]
- Hashim, M.J. User Interactivity in EHealth Applications: A Novel Taxonomy. In Proceedings of the 2016 12th International Conference on Innovations in Information Technology (IIT), Al-Ain, UAE, 28–30 November 2016; Institute of Electrical and Electronics Engineers (IEEE): New York, NY, USA, 2016; Volume 2016, pp. 42–45. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Instrument Items | Questions | References | |
|---|---|---|---|
| Intention to use | ITU1 | I intend to use MMT services in the future. | [20,25,57] |
| ITU2 | I believe I will use MMT services in the future. | ||
| ITU3 | I plan to use MMT services in the future. | ||
| Attitude toward use | ATT1 | Using MMT services is a good idea. | [25,48] |
| ATT2 | Using MMT services is a wise idea. | ||
| ATT3 | I like using MMT services. | ||
| Perceived usefulness | PU1 | MMT services are suitable for solving my health problems. | [25,27,49] |
| PU2 | MMT services are effective for solving my health problems. | ||
| PU3 | When using MMT services, my health problems are more likely to be resolved. | ||
| Technology anxiety | TA1 | I feel apprehensive about using MMT services. | [20,27,50,51] |
| TA2 | It scares me to think that I could cause the mobile device to induce bad consequences due to wrong operation. | ||
| TA3 | I hesitate to use technology for fear of making mistakes I cannot correct. | ||
| TA4 | I find MMT services somewhat intimidating. | ||
| Perceived ease of use | PEOU1 | Learning to operate MMT services will be easy for me. | [27] |
| PEOU2 | I can easily become skillful at using MMT services. | ||
| PEOU3 | I can use MMT applications effectively to achieve my specific goals. | ||
| PEOU4 | Overall, MMT services are easy to use. | ||
| Trust | TRU1 | This MMT service provider is trustworthy. | [11,19,52,53] |
| TRU2 | This MMT service provider provides reliable information. | ||
| TRU3 | This MMT service provider keeps promises and commitments. | ||
| TRU4 | This MMT service provider’s behavior meets my expectations | ||
| Interactivity | INT1 | Interacting with this MMT system is similar to having a conversation with a sociable, knowledgeable and warm representative from the company. | [46,54,55] |
| INT2 | I felt that this MMT system talked back to me while I was navigating. | ||
| INT3 | I perceive the MMT system to be sensitive to my information requirements. | ||
| INT4 | My interaction level with the MMT system was high. | ||
| INT5 | I did not interact much with the system much. | ||
| Personalization | PS1 | By disclosing my information, the MMT service provider can understand my needs. | [11,41] |
| PS2 | By disclosing my information, the MMT service provider can know what I require. | ||
| PS3 | By disclosing my information, the mHealth service provider will take my needs as its own preferences. | ||
| Privacy concerns | PC1 | My use of MMT services would make me lose control over the privacy of my information. | [11,56] |
| PC2 | Using MMT services would not cause any privacy problems. | ||
| PC3 | Signing up for and using MMT services would lead to a loss of privacy for me because my personal information could be used without my knowledge. | ||
| PC4 | Others might take control of my information if I use MMT services. | ||
| Frequency | Percentage (%) | ||
|---|---|---|---|
| Gender | Male | 143 | 47.2 |
| Female | 160 | 52.8 | |
| Age | 18–25 | 73 | 24.1 |
| 26–35 | 173 | 57.1 | |
| 36–45 | 43 | 14.2 | |
| 46–55 | 12 | 3.9 | |
| Above 56 | 2 | 0.7 | |
| Education level | Primary school | 1 | 0.3 |
| Middle school | 1 | 0.3 | |
| High school | 13 | 4.3 | |
| Undergraduate | 252 | 83.2 | |
| Postgraduate and above | 36 | 11.9 | |
| Monthly income (RMB) | Below 5000 | 81 | 26.7 |
| 5000–10,000 | 140 | 46.2 | |
| 10,000–15,000 | 53 | 17.5 | |
| Above 15,000 | 29 | 9.6 |
| Construct | Items | Mean (SD) | Standardized Factor Loading | CR | AVE |
|---|---|---|---|---|---|
| Intention to use | ITU1 | 4.3 (0.65) | 0.871 | 0.860 | 0.673 |
| ITU2 | 4.3 (0.71) | 0.812 | |||
| ITU3 | 4.3 (0.70) | 0.776 | |||
| Attitude toward use | ATT1 | 4.3 (0.56) | 0.721 | 0.798 | 0.569 |
| ATT2 | 4.3 (0.69) | 0.721 | |||
| ATT3 | 4.1 (0.77) | 0.816 | |||
| Perceived usefulness | PU1 | 3.9 (0.74) | 0.798 | 0.801 | 0.573 |
| PU2 | 3.8 (0.84) | 0.769 | |||
| PU3 | 3.9 (0.73) | 0.701 | |||
| Technology anxiety | TA1 | 2.1 (0.81) | 0.825 | 0.853 | 0.593 |
| TA2 | 2.2 (1.00) | 0.769 | |||
| TA3 | 2.1 (0.90) | 0.766 | |||
| TA4 | 1.7 (0.66) | 0.715 | |||
| Perceived ease of use | PEOU1 | 4.4 (0.70) | 0.797 | 0.855 | 0.596 |
| PEOU2 | 4.4 (0.73) | 0.786 | |||
| PEOU3 | 4.1 (0.73) | 0.785 | |||
| PEOU4 | 4.3 (0.70) | 0.716 | |||
| Trust | TRU1 | 4.1 (0.67) | 0.798 | 0.831 | 0.553 |
| TRU2 | 4.1 (0.77) | 0.753 | |||
| TRU3 | 4.1 (0.72) | 0.736 | |||
| TRU4 | 3.9 (0.72) | 0.684 | |||
| Perceived interactivity | INT1 | 3.8 (0.78) | 0.775 | 0.842 | 0.572 |
| INT2 | 4.0 (0.80) | 0.774 | |||
| INT3 | 3.8 (0.79) | 0.752 | |||
| INT4 | 2.2 (0.82) | 0.723 | |||
| Perceived personalization | PS1 | 4.0 (0.58) | 0.839 | 0.822 | 0.698 |
| PS2 | 4.0 (0.77) | 0.832 | |||
| Privacy concerns | PC1 | 2.7 (0.91) | 0.902 | 0.904 | 0.703 |
| PC2 | 3.0 (0.96) | 0.843 | |||
| PC3 | 3.0 (0.98) | 0.817 | |||
| PC4 | 3.2 (1.00) | 0.789 |
| ITU | ATT | PU | TA | PEOU | TRU | INT | PS | PC | |
|---|---|---|---|---|---|---|---|---|---|
| ITU | 0.820 | ||||||||
| ATT | 0.711 | 0.754 | |||||||
| PU | 0.482 | 0.511 | 0.757 | ||||||
| TA | −0.485 | −0.488 | −0.439 | 0.770 | |||||
| PEOU | 0.323 | 0.386 | 0.269 | −0.424 | 0.772 | ||||
| TRU | 0.587 | 0.620 | 0.565 | −0.511 | 0.401 | 0.744 | |||
| INT | 0.527 | 0.569 | 0.427 | −0.368 | 0.322 | 0.524 | 0.756 | ||
| PS | 0.327 | 0.352 | 0.358 | −0.304 | 0.315 | 0.366 | 0.376 | 0.836 | |
| PC | −0.369 | −0.455 | −0.430 | 0.474 | −0.218 | −0.421 | −0.375 | −0.202 | 0.839 |
| Hypothesis | Path | Path Coefficient | t-Value | Supported |
|---|---|---|---|---|
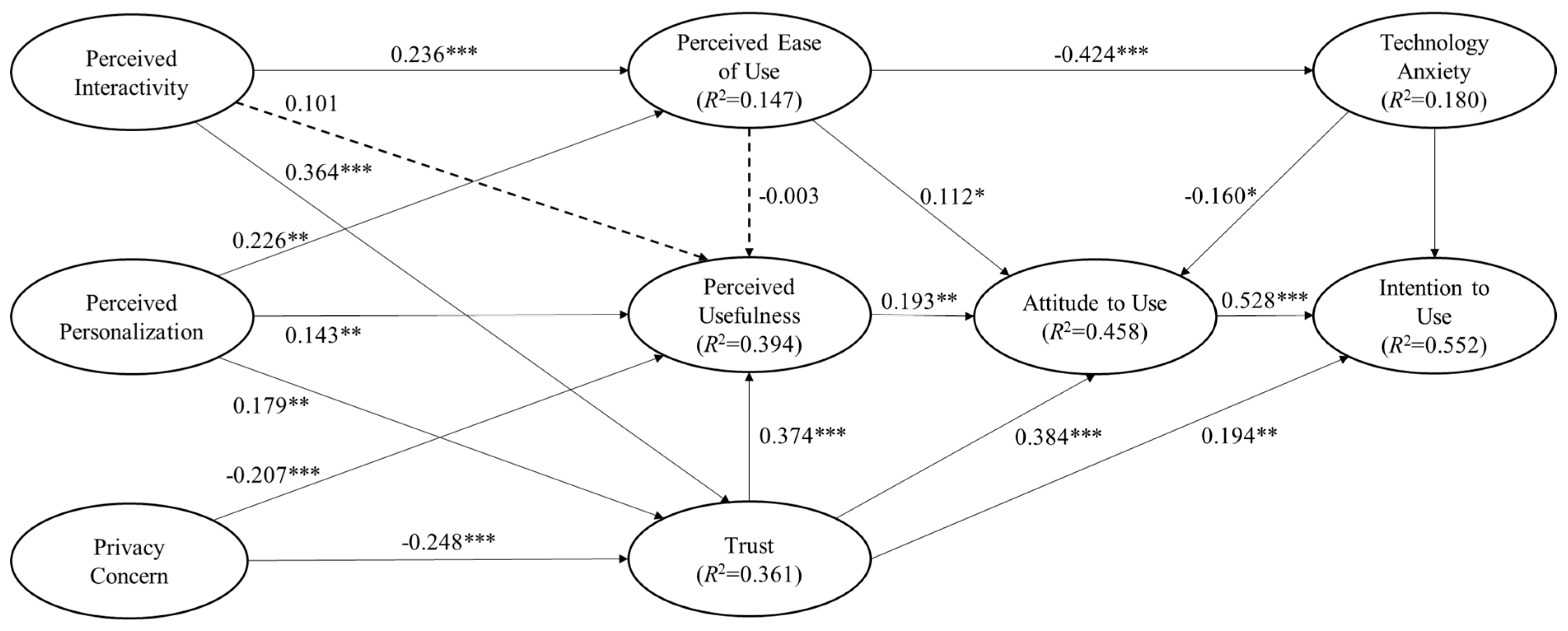
| H1 | ATT → ITU | 0.528 | 8.876 *** | Yes |
| H2 | PU → ATT | 0.193 | 3.543 ** | Yes |
| H3a | PEOU → ATT | 0.112 | 2.031 * | Yes |
| H3b | PEOU → PU | −0.003 | 0.064 | No |
| H3c | PEOU → TA | −0.424 | 9.400 *** | Yes |
| H4a | TA → ATT | −0.160 | 2.360 * | Yes |
| H4b | TA → ITU | −0.128 | 2.308 * | Yes |
| H5a | TRU → ITU | 0.194 | 3.452 ** | Yes |
| H5b | TRU → ATT | 0.384 | 5.623 *** | Yes |
| H5c | TRU → PU | 0.374 | 5.863 *** | Yes |
| H6a | PC → TRU | −0.248 | 4.750 *** | Yes |
| H6b | PC → PU | −0.207 | 3.975 *** | Yes |
| H7a | PS → TRU | 0.179 | 3.329 ** | Yes |
| H7b | PS → PEOU | 0.226 | 3.375 ** | Yes |
| H7c | PS → PU | 0.143 | 2.650 ** | Yes |
| H8a | INT → TRU | 0.364 | 6.280 *** | Yes |
| H8b | INT → PEOU | 0.236 | 4.141 *** | Yes |
| H8c | INT → PU | 0.101 | 1.580 | No |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Q. Healthcare at Your Fingertips: The Acceptance and Adoption of Mobile Medical Treatment Services among Chinese Users. Int. J. Environ. Res. Public Health 2020, 17, 6895. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186895
Li Q. Healthcare at Your Fingertips: The Acceptance and Adoption of Mobile Medical Treatment Services among Chinese Users. International Journal of Environmental Research and Public Health. 2020; 17(18):6895. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186895
Chicago/Turabian StyleLi, Qingchuan. 2020. "Healthcare at Your Fingertips: The Acceptance and Adoption of Mobile Medical Treatment Services among Chinese Users" International Journal of Environmental Research and Public Health 17, no. 18: 6895. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186895