A Call for Leadership and Management Competency Development for Directors of Medical Services—Evidence from the Chinese Public Hospital System


Abstract
:1. Introduction
1.1. Development of Clinical Managers—The Pathway
1.2. Overall Health Management Workforce Development
1.3. Chinese Public Hospitals at a Glance—The Challenges and Management
1.4. The Recruitment and Development of Clinical Leadership and Management in the Chinese Hospital System
2. Materials and Methods
2.1. Target Population
2.2. Questionnaire
- An explanation of the purpose of the study, instructions and consent to participate with assurance of identity protection;
- Demography, educational background (the lowest education category, ‘Technical College’ refers to a post school study program, a qualification or degree below that of an undergraduate or bachelor’s level.), and previous and current work experience;
- Past and current management related training and management difficulties encountered;
- Perceived importance and self-assessment of six core management competencies using the validated MCAP management competency tool, [20,31] which were:
- C1.
- Evidence-informed decision-making (Evidence)—13 behavioral items
- C2.
- Operations, administration and resource management (Resources)—17 behavioral items
- C3.
- Demonstrated knowledge of healthcare environment and the organization (Knowledge)—11 behavioral items
- C4.
- Interpersonal, communication qualities and relationship management (Communications)—19 behavioral items
- C5.
- Leading people and organizations (Leadership)—13 behavioral items
- C6.
- Enabling and managing change (Change)—9 behavioral items
2.3. Data Management and Analysis
2.4. Ethical Approval and Consent to Participate
3. Results
3.1. Demography and Employment Details
3.2. Qualifications and Disciplines
3.3. Informal Training
3.4. Informal Management Related Training
3.5. Participation in Training Focusing on Different Management Related Topics
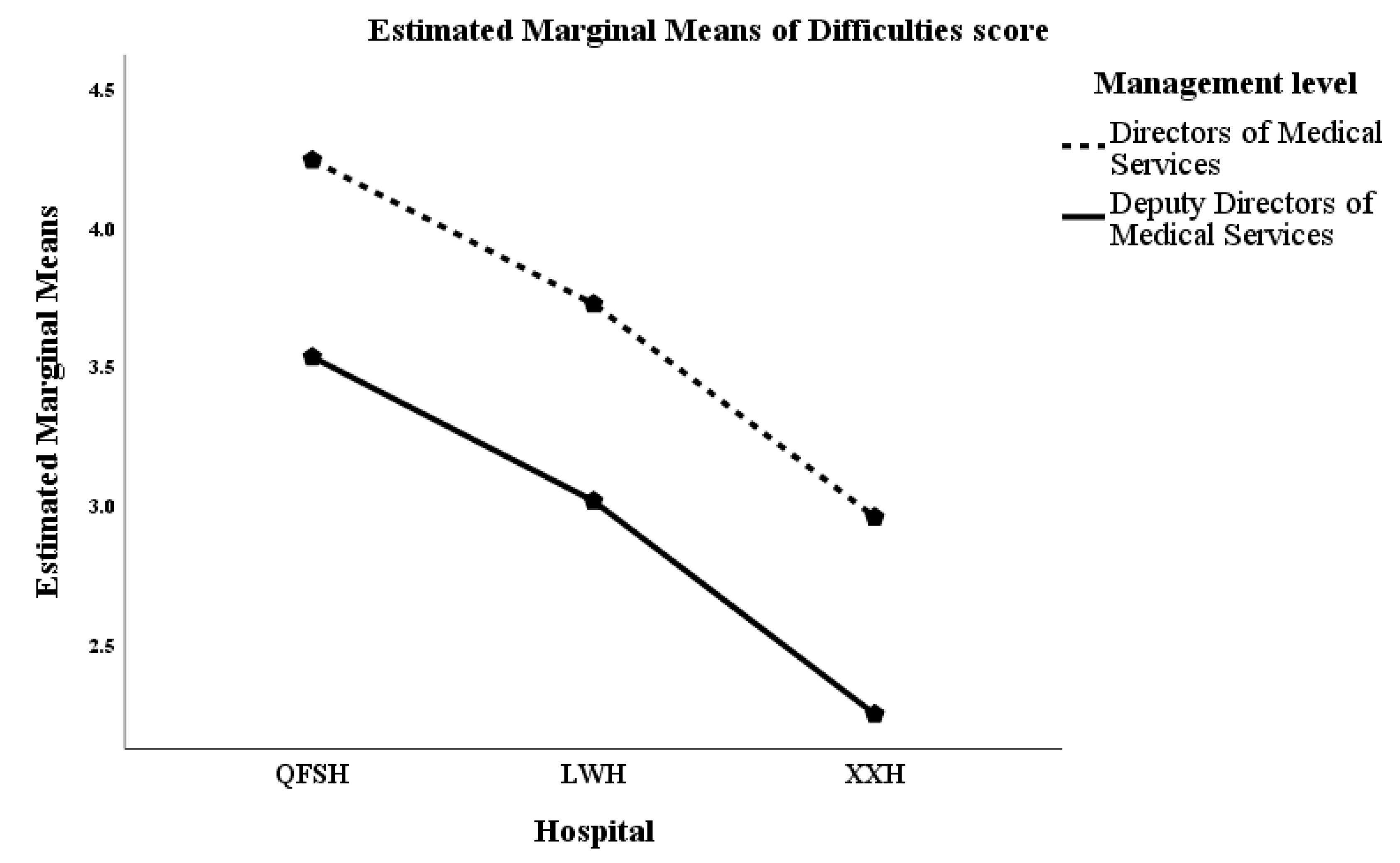
3.6. Difficulties Encountered in the Management Position
3.7. Perceived Importance and Self-Assessment of Management Competencies
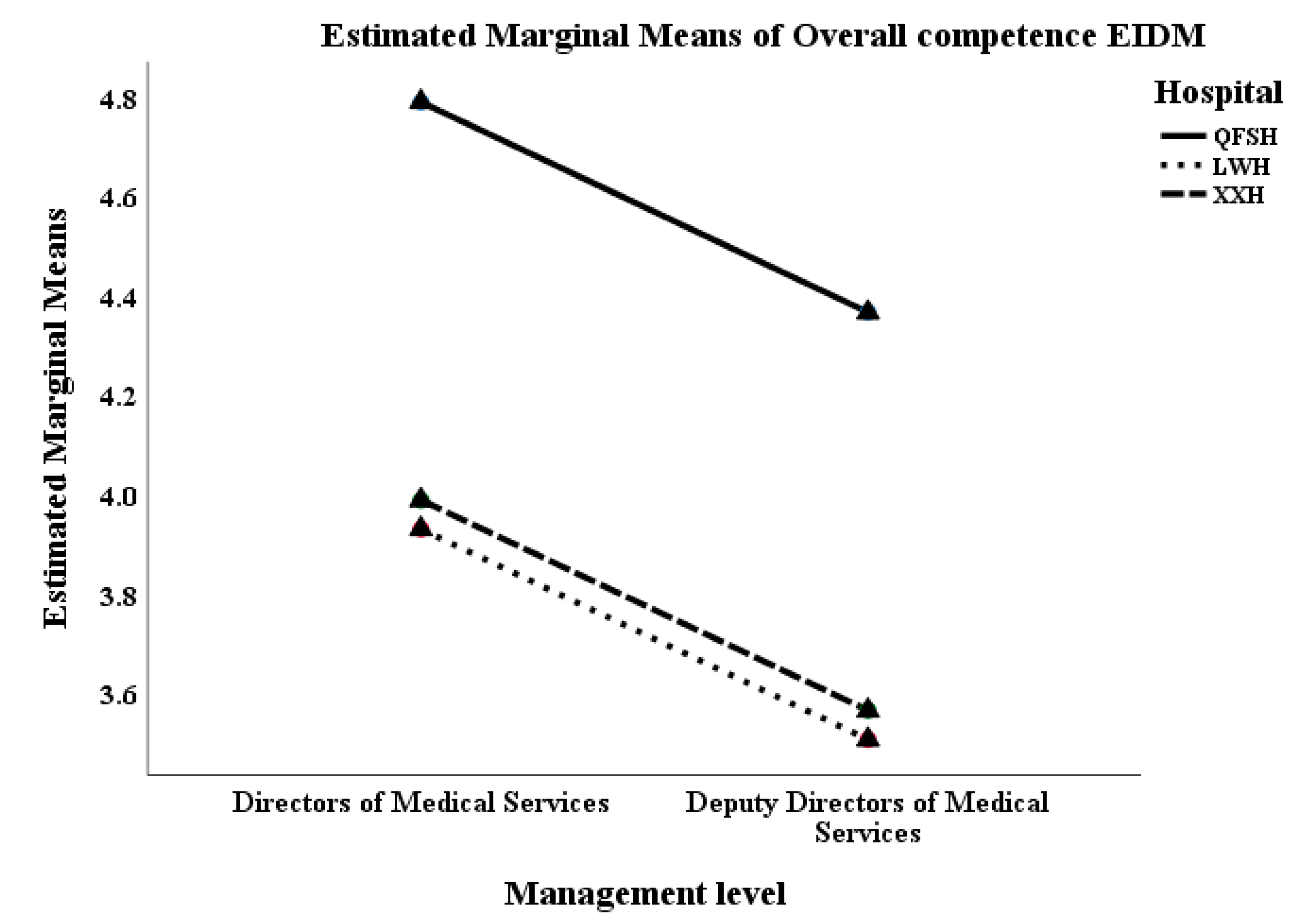
3.8. Overall Competency Level—Self-Assessment
4. Discussion
4.1. Lack of Self-Assessed Management Competence
4.2. Training, Difficulties, Competencies and Implications
- Dealing with conflicts with patients, staff members and their peers;
- Improving and managing performance: staff performance, service quality and management outcomes;
- Developing new skills; and
- Making decisions and managing change.
4.3. Strengths and Weaknesses
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Scale * | Level | Competency Level |
|---|---|---|
| 1 | Not competent | Do not understand the requirements and am not capable of applying it to my role |
| 2 | Basic or novice | May be capable of demonstrating minor aspects in my role |
| 3 | Advanced beginner | May be capable of demonstrating in my role, but not in all required aspects |
| 4 | Competent with occasional guidance | Can generally demonstrate in my role, but guidance is needed occasionally |
| 5 | Competent, no guidance | Can demonstrate in my role independently without guidance, but have not had extensive experience |
| 6 | Proficient | Always apply appropriately in my role with extensive experience |
| 7 | Superior expertise | Always apply appropriately in my role with extensive experience gained from diverse management roles at executive level and can teach this competency to others |
References
- Clark, J.; Armit, K. Leadership competency for doctors: A framework. Leadersh. Health Serv. 2010, 23, 115–129. [Google Scholar] [CrossRef]
- Swanwick, T.; McKimm, J. What is clinical leadership: Why is it important? Clin. Teach. 2011, 8, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Allen, D. Doctors in management or the revenge of the conquered: The role of management development for doctors. J. Manag. Med. 1995, 9, 44. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, L. Moving clinicians into management. A professional challenge or threat? J. Manag. Med. 1994, 8, 32–44. [Google Scholar] [CrossRef]
- Kralewski, J.; Wingert, T. The emerging role of the physician in administration. Physician Exec. 1994, 20, 3–7. [Google Scholar]
- Liang, Z.; Howard, P.; Wang, J.; Xu, M.; Zhao, M. Developing senior hospital managers: Does ‘one size fit all’? —Evidence from the evolving Chinese Health System. BMC Health Serv. Res. 2020, 20, 281. [Google Scholar] [CrossRef]
- Cummings, G.; Lee, H.; MacGregor, T.; Davey, M.; Wong, C.; Paul, L.; Stafford, E. Factors contributing to nursing leadership: A systematic review. J. Health Serv. Res. Policy 2008, 13, 240–248. [Google Scholar] [CrossRef]
- Walston, S.; Khaliq, A. The importance and use of continuing education: Findings of a national survey of hospital executives. J. Health Admin. Educ. 2010, 27, 113–125. [Google Scholar]
- Yarbrough, L.; Stowe, M.; Haefner, J. Competency assessment and development among health-care leaders: Results of a cross-sectional survey. Health Serv. Manag Res. 2012, 25, 78–86. [Google Scholar] [CrossRef]
- Adachi, H.; Sekiya, Y.; Kotaro Imamura, K.; Kazuhiro Watanabe, K.; Kawakami, N. The effects of training managers on management competencies to improve their management practices and work engagement of their subordinates: A single group pre- and pos-test study. J. Occup. Health 2020, 62, e12085. [Google Scholar] [CrossRef] [Green Version]
- Siren, A.; Gehrs, M. Engaging nurses in future management careers: Perspectives on leadership and management competency development through an internship initiative. Nurs. Leadersh. 2018, 31, 36–49. [Google Scholar] [CrossRef] [PubMed]
- Yoshioko-Maeda, K.; Shiomi, M.; Takafumi Katayama, T.; Hosoya, N.; Kuroda, M. Effectiveness of an educational program for mid-level Japanese public health nurses to improve program planning competencies: A preliminary randomized control trial. Public Health Nurs. 2019, 36, 388–400. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Blackstock, F.C.; Howard, P.F.; Briggs, D.S.; Leggat, S.G.; Wollersheim, D.; Edvardsson, D.; Rahman, A. An evidence-based approach to understanding the competency development needs of the health service management workforce in Australia. BMC Health Serv. Res. 2018, 18, 976. [Google Scholar] [CrossRef] [PubMed]
- Vince, R. The contradictions of impact: Action learning and power in organisations. Action Learn. Res. Pract. 2012, 9, 209–218. [Google Scholar] [CrossRef] [Green Version]
- Bartona, G.; Anne Bruceb, A.; Schreiberb, R. Teaching nurses teamwork: Integrative review of competency-based team training in nursing education. Nurse Educ. Pract. 2018, 32, 129–137. [Google Scholar] [CrossRef]
- Guerra, O.; Kurtz, D. Building collaboration: A scoping review of cultural competency and safety education and training for healthcare student and professionals in Canada. Teach. Learn. Med. 2017, 29, 129–142. [Google Scholar] [CrossRef]
- Kiel, J.M. Producing physician administrators: An evaluation of medical school curricula and management education for physicians. In Proceedings of the Association for Health Services Research Meeting, Washington, DC, USA, 21–23 June 1999; Volume 16, pp. 31–32. [Google Scholar]
- Sutherst, J.; Glascott, V. The Doctor-Manager; Churchill Livingstone: Edinburgh, UK, 1994. [Google Scholar]
- Edmonstone, J.D. Whither the elephant? The continuing development of clinical leadership in the UK National Health Services. Int. J. Health Plann. Mgmt. 2014, 29, 280–291. [Google Scholar] [CrossRef]
- Liang, Z.; Howard, P.; Leggat, S.; Bartram, T. Development and validation of health service management competencies. J. Health Organ. Manag. 2018, 32, 157–175. [Google Scholar] [CrossRef]
- Stefl, M. Common competencies for all healthcare managers: The healthcare Leadership Alliance model. J. Healthcare Manag. 2008, 53, 360. [Google Scholar] [CrossRef]
- Epstein, R.; Hundert, E. Defining and assessing professional competence. J. Am. Med. Assoc. 2002, 287, 226–235. [Google Scholar] [CrossRef]
- United Nation. Available online: https://www.worldometers.info/world-population/china-population/ (accessed on 14 July 2020).
- National Bureau Statistics of China. Statistical Communiqué of the People’s Republic of China on the 2019 National Economic and Social Development. Available online: http://www.stats.gov.cn/english/PressRelease/202002/t20200228_1728917.html (accessed on 15 July 2020).
- Niu, H.; Tian, M.; Ma, A.; Wang, C.; Zhang, L. Differences and determinants in access to essential public health services in China: A case study with hypertension people and under-sixes as target population. Chin. Med. J. 2014, 127, 1626–1632. [Google Scholar] [PubMed]
- Li, L.; Fu, H. China’s health care system reform: Progress and prospects. Int. J. Health Plann. Manag. 2017, 32, 40–253. [Google Scholar] [CrossRef] [PubMed]
- Cooke, F.L. A decade of transformation of HRM in China: A review of literature and suggestions for future studies. Asia Pac. J. Hum. Resour. 2009, 47, 6–40. [Google Scholar] [CrossRef]
- Linnander, E.L.; Mantopoulos, J.M.; Allen, N.; Nembhard, I.M.; Bradley, E.H. Professionalizing Healthcare Management: A descriptive case study. Int. J. Health Policy Manag. 2017, 6, 555–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pei, L.; Legge, D. Personnel reform in Chinese hospitals: Policy interdependence and the challenge of coherent incrementalism. China J. Soc. Work 2013, 6, 25–39. [Google Scholar]
- Liang, Z.; Blackstock, F.; Howard, P.; Liu, G.; Geoffrey, L.; Bartram, T. Managers in the publicly funded health services in China—Characteristics and responsibilities. BMC Health Serv. Res. 2020, 20, 721. [Google Scholar] [CrossRef] [PubMed]
- Howard, P.; Liang, Z.; Leggat, S.; Karimi, L. Validation of a management competency assessment tool for health service managers. J. Health Organ. Manag. 2018, 32, 113–134. [Google Scholar] [CrossRef]
- Chen, J.C.; Zhu, Y.L.; Zhang, Q.; Fan, Y.D. Analysis on the status quo of professionalization research of public hospital administrators in China. Acad. J. Guangzhou Univ. 2018, 46, 99–106. [Google Scholar]
- Zhou, M.; Zhao, L.; Sampy, K.S.; Wang, S. Changing of China’s health policy and Doctor–Patient relationship: 1949–2016. Health Policy Technol. 2017, 6, 358–367. [Google Scholar] [CrossRef]
- Yip, W.; Hsiao, W. China’s health care reform: A tentative assessment. China Econ. Rev. 2009, 20, 613–619. [Google Scholar] [CrossRef]
- Ha, J.; Longnecker, n. Doctor-patient communication: A review. Ochsner. J. 2010, 10, 38–43. [Google Scholar]
- Luo, T.; Liu, L. Discussion on status quo of medical dispute and its causes. Chin. Hosp. 2018, 22, 4–6. [Google Scholar]
- Chandra, S.; Mohammadnezhad, M.; Ward, P. Trust and communication in doctor-patient relationship: A literature review. J. Healthc. Commun. 2018, 3, 36. [Google Scholar] [CrossRef]
- Loh, E. How and why medically trained managers undertake postgraduate management training: A qualitative study from Victoria, Australia. J. Health Organ. Manag. 2015, 29, 438–454. [Google Scholar] [CrossRef] [PubMed]
- McKimm, J.; Swanwick, T. Leadership development for clinicians: What are we trying to achieve? Clin. Teach. 2011, 8, 181–185. [Google Scholar] [CrossRef] [PubMed]

| Position | Hospital Level | ||||
|---|---|---|---|---|---|
| Level 1 * | Level 2 * | Level 3 * | Total | ||
| Directors of Medical Services | Count (%) | 30 (68.2) a | 24 (57.1) a, b | 89 (42.6) b | 143 (48.5) |
| Deputy Directors of Medical Services | Count (%) | 14 (31.8) a | 18 (42.9) a, b | 120 (57.4) b | 152 (51.5) |
| Total | Count | 44 | 42 | 209 | 295 |
| Sex | Level 1 | Level 2 | Level 3 | Total | |
| Male | Count (%) | 33 (75.) a | 25 (59.5) a | 131 (62.7) a | 189 (64.1) |
| Female | Count (%) | 11 (25.0) a | 17 (40.5) a | 78 (37.3) a | 106 (35.9) |
| Highest education level | Level 1 | Level 2 | Level 3 | Total | |
| Technical college | Count (%) | 15 (34.1) a | 4 (9.5) b | 4 (1.9) c | 23 (7.8) |
| Bachelor’s degree | Count (%) | 29 (65.9) a | 33 (78.6) a | 40 (19.2) b | 102 (34.7) |
| Master’s degree | Count (%) | 0 (0.0) a | 5 (11.9) a, b | 49 (23.6) b | 54 (18.4) |
| Doctorate | Count (%) | 0 (0.0) a | 0 (0.0) a | 115 (55.3) b | 115 (39.1) |
| Age | Level 1 | Level 2 | Level 3 | Total | |
| Count | 44 | 42 | 209 | 295 | |
| Median (IRQ) | 41.0 (9) | 46.0 (4) | 48.0 (12) | 47.0 (11) | |
| Years at current hospital | Level 1 | Level 2 | Level 3 | Total | |
| Count | 44 | 42 | 209 | 295 | |
| Median (IRQ) | 17.50 (13) | 23.00 (9) | 25.00 (13) | 24.00 (13) | |
| Years as manager | Level 1 | Level 2 | Level 3 | Total | |
| Count | 44 | 42 | 209 | 295 | |
| Median (IRQ) | 8.0 (15) | 8.0 (12) | 9.0 (12) | 8.00 (12) | |
| Years in current management position | Level 1 | Level 2 | Level 3 | Total | |
| Count | 44 | 42 | 209 | 295 | |
| Median (IRQ) | 3.0 (6) | 6.0 (9) | 4.0 (8) | 4.0 (8) | |
| Training Type | Self-Study of Management-Related Topics | |||||||
|---|---|---|---|---|---|---|---|---|
| Hospital Level | ||||||||
| Management Level | Internal Management | External Management | Internal Non-Management | External Non-Management | Level 1 * | Level 2 * | Level 3 * | Combined |
| Directors of Medical Services | 69.0% | 40.8% | 54.9% | 54.2% | 28.6% | 7.1% | 64.3% | 65.6% |
| Deputy Directors of Medical Services | 75.0% | 40.3% | 57.6% | 45.1% | 4.5% | 13.6% | 81.8% | 34.4% |
| All Directors | 72.0% | 40.6% | 56.3% | 49.7% | 20.3% | 9.4% | 70.3% | 100% |
| Percentage of Participants | Mean Score of Training Types | |||||
|---|---|---|---|---|---|---|
| Before | During | Increase | Before | During | Increase | |
| Level 1 * | 20 (48) | 33 (77) | 29% | 2.18 | 3.45 | 58% |
| Level 2 * | 15 (37) | 21 (51) | 14% | 3.14 | 3.52 | 12% |
| Level 3 * | 108 (54) | 136 (67) | 13% | 3.28 | 4.44 | 35% |
| Total | 143 (50) | 190 (66) | 16% | 3.10 | 4.16 | 34% |
| Level 1 * | Level 2 * | Level 3 * | DoMS # | DDoMS # | |
|---|---|---|---|---|---|
| Mean Difficulty Scores | 2.74 | 3.43 | 3.85 | 3.89 | 3.36 |
| Difficulties | Level 1 | Level 2 | Level 3 | DoMS (%) | DDoMS (%) |
| Peer conflict | 23 | 25 | 29 | 27 | 28 |
| Team conflict | 19 | 23 | 27 | 28 | 23 |
| Staff turnover | 21 | 23 | 5 | 14 | 5 |
| Patient conflict | 40 | 48 | 50 | 46 | 50 |
| Innovative teamwork | 14 | 23 | 41 | 38 | 31 |
| Staff hiring | 5 | 3 | 9 | 7 | 7 |
| Loss of skilled staff | 16 | 18 | 10 | 13 | 11 |
| Team skill building | 14 | 8 | 26 | 23 | 21 |
| Ethical problems | 2 | 5 | 11 | 9 | 11 |
| Supervisor confrontation | 12 | 3 | 9 | 12 | 5 |
| Employee performance | 28 | 35 | 41 | 40 | 36 |
| Decision-making & change | 30 | 18 | 31 | 33 | 25 |
| New skill acquisition | 19 | 45 | 33 | 35 | 31 |
| Expected work quality | 14 | 43 | 33 | 34 | 29 |
| Management outcomes expectations | 16 | 28 | 27 | 30 | 22 |
| Competency | Not at All | Acquired to Limited Degree | Unsure | Cumulative Percentage | Acquired Most of It | Fully Acquired |
|---|---|---|---|---|---|---|
| C1 Evidence | 2.4% | 9.1% | 15.4% | 26.9% | 55.6% | 17.5% |
| C2 Resources | 5.9% | 8.4% | 23.8% | 38.1% | 49.0% | 12.9% |
| C3 Knowledge | 0.0% | 5.2% | 10.1% | 15.3% | 61.9% | 22.7% |
| C4 Communications | 0.0% | 5.2% | 9.4% | 14.6% | 59.1% | 26.2% |
| C5 Leadership | 3.8% | 8.7% | 20.3% | 32.8% | 50.7% | 16.4% |
| C6 Change | 6.3% | 10.1% | 21.0% | 37.4% | 46.5% | 16.1% |
| Competencies | Management Level | All Directors | Hospital Level | |||
|---|---|---|---|---|---|---|
| DoMS # | DDoMS # | Level 1 * | Level 2 * | Level 3 * | ||
| C1. Evidence | 4.47 | 4.19 | 4.33 | 3.86 | 3.75 | 4.55 |
| C2. Resources | 4.44 | 4.02 | 4.23 | 3.74 | 3.63 | 4.45 |
| C3. Knowledge | 4.78 | 4.42 | 4.59 | 4.07 | 3.98 | 4.83 |
| C4. Communications | 4.84 | 4.57 | 4.70 | 4.37 | 4.15 | 4.89 |
| C5. Leadership | 4.56 | 4.23 | 4.40 | 3.86 | 3.88 | 4.62 |
| C6. Change | 4.33 | 3.94 | 4.14 | 3.84 | 3.58 | 4.31 |
| Six competencies | 4.57 | 4.23 | 4.40 | 3.96 | 3.83 | 4.61 |
| Level | Strategies |
| Health system [6,18,27,28] |
|
| Higher education system [6,14,17] |
|
| Healthcare organisation [6,8,9,13,14,31] |
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, Z.; Howard, P.; Wang, J.; Xu, M. A Call for Leadership and Management Competency Development for Directors of Medical Services—Evidence from the Chinese Public Hospital System. Int. J. Environ. Res. Public Health 2020, 17, 6913. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186913
Liang Z, Howard P, Wang J, Xu M. A Call for Leadership and Management Competency Development for Directors of Medical Services—Evidence from the Chinese Public Hospital System. International Journal of Environmental Research and Public Health. 2020; 17(18):6913. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186913
Chicago/Turabian StyleLiang, Zhanming, Peter Howard, Jian Wang, and Min Xu. 2020. "A Call for Leadership and Management Competency Development for Directors of Medical Services—Evidence from the Chinese Public Hospital System" International Journal of Environmental Research and Public Health 17, no. 18: 6913. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186913