Public Awareness and Behaviour in Great Britain in the Context of Sunlight Exposure and Vitamin D: Results from the First Large-Scale and Representative Survey


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
- Knowledge about vitamin D, for instance: its benefits, its sources, and the exposure needed to produce adequate vitamin D.
- Current sunlight exposure behaviours.
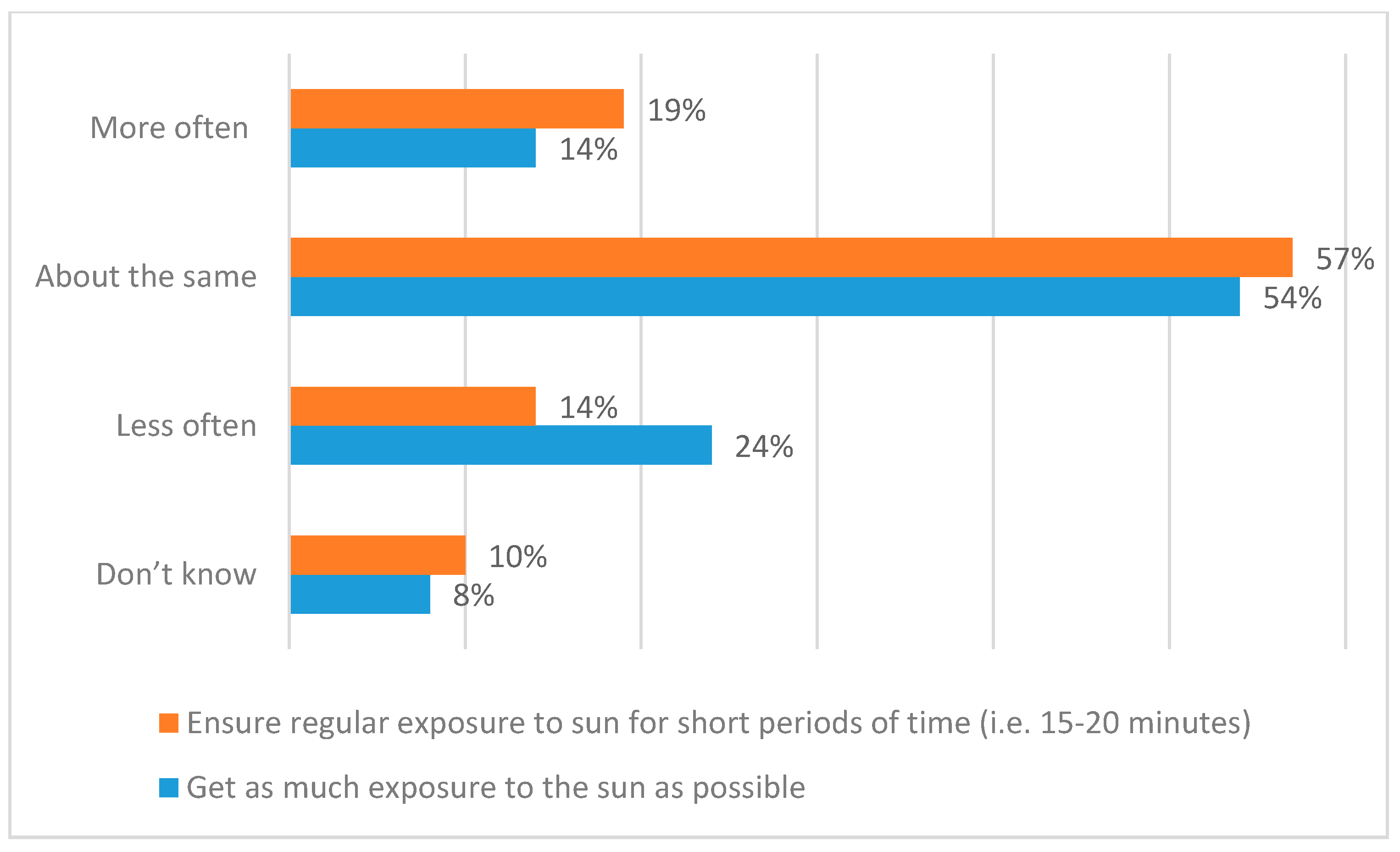
- Changes in sunlight exposure behaviours over the past ten years.
- Current perceptions of the extent to which public health communications with respect to sunlight exposure focus on the risks and the benefits.
- Changes in perceptions of the extent to which public health communications with respect to sunlight exposure focus on the risks and the benefits
- The extent to which these factors vary depending on skin type or demographic characteristics.
3. Results
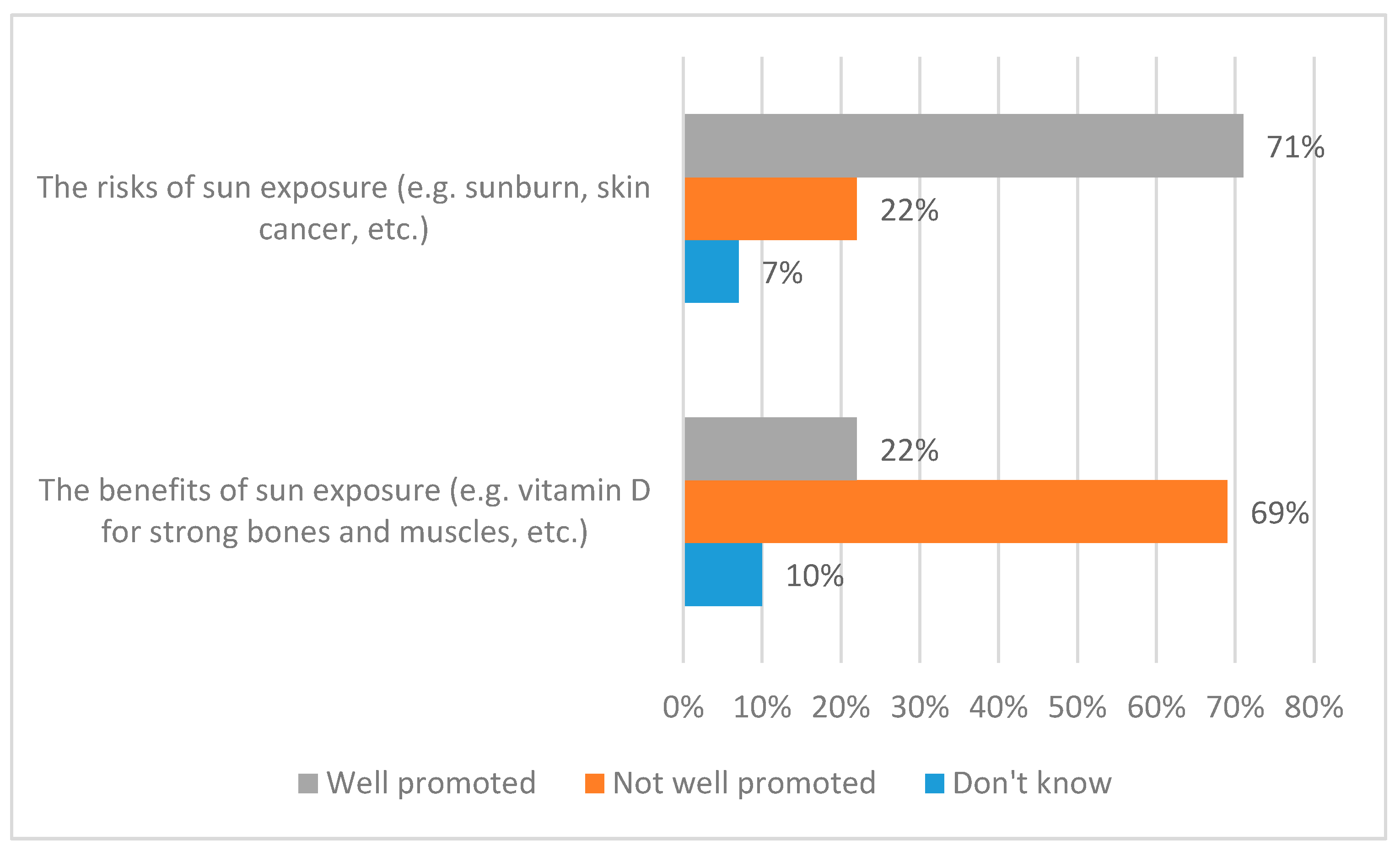
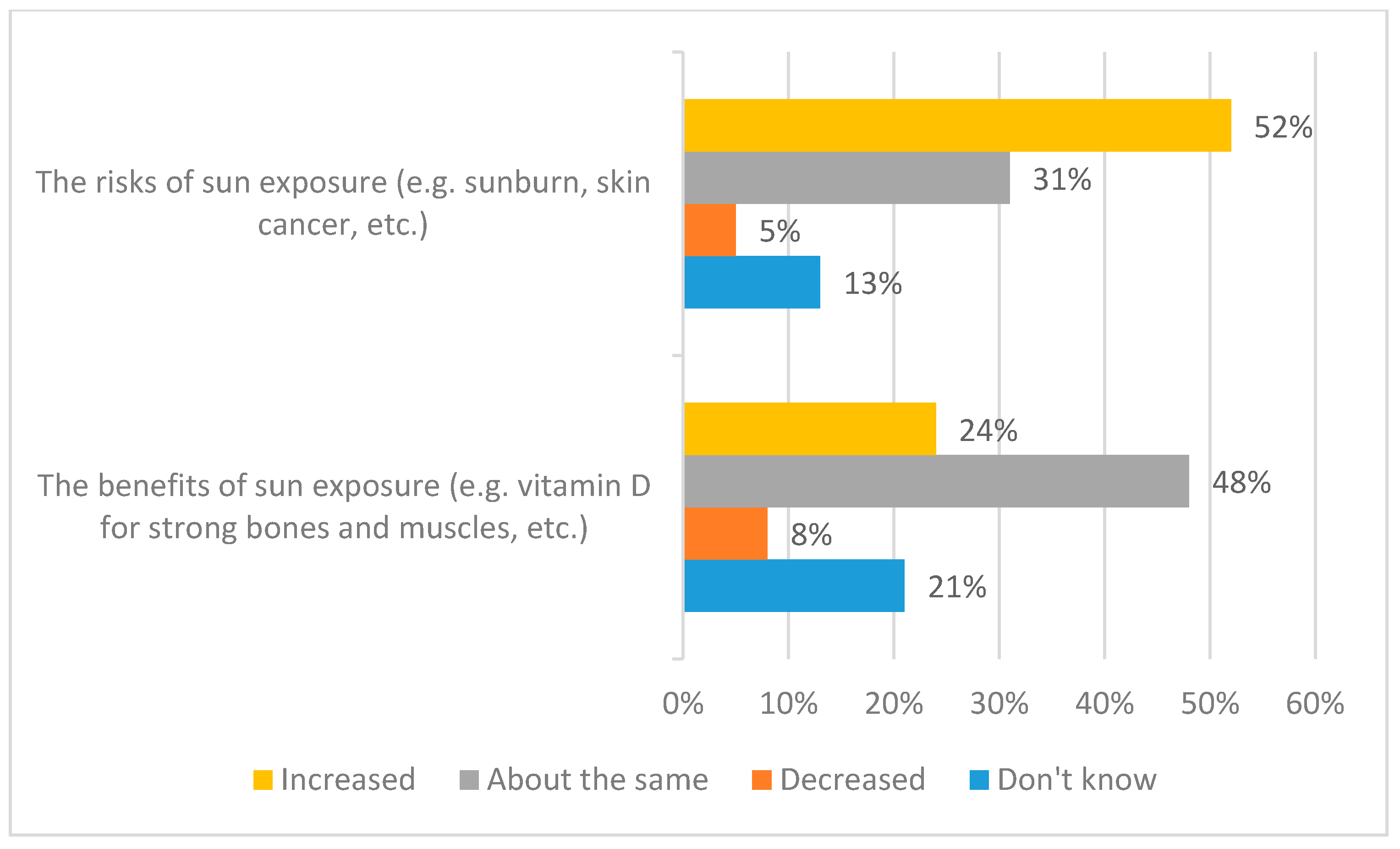
3.1. Awareness of the Promotion of Risks and Benefits
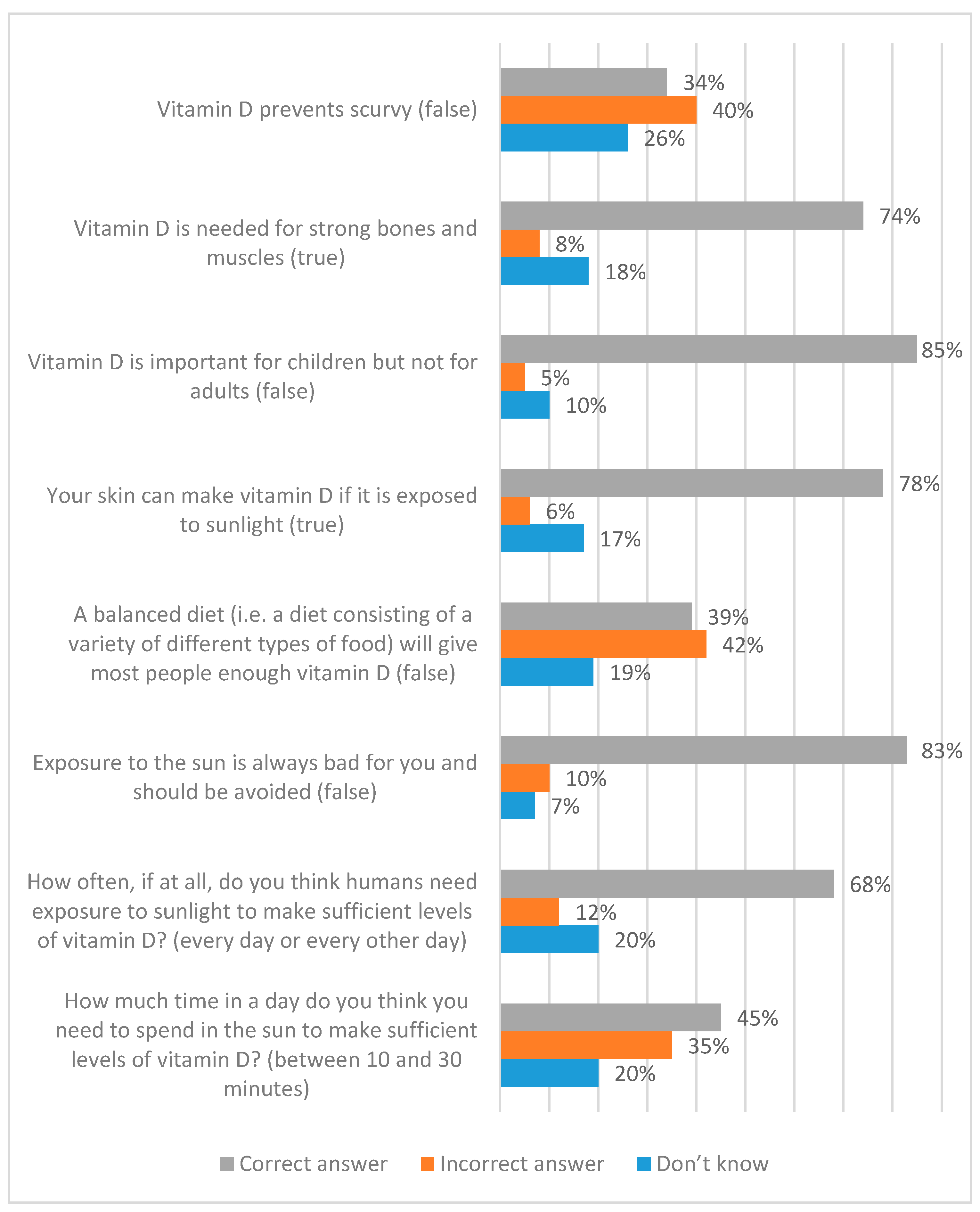
3.2. Knowledge
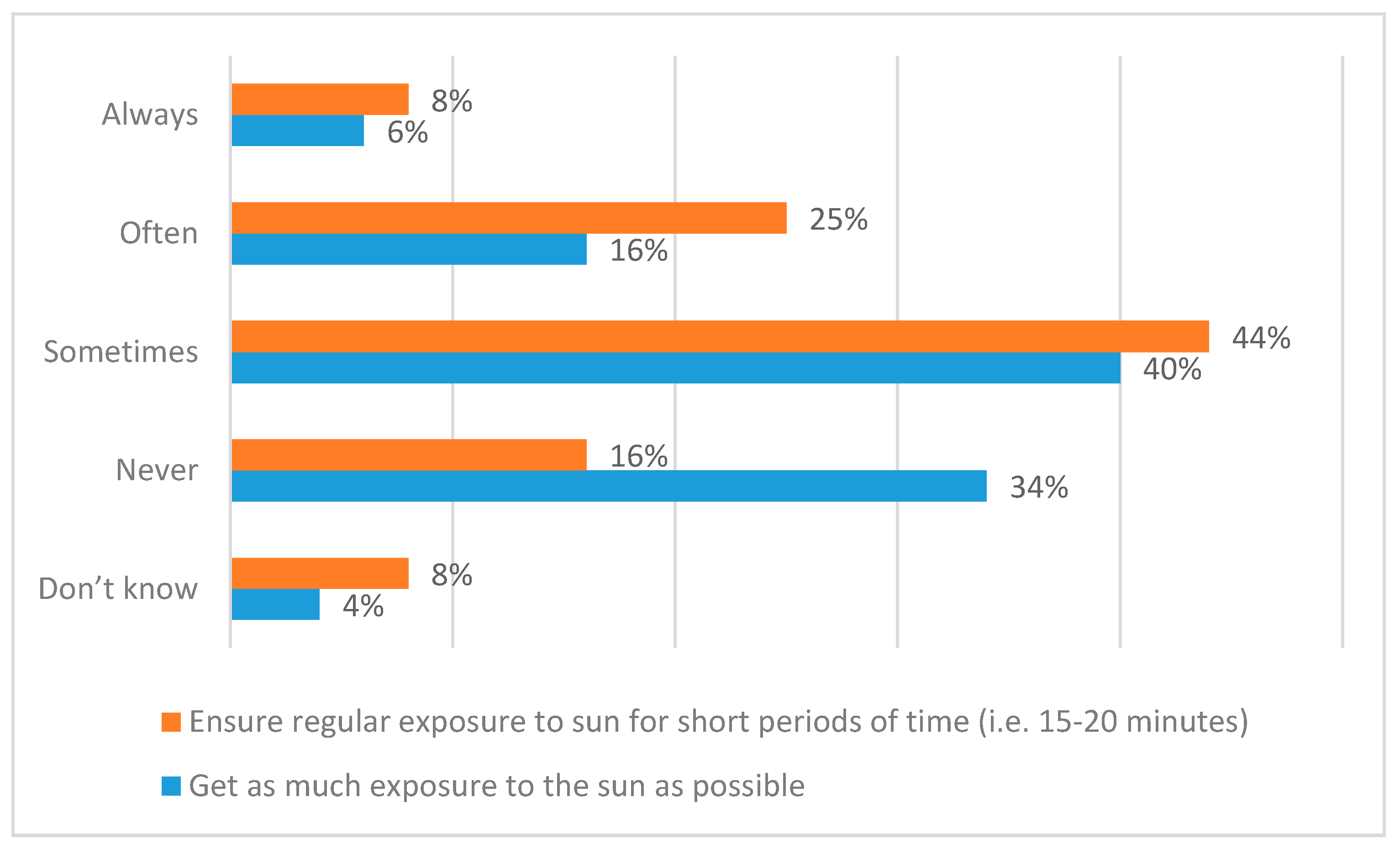
3.3. Behaviour
3.4. Demographic Characteristics
3.4.1. Introduction
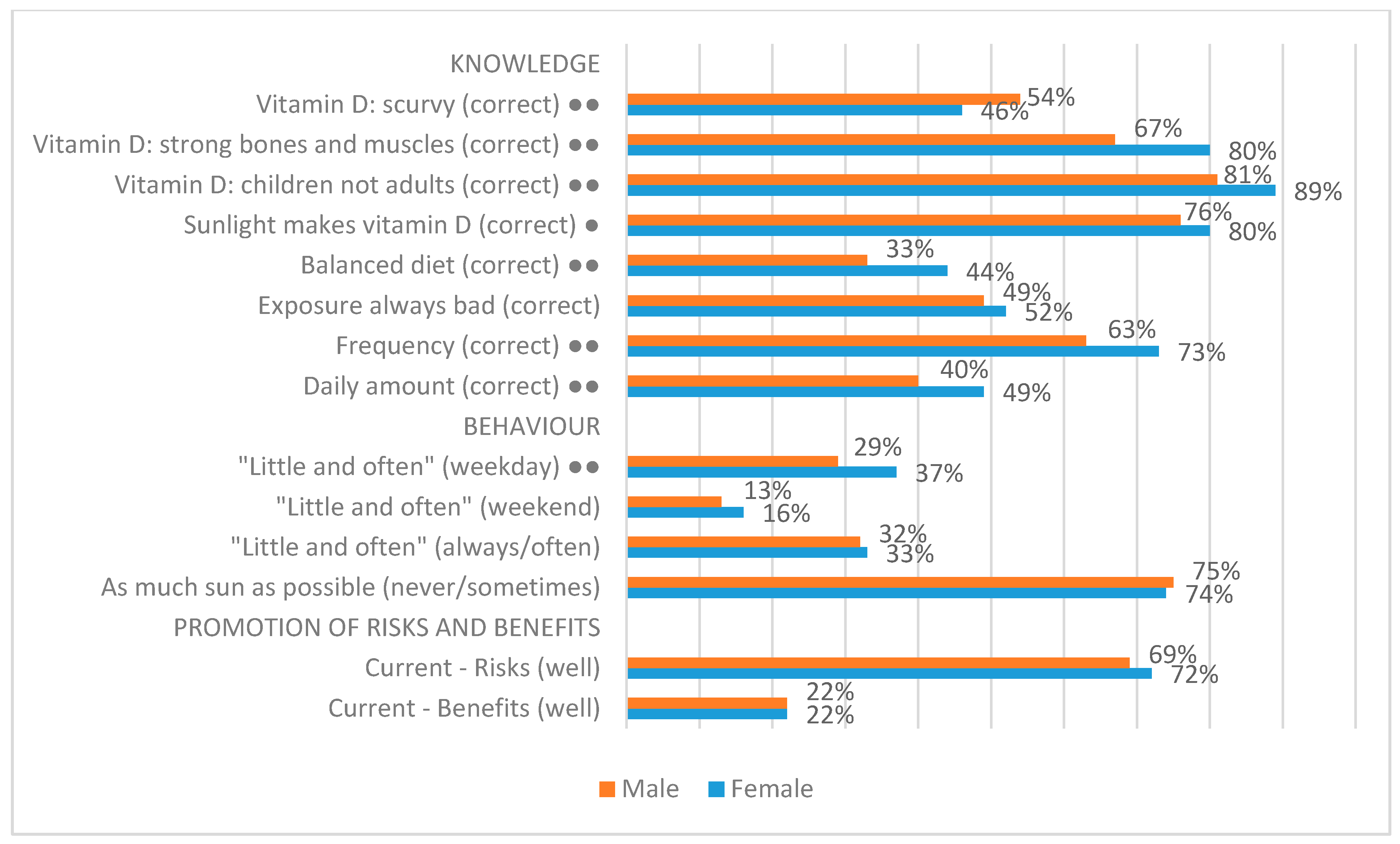
3.4.2. Gender
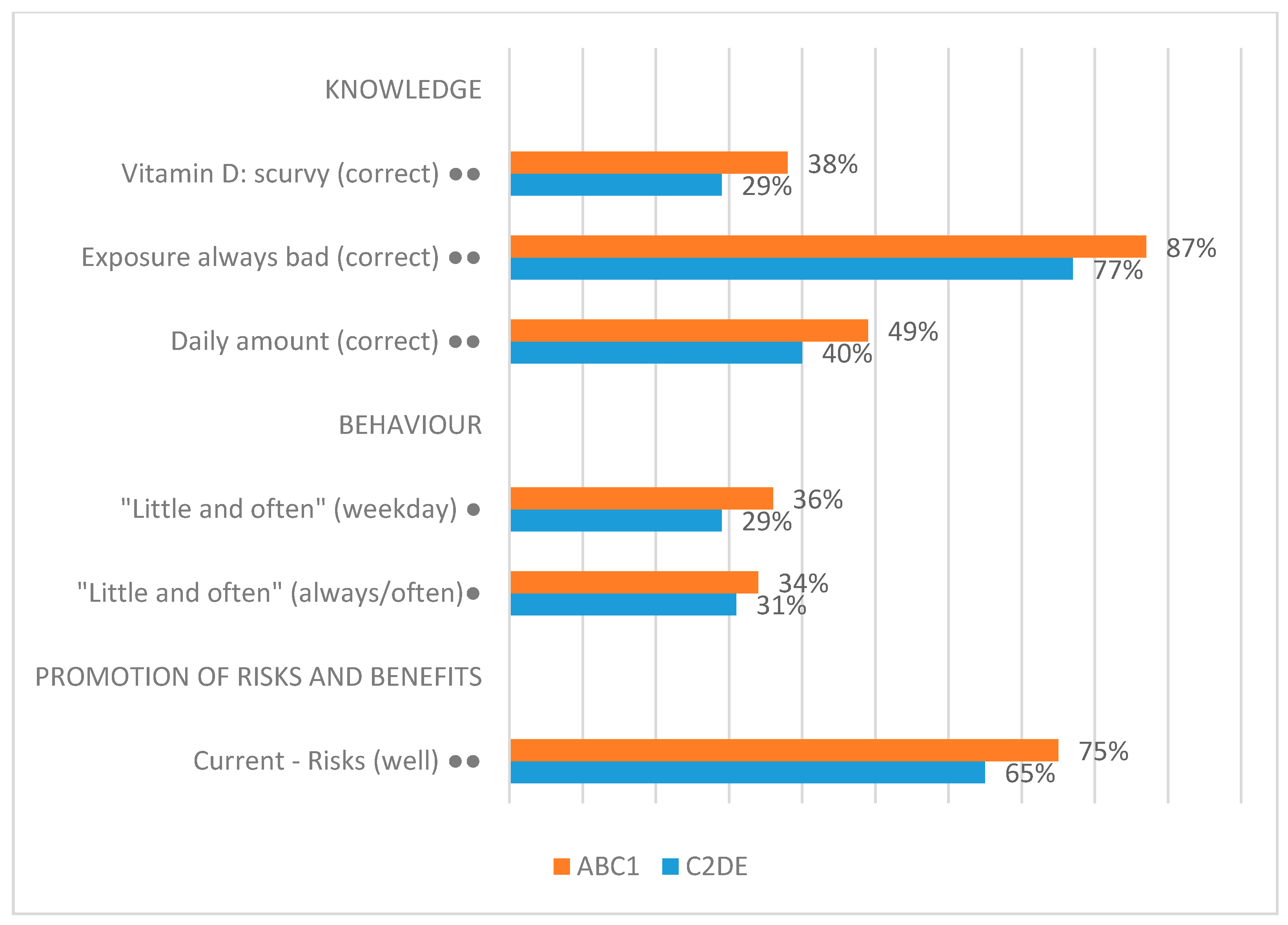
3.4.3. Socio-Economic Group
3.4.4. Other Variables
- Age: There is some evidence that older people are likely to be more knowledgeable about sunlight exposure and vitamin D than younger people. There is also evidence that people aged 55 and over—which, unfortunately, is a very large and varied category—may be more likely to exceed the levels of sunlight exposure that are recommended within the ‘little and often’ approach.
- Employment status: There is some evidence that people who are working are likely to know more about sunlight exposure and vitamin D than people who are not working (unemployed or retired). The sample is not representative by employment status.
- Skin type: As discussed earlier, we estimate that the sample is broadly representative by skin type. One implication of this is that the numbers of respondents in the darker skin categories are relatively small (see Supplementary Material File S2). There is evidence (not consistent across the relevant questions) that people with skin type VI (dark brown or black) may be likely to be more knowledgeable about sunlight exposure and vitamin D than people with lighter skin types. There is also inconsistent evidence that people with skin types I and II (those most likely to burn/least likely to tan) are more likely to conform to the prescriptions of the ‘little and often’ approach to sunlight exposure.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- DeLuca, H.F. Overview of general physiologic features and functions of vitamin D. Am. J. Clin. Nutr. 2004, 80, 1689S–1696S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scientific Advisory Committee on Nutrition. Vitamin D and Health. 2016. Available online: https://www.gov.uk/government/publications/sacn-vitamin-d-and-health-report (accessed on 31 July 2020).
- Public Health England. Ultraviolet Radiation and Vitamin D: The Effects on Health. 2017. Available online: https://www.gov.uk/government/publications/ultraviolet-radiation-and-vitamin-d-the-effects-on-health (accessed on 31 July 2020).
- Hart, P.H.; Norval, M.; Byrne, S.N.; Rhodes, L.E. Exposure to ultraviolet radiation in modulation of human diseases. Annu. Rev. Pathol. 2019, 14, 55–81. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.R.; Holick, M.F. The role of sunlight in the cutaneous production of vitamin D3. In Annual Review of Nutrition; Olson, R.E., Ed.; Annual Reviews Inc.: Palo Alto, CA, USA, 1988; Volume 8, pp. 375–399. ISBN 0-8243-2808-6. [Google Scholar]
- Oyebanjo, E.; Bushell, F. A critical evaluation of the UK SunSmart campaign and its relevance to Black and minority ethnic communities. Perspect. Public Health 2014, 134, 144–149. [Google Scholar] [CrossRef] [PubMed]
- US Institute of Medicine Food and Nutrition Board. Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- Black, L.J.; Seamans, K.M.; Cashman, K.D.; Kiely, M. An updated systematic review and meta-analysis of the efficacy of vitamin D food fortification. J. Nutr. 2012, 142, 1102–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cashman, K.D.; Kazantzidis, A.; Webb, A.R.; Keily, M. An integrated predictive model of population serum 25-hydroxycholecalciferol for application in strategy development for vitamin D deficiency prevention. J. Nutr. 2015, 145, 2419–2425. [Google Scholar] [CrossRef] [Green Version]
- British Association of Dermatologists. Vitamin D Information. 2020. Available online: https://www.skinhealthinfo.org.uk/sun-awareness/vitamin-d-information/ (accessed on 31 July 2020).
- Cancer Research UK. Sun and Vitamin D. 2020. Available online: https://www.cancerresearchuk.org/about-cancer/causes-of-cancer/sun-uv-and-cancer/sun-and-vitamin-d (accessed on 31 July 2020).
- Sunsmart, Australia. How Much Sun Is Enough? 2020. Available online: https://www.sunsmart.com.au/uv-sun-protection/how-much-sun-is-enough (accessed on 31 July 2020).
- Webb, A.R.; Kline, L.W.; Holick, M.F. Influence of season and latitude on the cutaneous synthesis of vitamin D: Exposure to winter sunlight in Boston and Edmonton will not promote vitamin D synthesis in human skin. J. Clin. Endocrinol. Metabol. 1988, 67, 373–378. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Clinical Excellence. NICE Guideline NG34: Sunlight Exposure: Risks and Benefits. 2016. Available online: https://www.nice.org.uk/guidance/ng34 (accessed on 31 July 2020).
- Rhodes, L.E.; Webb, A.R.; Fraser, H.; Kift, R.; Durkin, M.; Allan, D.; O’Brien, S.; Vail, A.; Berry, J.L. Recommended summer sunlight exposure levels can produce sufficient (≥20 ng ml-1) but not the proposed optimal (≥32 ng ml-1) 25(OH)D levels at UK latitudes. J. Investig. Dermatol. 2010, 130, 1411–1418. [Google Scholar] [CrossRef]
- Webb, A.R.; Kazantzidis, A.; Kift, R.; Farrar, M.D.; Wilkinson, J.; Rhodes, L.E. Meeting vitamin D requirements in white Caucasians at UK latitudes: Providing a choice. Nutrients 2018, 10, 497. [Google Scholar] [CrossRef] [Green Version]
- Webb, A.R.; Kazantzidis, A.; Kift, R.; Farrar, M.D.; Wilkinson, J.; Rhodes, L.E. Colour counts: Sunlight and skin type as drivers of vitamin D deficiency at UK latitudes. Nutrients 2018, 10, 457. [Google Scholar] [CrossRef] [Green Version]
- Webb, A.R.; Kift, R.; Durkin, M.; O’Brien, S.; Vail, A.; Berry, J.L.; Rhodes, L.E. The role of sunlight exposure in determining the vitamin D status of the UK white Caucasian adult population. Br. J. Dermatol. 2010, 163, 1050–1055. [Google Scholar] [CrossRef]
- Farrar, M.D.; Kift, R.; Felton, S.J.; Berry, J.L.; Durkin, M.; Allan, D.; Vail, A.; Webb, A.R.; Rhodes, L.E. Recommended summer sunlight exposure levels fail to produce sufficient vitamin D status in UK adults of South Asian origin. Am. J. Clin. Nutr. 2011, 94, 1219–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrar, M.D.; Webb, A.R.; Kift, R.; Durkin, M.; Allan, D.; Herbert, A.; Berry, J.L.; Rhodes, L.E. Efficacy of a dose-range of simulated sunlight exposures in raising vitamin D status in South Asian adults: Implications for targeted guidance on sun exposure. Am. J. Clin. Nutr. 2013, 97, 1210–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kift, R.; Berry, J.L.; Vail, A.; Durkin, M.; Rhodes, L.E.; Webb, A.R. Lifestyle factors including less cutaneous sun exposure contribute to starkly lower vitamin D status in UK South Asians compared to the white Caucasian population. Br. J. Dermatol. 2013, 169, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, L.E.; Webb, A.R.; Berry, J.L.; Felton, S.J.; Marjanovic, E.; Wilkinson, J.; Vail, A.; Kift, R. Sunlight exposure behaviour and vitamin D status in photosensitive patients: Longitudinal comparative study with healthy individuals at UK latitude. Br. J. Dermatol. 2014, 171, 1478–1486. [Google Scholar] [CrossRef]
- Felton, S.J.; Cooke, M.S.; Kift, R.; Berry, J.L.; Webb, A.R.; Lam, P.; de Gruijl, F.R.; Vail, A.; Rhodes, L.E. Concurrent beneficial (vitamin D production) and hazardous (cutaneous DNA damage) impact of repeated low-level summer sunlight exposures. Br. J. Dermatol. 2016, 175, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Shih, B.B.; Farrar, M.D.; Cooke, M.S.; Osman, J.; Langton, A.; Kift, R.; Webb, A.R.; Berry, J.L.; Watson, R.E.; Vail, A.; et al. Fractional sunburn threshold UVR doses generate equivalent vitamin D and DNA damage in skin types I-VI, but with epidermal DNA damage gradient correlated to skin darkness. J. Investig. Dermatol. 2018, 138, 2244–2252. [Google Scholar] [CrossRef] [Green Version]
- Manson, J.; Brannon, P.; Rosen, C.; Taylor, C. Vitamin D deficiency—Is there really a pandemic? N. Engl. J. Med. 2016, 375, 1817–1820. [Google Scholar] [CrossRef] [PubMed]
- Van Shoor, N.; Lips, P. Worldwide vitamin D Status. In Vitamin D, 4th ed.; Feldman, D., Ed.; Academic Pross: London, UK, 2018; Volume 2, ISBN 978-0-12-809963-6. [Google Scholar]
- Sahota, O. Understanding vitamin D deficiency. Age Age. 2014, 43, 589–591. [Google Scholar] [CrossRef] [Green Version]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; González-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [Green Version]
- Public Health England. NDNS: Time Trend and Income Analyses for Years 1 to 9. Public Health England; 2019. Available online: https://www.gov.uk/government/statistics/ndns-time-trend-and-income-analyses-for-years-1-to-9 (accessed on 31 July 2020).
- NHS. Hospital Admitted Patient Care Activity Statistics. 2019. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/hospital-admitted-patient-care-activity (accessed on 31 July 2020).
- Forrest, Y.; Stuhldreher, W. Prevalence and correlates of vitamin D deficiency in US adults. Nutr. Res. 2011, 31, 48–54. [Google Scholar] [CrossRef]
- Daly, R.M.; Gagnon, C.; Lu, Z.X.; Magliano, D.J.; Dunstan, D.W.; Sikaris, K.A.; Zimmet, P.Z.; Ebeling, P.R.; Shaw, J.E. Prevalence of vitamin D deficiency and its determinants in Australian adults aged 25 years and older: A national, population-based study. Clin. Endocrinol. 2011, 77, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Kotta, S.; Gadhvi, D.; Jakeways, N.; Saeed, M.; Sohanpal, R.; Hull, S.A.; Famakin, O.; Martineau, A.; Griffiths, C. “Test me and treat me”—Attitudes to vitamin D deficiency and supplementation: A qualitative study. BMJ Open 2015, 5, e007401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonevski, B.; Bryant, J.; Lambert, S.; Brozek, I.; Rock, V. The ABC of vitamin D: A qualitative study of the knowledge and attitudes regarding vitamin D deficiency amongst selected population groups. Nutrients 2013, 5, 915–927. [Google Scholar] [CrossRef] [PubMed]
- Ho-Pham, L.; Nguyen, M. Survey on knowledge and attitudes on vitamin D and sunlight exposure in an urban population in Vietnam. J. ASEAN Fed. Endoc. Soc. 2012, 27, 191–195. [Google Scholar]
- Janda, M.; Youl, P.; Bolz, K.; Niland, C.; Kimlin, M. Knowledge about health benefits of vitamin D in Queensland Australia. Prev. Med. 2010, 50, 215–216. [Google Scholar] [CrossRef]
- Rutkowski, D.; Farrar, M.D.; Osman, J.E.; Webb, A.R.; Rhodes, L.E. A qualitative study of the knowledge, behaviour and attitudes of patients with skin cancer regarding sunlight exposure and vitamin D. Photodermatol. Photoimmunol. Photomed. 2017, 33, 203–208. [Google Scholar] [CrossRef]
- Kung, A.; Lee, K. Knowledge of vitamin D and perceptions and attitudes toward sunlight among Chinese middle-aged and elderly women: A population survey in Hong Kong. BMC Public Health 2006, 6, 226. [Google Scholar] [CrossRef] [Green Version]
- Vu, L.; van der Pols, J.; Whiteman, D.; Kimlin, M.; Neale, R. Knowledge and attitudes about Vitamin D and impact on sun protection practices among urban office workers in Brisbane, Australia. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1784–1789. [Google Scholar] [CrossRef] [Green Version]
- Aljerfree, N.; Lee, P.; Ahmed, F. Exploring knowledge and attitudes about vitamin D among adults in Saudi Arabia: A qualitative study. Healthcare 2017, 5, 76. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, C.; Glatt, D.; White, L.; Revuelta Iniesta, R. Knowledge, attitudes and perceptions towards vitamin D in a UK adult population: A cross-sectional study. Int. J. Environ. Res. Public Health 2018, 15, 2387. [Google Scholar] [CrossRef] [Green Version]
- Kyle, R.G.; Macmillan, I.; Forbat, L.; Neal, R.D.; O’Carroll, R.E.; Haw, S.; Hubbard, G. Scottish adolescents’ sun-related behaviours, tanning attitudes and associations with skin cancer awareness: A cross-sectional study. BMJ Open. 2014, 4, e005137. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, T.B. The validity and practicality of sun-reactive skin type I through VI. Arch. Dermatol. 1988, 124, 869–871. [Google Scholar] [CrossRef] [PubMed]
- Lucas, R.; Rodney-Harris, R. Benefits of Sun Exposure: Vitamin D and Beyond. NIWA UV Workshop, Wellington. 4–6 April 2018. Available online: https://niwa.co.nz/sites/niwa.co.nz/files/Lucas_BenefitsofSun.pdf (accessed on 9 September 2020).








© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burchell, K.; Rhodes, L.E.; Webb, A.R. Public Awareness and Behaviour in Great Britain in the Context of Sunlight Exposure and Vitamin D: Results from the First Large-Scale and Representative Survey. Int. J. Environ. Res. Public Health 2020, 17, 6924. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186924
Burchell K, Rhodes LE, Webb AR. Public Awareness and Behaviour in Great Britain in the Context of Sunlight Exposure and Vitamin D: Results from the First Large-Scale and Representative Survey. International Journal of Environmental Research and Public Health. 2020; 17(18):6924. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186924
Chicago/Turabian StyleBurchell, Kevin, Lesley E. Rhodes, and Ann R. Webb. 2020. "Public Awareness and Behaviour in Great Britain in the Context of Sunlight Exposure and Vitamin D: Results from the First Large-Scale and Representative Survey" International Journal of Environmental Research and Public Health 17, no. 18: 6924. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186924