Thermal Sensation in Older People with and without Dementia Living in Residential Care: New Assessment Approaches to Thermal Comfort Using Infrared Thermography

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Size
2.3. Participants
2.4. Screening and Recruitment Pathway
2.5. Recruitment
2.6. Data Collection
2.6.1. Demographic Data
2.6.2. Frailty Assessment
2.6.3. Body Temperature Measurement
2.6.4. Past Medical History (PMH) and Current Medications
2.6.5. Indoor Environment
2.6.6. Clothing
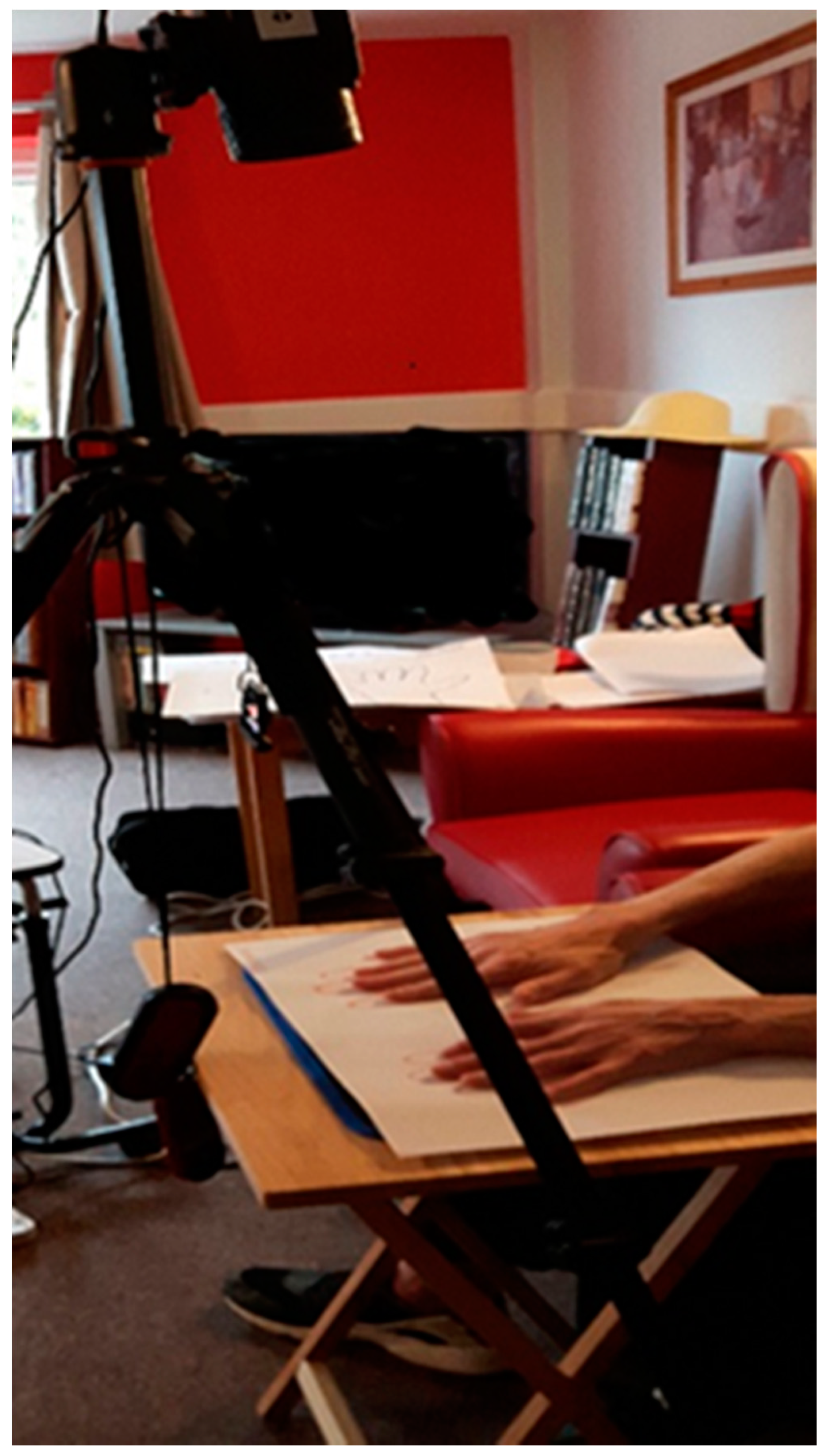
2.6.7. Imaging-Long Wave Infrared (LWIR) Thermography
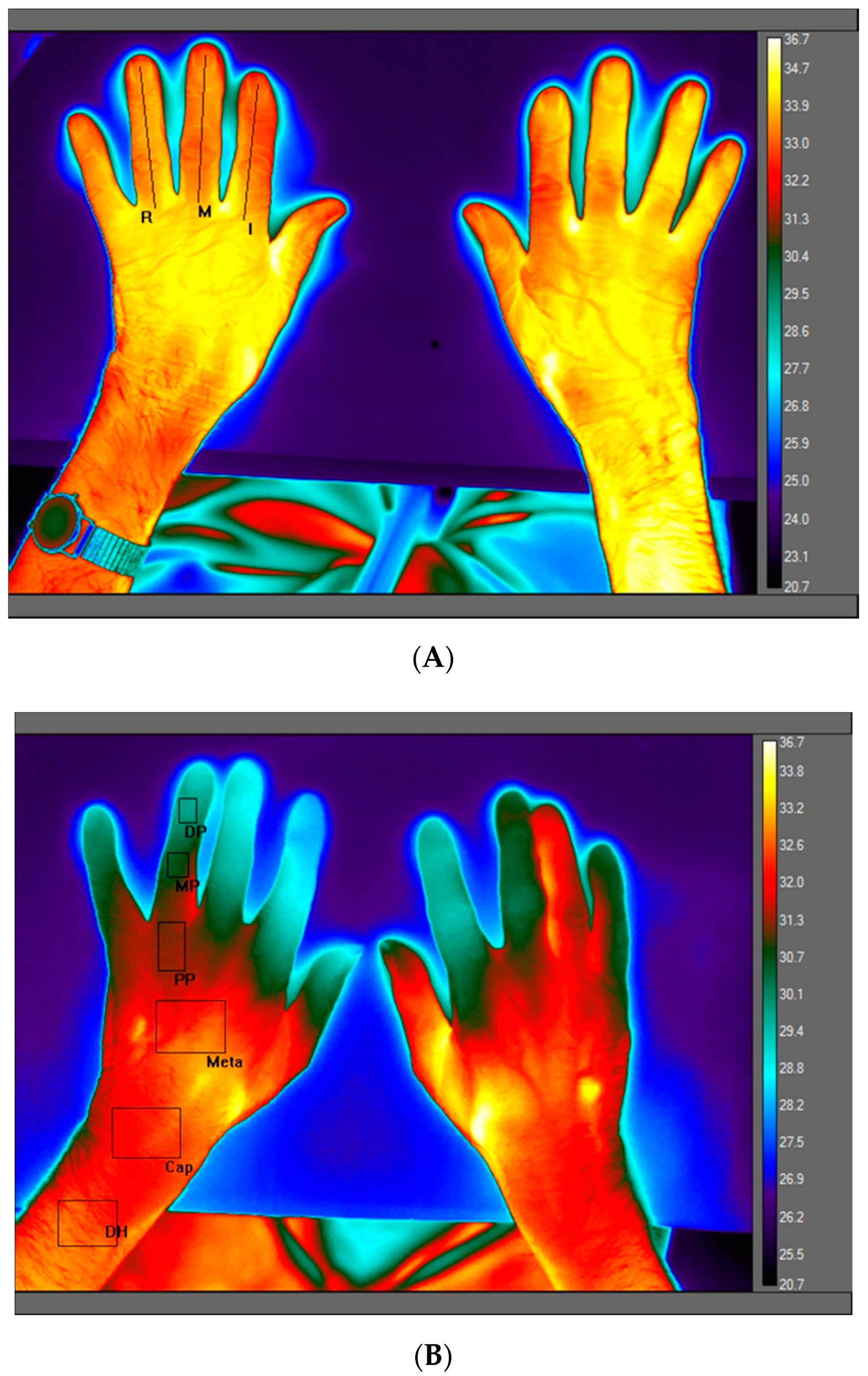
2.6.8. LWIR Region of Interest (ROI) and Image Processing
2.6.9. Calibration
2.6.10. Warmth Sensation Rating
2.6.11. Statistical Analyses
2.7. Ethics Approval, Screening and Recruitment
3. Results
3.1. Characteristics of Older Adults Living in Residential Care
3.2. Thermal Sensation (TS) Self-Rating
3.3. Thermal Sensation Ratings and Clothing Insulation
3.4. Core (Tympanic) Temperature
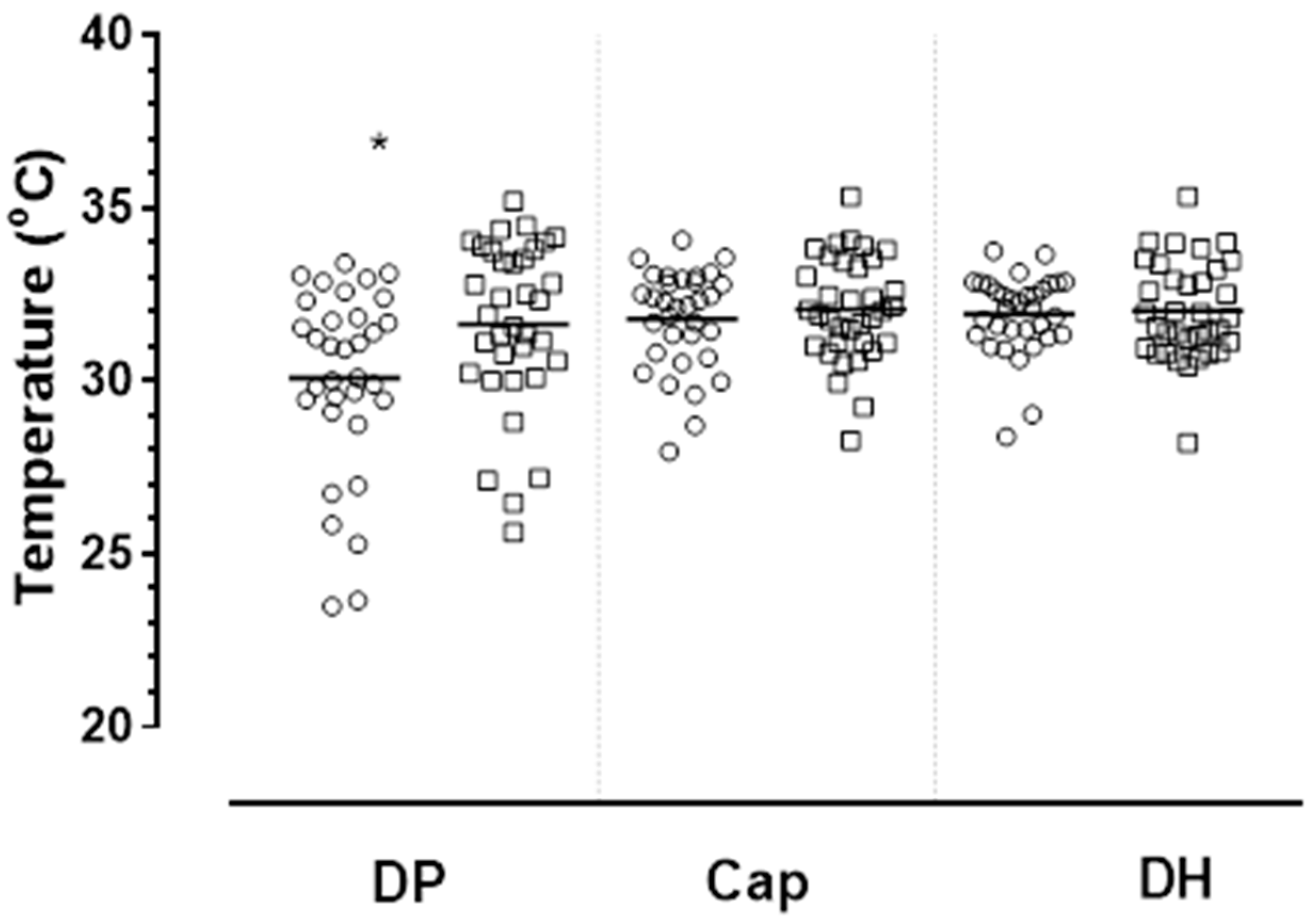
3.5. Skin Extremity Temperature
3.6. Comparisons Between Groups
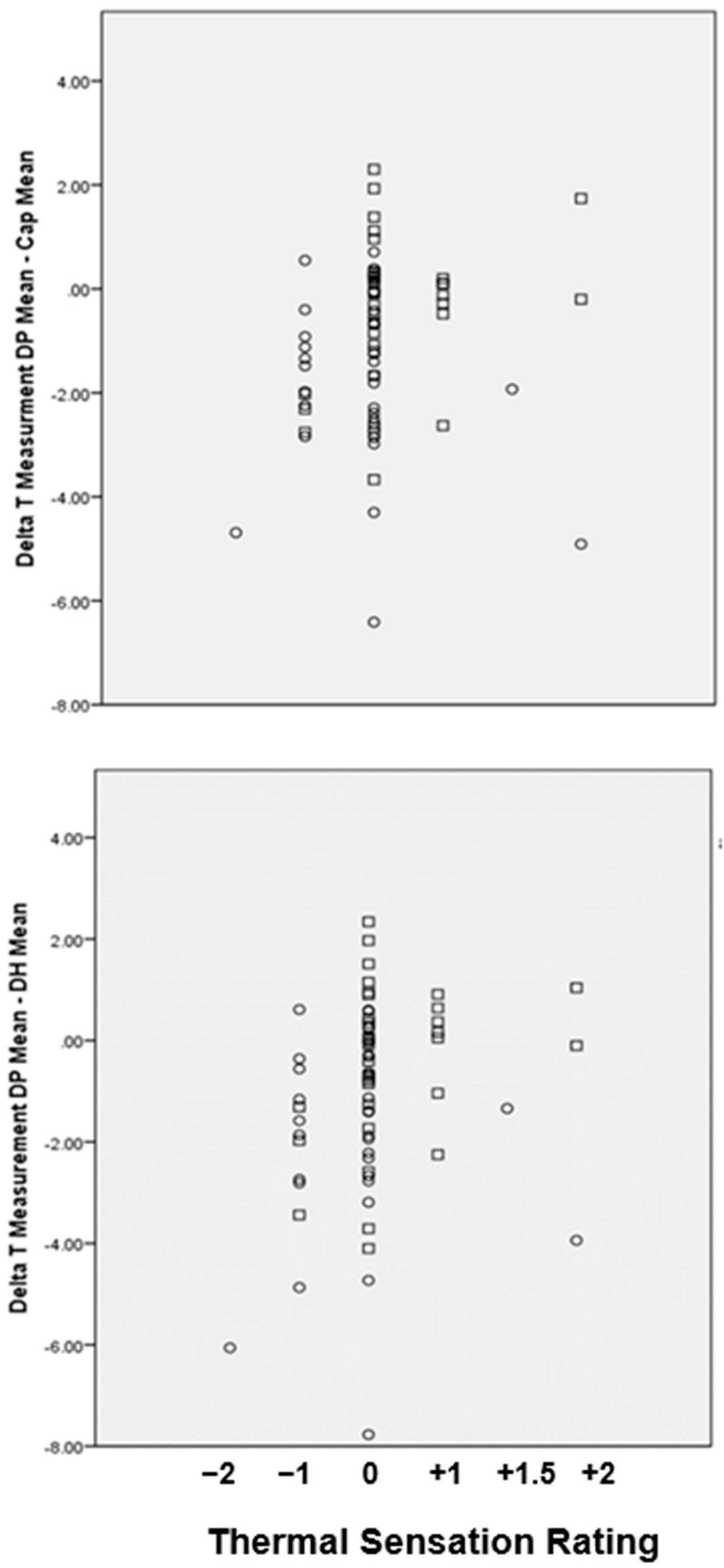
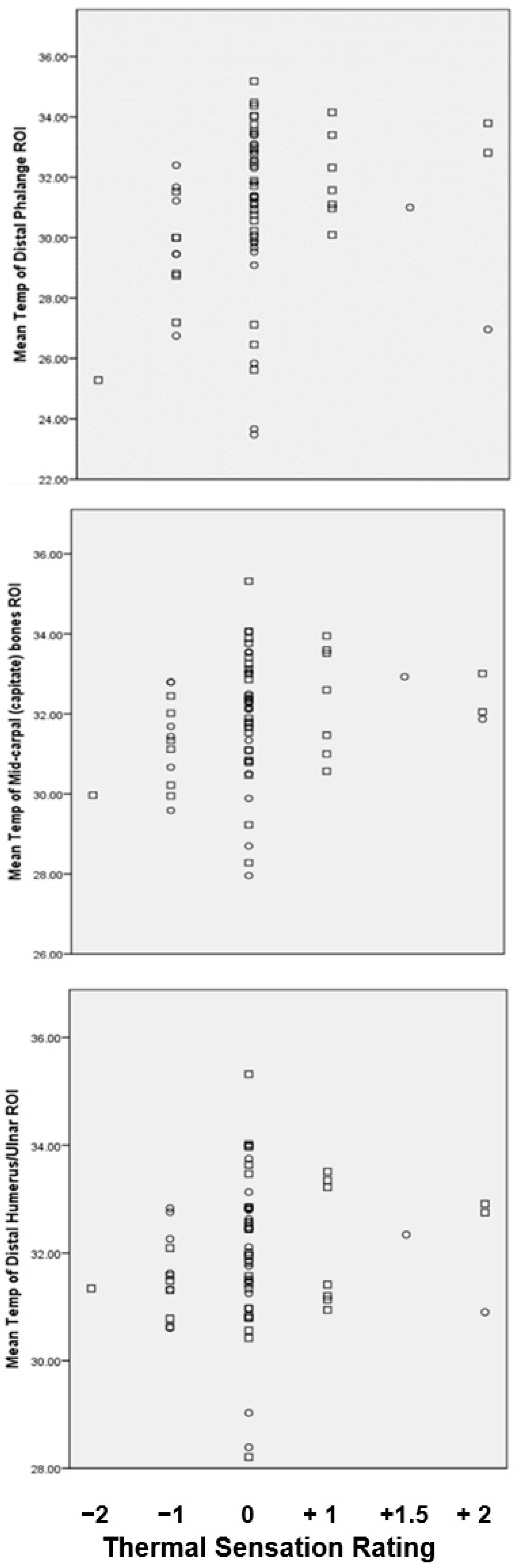
3.7. Extremity Temperature Values and Thermal Sensation Rating
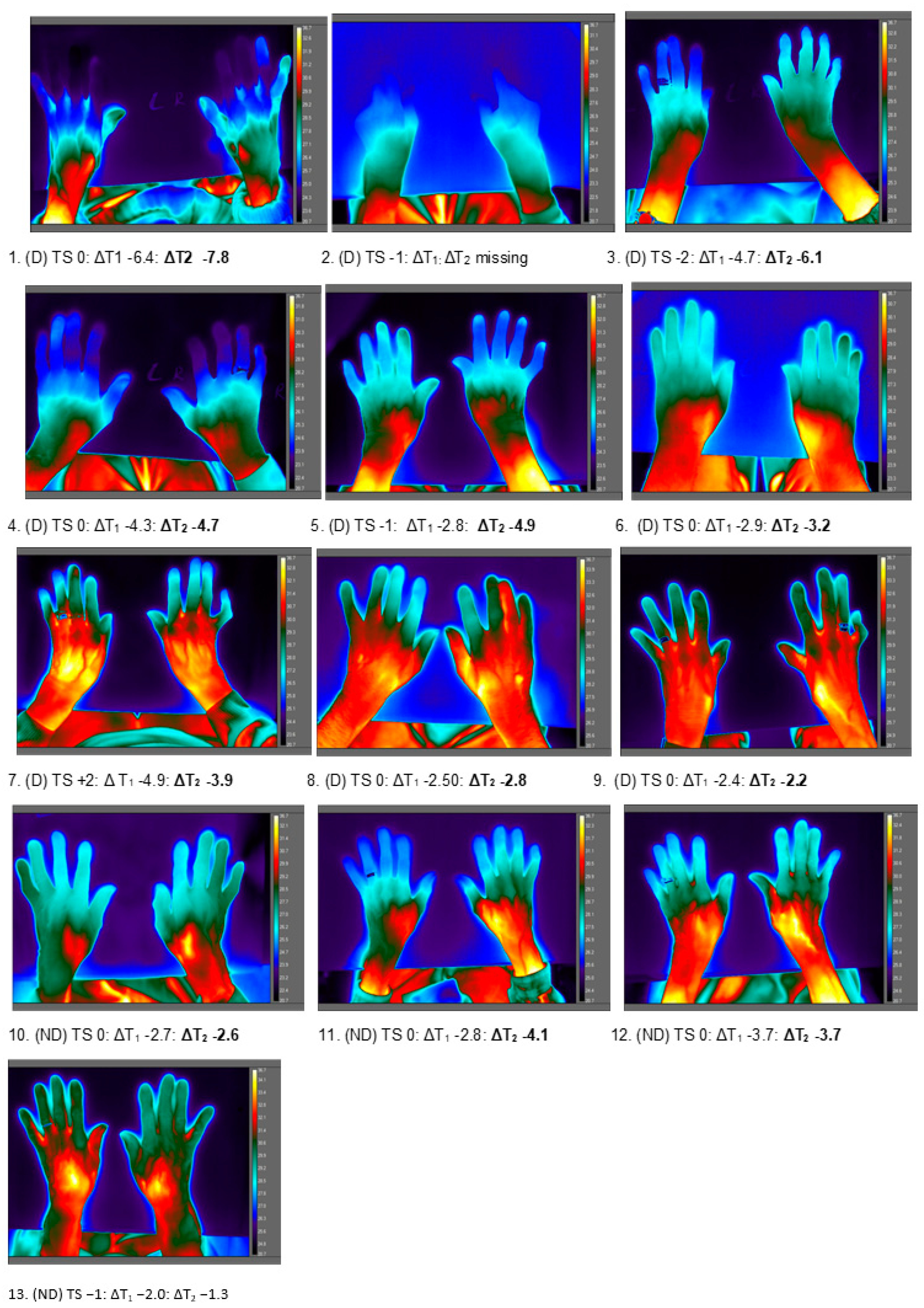
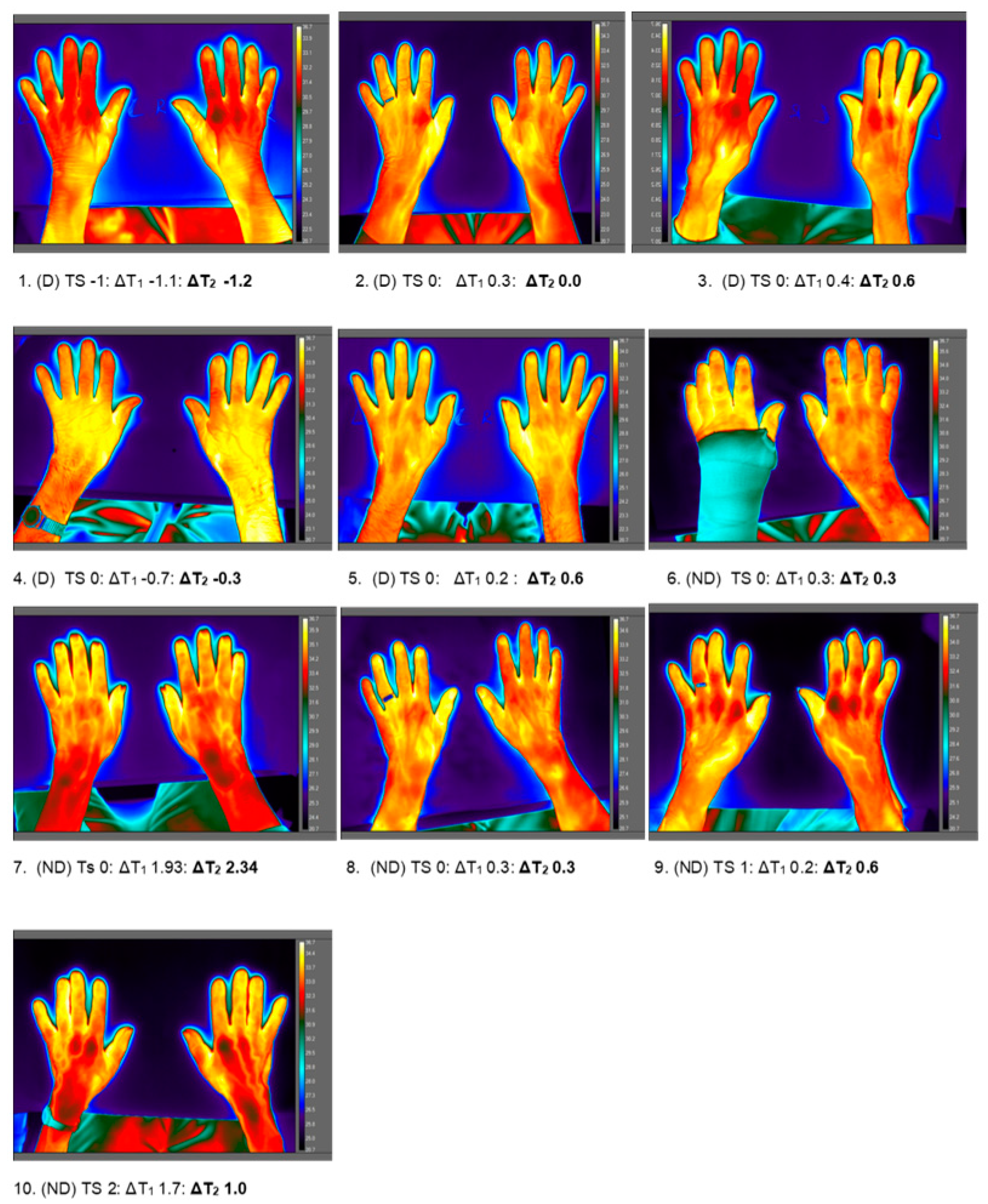
3.8. Thermal Mapping of Extremities: Correspondence Between the Thermal Map and Thermal Sensation Report
3.9. Medical History and Medications with Potential Influence on Perception of Temperature and Thermal Appearance
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AMT | Abbreviated Mental Test |
| ASHRAE | American Society of Heating, Refrigerating and Air-Conditioning Engineers |
| CIT | Cold induced thermogenesis |
| Clo | clothing insulation unit |
| CRN | clinical research network |
| Icl | overall insulation of assembly in Clo units (Clo) |
| FOV | field of view |
| LWIR | long wave infrared thermography |
| PMH | past medical history |
| RH | relative humidity |
| ROI | region of interest |
| SD | standard deviation |
| Ta | air temperature |
| Tr | rectal temperature |
| TDP | distal phalange skin temperature |
| TCAP | capitate bones skin temperature |
| TDH | distal humerus/ulnar skin temperature |
| Ttymp | tympanic membrane temperature |
| TV | thermal vote |
| Δ | delta |
| ΔT | temperature difference |
| UK | United Kingdom of Great Britain and Northern Ireland |
| TC | thermal comfort |
| TS | thermal sensation |
References
- Garre-Olmo, J.; Lopez-Pousa, S.; Turon-Estrada, A.; Juvinya, D.; Ballester, D.; Vilalta-Franch, J. Environmental determinants of quality of life in nursing home residents with severe dementia. J. Am. Geriatr. Soc. 2012, 60, 1230–1236. [Google Scholar] [CrossRef] [PubMed]
- Bills, R.; Soebarto, V.; Williamson, T. Thermal experiences of older people during hot conditions in Adelaide. In Fifty Years Later: Revisiting the Role of Architectural Science in Design and Practice: 50th International Conference of the Architectural Science Association, Adelaide, Australia, 6–9 December 2016; School of Architecture and Built Environment, The University of Adelaide: Adelaide, Australia, 2016; pp. 657–664. [Google Scholar]
- Van Hoof, J.H.B.; Hansen, A.; Kazak, J.K.; Soebarto, V. The living environment and thermal behaviours of older south Australians. Int. J. Environ. Public Health Res. 2019, 16, 935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ASHRAE: Standard 55-2013. Thermal Environmental Conditions for Human Occupancy; The American Society of Heating, Refrigerating and Air-Conditioning Engineers: Atlanta, GA, USA, 2013. [Google Scholar]
- International Standards Organisation (ISO). Ergonomics of the Thermal Environment–Analytical Determination and Interpretation of Thermal Comfort Using Calculation of the PMV And PPD Indices and Local Thermal Comfort Criteria; ISO 7730; ISO Standardization: Geneva, Switzerland, 2015. [Google Scholar]
- Bedford, T. The Warmth Factor in Comfort at Work. In A Physiological Study of Heating and Ventilation; H.M.S.O.: London, UK, 1936. [Google Scholar]
- Parsons, K.C. Human response to thermal environments Principles and methods. In Evaluation of Human Work; Wilson, J.R., Corlett, E.N., Eds.; Taylor and Francis: London, UK, 1990. [Google Scholar]
- Childs, C.; Gwilt, A.; Sherriff, G.; Homer, C. Old and Cold: Challenges in the Design of Personalised Thermal Comfort at Home. In Proceedings of the 3rd European Conference on Design4Health, Sheffield, UK, 13–16 July 2015; ISBN 978-1-84387-385-3. [Google Scholar]
- Cleary, M.; Raeburn, T.; West, S.; Childs, C. The environmental temperature of the residential care home: Role in thermal comfort and mental health. Contemp. Nurse 2019, 55, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Walker, G.; Brown, S.; Neven, L. Thermal comfort in care homes: Vulnerability, responsibility and ‘thermal care’. Build. Res. Inf. 2016, 44, 135–146. [Google Scholar] [CrossRef] [Green Version]
- Van Hoof, J.; Schellen, L.; Soebarto, V.; Wong, J.K.W.; Kazak, J.K. Ten questions concerning thermal comfort and ageing. Build. Environ. 2017, 120, 123–133. [Google Scholar] [CrossRef]
- Iommi, M.; Barbera, E. Thermal Comfort for older adults. An experimental study on the thermal requirements for older adults. In Proceedings of the CISBAT Conference, Lausanne, Switzerland, 9–11 September 2015; pp. 357–362. [Google Scholar]
- Schellen, L.; van Marken Lichtenbelt, W.; Loomans, M.G.L.C.; Frijns, A.; Toftum, J.; deWit, M. Thermal comfort physiological responses and performance of elderly during exposure to a moderate temperature drift. In Proceedings of the 9th International Conference and Exhibition on Healthy Buildings 2009 (HB09), Syracuse, NY, USA, 13–17 September 2009. [Google Scholar]
- Szekely, M.; Garai, J. Thermoregulation and age. In Handbook of Clinical Neurology; Thermoregulation: From basic Neuroscience to Clinical Neurology Part 1; Romanovsky, A., Ed.; Elsevier B.V.: Amsterdam, The Netherlands, 2018; Volume 156, pp. 715–725. [Google Scholar]
- Taylor, N.A.S.; Allsopp, N.K.; Parkes, D.G. Preferred Room Temperature of Young vs. Aged Males: The Influence of Thermal Sensation, Thermal Comfort, and Affect. J. Gerontol. Ser. A 1995, 50, M216–M221. [Google Scholar] [CrossRef]
- Blatteis, C.M. Age-dependent changes in temperature regulation—A mini review. Gerontology 2012, 58, 289–295. [Google Scholar] [CrossRef]
- Holowatz, L.A.; Thompson-Torgerson, C.; Kenney, W.L. Aging and the control of human skin blood flow. Front. Biosci. 2010, 15, 718–739. [Google Scholar] [CrossRef] [Green Version]
- Lloyd, E.L. Hypothermia and Cold Stress; Croom Helm: London, UK, 1986. [Google Scholar]
- Hodkinson, H.M. Evaluation of a mental test score for assessment of mental impairment in the elderly. Age Ageing 1972, 1, 233–238. [Google Scholar] [CrossRef]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Parsons, K. The thermal properties of clothing. In Human Thermal Environments; CRC Press: London, UK, 2014. [Google Scholar]
- McIntyre, D.A. Thermal sensation. A comparison of rating scales and cross modality matching. Int. J. Biometeorol. 1976, 20, 295. [Google Scholar] [CrossRef] [PubMed]
- Pathak, K.; Calton, E.K.; Soares, M.J.; Zhao, Y.; James, A.P.; Keane, K.; Newsholme, P. Forearm to fingertip skin temperature gradients in the thermoneutral zone were significantly related to resting metabolic rate: Potential implications for nutrition research. Eur. J. Clin. Nutr. 2017, 71, 1074–1079. [Google Scholar] [CrossRef] [PubMed]
- Soebarto, V.; Zhang, H.; Schiavon, S. A thermal comfort environmental chamber study of older and younger people. Build. Environ. 2019, 155, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Stephan, B.C.; Matthews, F.E.; Khaw, K.T.; Dufouil, C.; Brayne, C. Beyond mild cognitive impairment: Vascular cognitive impairment, no dementia (VCIND). Alzheimer’s Res. Ther. 2009, 1, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Vos, S.J.; Verhey, F.; Frölich, L.; Kornhuber, J.; Wiltfang, J.; Maier, W.; Peters, O.; Rüther, E.; Nobili, F.; Morbelli, S.; et al. Prevalence and prognosis of Alzheimer’s disease at the mild cognitive impairment stage. Brain 2015, 138, 1327–1338. [Google Scholar] [CrossRef] [Green Version]
- Blennow, K.; Zetterberg, H. Biomarkers for Alzheimer’s disease: Current status and prospects for the future. J. Intern. Med. 2018, 284, 643–663. [Google Scholar] [CrossRef] [Green Version]
- Tartarini, F.; Cooper, P.; Fleming, R.; Batterham, M. Indoor air temperature and agitation of nursing home residents with dementia. Am. J. Alzheimer’s Dis. Dement. 2017, 32, 272–281. [Google Scholar] [CrossRef] [Green Version]
- Day, K.; Carreon, D.; Stump, C. The Therapeutic Design of Environments for People with Dementia: A Review of the Empirical Research. Gerontology 2000, 40, 397–416. [Google Scholar]
- Wang, Z.; He, Y.; Hou, J.; Jiang, L. Human skin temperature and thermal responses in asymmetrical cold radiation environments. Build. Environ. 2013, 67, 217–223. [Google Scholar] [CrossRef]
- Liu, W.; Lian, Z.; Deng, Q. Use of mean skin temperature in evaluation of individual thermal comfort for a person in a sleeping posture under steady thermal environment. Indoor Built Environ. 2014, 24, 489–499. [Google Scholar] [CrossRef]
- Sakoi, T.; Tsuzuki, K.; Kato, S.; Ooka, R.; Song, D.; Zhu, S. Thermal comfort, skin temperature distribution, and sensible heat loss distribution in the sitting posture in various asymmetric radiant fields. Build. Environ. 2007, 42, 3984–3999. [Google Scholar] [CrossRef]
- Wang, D.; Zhang, H.; Arens, E.; Huizenga, C. Observations of upper-extremity skin temperature corresponding overall-body thermal sensations and comfort. Build. Environ. 2007, 42, 3933–3943. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; Li, N.; Cui, H.; Peng, J.; Chen, H.; Liu, P. Using Upper Extremity Skin Temperatures to Assess Thermal Comfort in Office Buildings in Changsha, China. Int. J. Environ. Res. Public Health 2017, 14, 1092. [Google Scholar]
- Horvath, S.; Radcliffe, C.E.; Hutt, B.K.; Spurr, G.B. Metabolic response of old people to a cold environment. J. Appl. Physiol. 1955, 8, 45–148. [Google Scholar] [CrossRef] [PubMed]
- Cavazzana, A.; Röhrborn, A.; Garthus-Niegel, S.; Larsson, M.; Hummel, T.; Croy, I. Sensory-specific impairment among older people. An investigation using both sensory thresholds and subjective measures across the five senses. PLoS ONE 2018, 13, e0202969. [Google Scholar] [CrossRef] [Green Version]
- Savage, M.V.; Brengelmann, G.L. Control of skin blood flow in the neutral zone of human body temperature regulation. J. Appl. Physiol. (1985) 1996, 80, 1249–1257. [Google Scholar] [CrossRef]
- Walløe, L. Arterio-venous anastomoses in the human skin and their role in temperature control. Temperature 2016, 3, 92–103. [Google Scholar] [CrossRef] [Green Version]
- Romanovsky, A.A. The thermoregulation system and how it works. Handb. Clin. Neurol. 2018, 156, 3–43. [Google Scholar]
- Wilson, T.E.; Zhang, R.; Levine, B.D.; Crandall, C.D. Dynamic autoregulation of cutaneous circulation: Differential control in glabrous versus nonglabrous skin. Heart Circ. Physiol. 2005, 289, H385–H391. [Google Scholar] [CrossRef] [Green Version]
- Cheung, S.S. Responses of the hands and feet to cold exposure. Temperature 2005, 2, 105–120. [Google Scholar] [CrossRef]
- Harazin, B.; Harazin-Lechowska, A.; Kalamarz, J. Effect of individual finger skin temperature on vibrotactile perception threshold. Int. J. Occup. Med. Environ. Health 2013, 26, 930–939. [Google Scholar] [CrossRef] [PubMed]
- Murray, A.K.; Herrick, A.L.; King, T.A. Laser Doppler imaging: A developing technique for application in the rheumatic diseases. Rheumatology 2004, 43, 1210–1218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, J.D.; Leggett, S.A.; Marjanovic, E.J.; Moore, T.L.; Allen, J.; Anderson, M.E.; Britton, J.; Buch, M.H.; Del Galdo, F.; Denton, C.P.; et al. A Multicenter Study of the Validity and Reliability of Responses to Hand Cold Challenge as Measured by Laser Speckle Contrast Imaging and Thermography: Outcome Measures for Systemic Sclerosis-Related Raynaud’s Phenomenon. Arthritis Rheumatol. 2018, 70, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Mathiassen, O.N.; Buus, N.H.; Olsen, H.W.; Larsen, M.L.; Mulvany, M.J.; Christensen, K.L. Forearm plethysmography in the assessment of vascular tone and resistance vasculature design: New methodological insights. Acta Physiol. 2006, 188, 91–101. [Google Scholar] [CrossRef]
- Charkoudian, N. Skin blood flow in adult human thermoregulation: How it works, when it does not, and why. Mayo Clin. Proc. 2003, 78, 603–612. [Google Scholar] [CrossRef] [Green Version]
- Fanger, P.O. Assessment of man’s thermal comfort in practice. Br. J. Ind. Med. 1973, 30, 313–324. [Google Scholar] [CrossRef] [Green Version]
- Shahzad, S.; Brennan, J.; Theodossopoulos, D.; Calautit, J.K.; Hughes, B. Does a neutral thermal sensation determine thermal comfort? Build. Serv. Eng. Res. Technol. 2018, 39, 183–195. [Google Scholar] [CrossRef]
- De Dear, R. Revisiting an old hypothesis of human thermal perception: Alliesthesia. Build. Res. Inf. 2011, 39, 108–117. [Google Scholar] [CrossRef]
- Florez-Duquet, M.; McDonald, R.B. Cold-induced thermogenesis and biological aging. Physiol. Rev. 1998, 78, 339–358. [Google Scholar] [CrossRef]
- White-Chu, E.F.; Graves, W.J.; Godfrey, S.M.; Bonner, A.; Sloane, P. Beyond the medical model: The culture change revolution in long-term care. J. Am. Med Dir. Assoc. 2009, 10, 370–378. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categorical Factor | Dementia Diagnosis/AMT < 8 Group D n = (%) | AMT 8–10 Group ND n = (%) | p Value | ||
|---|---|---|---|---|---|
| Male | 10 (45.5) | 12 (54.5) | 0.43 | ||
| Female | 24 (51.5) | 23 (48.9) | |||
| Age: years | |||||
| 60–70 | 2 (33.3) | 4 (66.7) | 0.25 | ||
| 71–80 | 9 (69.2) | 4 (30.8) | |||
| 81–90 | 16 (51.6) | 15 (48.4) | |||
| Over 90 | 7 (36.8) | 12 (63.2) | |||
| Ethnicity | |||||
| White British | 33 (50) | 33 (50) | 0.22 | ||
| White European | 0 | 2 (100) | |||
| White | 1 (100) | 0 | |||
| Frailty Score | |||||
| Well | 0 | 1(100) | 0.028 | ||
| Managing Well | 6 (75) | 2 (25) | |||
| Vulnerable | 1 (10) | 9 (90) | |||
| Mildly Frail | 1 (50) | 1 (50) | |||
| Moderately Frail | 9 (40.9) | 13 (59.1) | |||
| Severely Frail | 17 (65.4) | 9 (34.6) | |||
| Dominant Hand | |||||
| Right | 31 (49.2) | 32 (50.8) | 0.4 | ||
| Left | 3 (60) | 2 (40) | |||
| Ambidextrous | 0 | 1 (100) | |||
| Finger with greatest SD | |||||
| Left ring | 11 (68.8) | 5 (31.2) | 0.34 | ||
| Left middle | 5 (38.5) | 8 (61.5) | |||
| Left index | 14 (43.8) | 18 (56.2) | |||
| Right ring | 1 (100 | 0 | |||
| Right middle | 0 | 1 (100) | |||
| Right index | 2 (40) | 3 (60) | |||
| Clothing ensemble (Clo unit) | |||||
| Light | 6 (30) | 14 (70) | |||
| Medium | 26 (55.3) | 21 (44.7) | 0.05 | ||
| Heavy | 2 (100) | 0 | |||
| Thermal sensation rating | |||||
| −2 | 1 (100) | 0 | 0.02 | ||
| −1 | 10 (76.9) | 3 (23.1) | |||
| 0 | 21 (48.8) | 22 (51.2) | |||
| 1 | 0 | 7 (100) | |||
| 1.5 | 1 (100) | 0 | |||
| 2 | 1 (33.3) | 2 (66.7) | |||
| Thermal Vote | |||||
| Cooler | 1 (16) | 5 (84) | 0.09 | ||
| No change | 27 (49.1) | 28 (50.9) | |||
| Warmer | 6 (75) | 2 (25) | |||
| Temperature | n = (%) | Mean (SD) | n = (%) | Mean (SD) | |
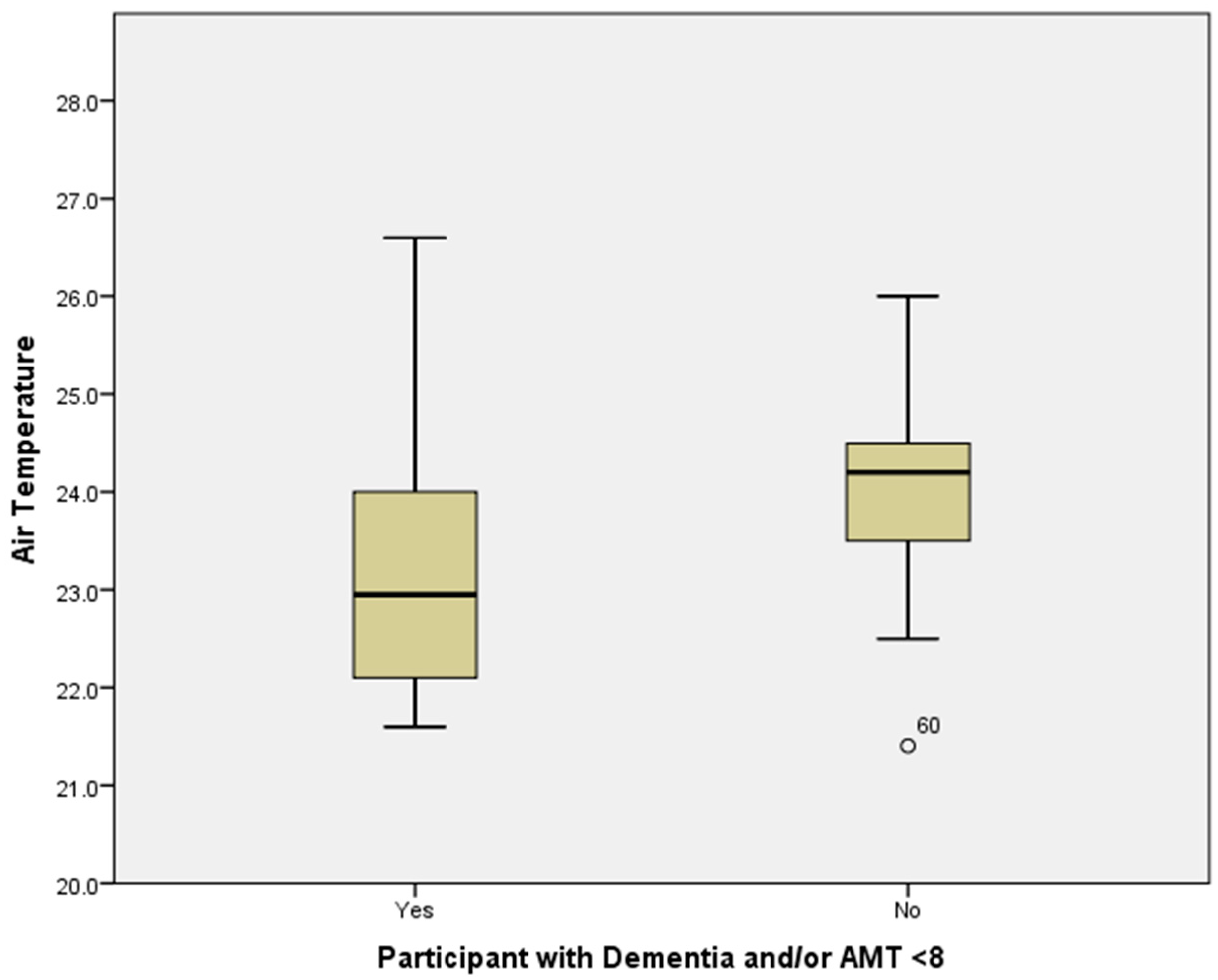
| Air temperature (°C) | 34 (49.3) | 23.1 (0.2) | 35 (50.7) | 24.1 (0.17) | 0.001 |
| Relative Humidity (%RH) | 34 (49.3) | 49 (1.1) | 35 (50.7) | 52.1 (1.6) | 0.2 |
| ROI: mean DP (°C) | 33 (48.5) | 30.0 (0.46) | 35 (51.5) | 31.6 (0.4) | 0.01 |
| ROI: mean Cap (°C) | 33 (48.5) | 31.7 (0.25) | 35 (51.5) | 32.0 (0.25) | 0.4 |
| ROI: mean DH (°C) | 33 (48.5) | 31.9 (0.19) | 35 (51.5) | 32.0 (0.24) | 0.1 |
| ΔT1 (mean DP- mean CAP) °C | 33 (48.5) | −1.7 (0.29) | 35 (51.5) | −0.43 (0.24) | 0.001 |
| ΔT2 (mean DP-mean DH) °C | 33 (48.5) | −1.8 (0.34) | 35 (51.5) | −0.39 (0.26) | 0.001 |
| Tympanic temperature (°C) | 34 (50) | 36.6 (0.07) | 34 (50) | 36.8 (0.6) | 0.01 |
| Site ID | Month/Day of Study | Mean Ta (°C) | Mean RH % | Thermal Sensation Rating | ||||
|---|---|---|---|---|---|---|---|---|
| Resident 1 | Resident 2 | Resident 3 | Resident 4 | Resident 5 | ||||
| 1 | 7 June | 24.3 | 60 | 0 | missing | 0 | ||
| 2 | 13 July | 24.0 | 47 | 0 | 0 | 0 | −1 | |
| 3 | 12 July | 24.3 | 56 | 0 | 1 | 1 | 1 | |
| 4 | 28 July | 22.5 | 54 | 0 | 0 | |||
| 5 | 6 September | 24.6 | 60 | 0 | 0 | 0 | ||
| 6 | 28 September | 25.8 | 52 | 0 | 1 | 1 | 0 | |
| 6 | 6 October | 23.6 | 38 | 0 | −1 | 0 | 0 | |
| 7 | 12 October | 23.1 | 57 | 2 | 0 | |||
| 8 | 20 October | 24.2 | 60 | 0 | 1 | 0 | 0 | |
| 9 | 7 November | 22.0 | 53 | −1 | −1 | |||
| 9 | 8 December | 24.0 | 32 | 1 | 0 | |||
| 10 | 11 April | 22.0 | 55 | 0 | 1.5 | |||
| 11 | 17 April | 24.5 | 48 | −1 | 0 | 0 | ||
| 11 | 24 April | 21.8 | 44 | 0 | 0 | −1 | ||
| 12 | 11 May | 25.3 | 37 | −1 | 0 | |||
| 13 | 16 May | 22.6 | 45 | 0 | 0 | 0 | 0 | |
| 14 | 18 May | 24.2 | 46 | 0 | 0 | 0 | ||
| 12 | 21 May | 22.7 | 50 | −1 | 0 | 0 | −1 | −1 |
| 11 | 12 June | 22.0 | 53 | −1 | 0 | 0 | ||
| 15 | 14 June | 23.6 | 54 | 0 | −2 | −1 | 0 | 2 |
| 11 | 19 June | 22.1 | 54 | 0 | −1 | 0 | ||
| 6 | 19 June | 24.0 | 58 | 0 | 2 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Childs, C.; Elliott, J.; Khatab, K.; Hampshaw, S.; Fowler-Davis, S.; Willmott, J.R.; Ali, A. Thermal Sensation in Older People with and without Dementia Living in Residential Care: New Assessment Approaches to Thermal Comfort Using Infrared Thermography. Int. J. Environ. Res. Public Health 2020, 17, 6932. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186932
Childs C, Elliott J, Khatab K, Hampshaw S, Fowler-Davis S, Willmott JR, Ali A. Thermal Sensation in Older People with and without Dementia Living in Residential Care: New Assessment Approaches to Thermal Comfort Using Infrared Thermography. International Journal of Environmental Research and Public Health. 2020; 17(18):6932. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186932
Chicago/Turabian StyleChilds, Charmaine, Jennifer Elliott, Khaled Khatab, Susan Hampshaw, Sally Fowler-Davis, Jon R. Willmott, and Ali Ali. 2020. "Thermal Sensation in Older People with and without Dementia Living in Residential Care: New Assessment Approaches to Thermal Comfort Using Infrared Thermography" International Journal of Environmental Research and Public Health 17, no. 18: 6932. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186932