Effectiveness of SaBang-DolGi Walking Exercise Program on Physical and Mental Health of Menopausal Women



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
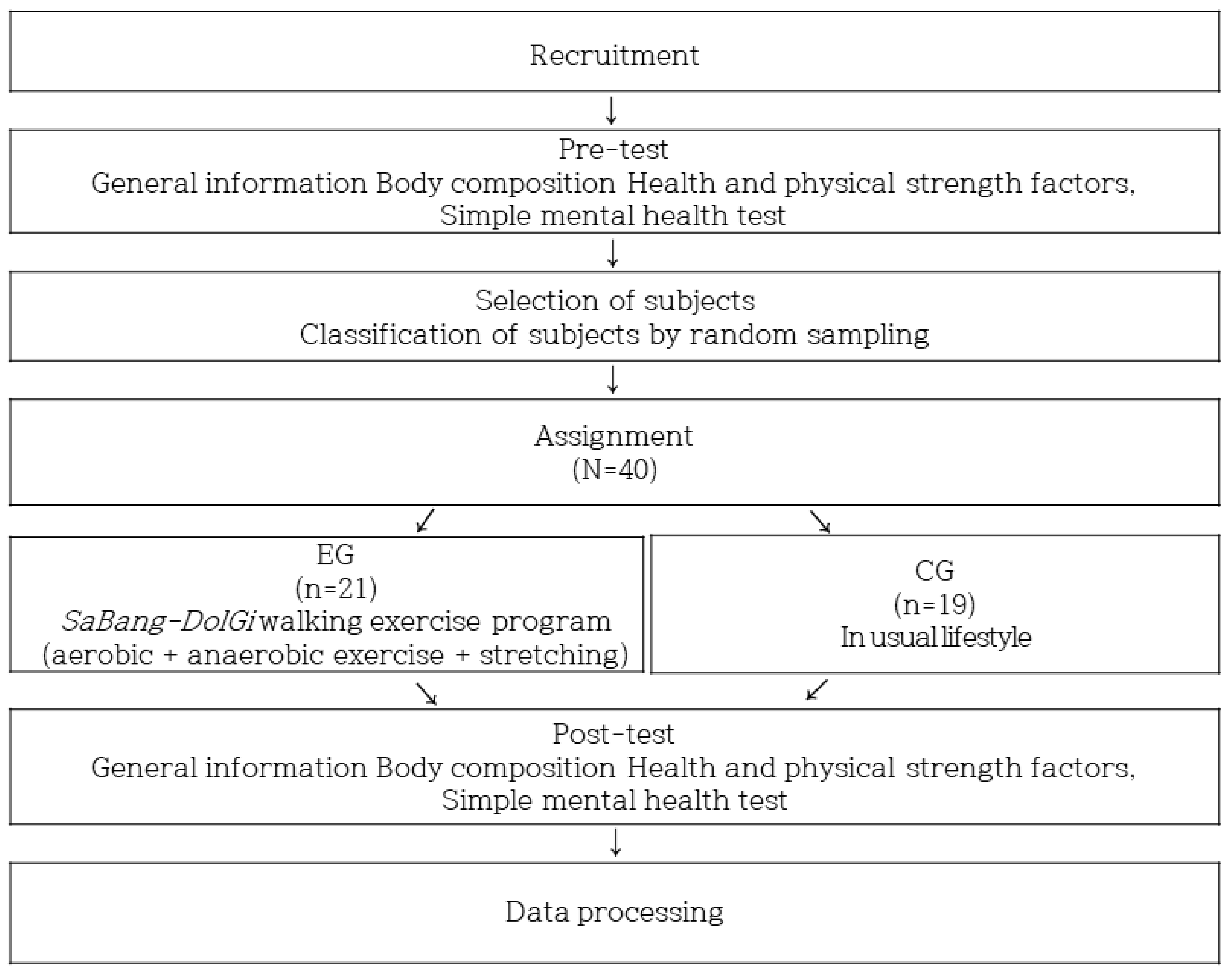
2.2. Study Design
2.3. Measurement
2.3.1. Body Composition
2.3.2. Physical Health Test
2.3.3. Mental Health Test
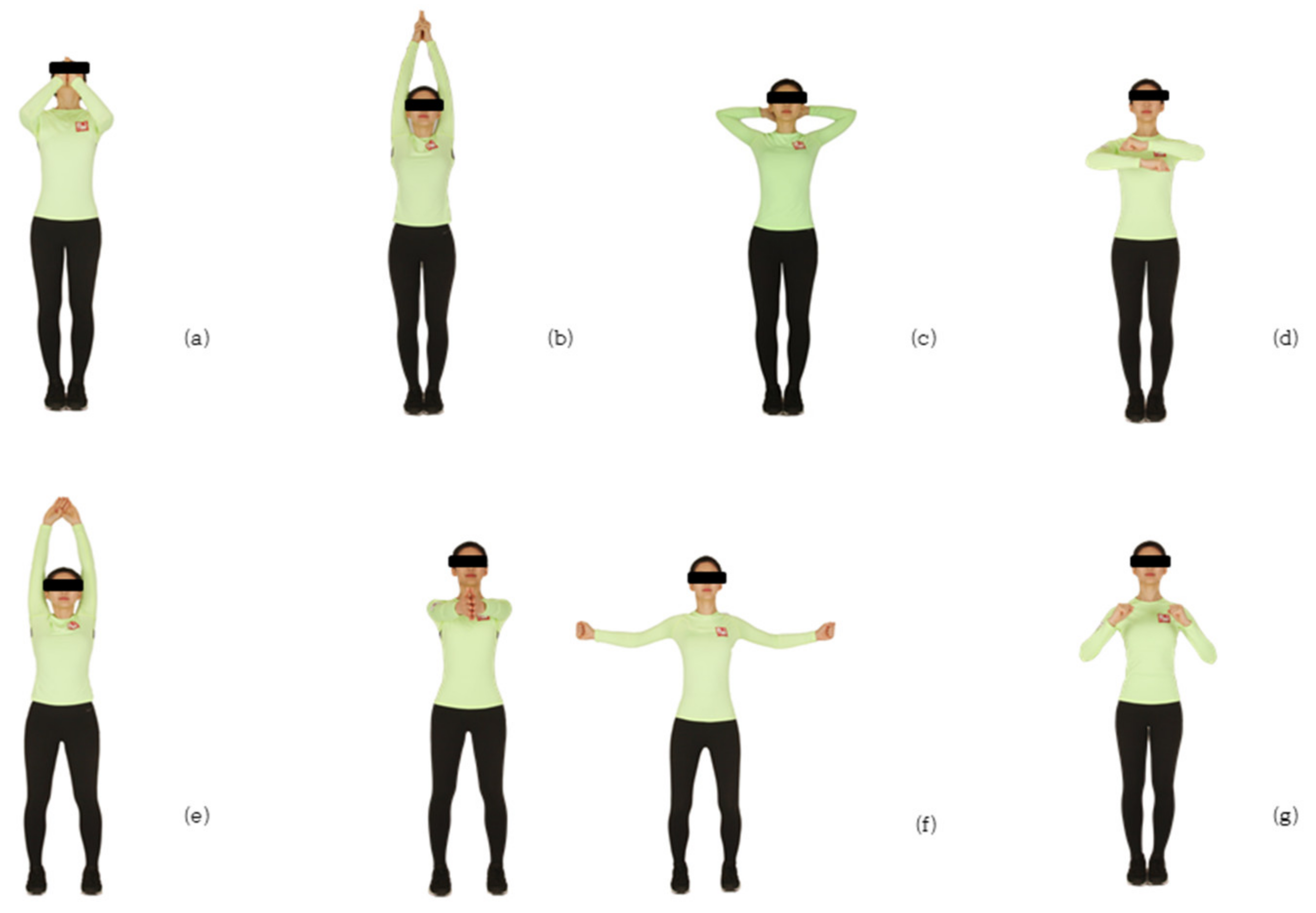
2.3.4. SaBang-DolGi Walking Exercise Program
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Nelson, D.B.; Samuel, M.D.; Freeman, H.W.; Lin, H.; Gracia, C.R.; Schmitz, K.H. Effect of physical activity on menopausal symptoms among urban women. Med. Sci. Sports Exerc. 2008, 40, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Yim, G.; Ahn, Y.; Chang, Y.; Ryu, S.; Lim, J.Y.; Kang, D.; Choi, E.K.; Ahn, J.; Cho, J.H.; Park, H.Y. Prevalence and severity of menopause symptoms and associated factors across menopause status in Korean women. Menopause 2015, 22, 1108–1116. [Google Scholar] [CrossRef]
- Berecki-Gisolf, J.; Begum, N.; Dobson, A.J. Symptoms reported by women in midlife: Menopausal transition or aging? Menopause 2009, 16, 1021–1029. [Google Scholar] [CrossRef]
- Jenabi, E.; Shobeiri, F.; Hazavehei, S.M.; Roshanaei, G. Assessment of questionnaire measuring quality of life in menopausal women: A systematic review. Oman Med. J 2015, 30, 151–156. [Google Scholar] [CrossRef]
- Cha, S.H. The Prevention and Treatment of Gynecological Diseases for Women; Garim Publishing House: Seoul, Korea, 2003; ISBN 8978951341. [Google Scholar]
- De Franciscis, P.; Colacurci, N.; Riemma, G.; Conte, A.; Pittana, E.; Guida, M.; Schiattarella, A. A nutraceutical approach to menopausal complaints. Medicina 2019, 55, 544. [Google Scholar] [CrossRef] [Green Version]
- De Franciscis, P.; Conte, A.; Schiattarella, A.; Riemma, G.; Cobellia, L.; Colacirci, N. Non-hormonal treatments for menopausal symptoms and sleep disturbances: A comparison between purified pollen extracts and soy isoflavones. Curr. Pharm. Des 2020, 20. [Google Scholar] [CrossRef] [PubMed]
- Stojanovska, L.; Apostolopoulos, V.; Polman, R.; Borkoles, E. To exercise, or, not to exercise, during menopause and beyond. Maturitas 2014, 77, 318–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalziel, K.; Segal, L.; Elley, C.R. Costutility analysis of physical activity counseling in general practice. Aust. N. Z. J. Public Health 2006, 30, 57–63. [Google Scholar] [CrossRef]
- Daley, A.; MacArthur, C.; McManus, R.; Stokes-Lampard, H.; Wilson, S.; Roalfe, A.; Mutrie, N. Factors associated with the use of complementary medicine and non-pharmacological interventions in symptomatic menopausal women. Climacteric 2006, 9, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Nelson, H.D.; Humphrey, L.L.; Nygren, P.; Teutsch, S.M.; Allan, J.D. Postmenopausal hormone replacement therapy: Scientific review. JAMA 2002, 288, 872–881. [Google Scholar] [CrossRef]
- Gabriel, K.K.P.; Morrow, J.R., Jr.; Woolsey, A.L. Framework for physical activity as a complex and multidimensional behavior. J. Phys. Act. Health 2012, 9, S11–S18. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.A.; Hsu, W.H.; Kuo, L.T.; Lin, Z.R.; Shen, W.J.; Hsu, R.W. The effects of high impact exercise intervention on bone mineral density, physical fitness, and quality of life in postmenopausal women with osteopenia: A retrospective cohort study. Medicine 2019, 98, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Courneya, K.S.; McNeil, J.; O’Reilly, R.; Morielli, A.R.; Friedenreich, C.M. Dose-Response effects of aerobic exerciseon quality of life in postmenopausal women: Results from the Breast cancer and Exercise Trialin Albert (BETA). Ann. Behav. Med. Jun 2017, 51, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Maki, P.M.; Kornstein, S.G.; Joffe, H.; Bromberger, J.T.; Freeman, E.W.; Athappilly, G.; Bobo, W.V.; Rubin, L.H.; Koleva, H.K.; Cohen, L.S.; et al. Guidelines for the evaluation and treatment of perimenopausal depression: Summary and recommendations. J. Women’s Health 2019, 28, 117–134. [Google Scholar] [CrossRef] [Green Version]
- Wegner, M.; Helmich, I.; Machado, S.; Nardi, A.E.; Arias-Carrion, O.; Budde, H. Effects of exercise on anxiety and depression disorders: Review of meta-analyses and neurobiological mechanisms. CNS Neurol. Disord. Drug Targets 2014, 13, 1002–1014. [Google Scholar] [CrossRef] [Green Version]
- Hunter, M. The South-East England longitudinal study of the climacteric and postmenopause. Maturities 1992, 14, 117–126. [Google Scholar] [CrossRef]
- Garn, A.C.; Morin, A.; Martin, C.S.; McCaughtry, N. A Reciprocal Effects Model of Children’s Body Fat Self-Concept: Relations with Physical Self-Concept and Physical Activity. J. Sport Exerc. Psychol 2016, 38, 255–267. [Google Scholar] [CrossRef]
- Dishman, R.K.; Gettman, L.R. Psychological influence on exercise adherence. J. Sport Exerc. Psychol 1980, 2, 295–310. [Google Scholar]
- Mishra, N.; Mishra, V.N.; Devanshi. Exercise beyond menopause: Do sand Don’ts. J. Midlife Health 2011, 2, 51–56. [Google Scholar]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A. The physical activity guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- Kemmler, W.; Kohl, M.; Von Stengel, S. Long-term effects of exercise in postmenopausal women: 16-year result s of the Erlangen Fitness and Osteoporosis Prevention Stud (EFOPS). Menopause 2017, 24, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Ebrahim, S.; Rowland, L. Towards a new strategy for health promotion for older women: Determinants of physical activity. Psychol. Health Med 1996, 1, 29–40. [Google Scholar] [CrossRef]
- Heesch, K.C.; Brown, D.R.; Blanton, C.J. Perceived barriers to exercise and stage of exercise adoption in older women of different racial/ethnic groups. Women Health 2000, 30, 61–76. [Google Scholar] [CrossRef] [PubMed]
- Scharff, D.P.; Homan, S.; Kreuter, M.; Brennan, L. Factors associated with physical activity in women across the life span: Implications for program development. Women Health 2008, 29, 115–134. [Google Scholar] [CrossRef]
- Moschny, A.; Platen, P.; Klaassen-Mielke, R.; Trampisch, U.; Hinrichs, T. Barriers to physical activity in older adults in Germany: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act 2011, 8, 121. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.B. A study on the aesthetic structure of korean dance-focusing on the structure of mechanistic thinking. Ph.D. Thesis, Graduate School of Sungkyunkwan University, Seoul, Korea, 2007. [Google Scholar]
- Cho, k.S.; Choi, H.K.; Nam, H.K. The effects of line dance program on muscle strength, balance, flexibility, pain, and mood state in post-menopausal women. J. Muscle Joint Health 2012, 19, 263–271. [Google Scholar] [CrossRef]
- Benvenuti, F.; Stanhope, S.J.; Thomas, S.L.; Panzer, V.P.; Hallett, M. Flexibility of anticipatory postural adjustments revealed by self-paced and reaction-time arm movements. Brain Res. 1997, 761, 59–70. [Google Scholar] [CrossRef]
- Lee, W.Y.; Kwon, S.S. Effects of a music therapy program on depression, balance, flexibility in the elderly. J. Korean Community Nurs. 2003, 14, 16–23. [Google Scholar]
- Shephard, R.; Montelpare, W. Geriatric Benefits of exercise as an adult. J. Gerontol. 1988, 43, 86–90. [Google Scholar] [CrossRef]
- Heber, L. Dance movement: A therapeutic program for psychiatric clients. Perspect. Psychiatr. Care 1993, 29, 22–29. [Google Scholar] [CrossRef]
- Forbes, E.J. Exercise: Wellness maintenance for the elderly client. Holist. Nurs. Pract. 1992, 6, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Kligman, E.W.; Pepsin, E. Prescribing physical activity for older patients. Geriatrics 1992, 47, 33–47. [Google Scholar] [PubMed]
- Hesse, S.; Bertett, C.; Jahnke, M.; Schaffrin, A.; Malezic, M.; Mauritz, K. Treadmill training with partial body weight support compared with physiotherapy in nonambulatory hemiparetic patients. Stroke 1995, 26, 976–981. [Google Scholar] [CrossRef] [PubMed]
- Swain, R.A.; Harris, A.B.; Wiener, E.C.; Dutka, M.V.; Morris, H.D.; Theien, B.E. Prolonged exercise induces angiogenesis and increases cerebral blood volume in primary motor cortex of the rat. Neuroscience 2003, 117, 1037–1046. [Google Scholar] [CrossRef]
- Stanley, J.C.; Kirt, I.E.; Paige, E.S.; Jenny, S.K.; Ruchika, P.; Edward, M.; Steriani, E.; David, X.M.; Liand, H.; Arthur, F.K. Aerobic exercise training increases brain volume in aging humans. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1166–1170. [Google Scholar]
- Kim, T.M.; Kim, J.H. Effects of 12-week balance walking PT on physical fitness, cardiovascular risk factors and quality of life in postmenopausal women. J. Korean Assoc. Phys. Educ. Sport Girls Women 2019, 6, 185–202. [Google Scholar] [CrossRef]
- Kim, D.S.; Kim, T.M.; Chung, N.J. The effects of static posture, gait variables, and balance ability before and after balance walking PT. Korea J. Sport 2020, 18, 635–646. [Google Scholar] [CrossRef]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef] [Green Version]
- Derogatis, L.R. SCL-90-R, Administration, Scoring, and Procedures Manual for the R(evised) Version; The Johns Hopkins University School of Medicine: Baltimore, MD, USA, 1977. [Google Scholar]
- Kim, T.M. BalanceWalking PT that Brings Happiness; Samcontents: Seoul, Korea, 2018; pp. 43–46. ISBN 9791189667009. [Google Scholar]
- Glaister, B.C.; Bernatz, G.C.; Klute, G.K.; Orendurff, M.S. Video task analysis of turning during activities of daily living. Gait Posture 2007, 25, 289–294. [Google Scholar] [CrossRef]
- Courtine, G.; Schieppati, M. Human walking along a curved path. I. Body trajectory, segment orientation and the effect of vision. Eur. J. Neurosci. 2003, 18, 177–190. [Google Scholar] [CrossRef]
- Poehlman, E.T.; Toth, M.J.; Gardner, A.W. Changes in energy balance and body composition at menopause: A controlled longitudinal study. Ann. Intern. Med. 1995, 123, 673–675. [Google Scholar] [CrossRef] [PubMed]
- Shapses, S.A.; Riedt, C.S. Bone, body weight, and weight reduction: What are the concerns? J. Nutr. 2006, 136, 1453–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.S.; Yang, S.W. Effects of Low-intensity combined exercise on body composition, bloodlipids, glucose, and leptin in post-menopausal obese middle-aged women. J. Sport Leis. Stud. 2009, 38, 951–960. [Google Scholar]
- Manson, J.E.; Hu, F.B.; Rich-Edwards, J.W.; Colditz, G.A.; Stampfer, M.J.; Willet, W.C.; Speizer, F.E.; Hennekens, C.H. A prospective study of walking as compared with vigorous exercise in the prevention of coronary heart disease in women. N. Engl. J. Med. 1999, 341, 650–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, J.S.; Stanforth, P.R.; Rankinen, S.T.; Rao, D.C.; Skinner, J.S.; Nouchard, C.; Wilmore, J.H. The effect of exercise training on abdominal visceral fat, body composition, and indicators of the metabolic syndrome in postmenopausal women with and without estrogen replacement therapy. Metabolism 2004, 53, 1192–1196. [Google Scholar] [CrossRef]
- Son, H.J.; So, W.Y.; Park, H.M.; Lee, S.M.; Baek, H.J.; Sung, D.J. Effect of public health center exercise program on physical fitness factors, body weight, body mass index and blood pressure in elderly women. J. Korea Public Health Nurs. 2011, 25, 17–27. [Google Scholar]
- Gary, R.H.; John, P.M.; Marcas, M.B. Effects of resistance training on older adults. Sports Med. 2004, 34, 329–348. [Google Scholar]
- Hagey, A.R.; Warren, M.P. Role of exercise and nutrition in menopause. Clin. Obstet. Gynecol. 2008, 51, 627–641. [Google Scholar] [CrossRef]
- Van Kan, G.A. Epidemiology and consequences of sarcopenia. J. Nutr. Health Aging 2009, 13, 708–712. [Google Scholar] [CrossRef]
- Dalleck, L.C.; Tischendorf, J.S. Guidelines for exercise testing and prescription. Am. Coll. Sports Med. 2012. [Google Scholar] [CrossRef]
- Lauretani, F.; Russo, C.R.; Bandinelli, S.; Bartali, B.; Cavazzini, C.; DiIorio, A.; Corsi, A.M.; Rantanen, T.; Guralnik, J.M.; Ferrucci, L. Age-associated changes in skeletal muscles and their effect on mobility: An operational diagnosis of sarcopenia. J. Appl. Physiol. 2003, 95, 1851–1860. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Hand-grip dynamometry predicts future outcomes in aging adults. J. Geriatr. Phys. Ther. 2008, 31, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Sayer, A.A.; Kirkwood, T.B. Grip strength and mortality: A biomarker of ageing? Lancet 2015, 386, 226–227. [Google Scholar] [CrossRef]
- Wolfe, R.R. The underappreciated role of muscle in health and disease. Am. J. Clin. Nutr. 2006, 84, 475–482. [Google Scholar] [CrossRef]
- Oksuzyan, A.; Maier, H.; Mcgue, M.; Vaupel, J.W.; Christensen, K. Sex differences in the level and rate of change of physical function and grip strength in the Danish 1905-cohort study. J. Aging Health 2010, 22, 589–610. [Google Scholar] [CrossRef] [Green Version]
- Stessman, J.; Rottenberg, Y.; Fischer, M.; Hammerman-Rozenberg, A.; Jacobs, J.M. Hand grip Strength in old and very old adults: Mood, cognition, function, and mortality. J. Am. Geriatr. Soc. 2017, 65, 526–532. [Google Scholar] [CrossRef]
- Li, F.; Harmer, P.; Fisher, K.J.; McAuley, E.; Chaumeton, N.; Eckstrom, E.; Wilson, N.L. Tai Chi and fall reductions in older adults: A randomized controlled trial. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 187–194. [Google Scholar] [CrossRef] [Green Version]
- Mazzeo, R.S.; Cavanagh, P.; Evans, W.J.; Maughan, R.J.; Montain, S.J.; Stachenfeld, N.S. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 1998, 30, 992–1008. [Google Scholar]
- Chandler, J.M.; Hadley, E.C. Exercise to improve physiologic and functional performance in old age. Clin. Geriatr. Med. 1996, 12, 761–784. [Google Scholar] [CrossRef]
- Schreiber, D.R.; Dautovich, N.D. Depressive symptoms and weight in midlife women: The role of stress eating and menopause status. Menopause 2017, 24, 1190–1199. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Khanzada, F.J.; Soomro, N.; Khan, S.Z. Association of physical exercise on anxiety and depression amongst adults. J. Coll. Phys. Surg. Pak. 2015, 25, 546–548. [Google Scholar]
- Apostolopoulos, V.; Borkoles, E.; Polman, R.; Stojanovska, L. Physical and immunological aspects of exercise in chronic diseases. Immunotherapy 2014, 6, 1145–1157. [Google Scholar] [CrossRef] [PubMed]
- Paffenbarger, R.S.; Hyde, R.T.; Wing, A.L.; Lee, I.M.; Jung, D.L.; Kampert, J.B. The association of changes in physical-activity level and other lifestyle characteristics with mortality among men. N. Engl. J. Med. 1993, 328, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Cho, J.; Ahn, Y.; Yim, G.; Park, H.Y. Association between physical activity and menopausal symptoms in perimenopausal women. BMC Womens Health 2014, 14, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAndrew, L.M.; Napolitano, M.A.; Albrecht, A.; Farrell, N.C.; Marcus, B.H.; Whiteley, J.A. When, why and for whom there is a relationship between physical activity and menopause symptoms. Maturitas 2009, 64, 119–125. [Google Scholar] [CrossRef]
- Slaven, L.; Lee, C. Mood and symptom reporting among middle-aged women: The relationship between menopausal status, hormone replacement therapy, and exercise participation. Health Psychol. 1997, 16, 203–208. [Google Scholar] [CrossRef]
- Ströhle, A. Physical activity, exercise, depression and anxiety disorders. J. Neural Transm. 2009, 116, 777–784. [Google Scholar] [CrossRef]
- NICE. Depression: The Treatment and Management of Depression in Adults (NICE Clinical Guideline 90); National Collaborating Centre Mental Health: London, UK, 2009. [Google Scholar]
- Van Milligen, B.A.; Lamers, F.; Hoop, G.T.; Smit, J.H.; H Penninx, B.W.J. Objective physical functioning in patients with depressive and /or anxiety disorders. J. Affect. Disord. 2011, 131, 193–199. [Google Scholar] [CrossRef]
- Suija, K.; Timonen, M.; Suviola, M.; Jokelainen, J.; Järvelin, M.R.; Tammelin, T. The association between physical fitness and depressive symptoms among young adults: Results of the Northern Finland 1966 birth cohort study. BMC Public Health. 2013, 13, 535. [Google Scholar] [CrossRef] [Green Version]
- Fukumori, N.; Yamamoto, Y.; Takegami, M.; Yamazaki, S.; Onishi, Y.; Sekiguchi, M.; Otani, K.; Konno, S.I.; Kikuchi, S.I.; Fukuhara, S.I. Association between hand-grip strength and depressive symptoms: Locomotive Syndrome and Health Outcomes in Aizu Cohort Study (LOHAS). Age Ageing 2015, 44, 592–598. [Google Scholar] [CrossRef] [Green Version]
- Gale, C.; Sayer, A. Factors associated with symptoms of anxiety and depression in five cohorts of community-based older people: The HALCyon (Healthy Ageing across the Life Course) Programme. Psychol. Med. 2011, 41, 2057–2073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDowell, C.P.; Gordon, B.R.; Herring, M.P. Sex-related differences in the association between grip strength and depression: Results from the Irish Longitudinal Study on Ageing. Exp. Gerontol. 2018, 104, 147–152. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Age (years) | Height (cm) | Body Weight (kg) | BMI (kg/m2) | Fat (%) | Waist Circumference (cm) |
|---|---|---|---|---|---|---|
| EG (N = 21) | 59.38 | 157.94 | 58.27 | 23.31 | 18.94 | 80.27 |
| ±3.76 | ±5.47 | ±7.37 | ±2.79 | ±5.27 | ±7.08 | |
| CG (N = 19) | 58.21 | 156.27 | 61.58 | 25.17 | 22.07 | 84.35 |
| ±3.99 | ±4.97 | ±10.58 | ±3.77 | ±6.17 | ±7.79 |
| Domain | Characteristic | 1 | 2 | 3 | Communalities | Cronbach’s α |
|---|---|---|---|---|---|---|
| Emotion | Social Desirability | 0.898 | −0.209 | 0.079 | 0.687 | 0.894 |
| Inconsistency | 0.870 | 0.334 | 0.258 | 0.771 | ||
| Depression | 0.857 | 0.342 | 0.249 | 0.752 | ||
| Anxiety | 0.819 | 0.493 | 0.072 | 0.764 | ||
| Phobic Anxiety | 0.796 | 0.433 | 0.201 | 0.646 | ||
| Panic Attack | 0.783 | 0.119 | 0.126 | 0.630 | ||
| Agoraphobia | 0.771 | −0.012 | 0.525 | 0.674 | ||
| Obsessive-Compulsive | 0.758 | −0.035 | −0.003 | 0.655 | ||
| Obsession | 0.739 | 0.393 | 0.272 | 0.599 | ||
| Obsessive-Compulsive Personality Trait | 0.683 | 0.106 | 0.024 | 0.791 | ||
| Posttraumatic Stress Disorder | 0.672 | 0.336 | 0.445 | 0.803 | ||
| Aggression | 0.650 | 0.116 | 0.118 | 0.699 | ||
| Somatization | 0.642 | 0.457 | 0.374 | 0.642 | ||
| Others | Suicide | 0.605 | 0.710 | 0.122 | 0.753 | 0.863 |
| Addiction | 0.363 | 0.648 | 0.077 | 0.638 | ||
| Sleep Problem | 0.214 | 0.634 | 0.018 | 0.601 | ||
| Stress Vulnerability | 0.268 | −0.070 | 0.702 | 0.670 | ||
| Interpersonal Sensitivity | 0.181 | 0.209 | 0.692 | 0.656 | ||
| Self-Regulation Problem | 0.037 | 0.223 | 0.607 | 0.619 | ||
| Adaptation to reality | Manic episode | 0.105 | 0.729 | 0.322 | 0.646 | 0.697 |
| Paranoia | 0.419 | 0.718 | 0.162 | 0.718 | ||
| Schizophrenia | 0.555 | 0.714 | 0.147 | 0.840 | ||
| Characteristic value | 10.299 | 1.796 | 1.560 | |||
| Explanation variance | 46.813 | 8.165 | 7.089 | |||
| Cumulative variance | 46.813 | 54.978 | 62.067 | |||
| KMO = 0.719 Bartlett’ Test of Sphericity = 1110.059 (df = 231, sig. = 0.000) | ||||||
| Item | Description | Intensity | Remark | Frequency |
|---|---|---|---|---|
| Warn-up exercise (Aerobics) 10 min | *1W, **3W 1. Walking while turning the wrist. 2. Tapping the head, tapping the chest, clapping. | RPE 6–8 | SaBang-DolGi (one or two turns) Healthy kinship Maintaining relationships | 3 sessions/week |
| Muscle strengthening 10 min | Stretching the chest, erector spinal muscle, stretching over the shoulders. Cross PT up, cross PT down, down walking. 10 new programs for each session. | HR max 40–60% RPE 9–11 (Weeks 1–6) | SaBang-DolGi (One or two turns) | |
| HR max 60–80% RPE 12–16 (Weeks 7–12) | ||||
| Complex exercise 25 min | ***1B1W 1. Stretching the chest, walking with the chin. 2. Turning shoulders, tapping the abdomen. ****1B2W 1. Erector spinal muscle, praying, stretching shoulders. 2. Stretching the chest, jjamjjam walking_right, left. 3. Stretching over shoulders, walking while turning the wrist_ in or outward. | HR max 40–60% RPE 9–11 (Weeks 1–6) | Muscle strengthening motion + walking motion + stretching SaBang-DolGi (one or two turns) | |
| HR max 60–80% RPE 12–16 (Weeks 7–12) | ||||
| Warm-down exercise 15 min | **3W 1. Jjamjjam, shaking the wrist, clapping. 2. Clapping and walking in the place. 3. Walking while tapping the shoulder of a person in front (Train walking). **3W and chanting balance slogans. | RPE 7-9 | SaBang-DolGi (one or two turns) Pursuing fun Chanting balance slogans. “Let’s live healthily! Let’s live happily! Let’s live with gratitude!” |
| Domain | Characteristic | Period | Exp. (N = 21) | Con. (N = 19) | ANOVA (p) | ||
|---|---|---|---|---|---|---|---|
| M ± SD | M ± SD | G | T | G × T | |||
| Physical health | Skeletal muscle mass | Pre | 21.13 ± 2.17 | 21.41 ± 3.82 | 0.971 | 0.588 | 0.001 *** |
| Post | 21.47 ± 2.26 | 21.13 ± 2.90 | |||||
| BMI | Pre | 23.31 ± 2.79 | 25.18 ± 3.77 | 0.035 * | 0.689 | 0.001 *** | |
| Post | 22.90 ± 2.64 | 25.55 ± 3.82 | |||||
| Body fat percentage | Pre | 32.09 ± 5.62 | 35.39 ± 4.33 | 0.020 * | 0.124 | 0.001 *** | |
| Post | 31.35 ± 5.75 | 35.84 ± 4.24 | |||||
| Waist circumference | Pre | 80.27 ± 7.08 | 84.35 ± 7.79 | 0.020 * | 0.957 | 0.001 *** | |
| Post | 78.63 ± 7.01 | 86.03 ± 8.24 | |||||
| Hip circumference | Pre | 95.05 ± 5.17 | 98.69 ± 7.42 | 0.109 | 0.010 ** | 0.047 * | |
| Post | 95.81 ± 5.44 | 98.79 ± 7.43 | |||||
| Grip strength | Pre | 21.69 ± 3.02 | 20.83 ± 5.72 | 0.107 | 0.404 | 0.001 *** | |
| Post | 23.35 ± 3.27 | 19.60 ± 5.53 | |||||
| Abdominal muscle strength | Pre | 14.62 ± 2.82 | 14.26 ± 2.42 | 0.001 *** | 0.001 *** | 0.001 *** | |
| Post | 21.19 ± 2.60 | 14.26 ± 2.21 | |||||
| Flexibility | Pre | 14.09 ± 8.10 | 12.18 ± 7.53 | 0.043 * | 0.001 *** | 0.001 *** | |
| Post | 18.79 ± 7.59 | 10.30 ± 8.48 | |||||
| Domain | Characteristic | Period | Exp. (N = 21) | Con. (N = 19) | ANOVA (p) | ||
|---|---|---|---|---|---|---|---|
| M ± SD | M ± SD | G | T | G × T | |||
| Emotion | Social Desirability | Pre | 54.00 ± 12.67 | 53.42 ± 6.40 | 0.570 | 0.872 | 0.160 |
| Post | 51.90 ± 13.62 | 56.05 ± 9.84 | |||||
| Inconsistency | Pre | 50.05 ± 10.66 | 50.89 ± 13.51 | 0.971 | 0.461 | 0.776 | |
| Post | 48.86 ± 9.55 | 48.21 ± 14.08 | |||||
| Depression | Pre | 48.38 ± 7.03 | 46.89 ± 8.56 | 0.963 | 0.001 *** | 0.013 * | |
| Post | 43.57 ± 7.02 | 45.84 ± 8.94 | |||||
| Anxiety | Pre | 51.71 ± 8.32 | 48.84 ± 10.48 | 0.650 | 0.037 * | 0.086 | |
| Post | 48.10 ± 6.56 | 48.47 ± 10.68 | |||||
| Phobic Anxiety | Pre | 49.19 ± 6.18 | 48.05 ± 8.65 | 0.798 | 0.072 | 0.016 * | |
| Post | 46.10 ± 4.66 | 48.53 ± 12.03 | |||||
| Panic Attack | Pre | 51.43 ± 9.07 | 47.53 ± 6.23 | 0.328 | 0.038 * | 0.090 | |
| Post | 46.90 ± 5.07 | 47.05 ± 7.03 | |||||
| Agoraphobia | Pre | 47.38 ± 5.76 | 49.00 ± 12.91 | 0.368 | 0.856 | 0.044 * | |
| Post | 46.00 ± 5.19 | 50.16 ± 14.32 | |||||
| Obsessive-Compulsive | Pre | 49.76 ± 9.47 | 49.74 ± 11.52 | 0.708 | 0.094 | 0.352 | |
| Post | 46.52 ± 5.46 | 48.79 ± 13.01 | |||||
| Obsession | Pre | 52.00 ± 10.12 | 46.63 ± 10.91 | 0.315 | 0.323 | 0.081 | |
| Post | 48.29 ± 8.18 | 47.68 ± 11.37 | |||||
| Obsessive-Compulsive Personality Trait | Pre | 46.90 ± 9.64 | 53.47 ± 14.60 | 0.109 | 0.119 | 0.515 | |
| Post | 45.52 ± 5.62 | 50.16 ± 15.17 | |||||
| Posttraumatic Stress Disorder | Pre | 49.05 ± 10.97 | 49.37 ± 14.24 | 0.863 | 0.126 | 0.888 | |
| Post | 46.14 ± 8.34 | 46.95 ± 12.17 | |||||
| Aggression | Pre | 46.52 ± 6.01 | 45.58 ± 8.51 | 0.834 | 0.240 | 0.621 | |
| Post | 44.86 ± 4.45 | 44.89 ± 10.11 | |||||
| Somatization | Pre | 51.00 ± 10.97 | 46.53 ± 7.21 | 0.150 | 0.001 *** | 0.496 | |
| Post | 46.14 ± 9.33 | 43.21 ± 6.12 | |||||
| Adaptation to reality | Manic episode | Pre | 51.71 ± 10.12 | 53.42 ± 15.99 | 0.484 | 0.571 | 0.596 |
| Post | 50.14 ± 8.84 | 53.37 ± 11.88 | |||||
| Paranoia | Pre | 46.38 ± 7.67 | 45.68 ± 8.16 | 0.904 | 0.904 | 0.552 | |
| Post | 45.86 ± 9.18 | 46.47 ± 9.82 | |||||
| Schizophrenia | Pre | 48.81 ± 7.75 | 50.84 ± 9.40 | 0.338 | 0.327 | 0.703 | |
| Post | 47.14 ± 6.53 | 50.11 ± 11.75 | |||||
| Others | Suicide | Pre | 45.76 ± 6.19 | 44.00 ± 5.89 | 0.781 | 0.914 | 0.242 |
| Post | 44.67 ± 7.69 | 45.31 ± 8.14 | |||||
| Addiction | Pre | 46.76 ± 2.41 | 50.89 ± 0.00 | 0.466 | 0.274 | 0.655 | |
| Post | 47.10 ± 3.63 | 46.79 ± 3.44 | |||||
| Sleep Problem | Pre | 53.95 ± 8.74 | 49.58 ± 10.21 | 0.410 | 0.144 | 0.050 * | |
| Post | 50.57 ± 8.98 | 50.05 ± 11.13 | |||||
| Stress Vulnerability | Pre | 51.71 ± 8.32 | 48.84 ± 10.48 | 0.488 | 0.026 * | 0.020 * | |
| Post | 48.10 ± 6.56 | 48.47 ± 10.68 | |||||
| Interpersonal Sensitivity | Pre | 52.24 ± 7.15 | 49.42 ± 10.83 | 0.796 | 0.318 | 0.072 | |
| Post | 49.00 ± 5.69 | 50.37 ± 12.98 | |||||
| Self-Regulation Problem | Pre | 51.19 ± 7.33 | 46.05 ± 8.79 | 0.265 | 0.005 ** | 0.029 * | |
| Post | 45.86 ± 7.30 | 45.32 ± 10.58 | |||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1 | ||||||||||||||||||||||||||
| 2 | −0.0208 | 1 | |||||||||||||||||||||||||
| 3 | −0.0473 ** | 0.627 ** | 1 | ||||||||||||||||||||||||
| 4 | 0.431 ** | −0.0519 ** | −0.0525 ** | 1 | |||||||||||||||||||||||
| 5 | 0.598 ** | −0.0539 ** | −0.0546 ** | 0.586 ** | 1 | ||||||||||||||||||||||
| 6 | −0.0316 * | 0.476 ** | −0.0501 ** | −0.0218 | −0.0459 ** | 1 | |||||||||||||||||||||
| 7 | 0.087 | −0.0310 | −0.0176 | 0.027 | 0.177 | −0.0250 | 1 | ||||||||||||||||||||
| 8 | −0.0289 | 0.233 | 0.310 | −0.0391 * | −0.0313 * | 0.114 | −0.0232 | 1 | |||||||||||||||||||
| 9 | −0.0115 | 0.179 | 0.177 | −0.0374 * | −0.0304 | 0.148 | 0.025 | 0.606 ** | 1 | ||||||||||||||||||
| 10 | −0.0202 | 0.196 | 0.285 | −0.0319 * | −0.0222 | 0.027 | −0.0097 | 0.397 * | 0.302 | 1 | |||||||||||||||||
| 11 | −0.0183 | 0.108 | 0.266 | −0.0280 | −0.0103 | −0.0032 | −0.0090 | 0.373 * | 0.263 | 0.863 ** | 1 | ||||||||||||||||
| 12 | −0.0061 | 0.251 | 0.135 | −0.0178 | −0.0287 | 0.137 | −0.0064 | 0.171 | 0.166 | 0.562 ** | 0.074 | 1 | |||||||||||||||
| 13 | 0.143 | 0.292 | 0.271 | −0.0125 | −0.0012 | 0.017 | 0.054 | 0.229 | 0.264 | 0.075 | 0.181 | −0.0102 | 1 | ||||||||||||||
| 14 | −0.0073 | 0.276 | 0.345 * | −0.0246 | −0.0121 | 0.080 | −0.0031 | 0.163 | 0.305 | 0.190 | 0.235 | 0.034 | 0.750 ** | 1 | |||||||||||||
| 15 | 0.320 * | 0.128 | 0.021 | 0.093 | 0.136 | −0.0090 | 0.129 | 0.152 | 0.061 | −0.0118 | −0.0011 | −0.0191 | 0.712 ** | 0.073 | 1 | ||||||||||||
| 16 | 0.034 | −0.0056 | −0.0033 | −0.0008 | 0.036 | 0.021 | −0.0123 | 0.373 * | 0.246 | 0.133 | 0.107 | 0.104 | 0.301 | 0.267 | 0.181 | 1 | |||||||||||
| 17 | −0.0039 | 0.143 | 0.066 | −0.0089 | −0.0080 | −0.0058 | 0.118 | 0.323 * | 0.548 ** | 0.479 ** | 0.466 ** | 0.162 | 0.311 | 0.159 | 0.285 | 0.175 | 1 | ||||||||||
| 18 | −0.0030 | 0.114 | 0.252 | −0.0227 | −0.0111 | −0.0155 | 0.178 | 0.300 | 0.307 | 0.467 ** | 0.466 ** | 0.148 | 0.392* | 0.349* | 0.211 | 0.318 * | 0.547 ** | 1 | |||||||||
| 19 | 0.116 | 0.103 | 0.035 | 0.016 | 0.060 | 0.453 ** | −0.0311 | 0.146 | 0.268 | −0.0025 | 0.059 | −0.0114 | 0.077 | 0.125 | −0.0038 | 0.290 | 0.180 | −0.0083 | 1 | ||||||||
| 20 | −0.0085 | 0.039 | 0.051 | −0.0257 | −0.0090 | −0.0074 | 0.061 | 0.322 * | 0.491 ** | 0.328 * | 0.354 * | 0.050 | 0.150 | 0.167 | 0.046 | −0.0031 | 0.598 ** | 0.195 | 0.238 | 1 | |||||||
| 21 | 0.023 | −0.0096 | 0.144 | −0.0104 | −0.0087 | 0.041 | 0.177 | 0.305 | 0.248 | 0.213 | 0.272 | −0.0017 | 0.192 | 0.399* | −0.0132 | 0.057 | −0.0052 | 0.144 | 0.031 | 0.365 * | 1 | ||||||
| 22 | −0.0175 | 0.138 | 0.201 | −0.0123 | −0.0266 | 0.019 | −0.0205 | 0.677 ** | 0.379 * | 0.139 | 0.039 | 0.192 | −0.0014 | −0.0204 | 0.194 | 0.127 | 0.271 | 0.065 | −0.0025 | 0.215 | 0.142 | 1 | |||||
| 23 | −0.0060 | 0.014 | 0.062 | 0.027 | −0.0040 | 0.120 | −0.0150 | 0.424 ** | 0.089 | −0.0024 | −0.0112 | 0.121 | 0.013 | −0.0179 | 0.208 | 0.333 * | −0.0034 | −0.0033 | 0.136 | −0.0131 | −0.0035 | 0.565 ** | 1 | ||||
| 24 | −0.0247 | 0.232 | 0.078 | −0.0216 | −0.0400 * | 0.302 | 0.064 | 0.220 | 0.496 ** | −0.0168 | −0.0156 | −0.0079 | 0.051 | 0.074 | −0.0012 | −0.0116 | 0.054 | −0.0034 | −0.0053 | 0.173 | 0.164 | 0.126 | −0.0046 | 1 | |||
| 25 | −0.0024 | 0.297 | 0.139 | −0.0346 * | −0.0348 * | 0.302 | 0.027 | 0.637 ** | 0.571 ** | 0.348 * | 0.266 | 0.288 | 0.256 | 0.237 | 0.123 | 0.369 * | 0.352 * | 0.313 * | 0.341 * | 0.327 * | 0.358 * | 0.447 ** | 0.288 | 0.145 | 1 | ||
| 26 | 0.008 | 0.255 | 0.037 | −0.0211 | −0.0286 | 0.201 | 0.082 | 0.468 ** | 0.433 ** | 0.321 * | 0.149 | 0.436 ** | 0.186 | 0.178 | 0.083 | 0.449 ** | 0.292 | 0.267 | 0.265 | 0.163 | 0.124 | 0.293 | 0.273 | −0.0038 | 0.866 ** | 1 | |
| 27 | −0.0070 | 0.241 | 0.215 | −0.0392 * | −0.0296 | 0.314 * | −0.0059 | 0.621 ** | 0.525 ** | 0.257 | 0.306 | 0.019 | 0.236 | 0.217 | 0.115 | 0.166 | 0.271 | 0.315* | 0.315* | 0.396* | 0.507 ** | 0.489 ** | 0.213 | 0.287 | 0.814 ** | 0.420 ** | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noh, E.; Kim, J.; Kim, M.; Yi, E. Effectiveness of SaBang-DolGi Walking Exercise Program on Physical and Mental Health of Menopausal Women. Int. J. Environ. Res. Public Health 2020, 17, 6935. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186935
Noh E, Kim J, Kim M, Yi E. Effectiveness of SaBang-DolGi Walking Exercise Program on Physical and Mental Health of Menopausal Women. International Journal of Environmental Research and Public Health. 2020; 17(18):6935. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186935
Chicago/Turabian StyleNoh, EunHee, JiYoun Kim, MunHee Kim, and EunSurk Yi. 2020. "Effectiveness of SaBang-DolGi Walking Exercise Program on Physical and Mental Health of Menopausal Women" International Journal of Environmental Research and Public Health 17, no. 18: 6935. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186935