Orthodontics First in Hemimandibular Hyperplasia. “Mind the Gap”


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
- Decompensating orthodontic treatment
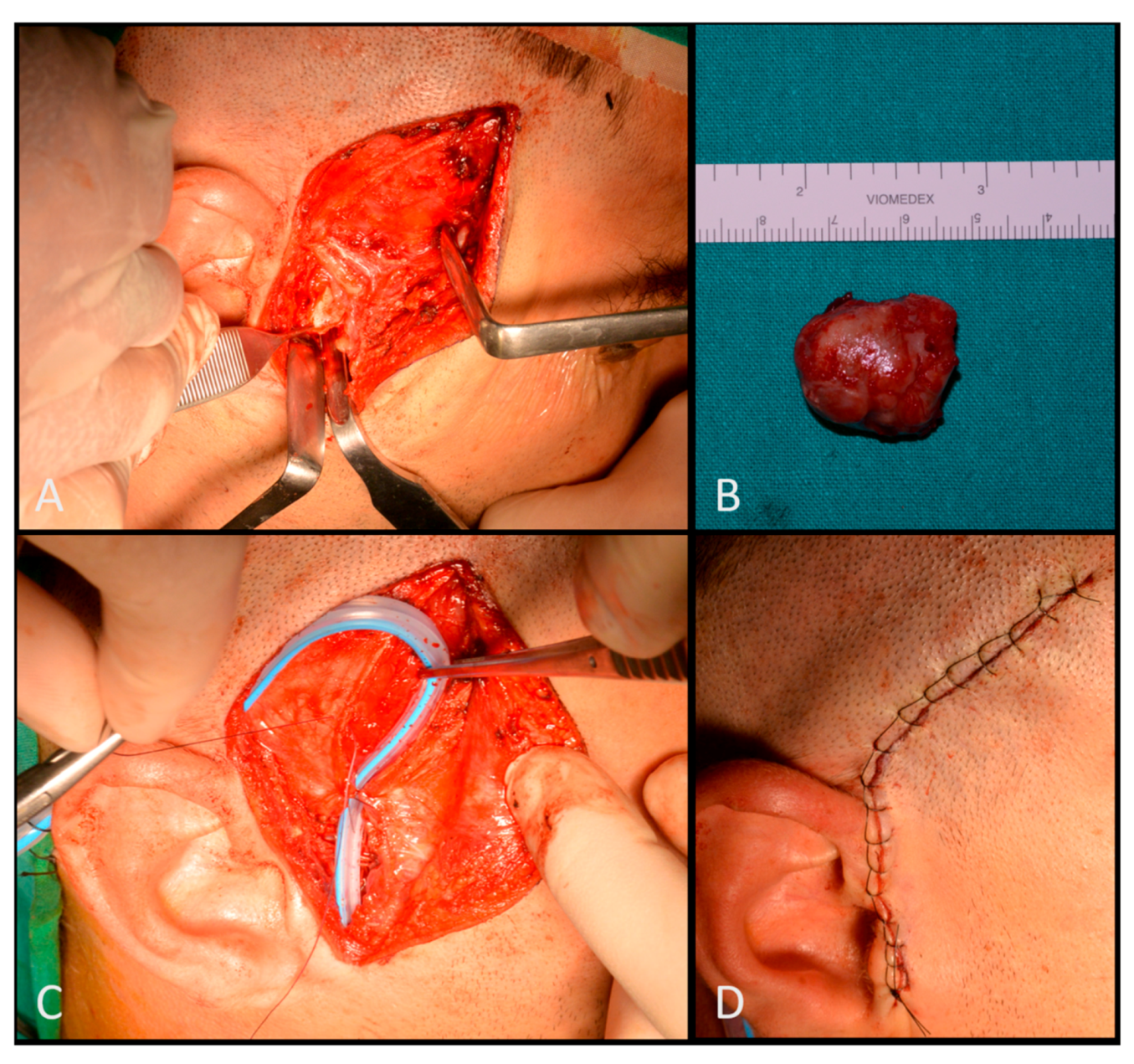
- Condylectomy
- Orthodontic refinement treatment
2.1. First Step
2.2. Second Step
2.3. Third Step
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Raijmakers, P.G.; Karssemakers, L.H.; Tuinzing, D.B. Female predominance and effect of gender on unilateral condylar hyperplasia: A review and meta-analysis. J. Oral Maxillofac. Surg. 2012, 70, e72–e76. [Google Scholar] [CrossRef] [PubMed]
- Almeida, L.E.; Zacharias, J.; Pierce, S. Condylar hyperplasia: An updated review of the literature. Korean J. Orthod. 2015, 45, 333–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obwegeser, H.L.; Obwegeser, J.A. New clinical-based evidence for the existence of 2 growth regulators in mandibular condyles: Hemimandibular elongation in hemifacial microsomia mandible. J. Craniofac. Surg. 2010, 21, 1595–1600. [Google Scholar] [CrossRef] [PubMed]
- Obwegeser, H.L.; Makek, M.S. Hemimandibular hyperplasia--hemimandibular elongation. J. Maxillofac. Surg. 1986, 14, 183–208. [Google Scholar] [CrossRef]
- Gray, R.J.; Sloan, P.; Quayle, A.A.; Carter, D.H. Histopathological and scintigraphic features of condylar hyperplasia. Int. J. Oral Maxillofac. Surg. 1990, 19, 65–71. [Google Scholar] [CrossRef]
- Gray, R.J.; Horner, K.; Testa, H.J.; Lloyd, J.J.; Sloan, P. Condylar hyperplasia: Correlation of histological and scintigraphic features. Dentomaxillofac. Radiol. 1994, 23, 103–107. [Google Scholar] [CrossRef]
- Eslami, B.; Behnia, H.; Javadi, H.; Khiabani, K.S.; Saffar, A.S. Histopathologic comparison of normal and hyperplastic condyles. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 96, 711–717. [Google Scholar] [CrossRef]
- Bertolini, F.; Bianchi, B.; De Riu, G.; Di Blasio, A.; Sesenna, E. Hemimandibular hyperplasia treated by early high condylectomy: A case report. Int. J. Adult Orthodon. Orthognath. Surg. 2001, 16, 227–234. [Google Scholar]
- Obwegeser, H.L. Mandibular Growth Anomalies: Terminology, Aetiology, Diagnosis, Treatment; Springer: Berlin/Heidelberg, Germany, 2001; p. 472. [Google Scholar]
- Saridin, C.P.; Raijmakers, P.G.; Tuinzing, D.B.; Becking, A.G. Bone scintigraphy as a diagnostic method in unilateral hyperactivity of the mandibular condyles: A review and meta-analysis of the literature. Int. J. Oral Maxillofac. Surg. 2011, 40, 11–17. [Google Scholar] [CrossRef]
- Lewis, E.L.; Dolwick, M.F.; Abramowicz, S.; Reeder, S.L. Contemporary imaging of the temporomandibular joint. Dent. Clin. N. Am. 2008, 52, 875–890. [Google Scholar] [CrossRef]
- Romano, A.; Lo Faro, C.; Salzano, G.; Dell’aversana Orabona, G.; Petrocelli, M.; Corvino, R.; Vaira, L.A.; Iaconetta, G.; Califano, L. Synovial chondromatosis of temporomandibular joint spreading into the cranial space. J. Oral Maxillofac. Surg. Med. Pathol. 2018, 30, 267–271. [Google Scholar] [CrossRef]
- Marchetti, C.; Cocchi, R.; Gentile, L.; Bianchi, A. Hemimandibular hyperplasia: Treatment strategies. J. Craniofac. Surg. 2000, 11, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.Y.; Fan, S.; Zhang, H.Q.; Lin, Z.Y.; Ye, J.T.; Li, J.S. Virtual Surgical Planning in Precise Maxillary Reconstruction With Vascularized Fibular Graft After Tumor Ablation. J. Oral Maxillofac. Surg. 2016, 74, 1255–1264. [Google Scholar] [CrossRef] [PubMed]
- Al-Kayat, A.; Bramley, P. A modified pre-auricular approach to the temporomandibular joint and malar arch. Br. J. Oral Surg. 1979, 17, 91–103. [Google Scholar] [CrossRef]
- Lo Giudice, R.; Puleio, F.; Rizzo, D.; Alibrandi, A.; Lo Giudice, G.; Centofanti, A.; Fiorillo, L.; Di Mauro, D.; Nicita, F. Comparative investigation of cutting devices on bone blocks: An SEM morphological analysis. Appl. Sci. 2019, 9, 351. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, J.W. Definitive surgical correction of the deformity resulting from hemimandibular hyperplasia. J. Craniomaxillofac. Surg. 2005, 33, 150–157. [Google Scholar] [CrossRef]
- Xu, M.; Chan, F.C.; Jin, X.; Xu, J.; Lu, J.; Zhang, C.; Teng, L. Hemimandibular hyperplasia: Classification and treatment algorithm revisited. J. Craniofac. Surg. 2014, 25, 355–358. [Google Scholar] [CrossRef]
- Hagensli, N.; Stenvik, A.; Espeland, L. Patients offered orthognathic surgery: Why do many refrain from treatment? J. Craniomaxillofac. Surg. 2014, 42, e296–e300. [Google Scholar] [CrossRef]
- Santagata, M.; De Luca, R.; Lo Giudice, G.; Troiano, A.; Lo Giudice, G.; Corvo, G.; Tartaro, G. Arthrocentesis and sodium hyaluronate infiltration in temporomandibular disorders treatment. Clinical and MRI evaluation. J. Funct. Morphol. Kinesiol. 2020, 5, 18. [Google Scholar] [CrossRef] [Green Version]
- Solow, B. The dentoalveolar compensatory mechanism: Background and clinical implications. Br. J. Orthod. 1980, 7, 145–161. [Google Scholar] [CrossRef]
- Lo Giudice, R.; Nicita, F.; Puleio, F.; Alibrandi, A.; Cervino, G.; Lizio, A.S.; Pantaleo, G. Accuracy of periapical radiography and CBCT in endodontic evaluation. Int. J. Dent. 2018, 2018, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perrotta, S.; Lo Giudice, G.; Bocchino, T.; Califano, L.; Valletta, R. Orthodontics First in Hemimandibular Hyperplasia. “Mind the Gap”. Int. J. Environ. Res. Public Health 2020, 17, 7087. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197087
Perrotta S, Lo Giudice G, Bocchino T, Califano L, Valletta R. Orthodontics First in Hemimandibular Hyperplasia. “Mind the Gap”. International Journal of Environmental Research and Public Health. 2020; 17(19):7087. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197087
Chicago/Turabian StylePerrotta, Stefania, Giorgio Lo Giudice, Tecla Bocchino, Luigi Califano, and Rosa Valletta. 2020. "Orthodontics First in Hemimandibular Hyperplasia. “Mind the Gap”" International Journal of Environmental Research and Public Health 17, no. 19: 7087. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197087