The Development of a Knowledge Test on Transgender Patients’ Care

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodology
2.2. Inclusion and Exclusion Criteria
2.3. Sample Description
3. Results
3.1. Demographic Characteristics of the Participants
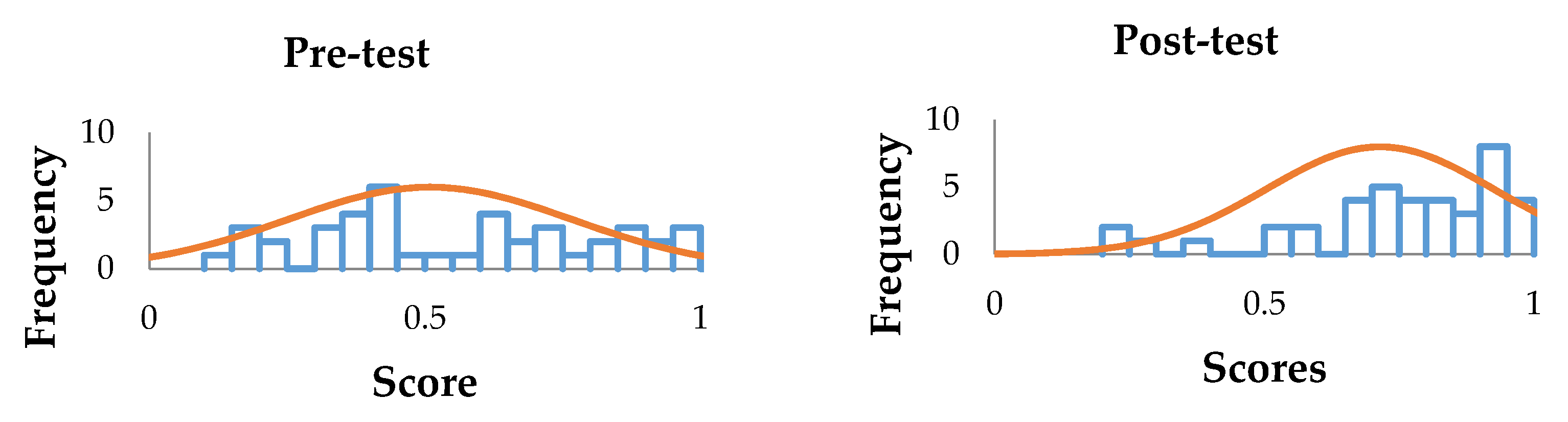
3.2. Assessment of the Preliminary Instrument Results as Pre and Post-Test
3.3. Basic Psychometrics, Internal Consistency, and Confidence Intervals
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Spanish Version of the Instrument with 42 Items (Pre-Test Copy)











Appendix B. Items by Unit in Pre and Post-Test
| Unidad | Item | Pre-Prueba | Post-Prueba | ||||||||
| SD | IDI | ID | ITC | SD | IDI | ID | ITC | ||||
| Unidad 1: Introducción al Cuidado de los Pacientes Transgénero | K 1.1 | 0.63 | 0.49 | 0.63 | 0.29 | 0.30 | 0.98 | 0.13 | 0.98 | 0.06 | 0.08 |
| K 1.2 | 0.89 | 0.31 | 0.89 | 0.24 | 0.32 | 0.86 | 0.35 | 0.86 | 0.19 | 0.21 | |
| K 1.3 | 0.56 | 0.50 | 0.56 | 0.29 | 0.31 | 0.69 | 0.47 | 0.69 | 0.44 | 0.36 | |
| K 1.4 | 0.59 | 0.50 | 0.59 | 0.65 | 0.45 | 0.79 | 0.41 | 0.79 | 0.25 | 0.20 | |
| K 1.5 | 0.59 | 0.50 | 0.59 | 0.76 | 0.56 | 0.84 | 0.37 | 0.84 | 0.25 | 0.26 | |
| K 1.6 | 0.91 | 0.29 | 0.91 | 0.00 | 0.07 | 0.95 | 0.22 | 0.95 | 0.06 | 0.18 | |
| K 1.7 | 0.94 | 0.24 | 0.94 | 0.18 | 0.20 | 0.95 | 0.23 | 0.95 | 0.19 | 0.31 | |
| Unidad 2: Otros Problemas de Salud de los Pacientes Transgénero | K 2.1 | 0.28 | 0.45 | 0.28 | 0.06 | 0.05 | 0.53 | 0.50 | 0.53 | 0.44 | 0.29 |
| K 2.2 | 0.67 | 0.47 | 0.67 | 0.41 | 0.21 | 0.79 | 0.41 | 0.79 | 0.13 | 0.08 | |
| K 2.3 | 0.08 | 0.27 | 0.08 | 0.12 | 0.18 | 0.21 | 0.41 | 0.21 | 0.13 | 0.02 | |
| K 2.4 | 0.94 | 0.24 | 0.94 | −0.06 | −0.06 | 0.88 | 0.33 | 0.88 | 0.13 | 0.18 | |
| K 2.5 | 0.66 | 0.48 | 0.66 | 0.47 | 0.39 | 0.74 | 0.44 | 0.74 | 0.38 | 0.38 | |
| K 2.6 | 0.56 | 0.50 | 0.56 | 0.18 | 0.19 | 0.64 | 0.49 | 0.64 | 0.56 | 0.44 | |
| K 2.7 | 0.38 | 0.49 | 0.38 | 0.65 | 0.45 | 0.66 | 0.48 | 0.66 | 0.38 | 0.36 | |
| K 2.8 | 0.38 | 0.49 | 0.38 | 0.59 | 0.47 | 0.90 | 0.31 | 0.90 | 0.25 | 0.32 | |
| K 2.9 | 0.11 | 0.31 | 0.11 | −0.12 | −0.27 | 0.53 | 0.50 | 0.53 | −0.13 | −0.05 | |
| K 2.10 | 0.36 | 0.48 | 0.36 | 0.65 | 0.51 | 0.81 | 0.40 | 0.81 | 0.25 | 0.30 | |
| K 2.11 | 0.81 | 0.39 | 0.81 | 0.24 | 0.31 | 0.62 | 0.49 | 0.62 | 0.44 | 0.37 | |
| K 2.12 | 0.14 | 0.35 | 0.14 | −0.06 | −0.09 | 0.16 | 0.37 | 0.16 | 0.25 | 0.28 | |
| K 2.13 | 0.72 | 0.45 | 0.72 | 0.29 | 0.29 | 0.86 | 0.35 | 0.86 | 0.38 | 0.39 | |
| K 2.14 | 0.84 | 0.37 | 0.84 | 0.12 | 0.11 | 0.88 | 0.33 | 0.88 | 0.25 | 0.30 | |
| Unidad 3: Terapia Hormonal para la Transición de Género | K 3.1 | 0.42 | 0.50 | 0.42 | 0.41 | 0.31 | 0.62 | 0.49 | 0.62 | 0.25 | 0.29 |
| K 3.2 | 0.52 | 0.50 | 0.52 | 0.41 | 0.39 | 0.74 | 0.44 | 0.74 | 0.31 | 0.41 | |
| K 3.3 | 0.38 | 0.49 | 0.38 | 0.29 | 0.26 | 0.91 | 0.28 | 0.91 | 0.31 | 0.55 | |
| K 3.4 | 0.77 | 0.43 | 0.77 | 0.35 | 0.29 | 0.91 | 0.28 | 0.91 | 0.25 | 0.38 | |
| K 3.5 | 0.45 | 0.50 | 0.45 | 0.29 | 0.26 | 0.90 | 0.31 | 0.90 | 0.25 | 0.37 | |
| K 3.6 | 0.84 | 0.37 | 0.84 | 0.06 | 0.08 | 0.97 | 0.18 | 0.97 | 0.06 | 0.27 | |
| K 3.7 | 0.28 | 0.45 | 0.28 | 0.29 | 0.14 | 0.33 | 0.47 | 0.33 | 0.44 | 0.41 | |
| K 3.8 | 0.34 | 0.48 | 0.34 | 0.35 | 0.30 | 0.67 | 0.47 | 0.67 | 0.31 | 0.37 | |
| K 3.9 | 0.36 | 0.48 | 0.36 | 0.29 | 0.23 | 0.47 | 0.50 | 0.47 | 0.44 | 0.38 | |
| K 3.10 | 0.27 | 0.45 | 0.27 | 0.29 | 0.20 | 0.84 | 0.37 | 0.84 | 0.13 | 0.22 | |
| K 3.11 | 0.34 | 0.48 | 0.34 | 0.24 | 0.12 | 0.71 | 0.46 | 0.71 | 0.63 | 0.44 | |
| K 3.12 | 0.64 | 0.48 | 0.64 | 0.24 | 0.24 | 0.67 | 0.47 | 0.67 | 0.44 | 0.39 | |
| K 3.13 | 0.77 | 0.43 | 0.77 | 0.47 | 0.50 | 0.88 | 0.33 | 0.88 | 0.19 | 0.38 | |
| K 3.14 | 0.31 | 0.47 | 0.31 | 0.29 | 0.32 | 0.72 | 0.45 | 0.72 | 0.44 | 0.43 | |
| K 3.15 | 0.38 | 0.49 | 0.38 | 0.53 | 0.42 | 0.48 | 0.50 | 0.48 | 0.69 | 0.48 | |
| K 3.16 | 0.33 | 0.47 | 0.33 | 0.41 | 0.39 | 0.76 | 0.43 | 0.76 | 0.50 | 0.43 | |
| K 3.17 | 0.66 | 0.48 | 0.66 | 0.29 | 0.35 | 0.67 | 0.47 | 0.67 | 0.19 | 0.25 | |
| K 3.18 | 0.13 | 0.33 | 0.13 | 0.06 | 0.13 | 0.79 | 0.41 | 0.79 | 0.38 | 0.39 | |
| K 3.19 | 0.86 | 0.35 | 0.86 | 0.18 | 0.28 | 0.86 | 0.35 | 0.86 | 0.31 | 0.36 | |
| K 3.20 | 0.16 | 0.37 | 0.16 | 0.00 | 0.00 | 0.62 | 0.49 | 0.62 | 0.38 | 0.30 | |
| K 3.21 | 0.16 | 0.37 | 0.16 | −0.06 | −0.03 | 0.19 | 0.40 | 0.19 | 0.38 | 0.34 | |
| = mean score; SD = standard deviation; IDI = item difficulty index; ID = item discrimination; ITC = item-total correlation. | |||||||||||
References
- Taber, K.S. The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res. Sci. Educ. 2017, 48, 1273–1296. [Google Scholar] [CrossRef]
- Taber, K.S. Classroom-Based Research and Evidence-Based Practice: An Introduction, 2nd ed.; Sage: London, UK, 2013. [Google Scholar]
- Eckstein, M.A.; Newsome, C.E.; Borrego, M.; Burnett, A.E.; Wittstrom, K.; Conklin, J. A cross-sectional survey evaluating transgender-related care education in United States pharmacy school curricula. Curr. Pharm. Teach. Learn. 2019, 11, 782–792. [Google Scholar] [CrossRef] [PubMed]
- Leach, C.; Layson-Wolf, C. Survey of community pharmacy residents’ perceptions of transgender health management. J. Am. Pharm. Assoc. 2016, 56, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Wilkening, G.L. The current status of transgender health education in doctor of pharmacy curricula in North America. Ment. Health Clin. 2017, 7, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Grundmann, O.; Segal, R.; Pullo, J.; Davis, L.; Felix-Irizarry, Y.; Da Silva, L.; Holets, T. The Pharmacist as an LGBTQ Ally. Am. J. Pharm. Educ. 2020, 84. [Google Scholar] [CrossRef]
- Llayton, C.K.; Caldas, L.M. Strategies for inclusion of lesbian, gay, bisexual, transgender, queer, intersex, and asexual (LGBTQIA+) education throughout pharmacy school curricula. Pharm. Pract. 2020, 18, 1862. [Google Scholar] [CrossRef]
- Melin, K.; Hilera-Botet, C.R.; Vega-Vélez, D.; Salgado-Crespo, V.M.; Santiago, D.; Hernández-Agosto, J.; Muñoz-Burgos, A.; Cajigas, Z.; Martínez-Vélez, J.J.; Rodríguez-Díaz, C.E. Readiness to provide pharmaceutical care to transgender patients: Perspectives from pharmacists and transgender individuals. J. Am. Pharm. Assoc. 2019, 59, 651–659. [Google Scholar] [CrossRef]
- Grant, J.M.; Mottet, L.A.; Tanis, J.; Harrison, J.; Herman, J.L.; Keisling, M. Injustice at Every Turn: A Report of the National Transgender Discrimination Survey. Available online: http://transequality.org/PDFs/NTDS_Report.pdf\nhttp://2fwww.thetaskforce.org/downloads/resources_and_tools/ntds_report_on_health.pdf (accessed on 31 August 2020).
- UCSF. Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People, 2nd ed.; Deutsch, M.B., Ed.; Center of Excellence for Transgender Health: San Francisco, CA, USA, 2016. [Google Scholar]
- Safer, J.D.; Coleman, E.; Feldman, J.; Garofalo, R.; Hembree, W.; Radix, A.; Sevelius, J. Barriers to healthcare for transgender individuals. Curr. Opin. Endocrinol. Diabetes Obes. 2016, 23, 168–171. [Google Scholar] [CrossRef] [Green Version]
- Kelley, L.; Chou, C.L.; Dibble, S.L.; Robertson, P.A. A Critical Intervention in Lesbian, Gay, Bisexual, and Transgender Health: Knowledge and Attitude Outcomes among Second-Year Medical Students. Teach. Learn. Med. 2008, 20, 248–253. [Google Scholar] [CrossRef]
- Banerjee, S.C.; Walters, C.B.; Staley, J.M.; Alexander, K.; Parker, P. Knowledge, Beliefs, and Communication Behavior of Oncology Health-care Providers (HCPs) regarding Lesbian, Gay, Bisexual, and Transgender (LGBT) Patient Health care. J. Health Commun. 2018, 23, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Dy, G.W.; Osbun, N.C.; Morrison, S.D.; Grant, D.W.; Merguerian, P.A. Exposure to and Attitudes Regarding Transgender Education Among Urology Residents. J. Sex. Med. 2016, 13, 1466–1472. [Google Scholar] [CrossRef] [PubMed]
- Rowan, S.P.; Lilly, C.L.; Shapiro, R.E.; Kidd, K.M.; Elmo, R.M.; Altobello, R.A.; Vallejo, M.C. Knowledge and Attitudes of Health Care Providers Toward Transgender Patients Within a Rural Tertiary Care Center. Transgender Health 2019, 4, 24–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colton, D.; Covert, R.W. Designing and Constructing Instruments for Social Research and Evaluation, 3rd ed.; John Wiley & Sons, Inc.: San Francisco, CA, USA, 2007. [Google Scholar]
- ESCO Group. Available online: https://www.escogroup.org/hvac/examdevelopment.aspx (accessed on 17 June 2020).
- Clark, L.A.; Watson, D. Constructing Validity: Basic Issues in Objective Scale Development. Psychol. Assess. 1995, 7, 309–319. [Google Scholar] [CrossRef]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research: A Primer. Front. Public Health 2018, 6. [Google Scholar] [CrossRef]
- Coleman, E.; Bockting, W.; Botzer, M.; Cohen-Kettenis, P.; Decuypere, G.; Feldman, J.; Fraser, L.; Green, J.; Knudson, G.; Meyer, W.J.; et al. Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7. Int. J. Transgenderism 2012, 13, 165–232. [Google Scholar] [CrossRef]
- Domínguez-Lara, S.A.; Merino-Soto, C. ¿Por qué es importante reportar los intervalos de confianza del coeficiente alfa de Cronbach? Rev. Latinoam. Cienc. Soc. Niñez Juv. 2015, 13, 1326–1328. [Google Scholar]
- Matlock-Hetzel, S. Basic Concepts in Item and Test Analysis. Available online: http://ericae.net/ft/tamu/Espy.htm (accessed on 3 July 2020).
- Caycho-Rodríguez, T. Intervalos de Confianza para el coeficiente alfa de Cronbach: Aportes a la investigación pediátrica. Acta Pediátrica México 2017, 38, 291. [Google Scholar] [CrossRef]
- Thompson, B.; Levitov, J.E. Using microcomputers to score and evaluate test items. Coll. Microcomput. 1985, 3, 163–168. [Google Scholar]
- Berger, R.; Hänze, M. Impact of Expert Teaching Quality on Novice Academic Performance in the Jigsaw Cooperative Learning Method. Int. J. Sci. Educ. 2014, 37, 294–320. [Google Scholar] [CrossRef]
- Bretz, S.L.; McClary, L. Students’ Understandings of Acid Strength: How Meaningful Is Reliability When Measuring Alternative Conceptions? J. Chem. Educ. 2014, 92, 212–219. [Google Scholar] [CrossRef]
- Ledesma, R.D. AlphaCI: Un programa de cálculo de intervalos de confianza para el coeficiente alfa de Cronbach. Psico-USF 2004, 9, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Confidence Intervals for a Sample Cronbach Coefficient Alpha Value Calculator. Available online: https://www.psyctc.org/stats/R/Feldt1.html (accessed on 3 July 2020).
- Schmitt, N. Uses and abuses of coefficient alpha. Psychol. Assess. 1996, 8, 350–353. [Google Scholar] [CrossRef]


{kind=link}
| Test Unit | Items | Total Items |
|---|---|---|
| Unit 1 | 1–7 | 7 |
| Unit 2 | 8–21 | 14 |
| Unit 3 | 22–42 | 21 |
| Statistic | Unit 1 | Unit 2 | Unit 3 | Overall Instrument | ||||
|---|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Pre-Test | Post-Test | Pre-Test | Post-Test | Pre-Test | Post-Test | |
| 0.7299 | 0.8670 | 0.4944 | 0.6576 | 0.4449 | 0.7011 | 0.5089 | 0.7142 | |
| s | 0.216 | 0.156 | 0.135 | 0.144 | 0.135 | 0.170 | 0.1112 | 0.1251 |
| CV | 29.59% | 17.99% | 27.31% | 21.90% | 30.34% | 24.25% | 21.85% | 17.52% |
| Statistical Test | Pre-Test | Post-Test |
|---|---|---|
| IDI | 0.08–0.94 | 0.16–0.98 |
| ID | 28 items > 0.20 | 30 items > 0.20 |
| ITC | 28 items > 0.20 | 36 items > 0.20 |
| 10 items 0 ≥ 0.19 | 5 items 0 ≥ 0.19 | |
| 4 items < 0 | 1 item < 0 |
| Section | α Pre-Test, (95%: CI-α) | α Post-Test, (95%: CI-α) |
|---|---|---|
| n = 64 | n = 58 | |
| Overall instrument | 0.65; (0.52–0.76) | 0.77; (0.68–0.85) |
| Unit 1 | 0.54; (0.34–0.69) | 0.42; (0.16–0.62) |
| Unit 2 | 0.33; (0.06–0.55) | 0.43; (0.19–0.62) |
| Unit 3 | 0.50; (0.30–0.66) | 0.75; (0.65–0.83) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Agosto, J.; Melin, K.; Rosa-Vega, J.; Carlo-Frontera, E.; Rodríguez-Ochoa, A.; Santiago-Quiñones, D. The Development of a Knowledge Test on Transgender Patients’ Care. Int. J. Environ. Res. Public Health 2020, 17, 7192. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197192
Hernández-Agosto J, Melin K, Rosa-Vega J, Carlo-Frontera E, Rodríguez-Ochoa A, Santiago-Quiñones D. The Development of a Knowledge Test on Transgender Patients’ Care. International Journal of Environmental Research and Public Health. 2020; 17(19):7192. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197192
Chicago/Turabian StyleHernández-Agosto, Jonathan, Kyle Melin, Jurynelliz Rosa-Vega, Edgar Carlo-Frontera, Andrés Rodríguez-Ochoa, and Darlene Santiago-Quiñones. 2020. "The Development of a Knowledge Test on Transgender Patients’ Care" International Journal of Environmental Research and Public Health 17, no. 19: 7192. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197192