The Association between Insulin Resistance and Cardiovascular Disease Risk: A Community-Based Cross-Sectional Study among Taiwanese People Aged over 50 Years


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Anthropometric
2.3. Laboratory Examinations
2.4. Assessment of Insulin Resistance
2.5. Cardiovascular Risk Assessments
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Patient Population
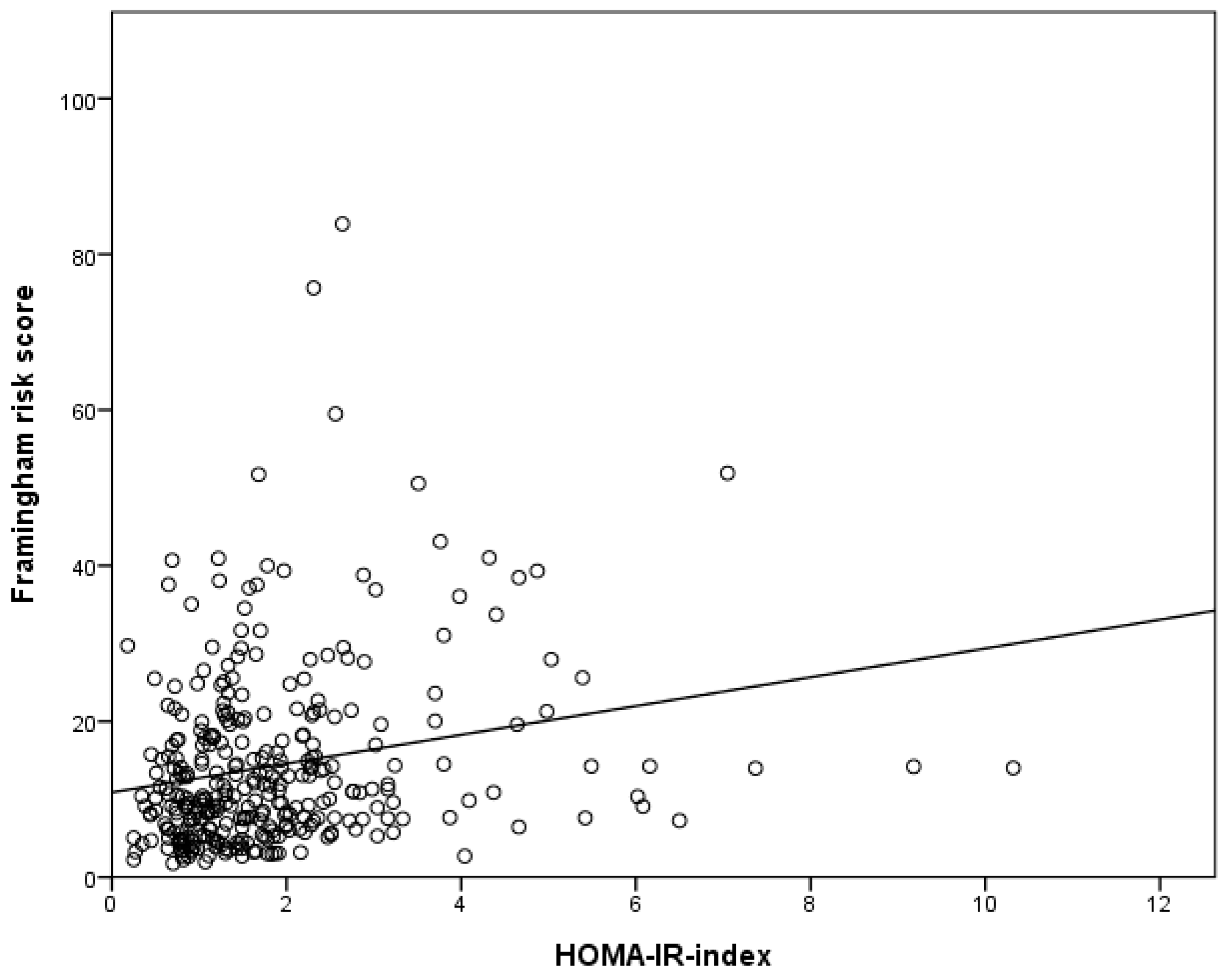
3.2. Correlation Analysis
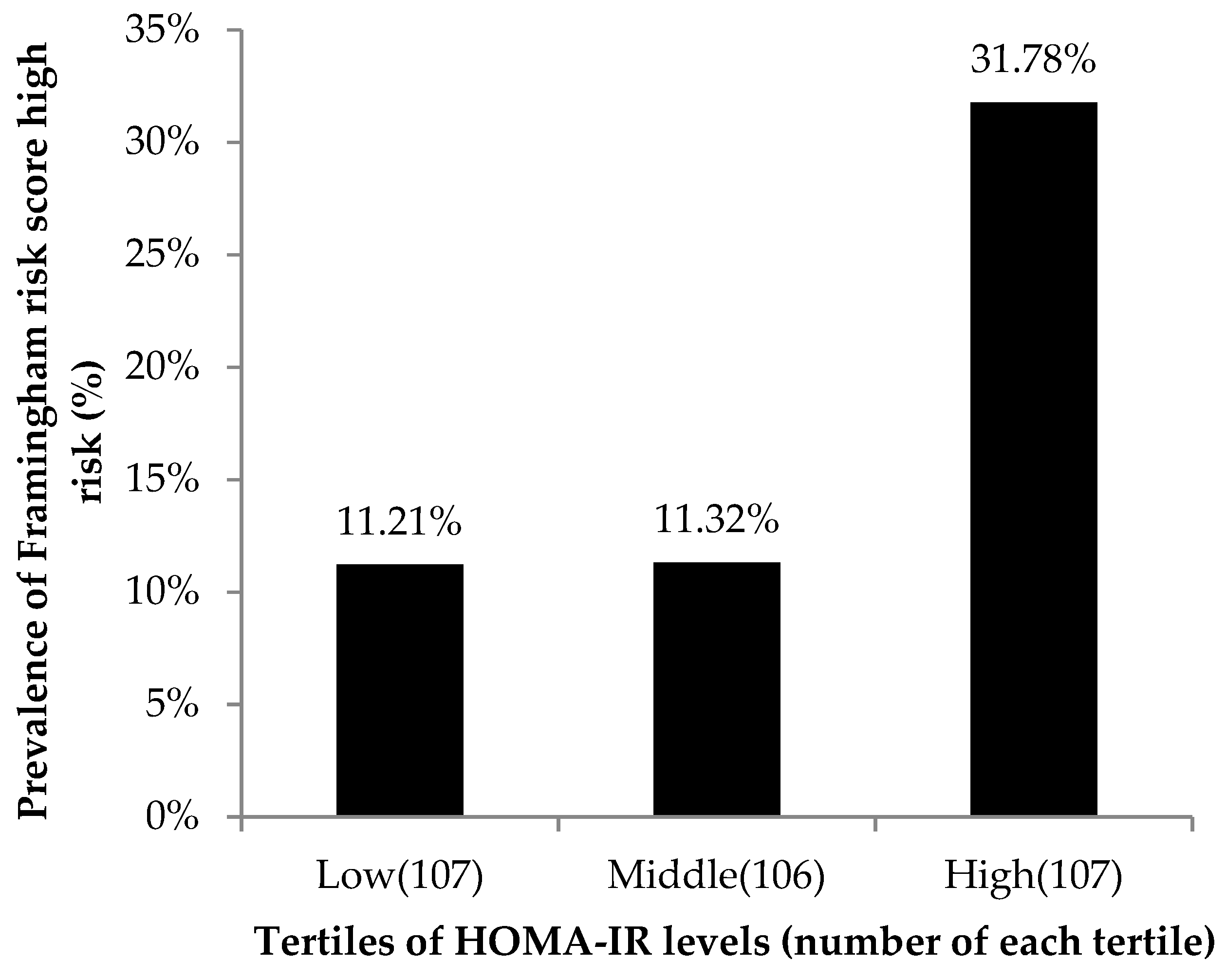
3.3. Association between the Tertiles of HOMA-IR Levels and the Framingham Risk Factors
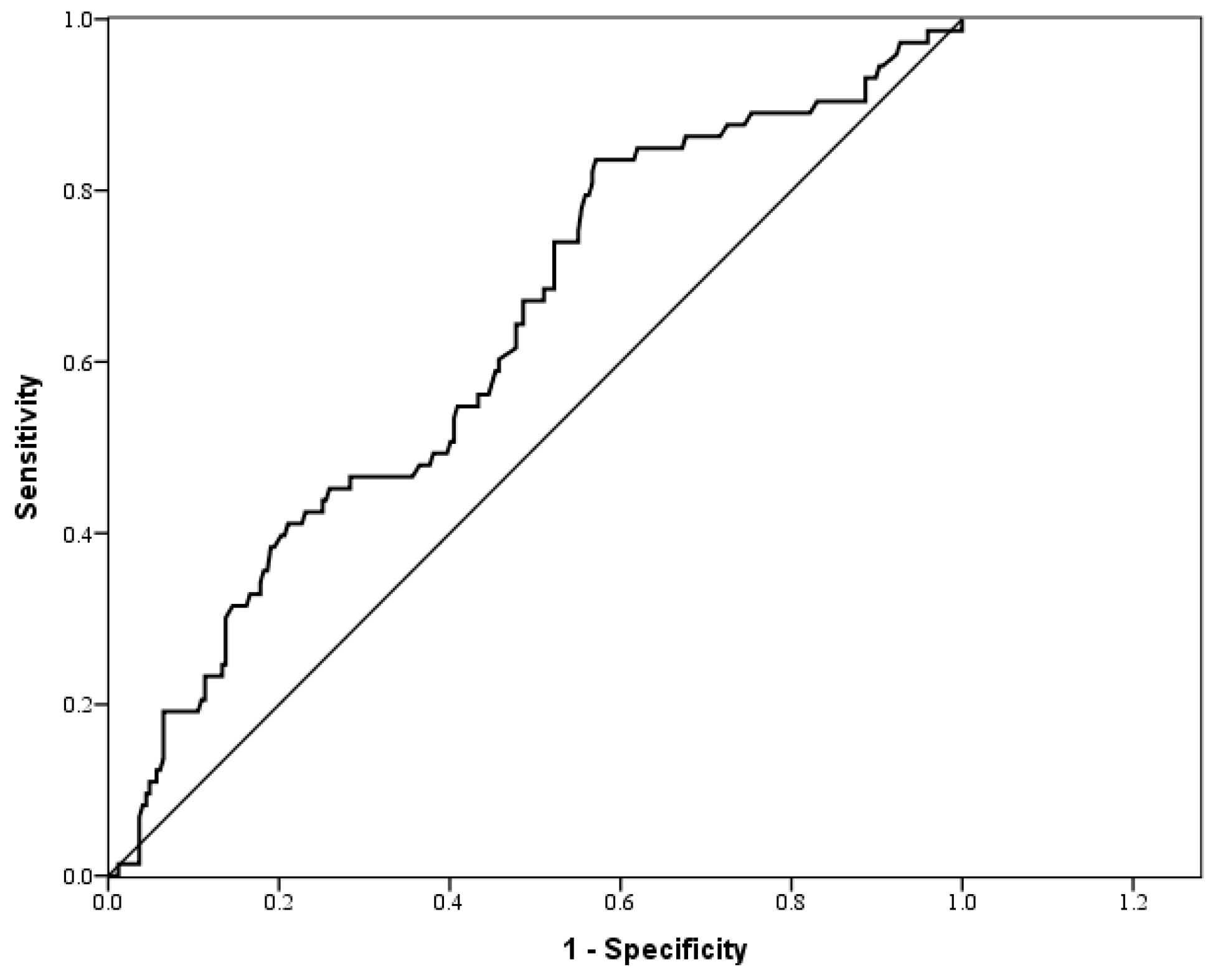
3.4. ROC Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| HOMA-IR | homeostasis model assessment of insulin resistance |
| IR | insulin resistance |
| CVD | cardiovascular disease |
| CKD | chronic kidney disease |
| WC | waist circumference |
| FRS | Framingham risk score |
| BMI | body mass index |
| BP | blood pressure |
| FPG | fasting plasma glucose |
| HDL-C | high-density lipoprotein cholesterol |
| LDL-C | low-density lipoprotein cholesterol |
| TG | triglyceride |
| ALT | alanine aminotransferase |
| eGFR | estimated glomerular filtration rate |
| ROC | receiver operating characteristic |
| AUC | area under the ROC curve |
| OR | odds ratio |
| aOR | adjusted odds ratio |
References
- DeFronzo, R. Insulin resistance: a multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidaemia and atherosclerosis. Neth. J. Med. 1997, 50, 191–197. [Google Scholar] [CrossRef]
- Beilby, J.P. Definition of Metabolic Syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association Conference on Scientific Issues Related to Definition. Clin. Biochem. Rev. 2004, 25, 195–198. [Google Scholar]
- Girman, C.J.; Rhodes, T.; Mercuri, M.; Pyörälä, K.; Kjekshus, J.; Pedersen, T.R.; A Beere, P.; Gotto, A.M.; Clearfield, M. The metabolic syndrome and risk of major coronary events in the Scandinavian Simvastatin Survival Study (4S) and the Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS). Am. J. Cardiol. 2004, 93, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Lakka, H.-M.; Laaksonen, D.E.; Lakka, T.; Niskanen, L.K.; Kumpusalo, E.; Tuomilehto, J.; Salonen, J.T. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA 2002, 288, 2709–2716. [Google Scholar] [CrossRef] [PubMed]
- Eckel, R.; Alberti, K.; Grundy, S.M.; Zimmet, P. The metabolic syndrome. Lancet 2010, 375, 181–183. [Google Scholar] [CrossRef]
- Reaven, G.M. Banting lecture 1988. Role of insulin resistance in human disease. Diabetes 1988, 37, 1595–1607. [Google Scholar] [CrossRef]
- Després, J.-P.; Lamarche, B.; Mauriège, P.; Cantin, B.; Dagenais, G.R.; Moorjani, S.; Lupien, P.-J. Hyperinsulinemia as an Independent Risk Factor for Ischemic Heart Disease. New Engl. J. Med. 1996, 334, 952–958. [Google Scholar] [CrossRef]
- Wang, F.; Han, L.; Hu, D. Fasting insulin, insulin resistance and risk of hypertension in the general population: A meta-analysis. Clin. Chim. Acta 2017, 464, 57–63. [Google Scholar] [CrossRef]
- Hernandez-Rodas, M.C.; Valenzuela, R.; A Videla, L. Relevant Aspects of Nutritional and Dietary Interventions in Non-Alcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2015, 16, 25168–25198. [Google Scholar] [CrossRef] [Green Version]
- E Kosmas, C.; Silverio, D.; Tsomidou, C.; Salcedo, M.D.; Montan, P.D.; Guzman, E. The Impact of Insulin Resistance and Chronic Kidney Disease on Inflammation and Cardiovascular Disease. Clin. Med. Insights: Endocrinol. Diabetes 2018, 11. [Google Scholar] [CrossRef]
- Petridou, E.T.; Sergentanis, T.; Antonopoulos, C.N.; Dessypris, N.; Matsoukis, I.L.; Aronis, K.N.; Efremidis, A.; Syrigos, C.; Mantzoros, C.S. Insulin resistance: an independent risk factor for lung cancer? Metab. 2011, 60, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Wang, J.; Li, Y. Insulin resistance and cognitive dysfunction. Clin. Chim. Acta 2015, 444, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, R.; Videla, L.A. The importance of the long-chain polyunsaturated fatty acid n-6/n-3 ratio in development of non-alcoholic fatty liver associated with obesity. Food Funct. 2011, 2, 644–648. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: insulin resistance and ?-cell function from fasting plasma glucose and insulin concentrations in man. Diabetol. 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selvarajah, S.; Kaur, G.; Haniff, J.; Cheong, K.C.; Hiong, T.G.; Van Der Graaf, Y.; Bots, M.L. Comparison of the Framingham Risk Score, SCORE and WHO/ISH cardiovascular risk prediction models in an Asian population. Int. J. Cardiol. 2014, 176, 211–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Wang, F.; Xu, H.; Qian, Y.; Zou, J.; Yang, M.; Zhu, H.; Yi, H.; Guan, J.; Yin, S. Interrelationships among common predictors of cardiovascular diseases in patients of OSA: A large-scale observational study. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, A.P.; Oliveira, C.E.R.; De França, N.M. Metabolic syndrome and risk factors for cardiovascular disease in obese children: the relationship with insulin resistance (HOMA-IR). J. de Pediatr. 2007, 83, 21–26. [Google Scholar] [CrossRef] [Green Version]
- D’Agostino, R.B.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.; Kannel, W.B. General Cardiovascular Risk Profile for Use in Primary Care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [Green Version]
- Stern, M.P.; Williams, K.; Gonzalez-Villalpando, C.; Hunt, K.J.; Haffner, S.M. Does the Metabolic Syndrome Improve Identification of Individuals at Risk of Type 2 Diabetes and/or Cardiovascular Disease? Diabetes Care 2004, 27, 2676–2681. [Google Scholar] [CrossRef] [Green Version]
- McNeill, A.M.; Rosamond, W.D.; Girman, C.J.; Golden, S.H.; Schmidt, M.I.; East, H.E.; Ballantyne, C.M.; Heiss, G. The Metabolic Syndrome and 11-Year Risk of Incident Cardiovascular Disease in the Atherosclerosis Risk in Communities Study. Diabetes Care 2005, 28, 385–390. [Google Scholar] [CrossRef] [Green Version]
- Hu, G.; Qiao, Q.; Tuomilehto, J.; Balkau, B.; Borch-Johnsen, K.; Pyorala, K. Prevalence of the Metabolic Syndrome and Its Relation to All-Cause and Cardiovascular Mortality in Nondiabetic European Men and Women. Arch. Intern. Med. 2004, 164, 1066–1076. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Shaper, A.G.; Lennon, L.T.; Morris, R. Metabolic Syndrome vs Framingham Risk Score for Prediction of Coronary Heart Disease, Stroke, and Type 2 Diabetes Mellitus. Arch. Intern. Med. 2005, 165, 2644–2650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zúñiga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef] [PubMed]
- Ragheb, R.; Shanab, G.M.; Medhat, A.M.; Seoudi, D.M.; Adeli, K.; Fantus, I. Free fatty acid-induced muscle insulin resistance and glucose uptake dysfunction: Evidence for PKC activation and oxidative stress-activated signaling pathways. Biochem. Biophys. Res. Commun. 2009, 389, 211–216. [Google Scholar] [CrossRef] [Green Version]
- Roden, M.; Price, T.B.; Perseghin, G.; Petersen, K.F.; Rothman, D.L.; Cline, G.W.; Shulman, G.I. Mechanism of free fatty acid-induced insulin resistance in humans. J. Clin. Investig. 1996, 97, 2859–2865. [Google Scholar] [CrossRef] [Green Version]
- Muniyappa, R.; Sowers, J.R. Role of insulin resistance in endothelial dysfunction. Rev. Endocr. Metab. Disord. 2013, 14, 5–12. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| HOMA-IR Levels | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Low (HOMA-IR ≤ 1.15) | Middle (1.15 < HOMA-IR ≤ 1.93) | High (HOMA-IR > 1.93) | ||||||
| Variables | (n = 320) | (n = 107) | (n = 106) | (n = 107) | p-value | ||||
| Age (year) | 61.88 | ±6.21 | 61.38 | ±6.13 | 61.72 | ±6.54 | 62.53 | ±5.93 | 0.38 |
| SBP (mmHg) | 128.76 | ±16.09 | 124.52 | ±16.77 | 129.20 | ±14.41 | 132.56 | ±16.11 | 0.001 |
| DBP (mmHg) | 78.12 | ±10.80 | 76.80 | ±11.56 | 78.01 | ±9.97 | 79.55 | ±10.72 | 0.176 |
| BMI (kg/m2) | 24.61 | ±3.52 | 22.95 | ±2.99 | 24.55 | ±2.82 | 26.32 | ±3.84 | <0.001 |
| Waist circumference (cm) | 84.54 | ±9.37 | 80.31 | ±7.52 | 83.62 | ±8.04 | 89.68 | ±9.89 | <0.001 |
| ALT (U/L) | 22.89 | ±12.89 | 19.61 | ±7.49 | 22.18 | ±11.71 | 26.89 | ±16.75 | <0.001 |
| Creatinine (mg/dL) | 0.72 | ±0.28 | 0.69 | ±0.16 | 0.73 | ±0.32 | 0.74 | ±0.34 | 0.37 |
| eGFR (ml/min/1.73m2) | 117.43 | ±30.65 | 121.03 | ±28.94 | 116.23 | ±31.53 | 115.01 | ±31.37 | 0.32 |
| FPG (mg/dL) | 95.33 | ±21.96 | 85.065 | ±8.44 | 92.113 | ±12.37 | 108.77 | ±30.49 | <0.001 |
| HDL-C (mg/dL) | 54.96 | ±13.83 | 61.037 | ±14.67 | 54.472 | ±12.36 | 49.36 | ±11.84 | <0.001 |
| HOMA-IR index | 1.85 | ±1.36 | 0.80 | ±0.23 | 1.51 | ±0.23 | 3.24 | ±1.52 | <0.001 |
| LDL-C (mg/dL) | 120.20 | ±31.85 | 121.77 | ±34.23 | 124.78 | ±30.51 | 114.10 | ±29.96 | 0.04 |
| Triglyceride (mg/dL) | 123.37 | ±65.14 | 93.97 | ±41.90 | 119.44 | ±54.73 | 156.66 | ±77.71 | <0.001 |
| Uric Acid (mg/dL) | 5.71 | ±1.41 | 5.39 | ±1.30 | 5.71 | ±1.41 | 6.03 | ±1.45 | 0.003 |
| Framingham risk score (%) | 14.31 | ±11.47 | 10.95 | ±7.85 | 13.94 | ±10.21 | 18.04 | ±14.33 | <0.001 |
| Current smoking, n (%) | 35 | (10.9) | 13 | (12.1) | 10 | (9.4) | 12 | (11.2) | 0.81 |
| Alcohol drinking ≥ 2 times/week, n (%) | 62 | (19.4) | 26 | (24.3) | 21 | (19.8) | 15 | (14.0) | 0.16 |
| Regular exercise, n (%) | 259 | (80.9) | 92 | (86.0) | 87 | (82.1) | 80 | (74.8) | 0.11 |
| HTN, n (%) | 152 | (47.5) | 40 | (37.4) | 42 | (39.6) | 70 | (65.4) | <0.001 |
| DM, n (%) | 54 | (16.9) | 2 | (1.9) | 13 | (12.3) | 39 | (36.4) | <0.001 |
| Hyperlipidemia, n (%) | 211 | (65.9) | 60 | (56.1) | 70 | (66.0) | 81 | (75.7) | 0.01 |
| HOMA-IR Index (n = 320) | ||
|---|---|---|
| Variables | Pearson’s coefficient | p-value |
| Age (year) | 0.02 | 0.68 |
| SBP (mmHg) | 0.16 | 0.005 |
| DBP (mmHg) | 0.09 | 0.126 |
| BMI (kg/m2) | 0.46 | <0.001 |
| Framingham risk score (%) | 0.22 | <0.001 |
| Waist circumference (cm) | 0.45 | <0.001 |
| FPG (mg/dL) | 0.58 | <0.001 |
| HDL-C (mg/dL) | −0.32 | <0.001 |
| TG (mg/dL) | 0.34 | <0.001 |
| LDL-C (mg/dL) | −0.11 | 0.04 |
| Uric Acid (mg/dL) | 0.16 | 0.003 |
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | OR | (95% CI) | p-value | OR | (95% CI) | p-value | OR | (95% CI) | p-value | OR | (95% CI) | p-value |
| Low | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Middle | 2.71 | (1.29–5.69) | 0.009 | 5.16 | (2.12–12.57) | <0.001 | 5.66 | (2.17–14.78) | <0.001 | 11.31 | (2.94–43.52) | <0.001 |
| High | 3.69 | (1.79–7.62) | <0.001 | 9.67 | (3.83–24.37) | <0.001 | 9.01 | (3.14–25.81) | <0.001 | 11.51 | (2.55–51.94) | 0.001 |
| p-value for trend | <0.001 | <0.001 | <0.001 | 0.002 | ||||||||
| Variables | AUC (95% CI) | p value | Cut-off point | Sensitivity | Specificity |
|---|---|---|---|---|---|
| HOMA-IR index | 0.627 | 0.001 | 1.215 | 0.836 | 0.429 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, M.-C.; Fang, W.-C.; Li, W.-C.; Yeh, W.-C.; Shieh, Y.-H.; Chen, J.-Y. The Association between Insulin Resistance and Cardiovascular Disease Risk: A Community-Based Cross-Sectional Study among Taiwanese People Aged over 50 Years. Int. J. Environ. Res. Public Health 2020, 17, 7195. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197195
Lu M-C, Fang W-C, Li W-C, Yeh W-C, Shieh Y-H, Chen J-Y. The Association between Insulin Resistance and Cardiovascular Disease Risk: A Community-Based Cross-Sectional Study among Taiwanese People Aged over 50 Years. International Journal of Environmental Research and Public Health. 2020; 17(19):7195. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197195
Chicago/Turabian StyleLu, Mei-Chun, Wei-Ching Fang, Wen-Cheng Li, Wei-Chung Yeh, Ying-Hua Shieh, and Jau-Yuan Chen. 2020. "The Association between Insulin Resistance and Cardiovascular Disease Risk: A Community-Based Cross-Sectional Study among Taiwanese People Aged over 50 Years" International Journal of Environmental Research and Public Health 17, no. 19: 7195. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197195