A Comprehensive Approach Limiting Extractions under General Anesthesia Could Improve Oral Health


Abstract
:1. Introduction
2. Materials and Methods
2.1. Type of Study
2.2. A Comprehensive and Conservative Approach for Dental Treatments under GA
2.3. Study Population
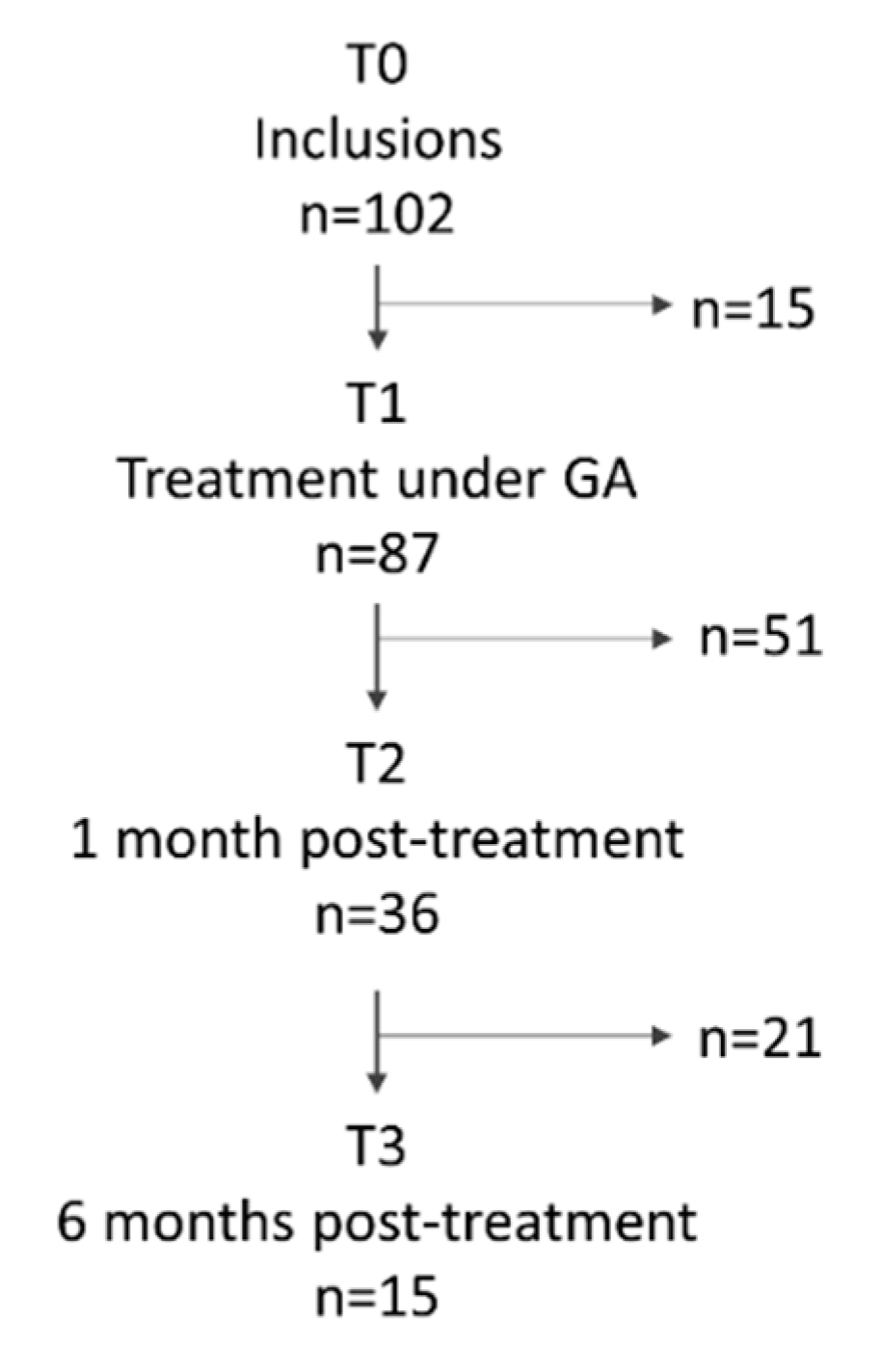
2.4. Experimental Procedure
2.5. Study Criteria
2.5.1. Dental Status
2.5.2. Dental Treatments
2.5.3. Oral Health-Related Quality of Life
2.5.4. Mastication Evaluation
2.6. Study Hypotheses
2.7. Sample Size Calculation
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Horner-Johnson, W.; Dobbertin, K.; Lee, J.C.; Andresen, E.M. Expert Panel on Disability and Health Disparities Disparities in health care access and receipt of preventive services by disability type: Analysis of the medical expenditure panel survey. Health Serv. Res. 2014, 49, 1980–1999. [Google Scholar] [CrossRef] [Green Version]
- Mahmoudi, E.; Meade, M.A. Disparities in access to health care among adults with physical disabilities: Analysis of a representative national sample for a ten-year period. Disabil. Health J. 2015, 8, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Hennequin, M.; Moysan, V.; Jourdan, D.; Dorin, M.; Nicolas, E. Inequalities in oral health for children with disabilities: A French national survey in special schools. PLoS ONE 2008, 3, e2564. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Clark, J.J. Tooth loss patterns in older adults with special needs: A Minnesota cohort. Int. J. Oral Sci. 2011, 3, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Anders, P.L.; Davis, E.L. Oral health of patients with intellectual disabilities: A systematic review. Spec. Care Dent. 2010, 30, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Kanaffa-Kilijanska, U.; Kaczmarek, U.; Kilijanska, B.; Frydecka, D. Oral health condition and hygiene habits among adult patients with respect to their level of dental anxiety. Oral Health Prev. Dent. 2014, 12, 233–239. [Google Scholar] [CrossRef]
- Brown, L.F.; Ford, P.J.; Symons, A.L. Periodontal disease and the special needs patient. Periodontol 2000 2017, 74, 182–193. [Google Scholar] [CrossRef]
- Farsi, D.J.; Farsi, N.J.; El-Housseiny, A.A.; Turkistani, J.M.; Farsi, N.M. Impact of Dental Rehabilitation on Oral Health-related Quality-of-life in Healthy Children and Those with Special Health Care Needs. J. Contemp. Dent. Pract. 2018, 19, 367–374. [Google Scholar] [CrossRef]
- Svensson, L.; Hakeberg, M.; Wide, U. Dental pain and oral health-related quality of life in individuals with severe dental anxiety. Acta Odontol. Scand. 2018, 76, 401–406. [Google Scholar] [CrossRef]
- Wong, A. Treatment planning considerations for adult oral rehabilitation cases in the operating room. Dent. Clin. N. Am. 2009, 53, 255–267. [Google Scholar] [CrossRef]
- Jockusch, J.; Sobotta, B.A.J.; Nitschke, I. Outpatient dental care for people with disabilities under general anaesthesia in Switzerland. BMC Oral Health 2020, 20, 225. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, H.; Baharvand, M.; Safi, Y. Death Rate of Dental Anaesthesia. J. Clin. Diagn. Res. 2017, 11, ZE07–ZE09. [Google Scholar] [CrossRef] [PubMed]
- Maestre, C. The use of general anaesthesia for tooth extraction in young handicapped adults in France. Br. Dent. J. 1996, 180, 297–302. [Google Scholar] [CrossRef]
- Gallagher, J.E.; Fiske, J. Special Care Dentistry: A professional challenge. Br. Dent. J. 2007, 202, 619–629. [Google Scholar] [CrossRef] [PubMed]
- Linas, N.; Faulks, D.; Hennequin, M.; Cousson, P.-Y. Conservative and endodontic treatment performed under general anesthesia: A discussion of protocols and outcomes. Spec. Care Dent. 2019, 39, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Linas, N.; Decerle, N.; Munoz-Sanchez, M.-L.; Faulks, D.; Collado, V.; Nicolas, E.; Hennequin, M.; Cousson, P.-Y. Long term outcomes of full pulpotomy in permanent molars for patients treated in a single, short session under special conditions. J. Endod. 2020. [Google Scholar] [CrossRef] [PubMed]
- Alsaleh, I.; Cousson, P.-Y.; Nicolas, E.; Hennequin, M. Is endodontic treatment performed under general anaesthesia technically acceptable? Clin. Oral Investig. 2012, 16, 1599–1606. [Google Scholar] [CrossRef] [PubMed]
- Eidelman, E.; Faibis, S.; Peretz, B. A comparison of restorations for children with early childhood caries treated under general anesthesia or conscious sedation. Pediatr. Dent. 2000, 22, 33–37. [Google Scholar]
- Jockusch, J.; Hopfenmüller, W.; Ettinger, R.; Nitschke, I. Outpatient, dental care of adult vulnerable patients under general anaesthesia-a retrospective evaluation of need for treatment and dental follow-up care. Clin. Oral Investig. 2020. [Google Scholar] [CrossRef]
- Mallineni, S.K.; Yiu, C.K.Y. A Retrospective Review of Outcomes of Dental Treatment Performed for Special Needs Patients under General Anaesthesia: 2-Year Follow-Up. Sci. World J. 2014, 2014, 748353. [Google Scholar] [CrossRef] [Green Version]
- Haute Autorité de Santé Indications et Contre-Indications de l’anésthésie Générale Pour les Actes Courants D’odontologie et de Stomatologie; Haute Autorité de Santé: Saint-Denis, France, 2005; p. 43.
- Société Française d’Anesthésie et de Réanimation Référentiel 2ème édition—1990–1994. L’anesthésie du Patient Ambulatoire. Available online: https://sfar.org/lanesthesie-du-patient-ambulatoire/ (accessed on 27 April 2020).
- Qaseem, A.; Snow, V.; Fitterman, N.; Hornbake, E.R.; Lawrence, V.A.; Smetana, G.W.; Weiss, K.; Owens, D.K.; Aronson, M.; Barry, P.; et al. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: A guideline from the American College of Physicians. Ann. Intern. Med. 2006, 144, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Smetana, G.W.; Lawrence, V.A.; Cornell, J.E. American College of Physicians Preoperative pulmonary risk stratification for noncardiothoracic surgery: Systematic review for the American College of Physicians. Ann. Intern. Med. 2006, 144, 581–595. [Google Scholar] [CrossRef] [PubMed]
- Orstavik, D.; Kerekes, K.; Eriksen, H.M. The periapical index: A scoring system for radiographic assessment of apical periodontitis. Endod Dent. Traumatol. 1986, 2, 20–34. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, K.R.; Kuzmina, I.; Bjørndal, L.; Thylstrup, A. Relationship between external and histologic features of progressive stages of caries in the occlusal fossa. Caries Res. 1995, 29, 243–250. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (Ed.) Oral Health Surveys: Basic Methods, 4th ed.; World Health Organization: Geneva, Switzerland, 1997; ISBN 978-92-4-154493-1. [Google Scholar]
- Armfield, J.M. How do we measure dental fear and what are we measuring anyway? Oral Health Prev. Dent. 2010, 8, 107–115. [Google Scholar]
- Tubert-Jeannin, S.; Riordan, P.J.; Morel-Papernot, A.; Porcheray, S.; Saby-Collet, S. Validation of an oral health quality of life index (GOHAI) in France. Commun. Dent. Oral Epidemiol. 2003, 31, 275–284. [Google Scholar] [CrossRef]
- Woda, A.; Nicolas, E.; Mishellany-Dutour, A.; Hennequin, M.; Mazille, M.-N.; Veyrune, J.-L.; Peyron, M.-A. The masticatory normative indicator. J. Dent. Res. 2010, 89, 281–285. [Google Scholar] [CrossRef]
- Woda, A.; Foster, K.; Mishellany, A.; Peyron, M.A. Adaptation of healthy mastication to factors pertaining to the individual or to the food. Physiol. Behav. 2006, 89, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Patton, L.L.; Kim, H.-Y. Impact of dental treatment under general anesthesia on the oral health-related quality of life of adolescents and adults with special needs. Eur. J. Oral Sci. 2014, 122, 363–371. [Google Scholar] [CrossRef]
- Hillebrecht, A.-L.; Hrasky, V.; Anten, C.; Wiegand, A. Changes in the oral health-related quality of life in adult patients with intellectual disabilities after dental treatment under general anesthesia. Clin. Oral Investig. 2019, 23, 3895–3903. [Google Scholar] [CrossRef]
- Fueki, K.; Yoshida, E.; Igarashi, Y. A structural equation model relating objective and subjective masticatory function and oral health-related quality of life in patients with removable partial dentures. J. Oral Rehabil. 2011, 38, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Pedroni-Pereira, A.; Marquezin, M.C.S.; Araujo, D.S.; Pereira, L.J.; Bommarito, S.; Castelo, P.M. Lack of agreement between objective and subjective measures in the evaluation of masticatory function: A preliminary study. Physiol. Behav. 2018, 184, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Bourdiol, P.; Hennequin, M.; Peyron, M.-A.; Woda, A. Masticatory Adaptation to Occlusal Changes. Front. Physiol. 2020, 11, 263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trulsson, M. Sensory and motor function of teeth and dental implants: A basis for osseoperception. Clin. Exp. Pharmacol. Physiol. 2005, 32, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Zanini, M.; Hennequin, M.; Cousson, P.-Y. A Review of Criteria for the Evaluation of Pulpotomy Outcomes in Mature Permanent Teeth. J. Endod. 2016, 42, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Cushley, S.; Duncan, H.F.; Lappin, M.J.; Tomson, P.L.; Lundy, F.T.; Cooper, P.; Clarke, M.; El Karim, I. Pulpotomy for mature carious teeth with symptoms of irreversible pulpitis: A systematic review. J. Dent. 2019, 88, 103158. [Google Scholar] [CrossRef]
- Randall, R.C. Preformed metal crowns for primary and permanent molar teeth: Review of the literature. Pediatr. Dent. 2002, 24, 489–500. [Google Scholar]
- Sigal, A.V.; Sigal, M.J.; Titley, K.C.; Andrews, P.B. Stainless steel crowns as a restoration for permanent posterior teeth in people with special needs: A retrospective study. J. Am. Dent. Assoc. 2020, 151, 136–144. [Google Scholar] [CrossRef]
- Lemmens, L.; Van Buggenhout, S.; Van Loey, A.M.; Hendrickx, M.E. Particle size reduction leading to cell wall rupture is more important for the beta-carotene bioaccessibility of raw compared to thermally processed carrots. J. Agric. Food Chem. 2010, 58, 12769–12776. [Google Scholar] [CrossRef]
- Pohjola, V.; Lahti, S.; Vehkalahti, M.M.; Tolvanen, M.; Hausen, H. Association between dental fear and dental attendance among adults in Finland. Acta. Odontol. Scand. 2007, 65, 224–230. [Google Scholar] [CrossRef]
- Goettems, M.L.; Schuch, H.S.; Demarco, F.F.; Ardenghi, T.M.; Torriani, D.D. Impact of dental anxiety and fear on dental care use in Brazilian women. J. Public Health Dent. 2014, 74, 310–316. [Google Scholar] [CrossRef] [PubMed]
- White, A.M.; Giblin, L.; Boyd, L.D. The Prevalence of Dental Anxiety in Dental Practice Settings. J. Dent. Hyg. 2017, 91, 30–34. [Google Scholar] [PubMed]
- Schneider, A.; Andrade, J.; Tanja-Dijkstra, K.; Moles, D.R. Mental imagery in dentistry: Phenomenology and role in dental anxiety. J. Anxiety Disord. 2018, 58, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Peyron, M.A.; Woda, A.; Bourdiol, P.; Hennequin, M. Age-related changes in mastication. J. Oral Rehabil. 2017, 44, 299–312. [Google Scholar] [CrossRef]
- Kankaala, T.; Määttä, T.; Tolvanen, M.; Lahti, S.; Anttonen, V. Outcome of Chair-Side Dental Fear Treatment: Long-Term Follow-Up in Public Health Setting. Int. J. Dent. 2019, 4, 5825067. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| General | |
|---|---|
| Operator: dental surgeon senior | |
| Operators | Assistant: dental surgeon junior or resident |
| Non-sterile operating aid: operating room nurse | |
| Suction | Surgical suction |
| Endodontic Treatments | |
| Isolation | Rubber dam with vinyl foils |
| Removal of carious dentin | Use of tungsten carbide bur |
| Preparation of access cavity | Use of Endo-Z® bur |
| Root canal treatment | |
| Indications | Visible apical lesion on the radiogram (PAI score >2 for at least one root) or pre-operative exposure of endocanal to saliva or lack of bleeding after per-operative pulp opening |
| Per operative radiography | Argentic and digital radiography with or without sensor holder |
| Work length determination | Per operative radiography or electronic measurement |
| Irrigation and disinfection | 2.5% Sodium hypochlorite solution; |
| Root canal preparation | Step down with manual files (Gates 4-3-2, lime K 15-20-25-30-35) or NiTi files (Protaper®, RevoS®, or Wave one®) |
| Drying | Sterile paper points |
| Root canal obturation | One gutta percha master point with zinc oxide eugenol sealer and thermomechanical compaction |
| Coronal restoration | Composite, GIC, bonded amalgams with GIC, Stainless Steel Crown depending on teeth and carious lesion extension |
| Full pulpotomy | |
| Indications | Absence of apical lesion on the radiogram (PAI score <2 for all roots) Bleeding after pulp opening |
| Coronal one third preparation | Gates Glidden burs (4-3) |
| Irrigation and disinfection | 2.5% Sodium hypochlorite solution |
| Hemostasis | Compression with sterile cotton pellet; Calcium hydroxide in cases of abundant bleeding |
| Pulp capping | Reinforced zinc oxide eugenol material (IRM®) |
| Pulp chamber obturation | High viscosity GIC (Fuji IX®) |
| Coronal restoration | Stainless Steel Crown for molars; bonded amalgams with GIC or composite based on GIC for premolars |
| Conservative treatments | |
| Incisor or canine | Composite resin |
| Bicuspid | With one or two marginal crest: GIC bonded Amalgam or Composite resin |
| Without marginal crest: Stainless Steel Crown, GIC bonded Amalgam or Composite resin | |
| After endodontic treatment: Stainless Steel Crown | |
| Molar | With one or two marginal crest: GIC bonded Amalgam |
| Without marginal crest or after pulpotomy or endodontic treatment: Stainless Steel Crown | |
| Cervical cavity | GIC bonded Amalgam or Composite resin |
| Extractions | |
| Indications | Periodontal disease with mobility Periodontal involvement of the furcation Extensive carious lesion with root and/or furcation involvement |
| Inclusion criteria |
|
| Exclusion criteria |
|
| G1–G2 (n = 66) | G2 (n = 36) | Student T-Test | G2–G3 (n = 21) | G3 (n = 15) | Student T-test | |
|---|---|---|---|---|---|---|
| Mean age (years) | 31.24 ± 10.44 | 28.29 ± 8.64 | NS | 28.37 ± 8.08 | 28.17 ± 9.66 | NS |
| Male-to-female ratio | 36/30 | 7/29 | p < 0.001 | 4/17 | 3/12 | NS |
| Carious index (DMFT) | ||||||
| Number of decayed teeth (D) | 14.19 ± 5.93 | 11.81 ± 5.47 | NS | 11.67 ± 5.50 | 12.00 ± 5.61 | NS |
| Number of missing teeth (M) | 3.49 ± 3.35 | 2.97 ± 2.43 | NS | 2.81 ± 2.11 | 3.20 ± 2.88 | NS |
| Number of filling teeth (F) | 2.07 ± 2.68 | 3.00 ± 4.11 | NS | 3.52 ± 4.72 | 2.27 ± 3.08 | NS |
| DMFT (teeth) | 18.77 ± 7.51 | 17.78 ± 5.76 | NS | 18.00 ± 5.99 | 17.47 ± 5.60 | NS |
| Number of posterior functional unit (PFU) | 4.63 ± 2.22 | 5.83 ± 2.29 | p = 0.012 | 5.81 ± 2.23 | 5.87 ± 2.47 | NS |
| Quality of life (GOHAI score) | ||||||
| Functional field (max: 20) | 14.28 ± 3.43 | 14.38 ± 3.76 | NS | 14.52 ± 4.25 | 14.47 ± 3.16 | NS |
| Psychosocial field (max: 25) | 13.39 ± 4.55 | 15.76 ± 5.34 | NS | 16.62 ± 5.201 | 14.60 ± 5.12 | NS |
| Pain or discomfort field (max: 15) | 7.19 ± 2.69 | 8.67 ± 2.95 | p = 0.013 | 8.81 ± 2.66 | 8.27 ± 3.35 | NS |
| Total (max: 60) | 34.86 ± 7.72 | 38.82 ± 10.36 | p = 0.022 | 39.95 ± 10.34 | 37.33 ± 10.11 | NS |
| Chewing parameters (raw carrot at swallowing time) | ||||||
| Number of chewing cycles | 48.23 ± 19.66 | 50.68 ± 47.21 | NS | 40.17 ± 19.80 | 62.58 ± 64.81 | NS |
| Chewing time (s) | 32.65 ± 14.64 | 35.08 ± 34.27 | NS | 27.55 ± 15.67 | 43.62 ± 46.61 | NS |
| Chewing frequency (cycles/s) | 1.50 ± 0.21 | 1.48 ± 0.23 | NS | 1.49 ± 0.27 | 1.47 ± 0.18 | NS |
| Bolus granulometry D50 (µm) | 8561 ± 2800 | 8294 ± 3045 | NS | 8957 ± 3221 | 7410 ± 2640 | NS |
| Chewing adaptation to food hardness parameters | ||||||
| Soft test food | ||||||
| Number of chewing cycles | 22.59 ± 14.01 | 22.23 ± 14.75 | NS | 20.58 ± 12.70 | 28.73 ± 21.86 | NS |
| Chewing time (s) | 19.08 ± 13.95 | 18.17 ± 12.56 | NS | 16.94 ± 10.73 | 23.33 ± 18.74 | NS |
| Chewing frequency (cycles/s) | 1.24 ± 0.24 | 1.25 ± 0.23 | NS | 1.23 ± 0.27 | 1.26 ± 0.16 | NS |
| Hard test food | ||||||
| Number of chewing cycles | 29.09 ± 13.06 | 30.63 ± 20.32 | NS | 29.33 ± 18.75 | 35.63 ± 23.39 | NS |
| Chewing time (s) | 24.29 ± 10.58 | 25.57 ± 17.71 | NS | 24.64 ± 16.43 | 29.17 ± 19.90 | NS |
| Chewing frequency (cycles/s) | 1.23 ± 0.21 | 1.22 ± 0.23 | NS | 1.21 ± 0.23 | 1.24 ± 0.21 | NS |
| Comparison of chewing frequency for hard/soft gelatins | NS | NS | NS | NS | ||
| GROUP 2 | T0 | T1 | Repeated Measured Process | ||
|---|---|---|---|---|---|
| F | PES | Significant | |||
| Carious index (DMFT) | |||||
| Number of patients (n) | 36 | 36 | |||
| Number of decayed teeth (D) | 11.81 ± 5.47 | 0.25 ± 0.91 | 181.52 | 0.84 | p < 0.001 |
| Number of missing teeth (M) | 2.97 ± 2.43 | 5.86 ± 3.27 | 39.90 | 0.53 | p < 0.001 |
| Number of filling teeth (F) | 3.00 ± 4.11 | 11.75 ± 5.07 | 124.17 | 0.79 | p < 0.001 |
| DMF (teeth) | 17.78 ± 5.76 | 17.86 ± 5.64 | 0.81 | 0.02 | NS |
| Number of Posterior Functional unit (PFU) | 5.83 ± 2.29 | 5.78 ± 2.27 | 0.70 | 0.004 | NS |
| Quality of life (GOHAI score) | |||||
| Number of patients (n) | 36 | 36 | |||
| Functional field (max: 20) | 14.38 ± 3.76 | 17.62 ± 2.76 | 28.92 | 0.47 | p < 0.001 |
| Psychosocial field (max: 25) | 15.76 ± 5.34 | 22.24 ± 3.67 | 72.22 | 0.69 | p < 0.001 |
| Pain or discomfort field (max: 15) | 8.67 ± 2.95 | 12.24 ± 2.23 | 47.31 | 0.59 | p < 0.001 |
| Total (max: 60) | 38.82 ± 10.36 | 52.09 ± 7.48 | 93.80 | 0.74 | p < 0.001 |
| Chewing parameters (raw carrot at swallowing time) | |||||
| Number of patients (n) | 35 (1 refusal) | 35 (1 refusal) | 35 | ||
| Number of chewing cycles | 50.68 ± 47.21 | 51.09 ± 54.54 | 2.04 | 0.07 | NS |
| Chewing time (s) | 35.08 ± 34.27 | 34.38 ± 42.19 | 0.58 | 0.02 | NS |
| Chewing frequency (cycles/s) | 1.48 ± 0.23 | 1.57 ± 0.25 | 10.17 | 0.26 | p = 0.003 |
| Bolus granulometry—D50 (µm) | 8294 ± 3045 | 7727 ± 2683 | 2.13 | 0.06 | NS |
| Chewing adaptation to food hardness parameters | |||||
| Number of patients (n) | 33 (3 refusal) | 33 (3 refusal) | 31 | ||
| Soft test food | |||||
| Number of chewing cycles | 24.29 ± 17.65 | 24.39 ± 22.75 | 1.31 | 0.04 | NS |
| Chewing time (s) | 19.85 ± 15.00 | 19.08 ± 18.62 | 0.50 | 0.02 | NS |
| Chewing frequency (cycles/s) | 1.25 ± 0.22 | 1.31 ± 0.23 | 1.88 | 0.06 | NS |
| Hard test food | |||||
| Number of chewing cycles | 32.20 ± 20.89 | 42.00 ± 37.23 | 9.74 | 0.25 | p = 0.004 |
| Chewing time (s) | 26.70 ± 17.94 | 33.44 ± 31.57 | 7.94 | 0.21 | p = 0.008 |
| Chewing frequency (cycles/s) | 1.22 ± 0.22 | 1.28 ± 0.23 | 4.02 | 0.12 | NS |
| Comparison of chewing frequency for hard/soft gelatins | NS F = 4,10 PES = 0.04 | NS F = 2.48 PES = 0.07 | |||
| Operating Time (min) | 115.5 ± 42.1 | ||||
| Treatments performed during: Tooth extraction | |||||
| Incisor or canine | 0.22 ± 0.48 | ||||
| Molar or premolar | 2.72 ± 3.05 | ||||
| Impacted or retained tooth | 0.12 ± 0.45 | ||||
| Total | 3.52 ± 3.19 | ||||
| Conservative treatments | |||||
| Composite restoration | 2.61 ± 3.72 | ||||
| Bonded amalgam restoration | 3.69 ± 2.66 | ||||
| Stainless steel crown | 0.39 ± 0.69 | ||||
| Glass ionomer cement restoration | 0.33 ± 1.53 | ||||
| Stainless steel crown and endodontic treatment | 0.65 ± 0.75 | ||||
| Bonded amalgam restoration and endodontic treatment | 0.12 ± 0.40 | ||||
| Composite restoration and endodontic treatment | 0.81 ± 1.37 | ||||
| Composite restoration with fiber post and endodontic treatment | 0.02 ± 0.15 | ||||
| Composite and pulpotomy | 0.12 ± 0.45 | ||||
| Bonded amalgam and pulpotomy | 0.12 ± 0.40 | ||||
| Stainless steel crown and pulpotomy | 0.67 ± 0.98 | ||||
| Ultrasonic scaling | 0.63 ± 0.49 | ||||
| GROUP 3 | T0 | T1 | T2 | Repeated Measured Process | ||
|---|---|---|---|---|---|---|
| F | PES | p | ||||
| Carious index (DMFT) | ||||||
| Number of patients (n) | 15 | 15 | 15 | |||
| Number of decayed teeth (D) | 12.00 ± 5.61 | 0 ± 0 | 0 ± 0 | 68.72 | 0.83 | p < 0.001 |
| Number of missing teeth (M) | 3.20 ± 2.88 | 5.60 ± 3.78 | 5.60 ± 3.78 | 7.68 | 0.35 | p = 0.002 |
| Number of filling teeth (F) | 2.27 ± 3.08 | 11.93 ± 4.43 | 11.93 ± 4.43 | 48.90 | 0.78 | p < 0.001 |
| DMF (teeth) | 17.47 ± 5.60 | 17.53 ± 5.33 | 17.53 ± 5.33 | 0.13 | 0.01 | NS |
| Number of posterior functional unit (PFU) | 5.87 ± 2.47 | 5.60 ± 2.32 | 6.21 ± 2.01 | 1.11 | 0.07 | NS |
| Quality of life (GOHAI score) | ||||||
| Number of patients (n) | 15 | 15 | 15 | |||
| Functional field (max: 20) | 14.47 ± 3.16 | 17.46 ± 2.47 | 18.88 ± 2.10 | 10.56 | 0.43 | p < 0.001 |
| Psychosocial field (max: 25) | 14.60 ± 5.12 | 21.85 ± 4.18 | 21.63 ± 5.07 | 18.96 | 0.58 | p < 0.001 |
| Pain or discomfort field (max: 15) | 8.27 ± 3.35 | 11.69 ± 2.50 | 13.00 ± 2.45 | 9.98 | 0.42 | p = 0.001 |
| Total (max: 60) | 37.33 ± 10.11 | 51.00 ± 7.44 | 53.50 ± 9.17 | 19.70 | 0.59 | p < 0.001 |
| Chewing parameters (raw carrot at swallowing time) | ||||||
| Number of patients (n) | 15 | 15 | 15 | |||
| Number of chewing cycles | 62.58 ± 64.81 | 63.85 ± 75.34 | 57.93 ± 38.64 | 0.61 | 0.05 | NS |
| Chewing time (s) | 43.62 ± 46.61 | 43.15 ± 58.41 | 39.67 ± 35.78 | 1.1 | 0.17 | NS |
| Chewing frequency (cycles/s) | 1.47 ± 0.18 | 1.59 ± 0.21 | 1.59 ± 0.25 | 5.66 | 0.32 | p = 0.01 |
| Bolus granulometry—D50 (µm) | 7410 ± 2634 | 6587 ± 1779 | 6276 ± 2126 | 4.01 | 0.22 | NS |
| Chewing adaptation to food hardness parameters | ||||||
| Number of patients (n) | 15 | 13 (2 refusals) | 15 | |||
| Soft test food | ||||||
| Number of chewing cycles | 28.73 ± 21.86 | 28.81 ± 29.94 | 36.77 ± 54.53 | 0.60 | 0.10 | NS |
| Chewing time (s) | 23.33 ± 18.74 | 22.27 ± 24.36 | 30.10 ± 50.02 | 1.06 | 0.08 | NS |
| Chewing frequency (cycles/s) | 1.26 ± 0.16 | 1.34 ± 0.21 | 1.32 ± 0.20 | 2.61 | 0.18 | NS |
| Hard test food | ||||||
| Number of chewing cycles | 35.63 ± 23.99 | 51.58 ± 47.30 | 45.90 ± 24.60 | 4.21 | 0.26 | NS |
| Chewing time (s) | 29.17 ± 19.90 | 39.85 ± 37.91 | 36.53 ± 23.74 | 4.14 | 0.26 | NS |
| Chewing frequency (cycles/s) | 1.24 ± 0.21 | 1.33 ± 0.21 | 1.31 ± 0.24 | 3.01 | 0.20 | NS |
| Comparison of chewing frequency for hard/soft gelatins | NS | NS | NS | |||
| Operating Time (min) | 123.3 ± 36.9 | |||||
| Treatments performed during the procedure Tooth extraction | ||||||
| Incisor or canine | 0.2 ± 0.41 | |||||
| Molar or bicuspid | 2.3 ± 3.62 | |||||
| Impacted or retained tooth | 0.13 ± 0.52 | |||||
| Total | 2.67 ± 3.77 | |||||
| Conservative treatments | ||||||
| Composite restoration | 3.87 ± 5.11 | |||||
| Bonded amalgam restoration | 3.47 ± 2.33 | |||||
| Stainless steel crown | 0.20 ± 0.56 | |||||
| Glass ionomer cement restoration | 0.07 ± 0.26 | |||||
| Stainless steel crown and endodontic treatment | 0.47 ± 0.52 | |||||
| Bonded amalgam restoration and endodontic treatment | 0.20 ± 0.41 | |||||
| Composite restoration and endodontic treatment | 0.60 ± 0.74 | |||||
| Composite restoration with fiber post and endodontic treatment | 0 | |||||
| Composite and pulpotomy | 0 | |||||
| Bonded amalgam and pulpotomy | 0.07 ± 0.26 | |||||
| Stainless steel crown and pulpotomy | 1.00 ± 1.13 | |||||
| Ultrasonic scaling | 0.53 ± 0.52 | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Decerle, N.; Cousson, P.-Y.; Nicolas, E.; Hennequin, M. A Comprehensive Approach Limiting Extractions under General Anesthesia Could Improve Oral Health. Int. J. Environ. Res. Public Health 2020, 17, 7336. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197336
Decerle N, Cousson P-Y, Nicolas E, Hennequin M. A Comprehensive Approach Limiting Extractions under General Anesthesia Could Improve Oral Health. International Journal of Environmental Research and Public Health. 2020; 17(19):7336. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197336
Chicago/Turabian StyleDecerle, Nicolas, Pierre-Yves Cousson, Emmanuel Nicolas, and Martine Hennequin. 2020. "A Comprehensive Approach Limiting Extractions under General Anesthesia Could Improve Oral Health" International Journal of Environmental Research and Public Health 17, no. 19: 7336. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197336