The Effect of Psychological First Aid Training on Knowledge and Understanding about Psychosocial Support Principles: A Cluster-Randomized Controlled Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
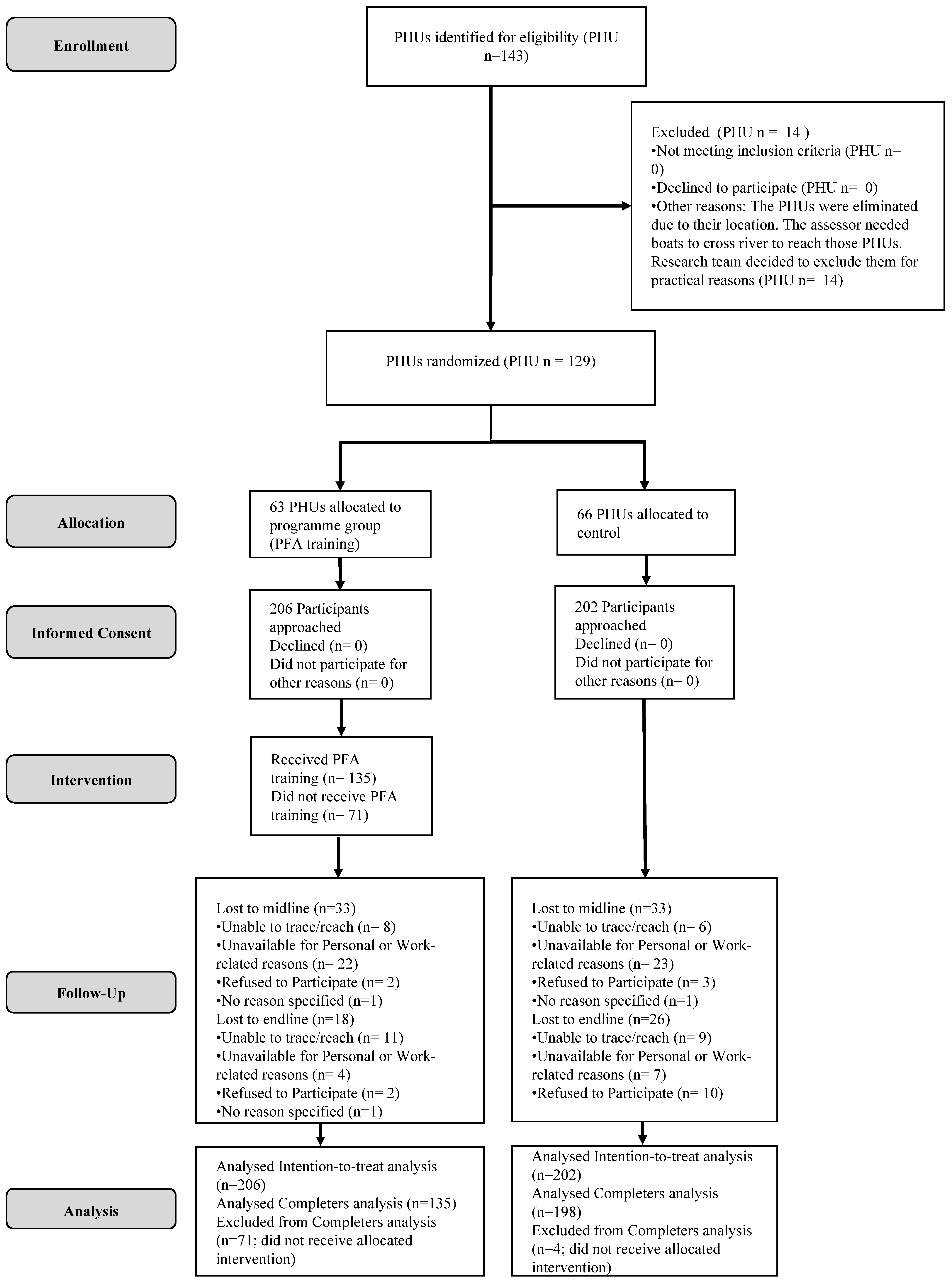
2.1. Participants and Procedures
2.2. Measures
2.3. PFA Training
2.4. Analyses
3. Results
3.1. Participants
3.2. Main Outcomes
3.3. Secondary Outcomes: Confidence, Professional Attitude and Professional Quality of Life
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ruzek, J.I.; Brymer, M.J.; Jacobs, A.K.; Layne, C.M.; Vernberg, E.M.; Watson, P.J. Psychological First Aid. J. Ment. Health Couns. 2007, 29, 17–49. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Psychological First Aid: Facilitator’s Manual for Orienting Field Workers; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. Psychological First Aid, Guide for Field Workers; WHO, War Trauma Foundation and World Vision International: Geneva, Switzerland, 2011. [Google Scholar]
- Sijbrandij, M.; Olff, M.; Reitsma, J.B.; Carlier, I.V.E.; Gersons, B.P.R. Emotional or educational debriefing after psychological trauma. Br. J. Psychiatry 2006, 189, 150–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, S.; Bisson, J.; Churchill, R.; Wessely, S. Psychological debriefing for preventing post traumatic stress disorder (PTSD). Cochrane Database Syst. Rev. 2002. [Google Scholar] [CrossRef] [PubMed]
- Inter-Agency Standing Committee (IASC)-A.S.C. IASC Guidelines on Mental Health and Psychosocial Support in Emergency Settings; IASC: Geneva, Switzerland, 2007. [Google Scholar]
- Bisson, J.I.; Lewis, C. Systematic Review of Psychological First Aid; Commissioned by the World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Hobfoll, S.E.; Watson, P.; Bell, C.C.; Bryant, R.A.; Brymer, M.J.; Friedman, M.J.; Friedman, M.; Gersons, B.P.; de Jong, J.T.; Layne, C.M.; et al. Five essential elements of immediate and mid-term mass trauma intervention: Empirical evidence. Psychiatry 2007, 70, 283–315. [Google Scholar] [CrossRef] [PubMed]
- Allen, B.; Brymer, M.J.; Steinberg, A.M.; Vernberg, E.M.; Jacobs, A.; Speier, A.H.; Pynoos, R.S. Perceptions of psychological first aid among providers responding to Hurricanes Gustav and Ike. J. Trauma. Stress 2010, 23, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.; Wurie, A.; Baingana, F.; Sevalie, S.; Beynon, F. Mental health nurses and disaster response in Sierra Leone. Lancet Glob. Health 2018, 6, e146–e147. [Google Scholar] [CrossRef] [Green Version]
- McCabe, O.L.; Everly, G.S., Jr.; Brown, L.M.; Wendelboe, A.M.; Abd Hamid, N.H.; Tallchief, V.L.; Links, J.M. Psychological first aid: A consensus-derived, empirically supported, competency-based training model. Am. J. Public Health 2014, 104, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Forbes, D.; Lewis, V.; Varker, T.; Phelps, A.; O’Donnell, M.; Wade, D.J.; Ruzek, J.I.; Watson, P.; Bryant, R.A.; Creamer, M. Psychological first aid following trauma: Implementation and evaluation framework for high-risk organizations. Psychiatry 2011, 74, 224–239. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; You, S.; Choi, Y.K.; Youn, H.Y.; Shin, H.S. A preliminary evaluation of the training effects of a didactic and simulation-based psychological first aid program in students and school counselors in South Korea. PLoS ONE 2017, 12, e0181271. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ebola Virus Disease. Key Facts. Available online: http://www.who.int/news-room/fact-sheets/detail/ebola-virus-disease (accessed on 27 July 2019).
- Horn, R.; O’May, F.; Esliker, R.; Gwaikolo, W.; Woensdregt, L.; Ruttenberg, L.; Ager, A. The myth of the 1-day training: The effectiveness of psychosocial support capacity-building during the Ebola outbreak in West Africa. Glob. Ment. Health 2019, 6, e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stamm, B.H. The Concise ProQOL Manual, 2nd ed.; ProQOL.org: Pocatello, ID, USA, 2010. [Google Scholar]
- Hunsaker, S.; Chen, H.C.; Maughan, D.; Heaston, S. Factors that influence the development of compassion fatigue, burnout, and compassion satisfaction in emergency department nurses. J. Nurs. Scholarsh. 2015, 47, 186–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasan, S.; Gohil, P.; Cornelius, V.; Taylor, C. Prevalence, causes and consequences of compassion satisfaction and compassion fatigue in emergency care: A mixed-methods study of UK NHS Consultants. Emerg. Med. J. 2015, 32, 588–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dieltjens, T.; Moonens, I.; Van Praet, K.; De Buck, E.; Vandekerckhove, P. A systematic literature search on psychological first aid: Lack of evidence to develop guidelines. PLoS ONE 2014, 9, e114714. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P. Examining the effects of prevention programs on the incidence of new cases of mental disorders: The lack of statistical power. Am. J. Psychiatry 2003, 160, 1385–1391. [Google Scholar] [CrossRef] [PubMed]
- Fox, J.H.; Burkle, F.M., Jr.; Bass, J.; Pia, F.A.; Epstein, J.L.; Markenson, D. The effectiveness of psychological first aid as a disaster intervention tool: Research analysis of peer-reviewed literature from 1990–2010. Disaster Med. Public Health Prep. 2012, 6, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Gilbody, S.; Whitty, P.; Grimshaw, J.; Thomas, R. Educational and organizational interventions to improve the management of depression in primary care: A systematic review. JAMA 2003, 289, 3145–3151. [Google Scholar] [CrossRef] [PubMed]
- Jonker, I.E.; Sijbrandij, M.; van Luijtelaar, M.J.; Cuijpers, P.; Wolf, J.R. The effectiveness of interventions during and after residence in women’s shelters: A meta-analysis. Eur. J. Public Health 2015, 25, 15–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, W.; Gevonden, M.; Shalev, A. Prevention of Post-Traumatic Stress Disorder after Trauma: Current Evidence and Future Directions. Curr. Psychiatry Rep. 2016, 18, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| PFA (n = 202) | Control (n = 206) | ||||
|---|---|---|---|---|---|
| Characteristic | Mean (SD) | Mean (SD) | t | df | p |
| Age (mean, SD) | 39.5 (9.26) | 38.5 (9.0) | 1.14 | 404 | 0.25 |
| Work experience in years (mean, SD) | 7.18 (6.38) | 7.88 (7.48) | −1.006 | 403 | 0.32 |
| n(%) | n(%) | Χ2 | df | p | |
| Gender 1 | 3.30 | 1 | 0.07 | ||
| Female | 165 (80.5) | 176 (87.1) | |||
| Male | 40 (19.5) | 26 (12.9) | |||
| Religion 2 | 0.72 | 1 | 0.40 | ||
| Christian | 117 (57.9) | 108 (53.7) | |||
| Muslim | 85 (42.1) | 93 (46.3) | |||
| Education | 1.76 | 5 | 0.88 | ||
| Junior Secondary School | 2 (1) | 2 (1) | |||
| Senior School | 28 (13.6) | 34 (16.8) | |||
| Certificate | 154 (74.8) | 148 (73.3) | |||
| Diploma | 19 (9.2) | 14 (6.9) | |||
| Undergraduate/Graduate | 3 (1.5) | 4 (2) | |||
| Profession | 5.09 | 4 | 0.28 | ||
| Nurse | 73 (35.4) | 89 (44.1) | |||
| Community Health Worker | 20 (9.7) | 12 (5.9) | |||
| Midwife | 15 (7.3) | 16 (7.9) | |||
| Maternal health assistant | 80 (38.8) | 73 (36.1) | |||
| Other (vaccinator, lab assistant, etc.) | 18 (8.7) | 12 (5.9) | |||
| Direct contact with people in distress | 0.34 | 1 | 0.56 | ||
| Yes | 200 (97.1) | 194 (96.0) | |||
| No | 6 (2.9) | 8 (4.0) |
| Descriptive Statistics Mean (SD) | Cohen’s d | Mixed Model Analysis * | ||||
|---|---|---|---|---|---|---|
| Outcomes | Time Point | PFA (n = 135) | Control (n = 198) | Difference in LS Mean (95% CI) | p-Value | |
| Knowledge retention score | Baseline | 12.18 (3.40) | 12.17 (3.05) | |||
| Post-assessment | 14.08 (3.53) | 12.34 (3.26) | 0.50 | 1.73 (0.98–2.47) | <.0001 | |
| Follow-up | 14.17 (3.34) | 12.60 (3.39) | 0.43 | 1.54 (0.76–2.33) | 0.0001 | |
| Scenario score | Baseline | 2.92 (1.39) | 2.80 (1.31) | |||
| Post-assessment | 3.36 (1.52) | 3.16 (1.38) | 0.04 | 0.19 (−0.14–0.51) | 0.26 | |
| Follow-up | 3.60 (1.38) | 2.98 (1.38) | 0.38 | 0.65 (0.31–0.98) | 0.0002 | |
| Professional attitude | Baseline | 30.66 (5.55) | 30.58 (5.28) | |||
| Post-assessment | 31.20 (4.58) | 30.58 (5.28) | 0.14 | 0.78 (−0.36–1.92) | 0.19 | |
| Follow-up | 31.57 (4.84) | 30.35 (5.32) | 0.23 | 1.26 (0.09–2.42) | 0.04 | |
| Confidence | Baseline | 19.42 (4.38) | 19.09 (4.45) | |||
| Post-assessment | 20.25 (4.45) | 19.34 (4.03) | 0.10 | 0.76 (−0.21–1.73) | 0.13 | |
| Follow-up | 19.56 (4.22) | 19.20 (4.15) | 0.01 | 0.29 (−0.65–1.24) | 0.54 | |
| Professional quality of life | Baseline | 37.07 (5.73) | 36.36 (5.69) | |||
| Post-assessment | 36.87 (5.52) | 36.30 (5.51) | 0.12 | 0.07 (−1.21–1.35) | 0.91 | |
| Follow-up | 36.79 (6.10) | 36.58 (5.52) | 0.03 | 0.51 (−0.81–1.83) | 0.45 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sijbrandij, M.; Horn, R.; Esliker, R.; O’May, F.; Reiffers, R.; Ruttenberg, L.; Stam, K.; de Jong, J.; Ager, A. The Effect of Psychological First Aid Training on Knowledge and Understanding about Psychosocial Support Principles: A Cluster-Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 484. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020484
Sijbrandij M, Horn R, Esliker R, O’May F, Reiffers R, Ruttenberg L, Stam K, de Jong J, Ager A. The Effect of Psychological First Aid Training on Knowledge and Understanding about Psychosocial Support Principles: A Cluster-Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(2):484. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020484
Chicago/Turabian StyleSijbrandij, Marit, Rebecca Horn, Rebecca Esliker, Fiona O’May, Relinde Reiffers, Leontien Ruttenberg, Kimberly Stam, Joop de Jong, and Alastair Ager. 2020. "The Effect of Psychological First Aid Training on Knowledge and Understanding about Psychosocial Support Principles: A Cluster-Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 2: 484. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020484