Variability of Lower Limb Artery Systolic–Diastolic Velocities in Futsal Athletes and Non-Athletes: Evaluation by Arterial Doppler Ultrasound

 , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedures
2.4. Statistical Analysis
2.4.1. Preliminary Analysis
2.4.2. Main Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Laughlin, M.; Newcomer, S.; Bender, S. Importance of hemodynamic forces as signals for exercise-induced changes in endothelial cell phenotype. J. Appl. Physiol. 2008, 104, 588–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, D.; Spence, A.; Halliwill, J.; Cable, N.; Thijssen, D. Exercise and vascular adaptation in humans. Exp. Physiol. 2011, 96, 57–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, D. Exercise training as vascular medicine: Direct impacts on the vasculature in humans. Exerc. Sport Sci. Rev. 2009, 37, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Spence, A.; Carter, H.; Naylor, L.; Green, D. A prospective randomized longitudinal study involving 6 months of endurance or resistance exercise. Conduit arteryadaptation in humans. J. Physiol. 2013, 591, 1265–1275. [Google Scholar] [CrossRef] [PubMed]
- Fischer, G.; Llaurado, J. Collagen and elastin content in canine arteries selected from functionally different vascular beds. Circ. Res. 1966, 19, 394–399. [Google Scholar] [CrossRef] [Green Version]
- McVeigh, G.; Bank, A.; Cohn, J. Arterial Compliance. In Cardiovascular Medicine, 2nd ed.; Willerson, J.T., Cohn, J., Eds.; Churchill Livingstone: Philadelphia, PA, USA, 2000. [Google Scholar]
- Aguiar, R.; Raimundo, J.; Lisbôa, F.; Salvador, A.; Pereira, K.; Cruz, R.; Turnes, T.; Caputo, F. Influence of aerobic and anaerobic variables on repeated sprint tests. Revista Brasileira de Educação Física e Esporte 2016, 30, 3. [Google Scholar] [CrossRef] [Green Version]
- Gotshall, R.; Gootman, J.; Byrnes, W.; Fleck, S.; Valovich, T. Noninvasive characterization of the blood pressure response to the double-leg press exercise. J. Exerc. Physiol. 1999, 2, 4. [Google Scholar] [CrossRef] [Green Version]
- Crawford, M.; DiMarco, J.; Paulus, W. Cardiology, 3rd ed.; Mosby Elsevier: Philadelphia, PA, USA, 2009. [Google Scholar]
- Schep, G.; Bender, M.; Schmikli, S.; Wijn, P. Color Doppler used to detect kinking and intravascular lesions in the iliac arteries in endurance athletes with claudication. Eur. J. Ultrasound. 2001, 14, 129–140. [Google Scholar] [CrossRef]
- Schep, G.; Bender, M.; Schmikli, S.; Mosterd, W.; Hammacher, E.; Scheltinga, M.; Wijn, P. Recognising vascular causes of leg complaints in endurance athletes. Part 2: The value of patient history, physical examination, cycling exercise test and echo-Doppler examination. Int. J. Sports Med. 2002, 23, 322–328. [Google Scholar] [CrossRef]
- Tschakovsky, M.; Saunders, N.; Webb, K.; O’Donnell, D. Muscle Blood-Flow Dynamics at Exercise Onset: Do The Limbs Differ? Med. Sci. Sports Exerc. 2006, 38, 1811–1818. [Google Scholar] [CrossRef] [Green Version]
- Holland, C.; Brown, J.; Scoutt, L.; Taylor, K. Lower extremity volumetric arterial blood flow in normal subjects. Ultrasound Med. Biol. 1998, 24, 1079–1086. [Google Scholar] [CrossRef]
- Laughlin, M.; Roseguini, B. Mechanisms for exercise training– induced increases in skeletal muscle blood flow capacity: Differences with interval sprint training versus aerobic endurance training. J. Physiol. Pharmacol. 2008, 59, S71–S88. [Google Scholar]
- Stebbings, G.; Morse, C.; McMahon, G.; Onambele, G. Resting arterial diameter and blood flow changes with resistance training and detraining in healthy young individuals. J. Athl. Train. 2013, 48, 209–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Splinter, R. Handbook of Physics in Medicine and Biology; CRC Press, Taylor & Francis: Boca Raton, FL, USA, 2010. [Google Scholar]
- Cotterill, R. Biophysics. An Introduction; John Wiley & Sons Inc.: Chichester, UK, 2008. [Google Scholar]
- Hwang, J. Doppler ultrasonography of the lower extremity arteries: Anatomy and scanning guidelines. Review article. Ultrasonography 2017, 36, 111–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peach, G.; Schep, G.; Palfreeman, R.; Beard, J.; Thompson, M.; Hinchiliffe, R. Endofibrosis and kinking of the iliac arteries in athletes: A systematic review. Eur. J. Vasc. Endovasc. Surg. 2012, 43, 208–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baecke, J.; Burema, J.; Frijters, J. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am. J. Clin. Nutr. 1982, 36, 936–942. [Google Scholar] [CrossRef]
- Vaughan, R.; Madigan, D.; Carter, G.; Nicholls, A. The Dark Triad in male and female athletes and non-athletes: Group differences and psychometric properties of the Short Dark Triad (SD3). Psychol. Sport Exerc. 2019, 43, 64–72. [Google Scholar] [CrossRef]
- World Medical Association. Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. WMJ 2008, 54, 122–125. [Google Scholar]
- Hirsch, A.; Haskal, Z.; Hertzer, N.; Bakal, C.; Creager, M.; Halperin, J.; Hiratzka, L.; Murphy, W.R.; Olin, J.; Puschett, J.; et al. ACC/AHA 2005 Practice Guidelines for the Management of Patients with Peripheral Arterial Disease (Lower Extremity, Renal, Mesenteric, and Abdominal Aortic). Circulation 2006, 113, e463–e465. [Google Scholar] [CrossRef] [Green Version]
- Gerhard-herman, M.; Gornik, H.; Barrett, C.; Barshes, N.; Corriere, M.; Drachman, D.; Fleisher, L.; Fowkes, F.; Hamburg, N.; Kinlay, S.; et al. AHA/ACC Guideline on the Management of Patients with Lower Extremity Peripheral Artery Disease: Executive Summary: A report of the american college of cardiology/American Heart Association task force on clinical practice guidelines. Circulation 2017, 135, 692. [Google Scholar] [CrossRef]
- George, M. Eco Doppler Arterial dos Membros Inferiores: Indicações Clínicas e Metodologia de Execução. Norma I da Direção Geral da Saúde. 2015, pp. 1–13. Available online: https://www.dgs.pt/directrizes-da-dgs/normas-e-circulares-normativas/norma-n-0342011-de-30092011-jpg.aspx (accessed on 26 June 2019).
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.; Babin, B.; Anderson, R.; Black, W. Multivariate Data Analysis, 8th ed.; Pearson Educational: Hoboken, NJ, USA, 2019. [Google Scholar]
- Hopkins, W.; Marshall, S.; Batterham, A.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, R. Handbook of Univariate and Multivariate Data Analysis with IBM SPSS, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar]
- Maiorana, A.; O’Driscoll, G.; Taylor, R.; Green, D. Exercise and the nitric oxide vasodilator system. Sports Med. 2003, 33, 1013–1035. [Google Scholar] [CrossRef] [PubMed]
- Prior, B.; Lloyd, P.; Yang, H.; Terjung, R. Exercise-induced vascular remodeling. Exerc. Sport Sci. Rev. 2003, 31, 26–33. [Google Scholar] [CrossRef]
- Hussain, S.; Smith, R.; Wood, R.; Bland, M. Observer variability in volumetric blood flow measurements in leg arteries using duplex ultrasound. Ultrasound Med. Biol. 1996, 3, 287–291. [Google Scholar] [CrossRef]
- Green, D.; Smith, K. Effects of Exercise on Vascular Function, Structure, and Health in Humans. Cold Spring Harb Perspect. Med. 2017, 8, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Rowley, N.; Dawson, E.; Hopman, M.; Gerorge, K.; Whyte, G.; Thijssen, D.; Green, D.J. Conduit Diameter and Wall Remodeling in Elite Athletes and Spinal Cord Injury. Med. Sci. Sports Exerc. 2012, 44, 844–849. [Google Scholar] [CrossRef]
- Sylvia, L.; Bernstein, E.; Hubbard, J.; Keating, L.; Anderson, E. Practical guide to measuring physical activity. J. Acad. Nutr. Diet. 2014, 114, 199–208. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Groups | N | M | SD | p | η2 | Effect Size | 90% CI | ICC (IC 95%) | CoV |
|---|---|---|---|---|---|---|---|---|---|---|
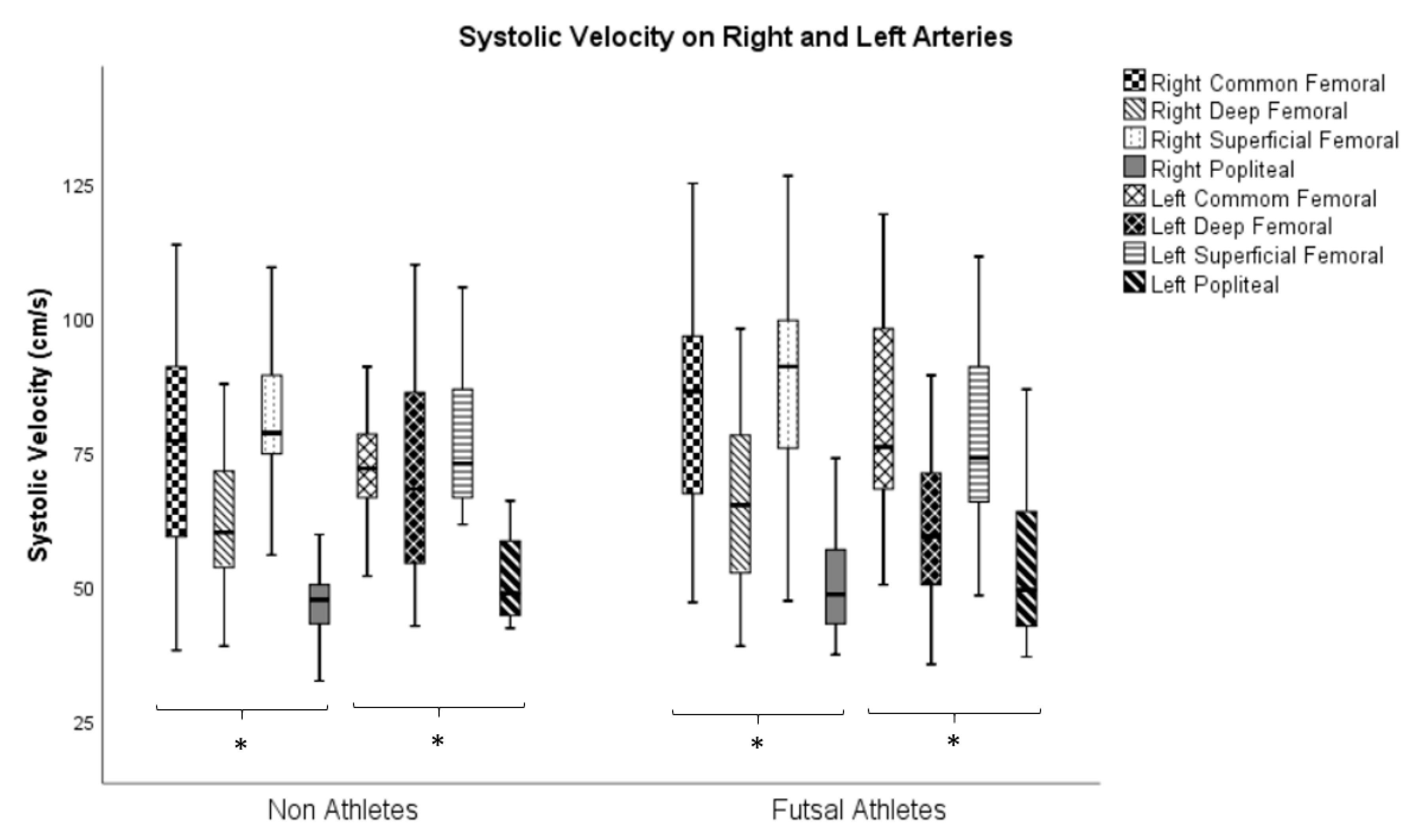
| systolic velocity—right common femoral artery | futsal athletes | 38 | 84.86 | 21.68 | 0.089 b | −0.396 | −0.935–0.143 | 1 (0.999–1) | 0.1% | |
| non-athletes | 38 | 76.35 | 21.33 | Small | 0.963 (0.938–0.980) | 1.7% | ||||
| systolic velocity—left common femoral artery | futsal athletes | 38 | 83.27 | 22.20 | 0.068 a | 0.044 | −0.428 | 1 (0.999–1) | 0.1% | |
| non-athletes | 38 | 73.99 | 17.88 | Small | 0.974 (0.957–0.986) | 1% | ||||
| systolic velocity—right deep femoral artery | futsal athletes | 38 | 66.23 | 15.12 | 0.274 b | −0.253 | −0.789–0.283 | 1 (0.999–1) | 0.1% | |
| non-athletes | 38 | 62.68 | 12.87 | Small | 1 (0.999–1) | 0.1% | ||||
| systolic velocity—left deep femoral artery | futsal athletes | 38 | 60.61 | 13.88 | 0.022 a,* | 0.069 | 0.546 | 1 (0.999–1) | 0.2% | |
| non-athletes | 38 | 72.14 | 20.75 | Small | 1 (0.999–1) | 0.2% | ||||
| systolic velocity—right superficial femoral artery | futsal athletes | 38 | 90.13 | 19.63 | 0.028 b,* | −0.515 | −1.057–0.028 | 1 (0.999–1) | 0.1% | |
| non-athletes | 38 | 81.43 | 13.63 | Small | 1 (0.999–1) | 0.1% | ||||
| systolic velocity—left superficial femoral artery | futsal athletes | 38 | 77.78 | 15.73 | 0.693 a | 0.002 | −0.091 | 1 (0.999–1) | 0.1% | |
| non-athletes | 38 | 76.38 | 12.13 | Trivial | 1 (0.999–1) | 0.1% | ||||
| systolic velocity—right popliteal artery | futsal athletes | 38 | 51.39 | 11.00 | 0.257 a | 0.017 | −0.262 | 1(0.999–1) | 0.2% | |
| non-athletes | 38 | 47.38 | 10.33 | Small | 1 (0.999–1) | 0.2% | ||||
| systolic velocity—left popliteal artery | futsal athletes | 38 | 54.45 | 14.08 | 0.975 a | 0.000 | −0.007 | 1 (0.999–1) | 0.1% | |
| non-athletes | 38 | 53.04 | 11.09 | Trivial | 1 (0.999–1) | 0.1% | ||||
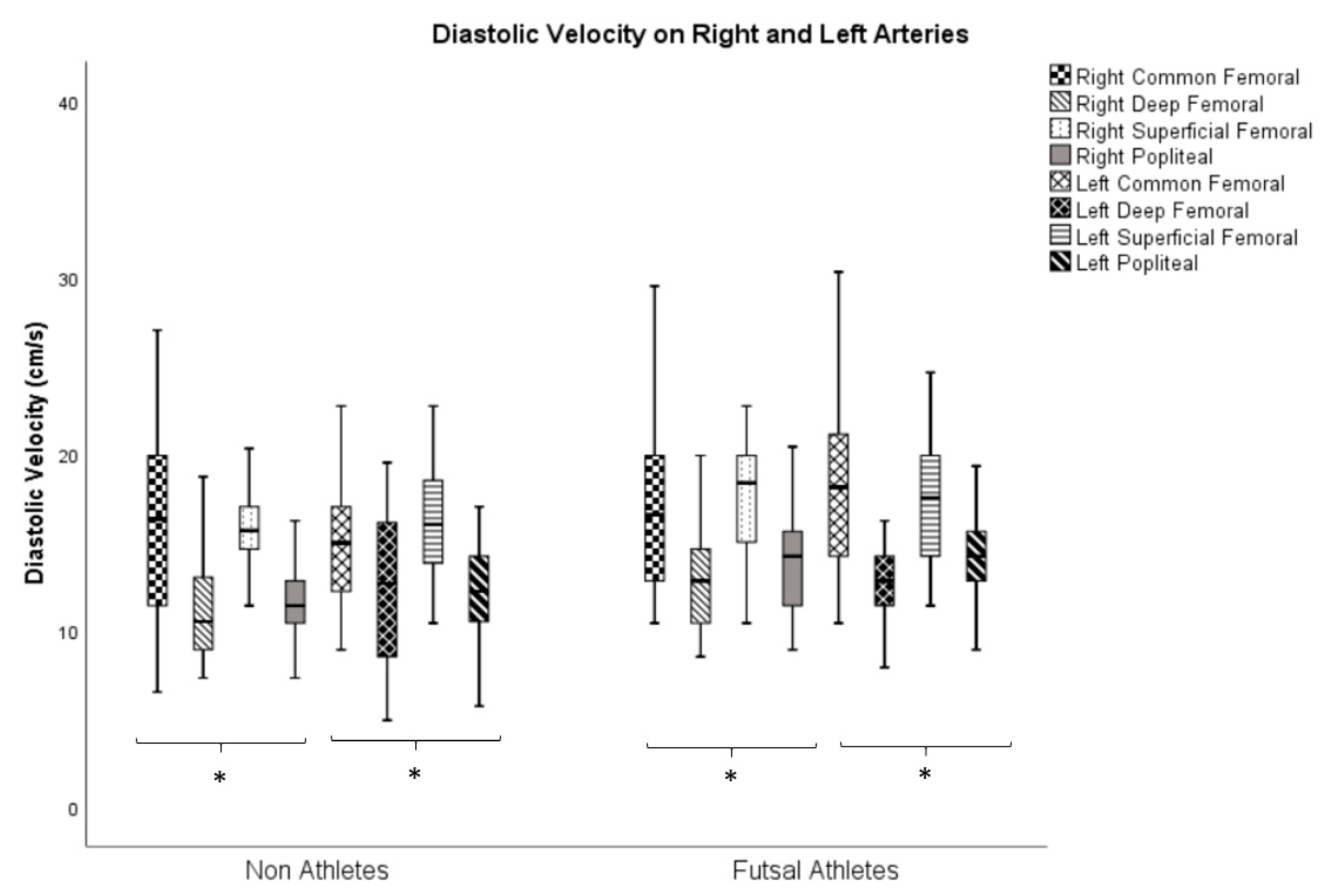
| diastolic velocity—right common femoral artery | futsal athletes | 38 | 17.18 | 5.17 | 0.533 a | 0.005 | −0.143 | 1 (0.999–1) | 0.9% | |
| non-athletes | 38 | 16.03 | 5.90 | Tivial | 0.996 (0.993–0.998) | 0.7% | ||||
| diastolic velocity—left common femoral artery | futsal athletes | 38 | 18.56 | 5.09 | 0.002 a,* | 0.123 | −0.748 | 1 (0.999–1) | 0.6% | |
| non-athletes | 38 | 15.19 | 4.00 | Moderate | 0.999 (0.998–0.999) | 0.9% | ||||
| diastolic velocity—right deep femoral artery | futsal athletes | 38 | 12.95 | 2.94 | 0.028 a,* | 0.064 | −0.521 | 0.895 (0.828–0.940) | 2.5% | |
| non-athletes | 38 | 11.55 | 3.77 | Small | 0.923 (0.898–0.972) | 1.1% | ||||
| diastolic velocity—left deep femoral artery | futsal athletes | 38 | 12.73 | 2.33 | 0.753 b | −0.073 | −0.607–0.46 | 0.972 (0.953–0.985) | 1.1% | |
| non-athletes | 38 | 12.49 | 3.99 | Trivial | 1 (0.999–1) | 0.8% | ||||
| diastolic velocity—right superficial femoral artery | futsal athletes | 38 | 17.67 | 3.31 | 0.026 b,* | −0.522 | −1.065–0.021 | 0.993 (0.988–0.996) | 1.1% | |
| non-athletes | 38 | 15.95 | 3.28 | Small | 0.998 (0.997–0.999) | 0.8% | ||||
| diastolic velocity—left superficial femoral artery | futsal athletes | 38 | 17.57 | 3.82 | 0.106 a | 0.034 | −0.377 | 1 (0.999–1) | 0.5% | |
| non-athletes | 38 | 16.35 | 3.93 | Small | 1 (0.999–1) | 0.6% | ||||
| diastolic velocity—right popliteal artery | futsal athletes | 38 | 13.66 | 2.74 | 0.002 a,* | 0.127 | −0.763 | 0.999 (0.998–0.999) | 0.7% | |
| non-athletes | 38 | 11.56 | 2.35 | Moderate | 0.999 (0.998–0.999) | 0.8% | ||||
| diastolic velocity—left popliteal artery | futsal athletes | 38 | 14.25 | 2.87 | 0.007 a,* | 0.097 | −0.655 | 0.999 (0.999–1) | 0.7% | |
| non-athletes | 38 | 12.53 | 3.29 | Moderate | 0.999 (0.999–1) | 0.9% |
| Systolic velocity | Limb | Group | N | p |
|---|---|---|---|---|
| common femoral/deep femoral | Right | futsal athletes | 38 | 0.001 * |
| non-athletes | 38 | 0.001 * | ||
| common femoral/superficial femoral | futsal athletes | 38 | 0.183 | |
| non-athletes | 38 | 0.155 | ||
| common femoral/popliteal | futsal athletes | 38 | 0.000 * | |
| non-athletes | 38 | 0.000 * | ||
| deep femoral/superficial femoral | futsal athletes | 38 | 0.000 * | |
| non-athletes | 38 | 0.000 * | ||
| deep femoral/popliteal | futsal athletes | 38 | 0.001 * | |
| non-athletes | 38 | 0.003 * | ||
| superficial femoral/popliteal | futsal athletes | 38 | 0.000 * | |
| non-athletes | 38 | 0.000 * | ||
| common femoral/deep femoral | Left | futsal athletes | 38 | 0.000 * |
| non-athletes | 38 | 0.286 | ||
| common femoral/superficial femoral | futsal athletes | 38 | 0.564 | |
| non-athletes | 38 | 0.790 | ||
| common femoral/popliteal | futsal athletes | 38 | 0.000 * | |
| non-athletes | 38 | 0.000 * | ||
| deep femoral/superficial femoral | futsal athletes | 38 | 0.000 * | |
| non-athletes | 38 | 0.183 | ||
| deep femoral/popliteal | futsal athletes | 38 | 0.120 | |
| non-athletes | 38 | 0.000 * | ||
| superficial femoral/popliteal | futsal athletes | 38 | 0.000 * | |
| non-athletes | 38 | 0.000 * |
| Diastolic Velocity | Limb | Group | N | p |
|---|---|---|---|---|
| common femoral/deep femoral | right | futsal athletes | 38 | 0.000 * |
| non-athletes | 38 | 0.000 * | ||
| common femoral/superficial femoral | futsal athletes | 38 | 0.450 | |
| non-athletes | 38 | 0.286 | ||
| common femoral/popliteal | futsal athletes | 38 | 0.000 * | |
| non-athletes | 38 | 0.000 * | ||
| deep femoral/superficial femoral | futsal athletes | 38 | 0.000 * | |
| non-athletes | 38 | 0.000 * | ||
| deep femoral/popliteal | futsal athletes | 38 | 0.689 | |
| non-athletes | 38 | 0.859 | ||
| superficial femoral/popliteal | futsal athletes | 38 | 0.000 * | |
| non-athletes | 38 | 0.000 * | ||
| common femoral/deep femoral | left | futsal athletes | 38 | 0.000 * |
| non-athletes | 38 | 0.190 | ||
| common femoral/superficial femoral | futsal athletes | 38 | 0.756 | |
| non-athletes | 38 | 0.076 | ||
| common femoral/popliteal | futsal athletes | 38 | 0.000 * | |
| non-athletes | 38 | 0.005 * | ||
| deep femoral/superficial femoral | futsal athletes | 38 | 0.000 * | |
| non-athletes | 38 | 0.000 * | ||
| deep femoral/popliteal | futsal athletes | 38 | 0.046 * | |
| non-athletes | 38 | 0.444 | ||
| superficial femoral/popliteal | futsal athletes | 38 | 0.000 * | |
| non-athletes | 38 | 0.000 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duarte-Mendes, P.; Paulo, R.; Coelho, P.; Rodrigues, F.; Marques, V.; Mateus, S. Variability of Lower Limb Artery Systolic–Diastolic Velocities in Futsal Athletes and Non-Athletes: Evaluation by Arterial Doppler Ultrasound. Int. J. Environ. Res. Public Health 2020, 17, 570. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020570
Duarte-Mendes P, Paulo R, Coelho P, Rodrigues F, Marques V, Mateus S. Variability of Lower Limb Artery Systolic–Diastolic Velocities in Futsal Athletes and Non-Athletes: Evaluation by Arterial Doppler Ultrasound. International Journal of Environmental Research and Public Health. 2020; 17(2):570. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020570
Chicago/Turabian StyleDuarte-Mendes, Pedro, Rui Paulo, Patrícia Coelho, Francisco Rodrigues, Vasco Marques, and Sónia Mateus. 2020. "Variability of Lower Limb Artery Systolic–Diastolic Velocities in Futsal Athletes and Non-Athletes: Evaluation by Arterial Doppler Ultrasound" International Journal of Environmental Research and Public Health 17, no. 2: 570. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020570