Spatiotemporal Epidemiology of Varicella in Chongqing, China, 2014–2018


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Case Definition
2.2. Study Area
2.3. Statistical Analysis
2.3.1. Descriptive and Geographical Analysis
2.3.2. Spatial Autocorrelation Analysis
2.3.3. Spatial and Space-Time Clustering Analysis
2.3.4. Statistical Software
3. Results
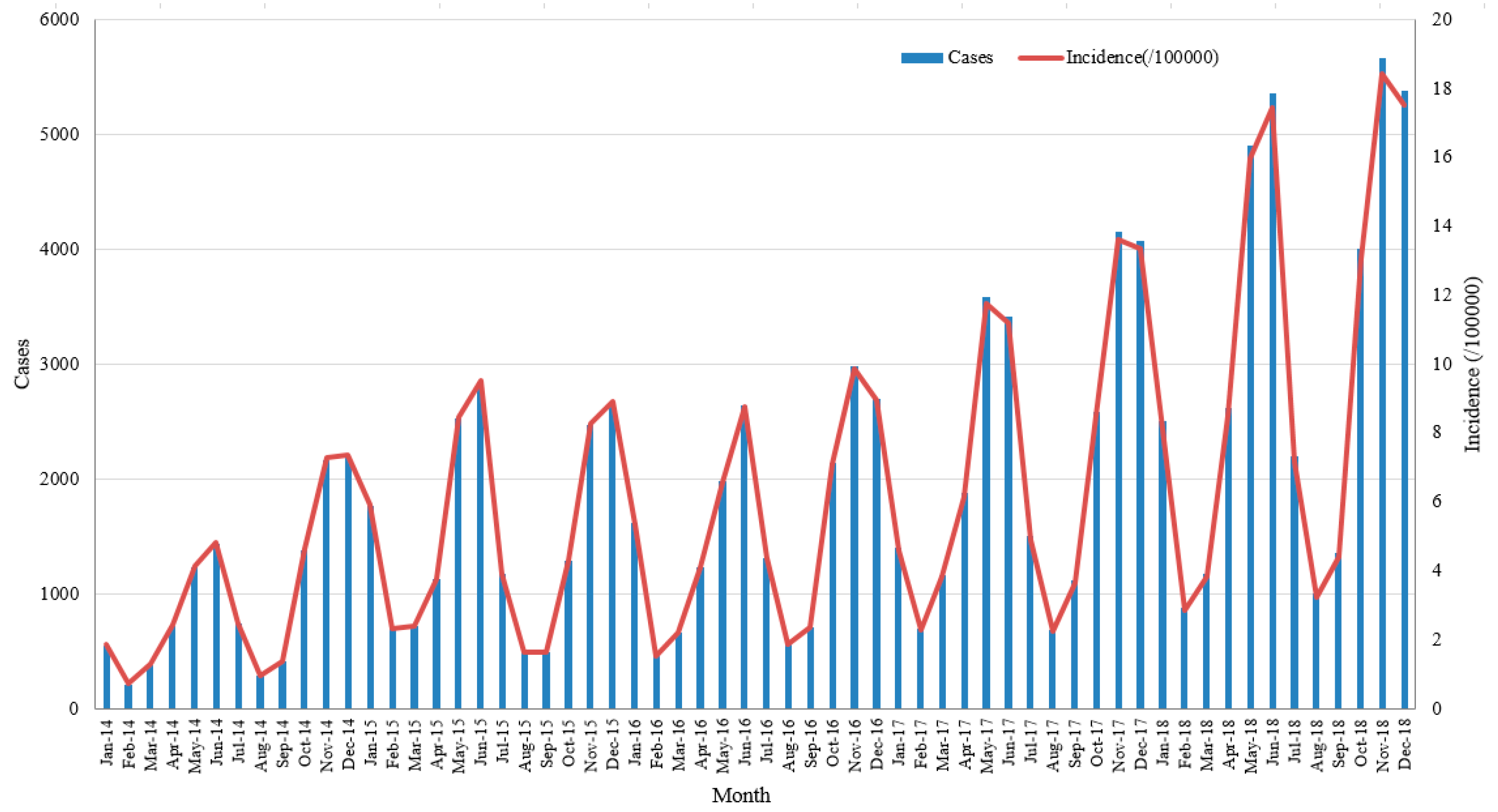
3.1. Epidemiological Characteristics
3.2. Spatial Distribution
3.3. Spatial Autocorrelation Analysis
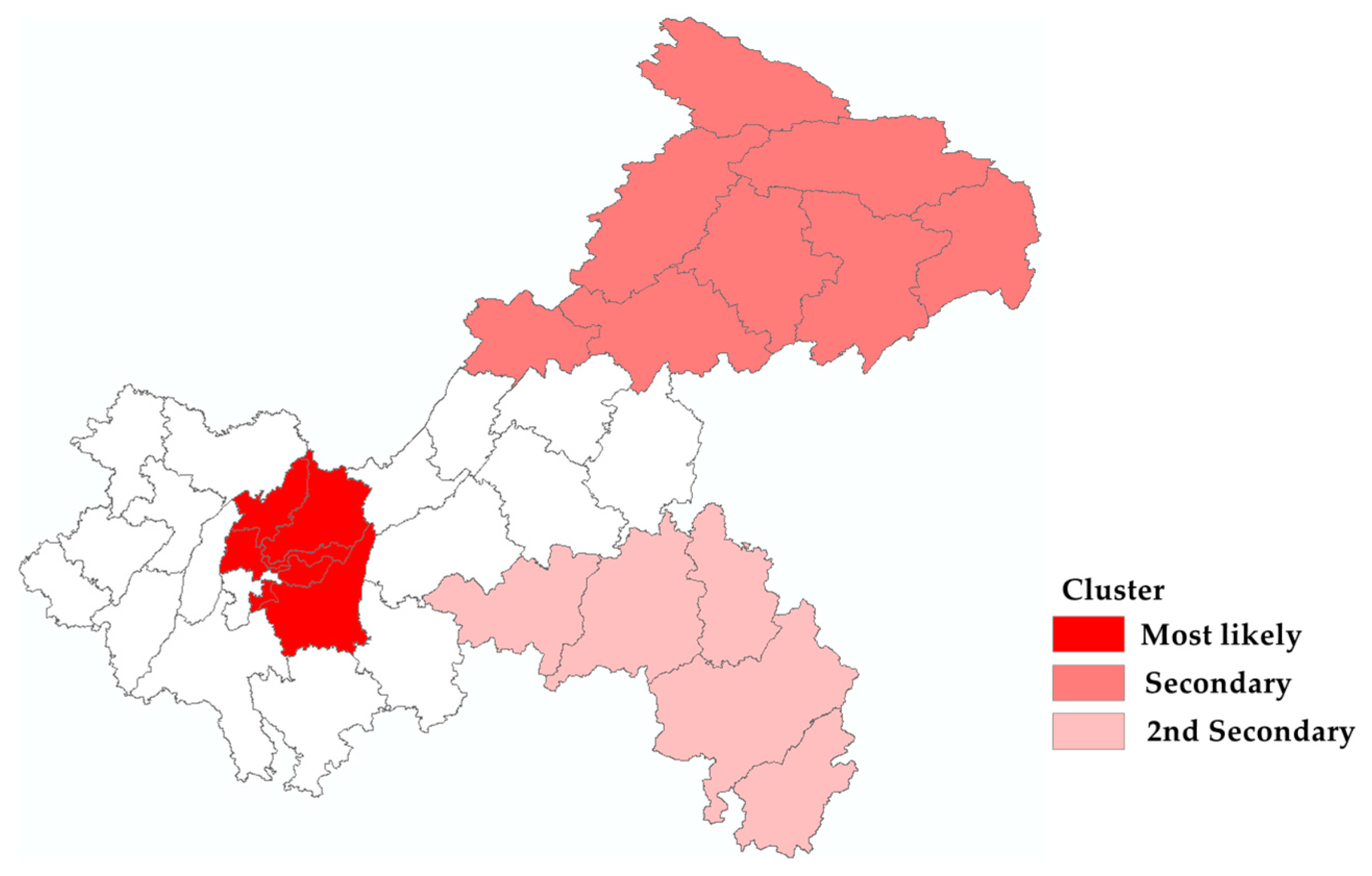
3.4. Cluster Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Arvin, A.M. Varicella-zoster virus. Clin. Microbiol. Rev. 1996, 6, 361–381. [Google Scholar] [CrossRef]
- Wharton, M. The epidemiology of varicella-zoster virus infections. Infect. Dis. Clin. N. Am. 1996, 10, 571–581. [Google Scholar] [CrossRef] [Green Version]
- Heininger, U.; Seward, J.F. Varicella. Lancet 2006, 368, 1365–1376. [Google Scholar] [CrossRef]
- Choo, P.W.; Donahue, J.G.; Manson, J.E.; Platt, R. The epidemiology of varicella and its complications. J. Infect. Dis. 1995, 172, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Jaeggi, A.; Zurbruegg, R.P.; Aebi, C. Complications of varicella in a defined central European population. Arch. Dis. Child. 1998, 79, 472–477. [Google Scholar] [CrossRef]
- Hope-Simpson, R.E. The nature of herpes zoster. Practitioner 1964, 193, 217–219. [Google Scholar]
- Lungu, O.; Annunziato, P.W.; Gershon, A.; Staugaitis, S.M.; Josefson, D.; LaRussa, P.; Silverstein, S.J. Reactivated and latent varicella-zoster virus in human dorsal root ganglia. Proc. Natl. Acad. Sci. USA 1995, 92, 10980–10984. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, P.G.E.; Gershon, A.A. Clinical Features of Varicella-Zoster Virus Infection. Viruses 2018, 10, 609. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Varicella and herpes zoster vaccines: WHO position paper, June 2014—Recommendations. Vaccine 2016, 34, 198–199. [Google Scholar] [CrossRef]
- Varela, F.H.; Pinto, L.A.; Scotta, M.C. Global impact of varicella vaccination programs. Hum. Vaccin. Immunother. 2019, 15, 645–657. [Google Scholar] [CrossRef] [Green Version]
- Hirose, M.; Gilio, A.E.; Ferronato, A.E.; Ragazzi, S.L. The impact of varicella vaccination on varicella-related hospitalization rates: Global data review. Rev. Paul. Pediatr. 2016, 34, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.S.; Zhang, J.; Marin, M. Epidemiology of Varicella During the 2-Dose Varicella Vaccination Program—United States, 2005–2014. Morb. Mortal. Wkly. Rep. 2016, 65, 902–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quian, J.; Ruttimann, R.; Romero, C.; Dall’Orso, P.; Cerisola, A.; Breuer, T.; Greenberg, M.; Verstraeten, T. Impact of universal varicella vaccination on 1-year-olds in Uruguay: 1997–2005. Arch. Dis. Child. 2008, 93, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Waye, A.; Jacobs, P.; Tan, B. The impact of the universal infant varicella immunization strategy on Canadian varicella-related hospitalization rates. Vaccine 2013, 31, 4744–4748. [Google Scholar] [CrossRef]
- Heywood, A.E.; Wang, H.; Macartney, K.K.; McIntyre, P. Varicella and herpes zoster hospitalizations before and after implementation of one-dose varicella vaccination in Australia: An ecological study. Bull. World Health Organ. 2014, 92, 593–604. [Google Scholar] [CrossRef]
- Siu, H.T.; Li, J.C.; Wang, M.; Liu, Y.M.; Yin, D.P. Varicella epidemiology in China, 2005–2015. Chin. J. Vaccines Immun. 2019, 2, 155–159. [Google Scholar]
- Chongqing Health and Family Planning Commission. Available online: http://www.cq.gov.cn/publicity_swsjsw/wsjhsyfnet/ws/310980?ad_check=1 (accessed on 19 August 2014).
- Bureau of Disease Control and Prevention. Available online: http://www.nhc.gov.cn/ewebeditor/uploadfile/2015/11/20151110131652539.docx (accessed on 29 October 2015).
- Huang, L.; Abe, E.M.; Li, X.X.; Bergquist, R.; Xu, L.; Xue, J.B.; Ruan, Y.; Cao, C.L.; Li, S.Z. Space-time clustering and associated risk factors of pulmonary tuberculosis in southwest China. Infect. Dis. Poverty 2018, 7, 91. [Google Scholar] [CrossRef]
- Lu, Q.; Wu, H.; Ding, Z.; Wu, C.; Lin, J. Analysis of Epidemiological Characteristics of Scarlet Fever in Zhejiang Province, China, 2004–2018. Int. J. Env. Res. Public. Health 2019, 16, 3454. [Google Scholar] [CrossRef] [Green Version]
- Mao, Y.; Zhang, N.; Zhu, B.; Liu, J.; He, R. A descriptive analysis of the Spatio-temporal distribution of intestinal infectious diseases in China. BMC Infect. Dis. 2019, 19, 766. [Google Scholar] [CrossRef]
- Iftimi, A.; Martinez-Ruiz, F.; Miguez Santiyan, A.; Montes, F. Spatio-temporal cluster detection of chickenpox in Valencia, Spain in the period 2008–2012. Geospat. Health 2015, 10, 341. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.H. Changes in the Epidemiology of Varicella after the Introduction of a Universal Vaccination Program in the Republic of Korea. Ph.D. Thesis, Seoul National University, Seoul, Korea, 2019. [Google Scholar]
- Xu, Y.Q.; Fu, Z.Z.; Zhou, J.Y.; Deng, G.H.; Gong, C.; Cai, F.W.; Han, S.S. Epidemiological characteristics on temporal-spatial distribution of varicella in Guangxi Zhuang Autonomous Region, 2014–2016. Zhonghua Liu Xing Bing Xue Za Zhi 2017, 38, 1390–1393. [Google Scholar] [CrossRef] [PubMed]
- Anselin, L.; Syabri, I.; Kho, Y. GeoDa: An Introduction to Spatial Data Analysis. Geogr. Anal. 2006, 38, 5–22. [Google Scholar] [CrossRef]
- Getis, A. Reflections on spatial autocorrelation. Reg. Sci. Urban Econ. 2007, 37, 491–496. [Google Scholar] [CrossRef]
- Luc, A. Local Indicators of Spatial Association—LISA. Geogr. Anal. 2010, 27, 93–115. [Google Scholar]
- Kulldorff, M. SaTScanTM User Guide for Version 9.5; SaTScan: Boston, MA, USA, 2018. [Google Scholar]
- Xu, J.W.; Wang, Q.; Kuang, S.S. Epidemiological Characteristics of Varicella in Chongqing, 2007–2013. J. Prev. Med. Inf. 2015, 31, 339–342. [Google Scholar]
- Chen, H.; Liu, L.G. Epidemiological characteristics of varicella in Sichuan Province from 2012–2017. Occup. Health 2018, 34, 2672–2674. [Google Scholar]
- Li, Z.J.; Wang, Y.; Wang, D.M.; Tao, Z.F.; Yu, C.; Sun, J.; Song, S.C. Epidemiological characteristics of varicella in Guizhou, 2013–2017. Mod. Prev. Med. 2019, 46, 3101–3103. [Google Scholar]
- Dai, P.; Wang, X.N.; Zhang, C.; Guan, X.H.; Wang, L. Epidemiological analysis of varicella in Hubei Province from 2008 to 2017. Mod. Prev. Med. 2018, 45, 2885–2890. [Google Scholar]
- Zhang, L.; Ma, W.; Liu, Y.; Wang, Y.; Sun, X.; Hu, Y.; Deng, X.; Lu, P.; Tang, F.; Wang, Z.; et al. Analysis of sero-epidemiological characteristics of varicella in healthy children in Jiangsu Province, China. BMC Infect. Dis. 2018, 18, 563. [Google Scholar] [CrossRef]
- Suo, L.; Lu, L.; Wang, Q.; Yang, F.; Wang, X.; Pang, X.; Marin, M.; Wang, C. Varicella outbreak in a highly-vaccinated school population in Beijing, China during the voluntary two-dose era. Vaccine 2017, 35, 4368–4373. [Google Scholar] [CrossRef] [Green Version]
- Smith-Norowitz, T.A.; Saadia, T.A.; Norowitz, K.B.; Joks, R.; Durkin, H.G.; Kohlhoff, S. Negative IgG Varicella Zoster Virus Antibody Status: Immune Responses Pre and Post Re-immunization. Infect. Dis. 2018, 7, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Marin, M.; Marti, M.; Kambhampati, A.; Jeram, S.M.; Seward, J.F. Global Varicella Vaccine Effectiveness: A Meta-analysis. Pediatrics 2016, 137, e20153741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melegaro, A.; Marziano, V.; Del Fava, E.; Poletti, P.; Tirani, M.; Rizzo, C.; Merler, S. The impact of demographic changes, exogenous boosting and new vaccination policies on varicella and herpes zoster in Italy: A modelling and cost-effectiveness study. BMC Med. 2018, 16, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.; Liu, S.; Che, X.; Liu, Y.; Zhang, X.; Du, J.; Zhang, X.; Wang, J.; Xu, E. Seroepidemiology of varicella in Hangzhou, China in the vaccine era. Hum. Vaccin. Immunother. 2018, 14, 2464–2471. [Google Scholar] [CrossRef] [Green Version]
- Luan, L.; Shen, X.; Qiu, J.; Jing, Y.; Zhang, J.; Wang, J.; Zhang, J.; Dong, C. Seroprevalence and molecular characteristics of varicella-zoster virus infection in Chinese children. BMC Infect. Dis. 2019, 19, 643. [Google Scholar] [CrossRef]
- Chongqing Health and Family Planning Commission. Available online: http://x2fyouy.cq.gov.cn/publicity_swsjsw/wsjhsyfnet/ws/573992 (accessed on 3 October 2018).
- Shi, W.; Yan, T.T.; Guan, L.Y.; Zhang, L.; Li, S.; Zhang, S.B.; Cao, N.J.; Liu, J.F.; Yu, P.B.; Xu, Y.; et al. Epidemiology of varicella in Shaanxi Province during 2005 and 2017. Xi’an Jiao Tong Da Xue Xue Bao Yi Xue Ban 2019, 40, 809. [Google Scholar]
- Goh, A.E.N.; Choi, E.H.; Chokephaibulkit, K.; Choudhury, J.; Kuter, B.; Lee, P.-I.; Marshall, H.; Kim, J.O.; Wolfson, L.J. Burden of varicella in the Asia-Pacific region: A systematic literature review. Expert. Rev. Vaccines 2019, 18, 475–493. [Google Scholar] [CrossRef] [Green Version]
- Krolasik, A.; Paradowska-Stankiewicz, I. Chickenpox in Poland in 2016. Przegl. Epidemiol. 2018, 72, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Huang, L.M.; Chang, I.S.; Tsai, F.Y.; Chang, L.Y. Disease burden and epidemiological characteristics of varicella in Taiwan from 2000 to 2005. J. Microbiol. Immunol. Infect. 2009, 42, 5–12. [Google Scholar]
- Yang, Y.; Chen, R.; Xu, J.; Li, Q.; Xu, X.; Ha, S.; Song, W.; Tan, J.; Xu, F.; Kan, H. The effects of ambient temperature on outpatient visits for varicella and herpes zoster in Shanghai, China: A time-series study. J. Am. Acad. Derm. 2015, 73, 660–665. [Google Scholar] [CrossRef]
- Lolekha, S.; Tanthiphabha, W.; Sornchai, P.; Kosuwan, P.; Sutra, S.; Warachit, B.; Chup-Upprakarn, S.; Hutagalung, Y.; Weil, J.; Bock, H.L. Effect of climatic factors and population density on varicella zoster virus epidemiology within a tropical country. Am. J. Trop. Med. Hyg. 2001, 64, 131–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumi, A. Role of temperature in reported chickenpox cases in northern European countries: Denmark and Finland. BMC Res. Notes 2018, 11, 377. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.W. Review of varicella zoster seroepidemiology in India and Southeast Asia. Trop. Med. Int. Health 1998, 3, 886–890. [Google Scholar] [CrossRef] [PubMed]
- Varicella. Available online: https://www.who.int/immunization/diseases/varicella/en/4 (accessed on 15 April 2015).
- Chan, J.Y.; Leung, K.M.; Tam, W.W.; Lee, A. Varicella vaccine uptake and associated factors in children in Hong Kong. Epidemiol. Infect. 2014, 142, 994–1001. [Google Scholar] [CrossRef]
- Hu, Y.; Chen, Y.; Wang, Y.; Liang, H. Knowledge, Attitude and Practice of Pregnant Women towards Varicella and Their Children’s Varicella Vaccination: Evidence from Three Distrcits in Zhejiang Province, China. Int. J. Env. Res. Public Health 2017, 14, 1110. [Google Scholar] [CrossRef] [Green Version]
- Liu, A.P.; Sun, L.L. Meta-analysis of varicella vaccine coverage among Chinese children. Chin. J. Vaccines Immun. 2017, 23, 698–704. [Google Scholar]
- Zhu, S.; Zeng, F.; Xia, L.; He, H.; Zhang, J. Incidence rate of breakthrough varicella observed in healthy children after 1 or 2 doses of varicella vaccine: Results from a meta-analysis. Am. J. Infect. Control. 2018, 46, e1–e7. [Google Scholar] [CrossRef]
- Wutzler, P.; Bonanni, P.; Burgess, M.; Gershon, A.; Sáfadi, M.A.; Casabona, G. Varicella vaccination—The global experience. Expert. Rev. Vaccines 2017, 16, 833–843. [Google Scholar] [CrossRef] [Green Version]
- Ciofi degli Atti, M.L.; Rota, M.C.; Mandolini, D.; Bella, A.; Gabutti, G.; Crovari, P.; Salmaso, S. Assessment of varicella underreporting in Italy. Epidemiol. Infect. 2002, 128, 479–484. [Google Scholar] [CrossRef]
- Socan, M. Evaluation of mandatory case-based reporting system for varicella in the prevaccine era. Cent. Eur. J. Public Health 2010, 18, 99–103. [Google Scholar] [CrossRef]
- Lopez, A.S.; Lichtenstein, M.; Schmid, S.D.; Bialek, S. Assessment of varicella surveillance and outbreak control practices—United States, 2012. Mmwr. Morb. Mortal. Wkly. Rep. 2014, 63, 785–788. [Google Scholar] [PubMed]
- Xie, X.Q.; Chen, C.; Yang, X.Y.; Wei, Z.H.; Liu, J.L. [Analysis of the quality of notifiable infectious disease report in Beijing medical treatment organizations]. Zhonghua Yu Fang Yi Xue Za Zhi 2008, 42, 335–338. [Google Scholar] [PubMed]
- Jin, L.Z.; Ge, H.; Du, X.J.; Chen, M.; Yu, M.; Zheng, H.; Guo, Q. Reporting quality of notifiable communicable diseases in hospitals in China, 2015. Dis. Surveill. 2016, 31, 883–886. [Google Scholar] [CrossRef]
- Wang, L.P.; Cao, Y.; Zeng, L.J.; Ren, X.; Li, Z.J.; Yu, H.J. Diagnosis and reporting of communicable diseases in basic medical institutions in China. Dis. Surveill. 2014, 29, 176–180. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2014 | 2015 | 2016 | 2017 | 2018 | Total | |
|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | |
| Age (year) | ||||||
| 0~ | 323 (2.8) | 597 (3.3) | 607 (3.2) | 837 (3.2) | 932 (2.5) | 3296 (2.9) |
| 1~ | 383 (3.3) | 535 (2.9) | 652 (3.4) | 786 (3.0) | 975 (2.6) | 3331 (3.0) |
| 2~ | 246 (2.1) | 388 (2.1) | 410 (2.2) | 544 (2.1) | 769 (2.1) | 2357 (2.1) |
| 3~ | 429 (3.7) | 681 (3.7) | 653 (3.4) | 886 (3.4) | 1531 (4.1) | 4180 (3.7) |
| 4~ | 660 (5.7) | 1039 (5.7) | 988 (5.2) | 1247 (4.8) | 1888 (5.1) | 5822 (5.2) |
| 5~ | 995 (8.5) | 1440 (7.9) | 1223 (6.4) | 1751 (6.7) | 2452 (6.6) | 7861 (7.0) |
| 6~ | 1124 (9.6) | 1710 (9.4) | 1494 (7.9) | 1866 (7.1) | 2841 (7.6) | 9035 (8.1) |
| 7~ | 1204 (10.3) | 1830 (10.0) | 1770 (9.3) | 2245 (8.6) | 3031 (8.2) | 10,080 (9.0) |
| 8~ | 947 (8.1) | 1686 (9.2) | 1548 (8.1) | 2265 (8.6) | 3102 (8.4) | 9548 (8.5) |
| 9~ | 746 (6.4) | 1192 (6.5) | 1240 (6.5) | 1965 (7.5) | 2622 (7.1) | 7765 (6.9) |
| 10~ | 2188 (18.7) | 3802 (20.8) | 4283 (22.5) | 6406 (24.4) | 9764 (26.3) | 26,443 (23.6) |
| 15~ | 1095 (9.4) | 1438 (7.9) | 1878 (9.9) | 2406 (9.1) | 3211 (8.7) | 10,028 (8.9) |
| 20~ | 565 (4.8) | 715 (3.9) | 785 (4.1) | 1023 (3.9) | 1216 (3.3) | 4304 (3.8) |
| 25~ | 456 (3.9) | 729 (4.0) | 841 (4.4) | 980 (3.7) | 1211 (3.3) | 4217 (3.8) |
| 30~ | 224 (1.9) | 331 (1.8) | 449 (2.4) | 708 (2.7) | 1014 (2.7) | 2726 (2.4) |
| 35~ | 99 (0.8) | 156 (0.9) | 201 (1.1) | 328 (1.2) | 496 (1.3) | 1280 (1.1) |
| Gender | ||||||
| Male | 6172 (52.8) | 9709 (53.1) | 10,062 (52.9) | 13,742 (52.4) | 19,212 (51.8) | 58,897 (52.5) |
| Female | 5512 (47.2) | 8560 (46.9) | 8960 (47.1) | 12,501 (47.6) | 17,843 (48.2) | 53,376 (47.5) |
| Sex ratio | 1.12 | 1.13 | 1.12 | 1.10 | 1.08 | 1.10 |
| Occupation | ||||||
| Scattered children 1 | 1226 (10.5) | 1901 (10.4) | 1963 (10.4) | 2455 (9.4) | 3108 (8.4) | 10,653 (9.5) |
| Kindergarten children | 2397 (20.5) | 3842 (21.0) | 3406 (17.9) | 4562 (17.4) | 6946 (18.7) | 21,153 (18.8) |
| Student | 6729 (57.6) | 10,613 (58.0) | 11,400 (59.9) | 16,309 (62.1) | 23,149 (62.5) | 68,200 (60.8) |
| others | 1332 (11.4) | 1913 (10.47) | 2253 (11.8) | 2917 (11.1) | 3852 (10.4) | 12,267 (10.9) |
| Total | 11,684 | 18,269 | 19,022 | 26,243 | 37,055 | 112,273 |
| Year | Moran’s I | Z-Score | p-Value |
|---|---|---|---|
| 2014 | 0.0274 | 0.5354 | 0.272 |
| 2015 | 0.1049 | 1.1856 | 0.124 |
| 2016 | 0.2030 | 2.2173 | 0.021 |
| 2017 | 0.0383 | 0.6808 | 0.249 |
| 2018 | 0.1048 | 1.2736 | 0.109 |
| Cluster Type | Counties (n) | Observed/Expected | Radius (km) | Relative Risk | Log Likelihood Ratio | p-Value |
|---|---|---|---|---|---|---|
| Most likely | 4 | 1.68 | 31.61 | 1.89 | 3517.23 | <0.001 |
| Secondary | 3 | 1.32 | 22.23 | 1.36 | 577.31 | <0.001 |
| 2nd Secondary | 1 | 1.52 | 0 | 1.55 | 518.26 | <0.001 |
| 3rd Secondary | 1 | 1.60 | 0 | 1.62 | 263.35 | <0.001 |
| 4th Secondary | 1 | 1.54 | 0 | 1.55 | 227.48 | <0.001 |
| 5th Secondary | 1 | 1.21 | 0 | 1.22 | 51.92 | <0.001 |
| 6th Secondary | 1 | 1.15 | 0 | 1.16 | 48.63 | <0.001 |
| 7th Secondary | 1 | 1.20 | 0 | 1.21 | 34.17 | <0.001 |
| Cluster Type | Cluster Time | Counties (n) | Observed/Expected | Radius (km) | Relative Risk | Log Likelihood Ratio | p-Value |
|---|---|---|---|---|---|---|---|
| Most likely | 2016/10–2018/12 | 8 | 1.98 | 31.18 | 2.25 | 5379.65 | <0.001 |
| Secondary | 2018/10–2018/12 | 8 | 2.66 | 166.76 | 2.71 | 1098.91 | <0.001 |
| 2nd Secondary | 2017/11–2017/12 | 5 | 3.95 | 160.56 | 3.98 | 717.76 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, H.; Zhao, H.; Ou, R.; Zeng, Q.; Hu, L.; Qiu, H.; Sharma, M.; Ye, M. Spatiotemporal Epidemiology of Varicella in Chongqing, China, 2014–2018. Int. J. Environ. Res. Public Health 2020, 17, 662. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020662
Zhu H, Zhao H, Ou R, Zeng Q, Hu L, Qiu H, Sharma M, Ye M. Spatiotemporal Epidemiology of Varicella in Chongqing, China, 2014–2018. International Journal of Environmental Research and Public Health. 2020; 17(2):662. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020662
Chicago/Turabian StyleZhu, Hua, Han Zhao, Rong Ou, Qing Zeng, Ling Hu, Hongfang Qiu, Manoj Sharma, and Mengliang Ye. 2020. "Spatiotemporal Epidemiology of Varicella in Chongqing, China, 2014–2018" International Journal of Environmental Research and Public Health 17, no. 2: 662. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020662