Effect of Income Level and Perception of Susceptibility and Severity of COVID-19 on Stay-at-Home Preventive Behavior in a Group of Older Adults in Mexico City

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Statistical Analysis
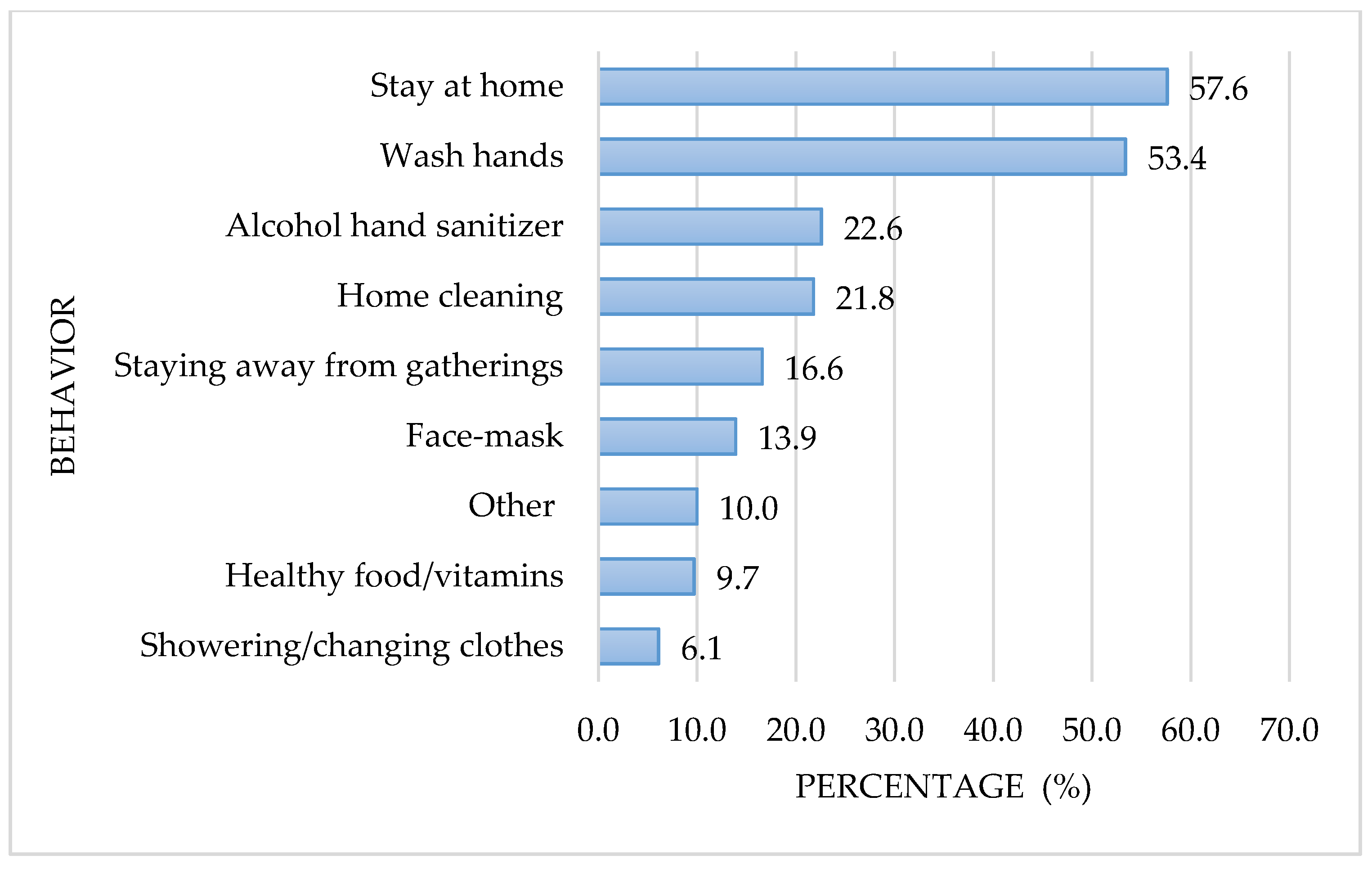
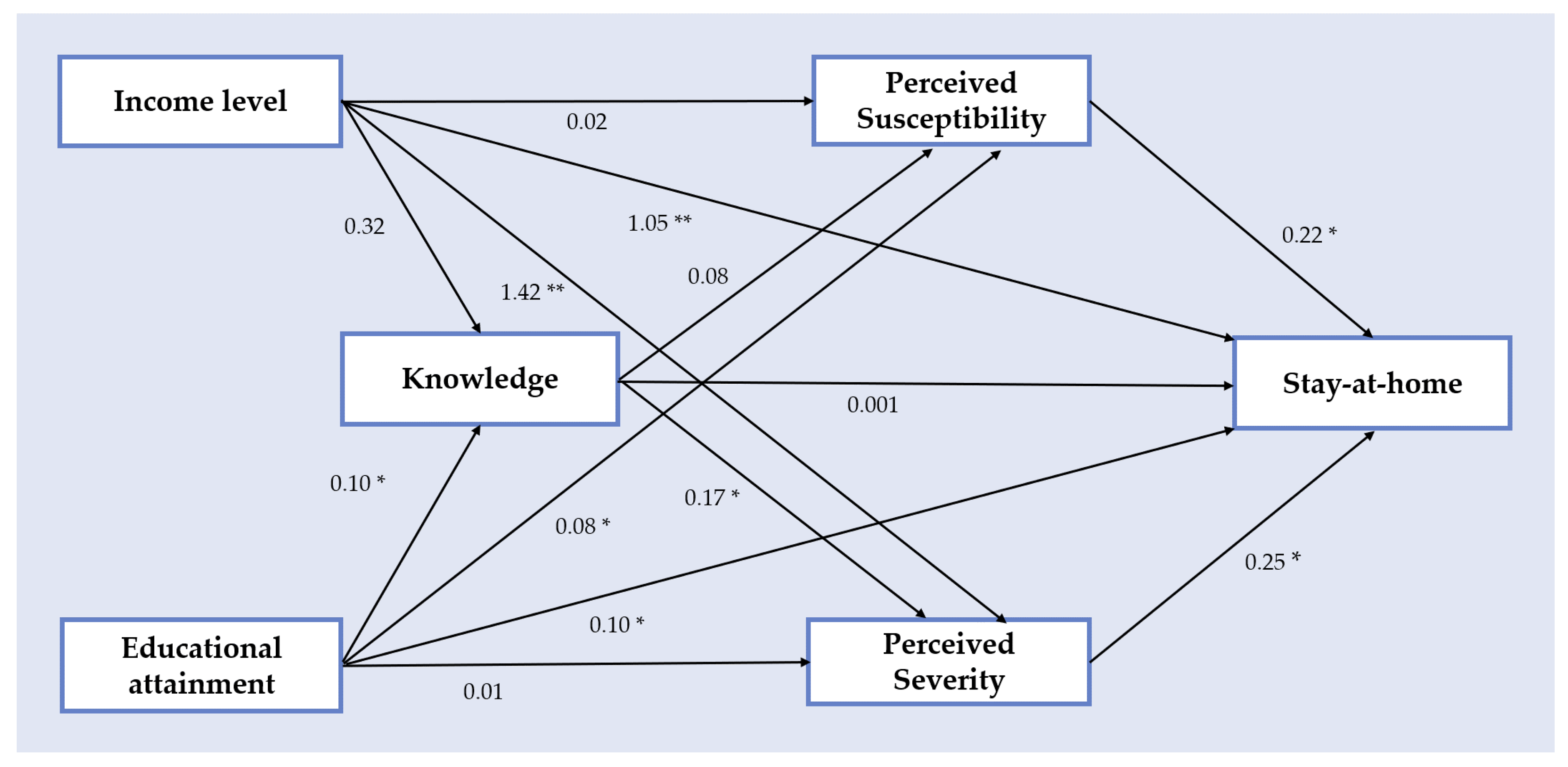
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. 2019-nCoV Outbreak Is an Emergency of International Concern. Available online: http://www.euro.who.int/en/health-topics/emergencies/pages (accessed on 19 July 2020).
- Cascella, M.; Rajnik, M.; Cuomo, A.; Dulebohn, S.C.; di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19); StatPearls Publishing [Internet]: Treasure Island, FL, USA, 2020. [Google Scholar]
- 3BBC News Mundo Coronavirus en México: Confirman los Primeros Casos de Covid-19 en el País. Available online: https://www.bbc.com/mundo/noticias-america-latina-51677751 (accessed on 19 July 2020).
- López-Ortiz, E.; López-Ortiz, G.; Mendiola-Pastrana, I.R.; Mazón-Ramírez, J.J.; Díaz-Quiñonez, J.A. From the handling of an outbreak by an unknown pathogen in Wuhan to the preparedness and response in the face of the emergence of Covid-19 in Mexico. Gac. Med. Mex. 2020, 156, 132–137. [Google Scholar] [CrossRef] [Green Version]
- Mexican Ministry of Health Daily Technical Statement New Coronavirus in the World (COVID-19) March 24 [Comunicado Técnico Diario Nuevo Coronavirus en el Mundo (COVID-19) 24 de Marzo]. Available online: https://www.gob.mx/cms/uploads/attachment/file/571238/Comunicado_Tecnico_Diario_COVID-19_2020.03.24.pdf (accessed on 18 July 2020).
- National Institute of Statistic Geography and Informatics Statistics on the International Day of Older Persons (October 1) National Data [Estadísticas a Propósito del día Internacional de las Personas de Edad (1° de Octubre) Datos Nacionales]. Available online: https://www.inegi.org.mx/contenidos/saladeprensa/aproposito/2019/edad2019_Nal.pdf (accessed on 12 August 2020).
- Kang, S.-J.; Jung, S.-I. Age-Related Morbidity and Mortality among Patients with COVID-19. Infect. Chemother. 2020, 52, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Bor, S.J.; Cohen, G.H.; Galea, S. Population health in an era of rising income inequality: USA, 1980–2015. Lancet 2017, 389, 1475–1490. [Google Scholar] [CrossRef]
- Nolasco, A.; Moncho, J.; Quesada, J.A.; Melchor, I.; Pereyra-Zamora, P.; Tamayo-Fonseca, N.; Martinez-Beneito, M.A.; Zurriaga, O.; Ballesta, M.; Daponte, A.; et al. Trends in socioeconomic inequalities in preventable mortality in urban areas of 33 Spanish cities, 1996–2007 (MEDEA project). Int. J. Equity Health 2015, 14, 33. [Google Scholar] [CrossRef] [Green Version]
- Galobardes, B. Indicators of socioeconomic position (part 1). J. Epidemiol. Community Health 2006, 60, 7–12. [Google Scholar] [CrossRef] [Green Version]
- O’Sullivan, T.L.; Phillips, K.P. From SARS to pandemic influenza: The framing of high-risk populations. Nat. Hazards 2019, 98, 103–117. [Google Scholar] [CrossRef] [Green Version]
- Khalatbari-Soltani, S.; Cumming, R.G.; Delpierre, C.; Kelly-Irving, M. Importance of collecting data on socioeconomic determinants from the early stage of the COVID-19 outbreak onwards. J. Epidemiol. Community Health 2020, 74, 620–623. [Google Scholar] [CrossRef]
- Chokshi, D.A. Income, Poverty, and Health Inequality. JAMA 2018, 319, 1312–1313. [Google Scholar] [CrossRef]
- Marmot, M. The Influence of Income on Health: Views of an Epidemiologist. Health Aff. 2002, 21, 31–46. [Google Scholar] [CrossRef]
- Government of Mexico Universal Pension for the Elderly [Pensión Universal Para Personas Adultas Mayores]. Available online: https://www.gob.mx/pensionpersonasadultasmayores (accessed on 12 August 2020).
- Government of Mexico. Presidency of the Republic. More than Eight Million Older Mexican Adults Receive a Double Universal Pension, Informs the President [Más de ocho Millones de Adultos Mayores Mexicanos Reciben Pensión Universal al Doble, Informa Presidente]. Available online: https://www.gob.mx/presidencia/prensa/mas-de-ocho-millones-de-adultos-mayores-mexicanos-reciben-pension-universal-al-doble-informa-presidente#:~:text=Ciudad%20de%20M%C3%A9xico%2C%2010%20de,96%20mil%20millones%20de%20pesos (accessed on 12 August 2020).
- HelpAge International Older Women and Social Protection. Statement to the 63rd Commission on the Status of Women, March 2019. Available online: https://age-platform.eu/sites/default/files/HelpAge_Statement_to_CSW2019.pdf (accessed on 19 September 2020).
- World Health Organization. Coronavirus Disease (COVID-19) Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 20 July 2020).
- Johns Hopkins University COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. Available online: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed on 8 July 2020).
- Scherr, C.L.; Jensen, J.D.; Christy, K. Dispositional pandemic worry and the health belief model: Promoting vaccination during pandemic events. J. Public Health 2017, 39, e242–e250. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M. Effect of HBM Rehabilitation Exercises on Depression, Anxiety and Health Belief in Elderly Patients with Osteoporotic Fracture. Psychiatr. Danub. 2017, 29, 466–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleland, J.; Tan, E.C.P.; Tham, K.Y.; Low-Beer, N. How Covid-19 opened up questions of sociomateriality in healthcare education. Adv. Heal. Sci. Educ. 2020, 25, 479–482. [Google Scholar] [CrossRef]
- Tachfouti, N.; Slama, K.; Berraho, M.; Nejjari, C. The impact of knowledge and attitudes on adherence to tuberculosis treatment: A case-control study in a Moroccan region. Pan Afr. Med. J. 2012, 12, 12. [Google Scholar]
- Zhong, B.-L.; Luo, W.; Li, H.-M.; Zhang, Q.-Q.; Liu, X.-G.; Li, W.-T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef]
- Chow, S.; Shao, J.W.H. Sample Size Calculations in Clinical Research, 2nd ed.; Chapman & Hall/CRC Biostatistics Series: Boca Raton, FL, USA, 2008. [Google Scholar]
- Taherdoost, H. Validity and Reliability of the Research Instrument; How to Test the Validation of a Questionnaire/Survey in a Research. SSRN Electron. J. 2016, 5. [Google Scholar] [CrossRef]
- National Institute of Statistic Geography and Informatics Household Income and Expenses [Ingresos y Gastos de los Hogares]. Available online: https://www.inegi.org.mx/temas/ingresoshog/ (accessed on 20 July 2020).
- STATA. Structural Equation Modeling Reference Manual Release 13, 13th ed.; A Stata Press Publication: College Station, TX, USA, 2013. [Google Scholar]
- Buis, M. Direct and indirect effects in a logit model. Stata J. Promot. Commun. Stat. Stata 2010, 10, 11–29. [Google Scholar] [CrossRef] [Green Version]
- Nussbaumer-Streit, B.; Mayr, V.; Dobrescu, A.I.; Chapman, A.; Persad, E.; Klerings, I.; Wagner, G.; Siebert, U.; Christof, C.; Zachariah, C.; et al. Quarantine alone or in combination with other public health measures to control COVID-19: A rapid review. Cochrane Database Syst. Rev. 2020, 4, D013574. [Google Scholar] [CrossRef]
- Fang, Y.; Nie, Y.; Penny, M. Transmission dynamics of the COVID-19 outbreak and effectiveness of government interventions: A data-driven analysis. J. Med. Virol. 2020, 92, 645–659. [Google Scholar] [CrossRef] [Green Version]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and Social Isolation as Risk Factors for Mortality. Perspect. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef] [Green Version]
- Plagg, B.; Engl, A.; Piccoliori, G.; Eisendle, K. Prolonged social isolation of the elderly during COVID-19: Between benefit and damage. Arch. Gerontol. Geriatr. 2020, 89, 104086. [Google Scholar] [CrossRef]
- Bouillon-Minois, J.-B.; Lahaye, C.; Dutheil, F. Coronavirus and quarantine: Will we sacrifice our elderly to protect them? Arch. Gerontol. Geriatr. 2020, 90, 104118. [Google Scholar] [CrossRef] [PubMed]
- De Leo, D.; Trabucchi, M. COVID-19 and the Fears of Italian Senior Citizens. Int. J. Env. Res. Public Health 2020, 17, 3572. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Chen, Y.; Lin, R.; Han, K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J. Infect. 2020, 80, e14–e18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bello-Chavolla, O.Y.; Rojas-Martinez, R.; Aguilar-Salinas, C.A.; Hernández-Avila, M. Epidemiology of diabetes mellitus in Mexico. Nutr. Rev. 2017, 75, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Ruilope, L.M.; Filho, A.N.; Nadruz, W.; Rosales, F.R.; Verdejo-Paris, J. Obesity and hypertension in Latin America: Current perspectives. Hipertens. Y Riesgo Vasc. 2018, 35, 70–76. [Google Scholar] [CrossRef]
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Patidar, R.; Younis, K.; Desai, P.; Hosein, Z.; Padda, I.; Mangat, J.; Altaf, M. Comorbidity and its Impact on Patients with COVID-19. SN Compr. Clin. Med. 2020, 2, 1069–1076. [Google Scholar] [CrossRef]
- Zhou, X.; Zhu, J.; Xu, T. Clinical characteristics of coronavirus disease 2019 (COVID-19) patients with hypertension on renin–angiotensin system inhibitors. Clin. Exp. Hypertens. 2020, 42, 656–660. [Google Scholar] [CrossRef]
- Guo, Y.-R.; Cao, Q.-D.; Hong, Z.-S.; Tan, Y.-Y.; Chen, S.-D.; Jin, H.-J.; Tan, K.-S.; Wang, D.Y.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak—An update on the status. Mil. Med. Res. 2020, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Mielck, A.; Vogelmann, M.; Leidl, R. Health-related quality of life and socioeconomic status: Inequalities among adults with a chronic disease. Health Qual. Life Outcomes 2014, 12, 58. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Jung, M. Associations between media use and health information-seeking behavior on vaccinations in South Korea. BMC Public Health 2017, 17, 700. [Google Scholar] [CrossRef]
- Lee, S.-M.; Kim, H.-N.; Lee, J.-H.; Kim, J.-B. Association between maternal and child oral health and dental caries in Korea. J. Public Health 2018, 27, 219–227. [Google Scholar] [CrossRef] [Green Version]
- Soler-Vila, H.; Lopez-Garcia, E.; Banegas, J.R.; Rodríguez-Artalejo, F.; García-Esquinas, E.; León-Muñoz, L.M. Contribution of health behaviours and clinical factors to socioeconomic differences in frailty among older adults. J. Epidemiol. Community Health 2015, 70, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Jiang, H.; Li, M.; Lu, Y.; Liu, K.; Sun, X. The Mediating Role of Self-Efficacy in Shaping Self-Management Behaviors Among Adults with Type 2 Diabetes. Worldviews Evid. Based Nurs. 2019, 16, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Lipman, S.A.; Burt, S.A. Self-reported prevalence of pests in Dutch households and the use of the health belief model to explore householders’ intentions to engage in pest control. PLoS ONE 2017, 12, e0190399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Usuwa, I.S.; Akpa, C.O.; Umeokonkwo, C.D.; Umoke, M.; Oguanuo, C.S.; Olorukooba, A.A.; Bamgboye, E.A.; Balogun, M.S. Knowledge and risk perception towards Lassa fever infection among residents of affected communities in Ebonyi State, Nigeria: Implications for risk communication. BMC Public Health 2020, 20, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, E.D.; Tapp, R.J.; Magliano, D.J.; Shaw, J.E.; Zimmet, P.Z.; Oldenburg, B. Health behaviours, socioeconomic status and diabetes incidence: The Australian Diabetes Obesity and Lifestyle Study (AusDiab). Diabetologia 2010, 53, 2538–2545. [Google Scholar] [CrossRef] [Green Version]
- Lowcock, E.C.; Rosella, L.C.; Foisy, J.; McGeer, A.; Crowcroft, N.S. The Social Determinants of Health and Pandemic H1N1 2009 Influenza Severity. Am. J. Public Health 2012, 102, e51–e58. [Google Scholar] [CrossRef]
- Ross, C.E.; Mirowsky, J. Sex differences in the effect of education on depression: Resource multiplication or resource substitution? Soc. Sci. Med. 2006, 63, 1400–1413. [Google Scholar] [CrossRef]
- Montez, J.K.; Barnes, K. The Benefits of Educational Attainment for U.S. Adult Mortality: Are they Contingent on the Broader Environment? Popul. Res. Policy Rev. 2015, 35, 73–100. [Google Scholar] [CrossRef]
- Durham, D.P.; Casman, E.A. Incorporating individual health-protective decisions into disease transmission models: A mathematical framework. J. R. Soc. Interface 2011, 9, 562–570. [Google Scholar] [CrossRef] [Green Version]
- Klemm, C.; Hartmann, T.; Das, E. Fear-Mongering or Fact-Driven? Illuminating the Interplay of Objective Risk and Emotion-Evoking Form in the Response to Epidemic News. Health Commun. 2017, 34, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, T.; Bardo, A.R.; Cummins, P.A.; Millar, R.J.; Sahoo, S.; Liu, D. The Roles of Education, Literacy, and Numeracy in Need for Health Information during the Second Half of Adulthood: A Moderated Mediation Analysis. J. Health Commun. 2019, 24, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Tang, K. Combating COVID-19: Health equity matters. Nat. Med. 2020, 26, 458. [Google Scholar] [CrossRef] [PubMed]
- Hitczenko, M. The influence of gender and income on the household division of financial responsibility. Res. Dep. Work. Pap. 2016, 16–20. [Google Scholar]
- Hill, M.A.; King, E.M. Women’s education and economic well-being. Fem. Econ. 1995, 1, 21–46. [Google Scholar] [CrossRef]
- Shoaib, M.; Saeed, Y. Education and women’s empowerment at household level: A case study of women in rural Chiniot, Pakistan. Acad. Res. Int. 2015, 2, 519–526. [Google Scholar]
- Gillam, S.J. Understanding the uptake of cervical cancer screening: The contribution of the health belief model. Br. J. Gen. Pract. 1991, 41, 510–513. [Google Scholar]
- Funk, S.; Salathé, M.; Jansen, V.A.A. Modelling the influence of human behaviour on the spread of infectious diseases: A review. J. R. Soc. Interface 2010, 7, 1247–1256. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 1. Compared to other people, how likely are you to get COVID-19? |
| (a) Very high |
| (b) High |
| (c) Low |
| (d) Very low |
| 2. How severe do you think COVID-19 infection is? |
| (a) Not at all serious |
| (b) Slightly serious |
| (c) Moderately serious |
| (d) Severely serious |
| 3. Do you know what the main symptoms of this infection are? |
| (a) No |
| (b) Yes, mention them: ____ |
| 4. Which age group has the greatest chance of complications if they get COVID-19? |
| (a) Children |
| (b) Young adult |
| (c) Adults |
| (d) Older adults |
| 5. Have you taken any steps to prevent COVID-19 contagion? |
| (a) No |
| (b) Yes, mention them: ____ |
| 6. What has been your main source of COVID-19 information? |
| (a) Television |
| (b) Radio |
| (c) Newspaper |
| (d) Family and friends |
| (e) Web/social media |
| (f) Other_____ |
| Characteristic | ||
|---|---|---|
| Age mean (± sd *) | 72.9 | (±8.0) |
| n | (%) | |
| Sex | ||
| Men | 91 | 23.9 |
| Women | 289 | 76.1 |
| IL ** | ||
| Low | 168 | 44.2 |
| Middle | 212 | 55.8 |
| Years of schooling | ||
| <3 | 74 | 19.5 |
| 3–6 | 58 | 15.3 |
| 7–8 | 83 | 21.8 |
| 9–10 | 69 | 18.1 |
| >10 | 96 | 25.3 |
| Symptoms of COVID-19 | ||
| Fever | 220 | 57.9 |
| Cough | 179 | 47.1 |
| Tiredness | 41 | 10.8 |
| Breathing difficulties | 125 | 32.9 |
| Flue/sore throat | 131 | 34.5 |
| Headache | 107 | 28.2 |
| Other | 87 | 22.9 |
| Did not know any of the symptoms | 46 | 12.1 |
| Age group at highest risk of COVID-19 complications | ||
| Children | 22 | 5.8 |
| Young adults | 2 | 0.5 |
| Middle-aged adults | 18 | 4.7 |
| Older adults | 264 | 69.5 |
| All age groups equally | 74 | 19.5 |
| Sources of information on COVID-19 | ||
| Television | 257 | 67.6 |
| Radio | 115 | 30.3 |
| Newspaper/magazines | 53 | 13.9 |
| Web/Social-Media | 44 | 11.6 |
| Family/friends | 60 | 15.8 |
| Stay-at- Home No | Stay-at- Home Yes | OR | (95% CI) | p-Value | |
|---|---|---|---|---|---|
| Characteristic | |||||
| Age mean (± sd *) | 72.8 (±7.8) | 73.0 (±8.1) | 1.00 | (0.97, 1.03) | 0.875 |
| n (%) | n (%) | ||||
| Sex | |||||
| Men | 45 (49.5) | 46 (50.6) | 1 (Reference) ** | ||
| Women | 132 (45.7) | 157 (54.3) | 1.16 | (0.73, 1.86) | 0.529 |
| IL *** | |||||
| Low | 106 (63.1) | 62 (36.9) | 1 (Reference) ** | ||
| Middle | 71 (33.5) | 141 (66.5) | 3.40 | (2.22, 5.19) | <0.001 |
| Years of schooling | |||||
| <3 | 50 (67.6) | 24 (32.4) | 1 (Reference) ** | ||
| 3–6 | 21 (36.2) | 37 (63.8) | 3.67 | (1.78, 7.57) | <0.001 |
| 7–8 | 44 (53.0) | 39 (47.0) | 1.85 | (0.96, 3.54) | 0.064 |
| 9–10 | 24 (34.8) | 45 (65.2) | 3.91 | (1.95, 7.82) | <0.001 |
| >10 | 38 (39.6) | 58 (60.4) | 3.18 | (1.68, 6.01) | <0.001 |
| Symptoms of COVID-19 | |||||
| Fever a | 90 (40.9) | 130 (59.1) | 1.72 | (1.14, 2.60) | 0.010 |
| Cough b | 76 (42.5) | 103 (57.5) | 1.37 | (0.91, 2.05) | 0.129 |
| Tiredness c | 19 (46.3) | 22 (53.7) | 1.01 | (0.53, 1.94) | 0.974 |
| Breathing difficulty d | 60 (48.0) | 65 (52.0) | 0.92 | (0.60, 1.41) | 0.697 |
| Flue/sore throat e | 65 (49.6) | 66 (50.4) | 0.83 | (0.54,1.27) | 0.389 |
| Headache f | 46 (43.0) | 61 (57.0) | 1.22 | (0.78, 1.92) | 0.380 |
| Did not know any of the symptoms g | 25 (54.4) | 21 (45.7) | 0.70 | (0.38, 1.30) | 0.262 |
| Age group with most COVID-19 complications | |||||
| Other age groups | 63 (54.3) | 53 (45.7) | 1 (Reference) ** | ||
| Old adults | 114 (43.2) | 150 (56.8) | 1.56 | (1.01, 2.43) | 0.046 |
| Sources of information on COVID-19 | |||||
| Television | 114 (44.4) | 143 (55.6) | 1.32 | (0.86, 2.03) | 0.210 |
| Radio | 70 (60.9) | 45 (39.1) | 0.43 | (0.28, 0.68) | <0.001 |
| Newspaper/magazines | 27 (50.9) | 26 (49.1) | 0.82 | (0.46, 1.46) | 0.493 |
| Web/Social media | 10 (22.7) | 34 (77.3) | 3.36 | (1.61, 7.02) | <0.001 |
| Family/friends | 27 (45.0) | 33 (55.0) | 1.08 | (0.62, 1.88) | 0.789 |
| Perception | Stay-at- Home No n (Row %) | Stay-at- Home Yes n (Row %) | Total n (Column %) | OR | (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Perceived Susceptibility | ||||||
| Very low | 25 (61.0) | 16 (39.0) | 41 (10.8) | 1 (Reference) * | ||
| Low | 79(47.9) | 86(52.1) | 165 (43.4) | 1.70 | (0.85, 3.42) | 0.136 |
| High | 58 (43.6) | 75 (56.4) | 133 (35.0) | 2.02 | (0.99, 4.13) | 0.054 |
| Very High | 15 (36.6) | 26 (63.4) | 41 (10.8) | 2.70 | (1.11, 6.62) | 0.029 |
| Perceived Severity | ||||||
| Very low | 27 (60.0) | 18 (40.0) | 45 (11.8) | 1 (Reference) * | ||
| Low | 52 (63.4) | 30 (36.6) | 82 (21.6) | 0.87 | (0.41, 1.83) | 0.704 |
| High | 56 (42.4) | 76 (57.6) | 132 (34.8) | 2.04 | (1.02, 4.05) | 0.043 |
| Very High | 42 (34.7) | 79 (65.3) | 121 (31.8) | 2.82 | (1.40, 5.71) | 0.004 |
| Variable | β Coefficient | (95% CI) 1 | p-Value |
| Income Level | |||
| Total | |||
| Middle vs. Low | 1.222 | (0.813, 1.632) | 0.001 |
| Indirect | |||
| 0.184 | (0.040, 0.329) | 0.013 | |
| Direct | |||
| 1.038 | (0.600, 1.476) | 0.001 | |
| Education level (years of schooling) | β Coefficient | (95% CI) 1 | p-Value |
| Total | |||
| 3–6 vs. <3 | 1.300 | (0.553, 2.048) | 0.001 |
| Indirect | |||
| 0.161 | (−0.043, 0.365) | 0.122 | |
| Direct | |||
| 1.300 | (0.553, 2.048) | 0.001 | |
| Total | |||
| 7–8 vs. <3 | 0.613 | (0.091, 1.136) | 0.021 |
| Indirect | |||
| 0.061 | (−0.112, 0.233) | 0.491 | |
| Direct | |||
| 0.553 | (0.024, 1.081) | 0.040 | |
| Total | |||
| 9–10 vs. <3 | 1.363 | (0.621, 2.105) | 0.001 |
| Indirect | |||
| 0.131 | (−0.040, 0.302) | 0.132 | |
| Direct | |||
| 1.231 | (0.501, 1.961) | 0.001 | |
| Total | |||
| >10 vs. <3 | 1.157 | (0.461, 1.852) | 0.001 |
| Indirect | |||
| 0.175 | (0.029, 0.321) | 0.019 | |
| Direct | |||
| 0.982 | (0.298, 1.675) | 0.005 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Irigoyen-Camacho, M.E.; Velazquez-Alva, M.C.; Zepeda-Zepeda, M.A.; Cabrer-Rosales, M.F.; Lazarevich, I.; Castaño-Seiquer, A. Effect of Income Level and Perception of Susceptibility and Severity of COVID-19 on Stay-at-Home Preventive Behavior in a Group of Older Adults in Mexico City. Int. J. Environ. Res. Public Health 2020, 17, 7418. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207418
Irigoyen-Camacho ME, Velazquez-Alva MC, Zepeda-Zepeda MA, Cabrer-Rosales MF, Lazarevich I, Castaño-Seiquer A. Effect of Income Level and Perception of Susceptibility and Severity of COVID-19 on Stay-at-Home Preventive Behavior in a Group of Older Adults in Mexico City. International Journal of Environmental Research and Public Health. 2020; 17(20):7418. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207418
Chicago/Turabian StyleIrigoyen-Camacho, Maria Esther, Maria Consuelo Velazquez-Alva, Marco Antonio Zepeda-Zepeda, Maria Fernanda Cabrer-Rosales, Irina Lazarevich, and Antonio Castaño-Seiquer. 2020. "Effect of Income Level and Perception of Susceptibility and Severity of COVID-19 on Stay-at-Home Preventive Behavior in a Group of Older Adults in Mexico City" International Journal of Environmental Research and Public Health 17, no. 20: 7418. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207418