How Does the Execution of the Pilates Method and Therapeutic Exercise Influence Back Pain and Postural Alignment in Children Who Play String Instruments? A Randomized Controlled Pilot Study


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
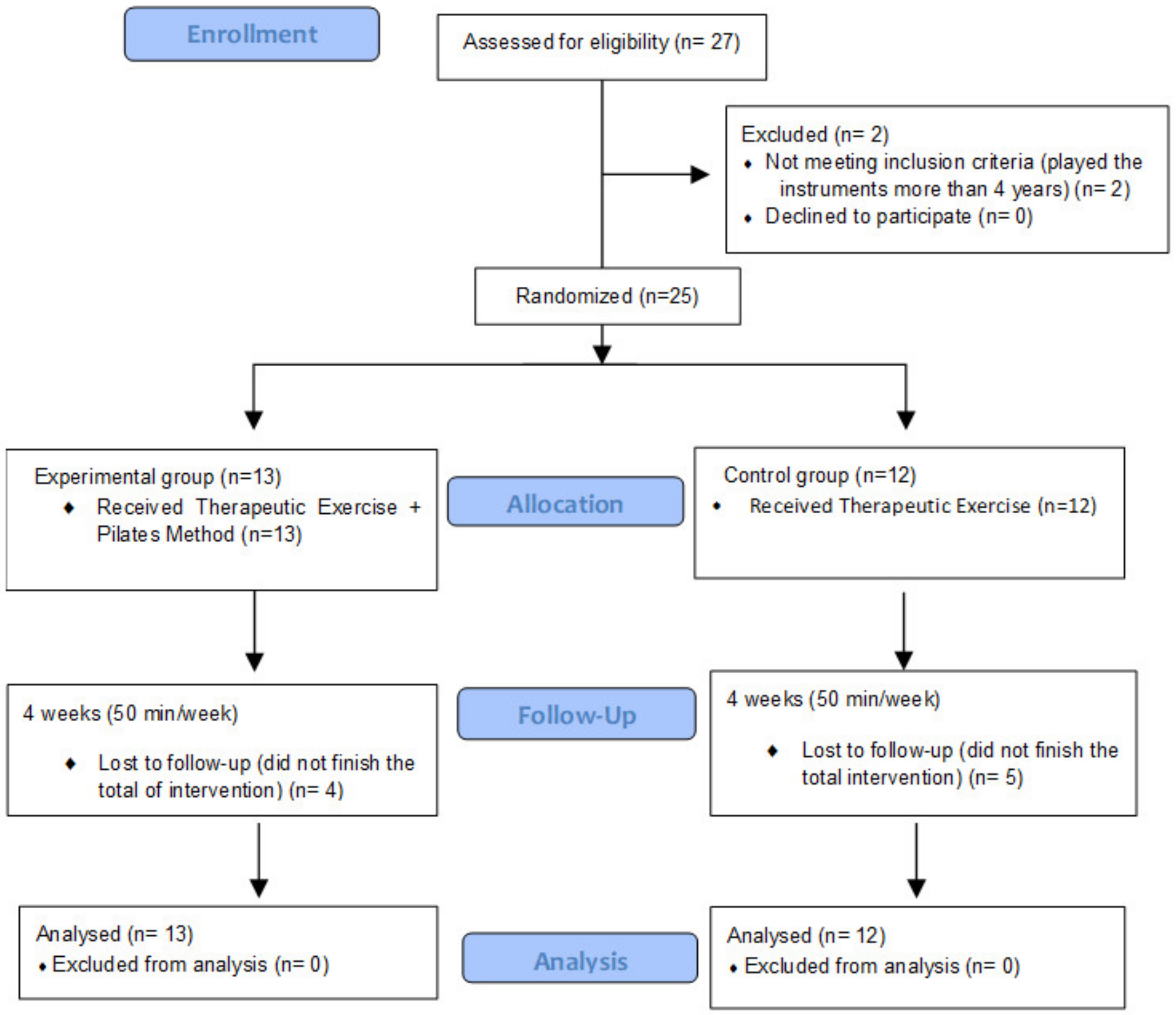
2.1. Study Design
2.2. Participants
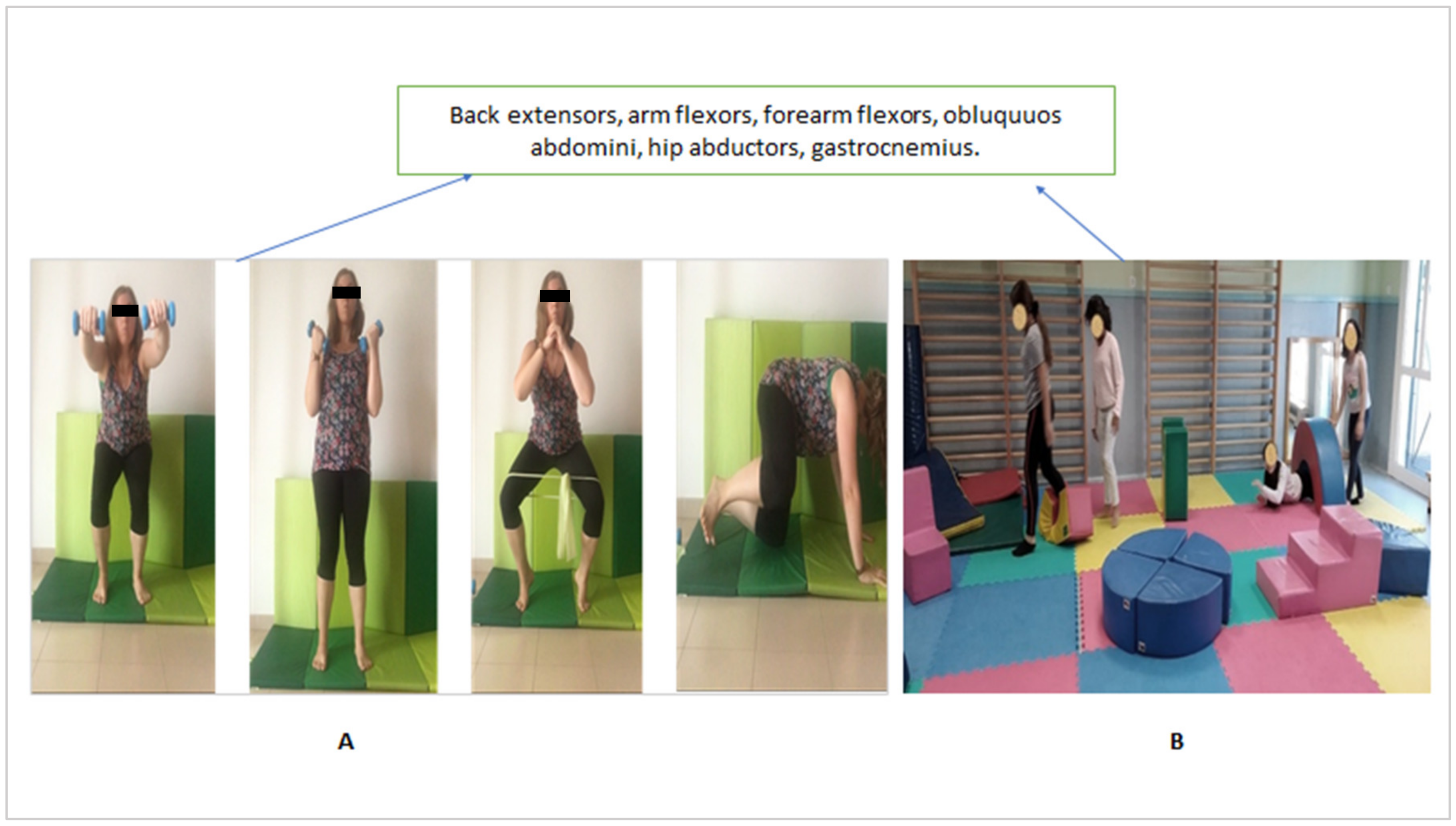
2.3. Interventions
2.4. Assessments, Study Variables, and Measuring Instruments
2.4.1. Study Variables and Measuring Instruments
First Outcome Measurement: Back Pain Perceived before, during, and after Practicing with the String Instrument
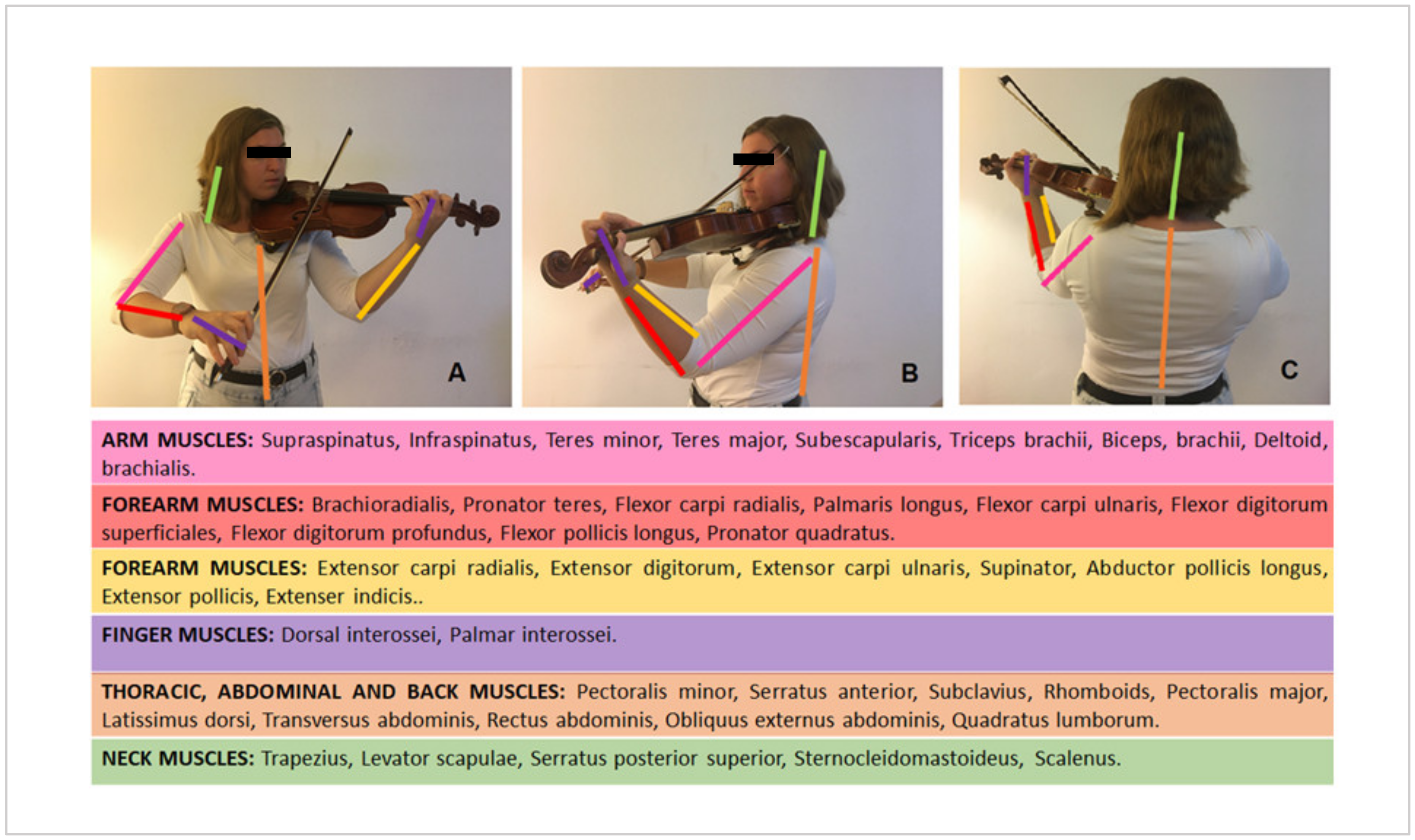
Second Outcome Measurement: Postural Alignment: Shoulders and Hips
2.5. Statistical Analysis
3. Results
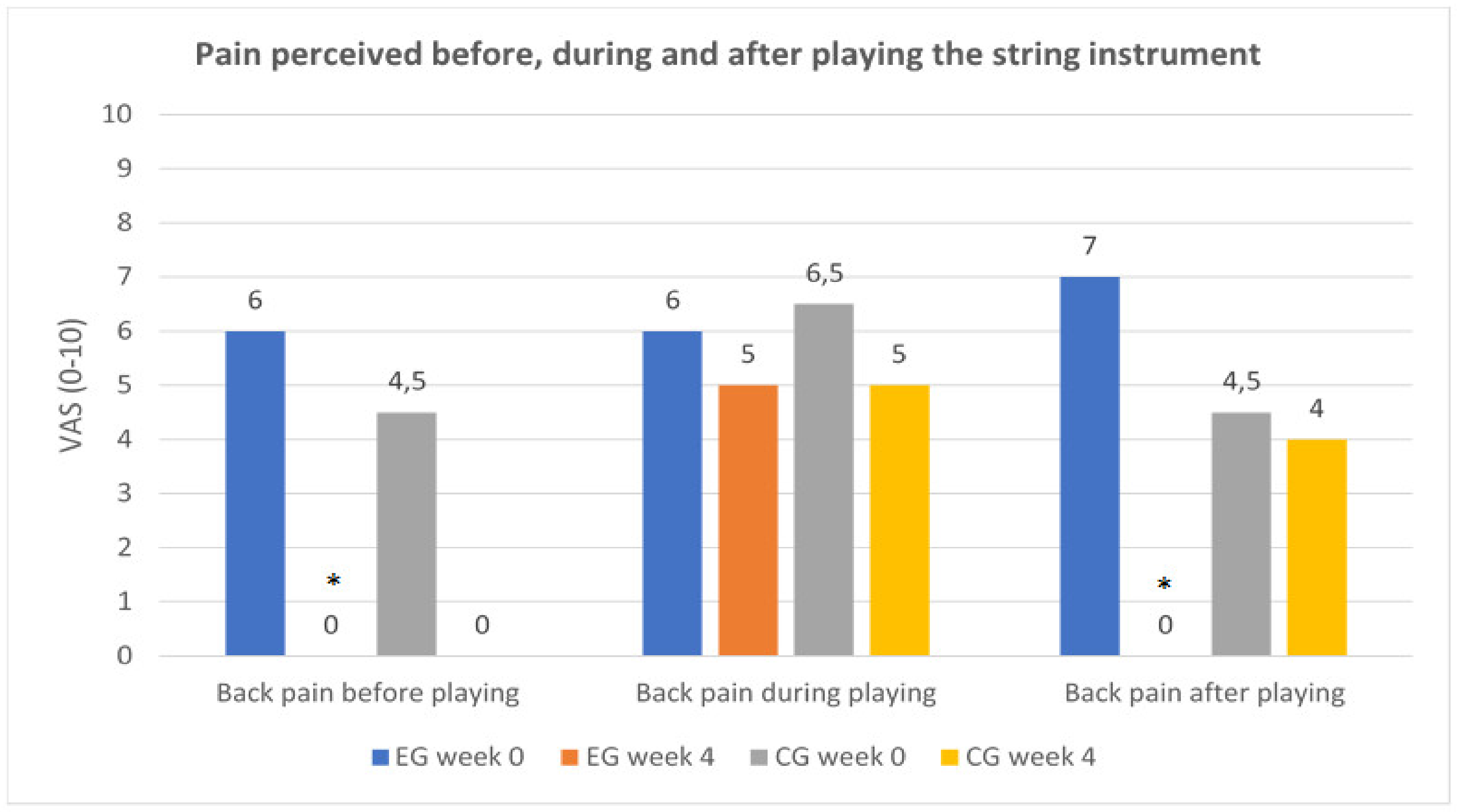
3.1. Primary Outcomes: Pain Perceived before, during, and after Practicing with the String Instrument
3.2. Secondary Outcomes
3.3. Third Outcomes: Correlation of the Experimental Group Post–Pre-Treatment Difference in Back Pain (Pre–During–After) with Age and Time Playing the Instrument
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sardà, R.E. En Forma. Ejercicios para Músicos, 1st ed.; Ediciones Paidós Ibérica: Barcelona, Spain, 2003. [Google Scholar]
- Echan, C.; Ackermann, B.J. Evidence-informed physical therapy management of performance-related musculoskeletal disorders in musicians. Front. Psychol. 2014, 5, 706. [Google Scholar] [CrossRef] [Green Version]
- Hoenig, K.; Müller, C.; Herrnberger, B.; Sim, E.J.; Spitzer, M.; Ehret, G.; Kiefer, M. Neuroplasticity of semantic representations for musical instruments in professional musicians. Neuroimage 2011, 56, 1714–1725. [Google Scholar] [CrossRef] [PubMed]
- Brandfonbrener, A. Etiologies of medical problems in performing artists. In Performing Arts Medicine; Science & Medicine: Narberth, PA, USA, 2010; p. 25. [Google Scholar]
- Ackermann, B.J.; Driscoll, T.; Kenny, D.T. Musculoskeletal pain and injury in profesional orchestral musicians in Australia. Med. Probl. Perform. Artist 2012, 27, 181–187. [Google Scholar] [CrossRef]
- Leaver, R.; Harris, E.C.; Palmer, K.T. Musculoskeletal pain in elite professional musicians from British symphony orchestras. Occup. Med. 2011, 61, 549–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paarup, H.M.; Baelum, J.; Holm, J.W.; Manniche, C.; Wedderkopp, N. Prevalence and consequences of musculoskeletal symptoms in symphony orchestra musicians vary by gender: A cross-sectional study. BMC Musculoskelet. Disord. 2011, 12, 223. [Google Scholar] [CrossRef] [Green Version]
- Cerveró, C.G.; Ruiz, J.M.; Sanchis, L.R.; Ros, C.R. Pain Perception in Clarinetists with Playing-Related Pain After Implementing a Specific Exercise Program. Med. Probl. Perform. Artist 2018, 33, 238–242. [Google Scholar] [CrossRef]
- Gasenzer, E.R.; Klumpp, M.J.; Pieper, D.; Neugebauer, E.A.M. The prevalence of chronic pain in orchestra musicians. Ger. Med. Sci. 2017, 15, 1–9. [Google Scholar] [CrossRef]
- Ioannou, C.I.; Altenmüller, E. Approaches to and Treatment Strategies for Playing-Related Pain Problems Among Czech Instrumental Music Students: An Epidemiological Study. Med. Probl. Perform. Artist 2015, 30, 135–142. [Google Scholar] [CrossRef]
- Rensing, N.; Schemmann, H.; Zalpour, C. Musculoskeletal Demands in Violin and Viola Playing: A Literature Review. Med. Probl. Perform. Artist 2018, 33, 265–274. [Google Scholar] [CrossRef]
- Lee, H.S.; Park, H.Y.; Yoon, J.O.; Kim, J.S.; Chun, J.M.; Aminata, I.W.; Cho, W.J.; Jeon, I.H. Musicians’ Medicine: Musculoskeletal Problems in String Players. Clin. Orthop. Surg. 2013, 5, 155–160. [Google Scholar] [CrossRef] [Green Version]
- Moraes, G.F.D.S.; Antunes, A.P. Musculo skeletal disorders in professional violinists and violists. Systematic review. Acta Ortop. Bras. 2012, 20, 43–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovero, O.; Kononen, M.; Pirinen, S. The effect of violin playing on the bony facial structures in adolescents. Eur. J. Orthod. 1997, 19, 369–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, G.; Wang, K.; Demaree, C.J.; Jiang, J.S.; Cheung, M.; Bechara, C.F.; Lin, P.H. A Prospective Evaluation of Duplex Ultrasound for Thoracic Outlet Syndrome in High-Performance Musicians Playing Bowed String Instruments. Diagnostics 2018, 8, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kochem, F.B.; Silva, J.G. Prevalence of Playing-related Musculoskeletal Disorders in String Players: A Systematic Review. J. Manip. Physiol. Ther. 2018, 41, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Nordio, S.; Bernitsas, E.; Meneghello, F.; Palmer, K.; Stabile, M.R.; Dipietro, L.; Di Stadio, A. Expiratory and phonation times as measures of disease severity in patients with Multiple Sclerosis. A case-control study. Mult. Scler. Relat. Disord. 2018, 23, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Zatorre, R.J.; Chen, J.L.; Penhune, V.B. When the brain plays music: Auditory-motor interactions in music perception and production. Nat. Rev. Neurosci. 2007, 8, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Joret, M.E.; Germeys, F.; Gidron, Y. Cognitive inhibitory control in children following early childhood music education. Musicae Sci. 2017, 21, 303–315. [Google Scholar] [CrossRef]
- Hennessy, S.L.; Sachs, M.E.; Ilari, B.; Habibi, A. Effects of Music Training on Inhibitory Control and Associated Neural Networks in School-Aged Children: A Longitudinal Study. Front. Neurosci. 2019, 13, 1080. [Google Scholar] [CrossRef]
- Degé, F.; Schwarzer, G. The Effect of a Music Program on Phonological Awareness in Preschoolers. Front. Psychol. 2011, 2, 124. [Google Scholar] [CrossRef] [Green Version]
- Rydeard, R.; Leger, A.; Smith, D. Pilates-based therapeutic exercise: Effect on subjects with nonspecific chronic low back pain and functional disability: A randomized controlled trial. J. Orthop. Sports Phys. Ther. 2006, 36, 472–484. [Google Scholar] [CrossRef] [Green Version]
- Britto, M.T.; Slap, G.B.; DeVellis, R.F.; Hornung, R.W.; Atherton, H.D.; Knopf, J.M.; DeFriese, G.H. Specialists Understanding of the Health Care Preferences of Chronically Ill Adolescents. J. Adolesc. Health 2007, 40, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Mah, J.K.; Tough, S.; Fung, T.; Douglas-England, K.; Verhoef, M. Adolescent quality of life and satisfaction with care. J. Adolesc. Health 2006, 38, 607. [Google Scholar] [CrossRef] [PubMed]
- Ávalos, F.S.; Florensa, S.G.T. La Columna vertebral del niño en crecimiento: Desviaciones. Offarm 2011, 30, 66–71. [Google Scholar]
- Bridwell, K. Columna Vertebral. Available online: https://www.spineuniverse.com/espanol/anatomia/columna-vertebral (accessed on 24 September 2020).
- González-Gálvez, N.; Marcos-Pardo, P.J.; Trejo-Alfaro, H.; Vaquero-Cristóbal, R. Effect of 9-month Pilates program on sagittal spinal curvatures and hamstring extensibility in adolescents: Randomised controlled trial. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Taylor, N.F.; Dodd, K.J.; Shields, N.; Bruder, A. Therapeutic exercise in physiotherapy practice is beneficial: A summary of systematic reviews 2002-2005. Aust. J. Physiother. 2007, 53, 7–16. [Google Scholar] [CrossRef] [Green Version]
- Lundborg, B.; Grooten, W.J.A. Resistance training for professional string musicians: A prospective intervention study. Med. Probl. Perform. Artist 2018, 33, 102–110. [Google Scholar] [CrossRef]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Jönsson, T.; Hansson, E.E.; Thorstensson, C.A.; Eek, F.; Bergman, P.; Dahlberg, L.E. The effect of education and supervised exercise on physical activity, pain, quality of life and self-efficacy—An intervention study with a reference group. BMC Musculoskelet Disord 2018, 19, 198. [Google Scholar] [CrossRef]
- Moreno, R.C.; Morera, C.F. Manual Completo de Pilates Suelo; Paidotribo: Barcelona, Spain, 2009. [Google Scholar]
- Campos, R.R.; Dias, J.M.; Pereira, L.M.; Obara, K.; Barreto, M.S.; Siva, M.F.; Mazuquin, B.F.; Christofaro, D.G.; Fernandes, R.A.; Iversen, M.D.; et al. The effect of the Pilates method on the physical conditioning of healthy subjects: A systematic review with meta-analysis. J. Sports Med. Phys. Fit. 2015, 56, 864–873. [Google Scholar]
- Kloubec, J.A. Pilates for improvement ofmuscle endurance, flexibility, balance, and posture. J. Strength Cond. Res. 2010, 24, 661–667. [Google Scholar] [CrossRef]
- Geremia, J.M.; Iskiewicz, M.M.; Marschner, R.A.; Lehnen, T.E.; Lehnen, A.M. Effect of a physical training program using the Pilates method on flexibility in elderly subjects. AGE 2015, 37, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Lopes, S.; Correia, C.; Félix, G.; Lopes, M.; Cruz, A.; Ribeiro, F. Immediate effects of Pilates based therapeutic exercise on postural control of young individuals with non-specific low back pain: A randomized controlled trial. Complement. Ther. Med. 2017, 34, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Kuntze, G.; Nesbitt, C.; Whittaker, J.L.; Nettel-Aguirre, A.; Toomey, C.; Esau, S.; Doyle-Baker, P.K.; Shank, J.; Brooks, J.; Benseler, S.; et al. Exercise Therapy in Juvenile Idiopathic Arthritis: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2018, 99, 178–193. [Google Scholar] [CrossRef] [PubMed]
- Klepper, S.; Mano Khong, T.T.; Klotz, R.; Gregorek, A.O.; Chan, Y.C.; Sawade, S. Effects of Structured Exercise Training in Children and Adolescents with Juvenile Idiopathic Arthritis. Pediatr. Phys. Ther. 2019, 31, 3–21. [Google Scholar] [CrossRef] [PubMed]
- García-Soidán, J.L.; Giraldez, V.A.; Zagalaz, J.C.; Lara-Sánchez, A.J. Does pilates exercise increase physical activity, quality of life, latency, and sleep quantity in middle-aged people? Percept. Mot. Skills 2014, 119, 838–850. [Google Scholar] [CrossRef]
- Mikkelsson, L.O.; Nupponen, H.; Kaprio, J.; Kautiainen, H.; Mikkelsson, M.; Kujala, U.M. Adolescent flexibility, endurance strength, and physical activity as predictors of adult tension neck, low back pain, and knee injury: A 25 year follow up study. Br. J. Sports Med. 2006, 40, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Cibinello, F.U.; Neves, J.C.D.J.; Carvalho, M.Y.L.; Valenciano, P.J.; Fujisawa, D.S. Effect of Pilates Matwork Exercises on Posterior Chain Flexibility and Trunk Mobility in School Children: A Randomized Clinical Trial. J. Bodyw. Mov. Ther. 2020, 24, 176–181. [Google Scholar] [CrossRef]
- De Araújo, M.E.A.; Da Silva, E.B.; Mello, D.B.; Cader, S.A.; Salgado, A.S.I.; Dantas, E.H.M. The effectiveness of the Pilates method: Reducing the degree of non-structural scoliosis, and improving flexibility and pain in female college students. J. Bodyw. Mov. Ther. 2012, 16, 191–198. [Google Scholar] [CrossRef]
- Aladro-Gonzalvo, A.R.; Araya-Vargas, G.A.; Machado-Díaz, M.; Salazar-Rojas, W. Pilates-based exercise for persistent, non-specific low back pain and associated functional disability: A meta-analysis with meta-regression. J. Bodyw. Mov. Ther. 2013, 17, 125–136. [Google Scholar] [CrossRef]
- Lim, E.C.W.; Poh, R.L.C.; Low, A.Y.; Wong, W.P. Effects of pilates-based exercises on pain and disability in individuals with persistent nonspecific low back pain: A systematic review with meta-analysis. J. Orthop. Sports Phys. Ther. 2011, 41, 70–80. [Google Scholar] [CrossRef]
- Suh, J.; Choi, H.S.; Kwon, A.; Chae, H.W.; Eom, S.; Kim, H.S. Once-weekly supervised combined training improves neurocognitive and psychobehavioral outcomes in young patients with type 1 diabetes mellitus. J. Pediatr. Endocrinol. Metab. 2019, 32, 1–10. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Demetriou, Y.; Reimers, A.K.; Alesi, M.; Scifo, L.; Borrego, C.C.; Monteiro, D.; Kelso, A. Effects of school-based interventions on motivation towards physical activity in children and adolescents: Protocol for a systematic review. Syst. Rev. 2019, 8, 113. [Google Scholar] [CrossRef] [PubMed]
- Knuth, A.G.; Hallal, P.C. Temporal trends in physical activity: A systematic review. J. Phys. Act. Health 2009, 6, 548–559. [Google Scholar] [CrossRef] [PubMed]
- Hadders-Algra, M. Typical and atypical development of reaching and postural control in infancy. Dev. Med. Child Neurol. 2013, 55, 5–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Houdenhove, B.; Verheyen, L.; Pardaens, K.; Luyten, P.; Van Wambeke, P. Rehabilitation of decreased motor performance in patients with chronic fatigue syndrome: Should we treat low effort capacity or reduced effort tolerance? Clin. Rehabil. 2007, 21, 1121–1142. [Google Scholar] [CrossRef] [PubMed]
- Detsch, C.; Luz, A.M.H.; Candotti, C.T.; de Oliveira, D.S.; Lazaron, F.; Guimarães, L.K.; Schimanoski, P. Prevalence of postural changes in high school students in a city in southern Brazil. Pan Am. J. Public Health 2007, 21, 231–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ossipov, M.H.; Morimura, K.; Porreca, F. Descending pain modulation and chronification of pain. Curr. Opin. Support. Palliat. Care 2014, 8, 143–151. [Google Scholar] [PubMed] [Green Version]
- Infomed. Visual Analog Scale. Available online: http://www.sld.cu/galerias/pdf/sitios/rehabilitacion/eav_1.pdf (accessed on 24 September 2020).
- Huskisson, E.C. Measurement of pain. Lancet 1974, 304, 1127–1131. [Google Scholar] [CrossRef]
- Puig-Diví, A.; Escalona-Marfil, C.; Padullés-Riu, J.M.; Busquets, A.; Padullés-Chando, X.; Marcos-Ruiz, D. Validity and reliability of the Kinovea program in obtaining angles and distances using coordinates in 4 perspectives. PLoS ONE 2019, 14, e0216448. [Google Scholar] [CrossRef] [PubMed]
- Kaufman-Cohen, Y.; Ratzon, N.Z. Correlation between risk factors and musculoskeletal disorders among classical musicians. Occup. Med. 2011, 61, 90–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fishbein, M.; Middlestadt, S.E.; Ottati, V.; Straus, S. Medical problems among ICSOM musicians: Overview of a national survey. Med. Probl. Perform. Artist 1988, 3, 1–8. [Google Scholar]
- Grimmer, K.; Williams, M. Gender-age environmental associates of adolescent low back pain. Appl. Ergon. 2000, 31, 343–360. [Google Scholar] [CrossRef]
- Ludvig, D.; Preuss, R.; Larivière, C. The effect of extensible and non-extensible lumbar belts on trunk muscle activity and lumbar stiffness in subjects with and without low-back pain. Clin. Biomech. 2019, 67, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, T.M.; Terreri, M.T.; Silva, C.H.; Neto, M.B.; Pinto, R.M.; Natour, J.; Len, C.A. Effects of pilates exercises on health-related quality of life in individuals with juvenile idiopathic arthritis. Arch. Phys. Med. Rehabil. 2013, 94, 2093–2102. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Díaz, D.; Martínez-Amat, A.; Osuna-Pérez, M.C.; de La Torre-Cruz, M.J.; Hita-Contreras, F. Short- and long-term effects of a six-week clinical Pilates program in addition to physical therapy on postmenopausal women with chronic low back pain: A randomized controlled trial. Disabil. Rehabil. 2016, 38, 1300–1308. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.N.; Mann, S.; Juul-Kristensen, B.; Søgaard, K. Comparing the impact of specific strength training vs general fitness training on professional symphony orchestra musicians: A feasibility study. Med. Probl. Perform. Artist 2017, 32, 94–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, C.; Driscoll, T.; Ackermann, B. Development of a specific exercise programme for professional orchestral musicians. Inj. Prev. 2013, 19, 257–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kava, K.S.; Larson, C.A.; Stiller, C.H.; Maher, S.F. Trunk endurance exercise and the effect on instrumental performance: A preliminary study comparing Pilates exercise and a trunk and proximal upper extremity endurance exercise program. Music Perform. Res. 2010, 3, 1–30. [Google Scholar]
- Key, J. “The core”: Understanding it, and retraining its dysfunction. J. Bodyw. Mov. Ther. 2013, 17, 541–559. [Google Scholar] [CrossRef]
- Zheng, Y.; Ke, S.; Lin, C.; Li, X.; Liu, C.; Wu, Y.; Xin, W.; Ma, C.; Wu, S.; Wieczorek, A. Effect of core stability training monitored by rehabilitative ultrasound image and surface electromyogram in local core muscles of healthy people. Pain Res. Manag. 2019, 2019. [Google Scholar] [CrossRef] [Green Version]
- Schreiber, S.; Parent, E.C.; Moez, E.K.; Hedden, D.M.; Hill, D.L.; Moreau, M.; Lou, E.; Watkins, E.M.; Southon, S.C. Schroth physiotherapeutic scoliosis-specific exercises added to the standard of care lead to better cobb angle outcomes in adolescents with idiopathic scoliosis—an assessor and statistician blinded randomized controlled trial. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.L.; Tully, E.A.; Galea, M.P. Sagittal spinal posture after pilates-based exercise in healthy older adults. Spine 2009, 34, 1046–1051. [Google Scholar] [CrossRef]
- Emery, K.; de Serres, S.J.; McMillan, A.; Côté, J.N. The effects of a Pilates training program on arm-trunk posture and movement. Clin. Biomech. 2010, 25, 124–130. [Google Scholar] [CrossRef]
- Hornsby, E.; Johnston, L.M. Effect of Pilates Intervention on Physical Function of Children and Youth: A Systematic Review. Arch. Phys. Med. Rehabil. 2020, 101, 317–328. [Google Scholar] [CrossRef]
- Jago, R.; Jonker, M.L.; Missaghian, M.; Baranowski, T. Effect of 4 weeks of Pilates on the body composition of young girls. Prev. Med. 2006, 42, 177–180. [Google Scholar] [CrossRef]
- Jung, M.E.; Bourne, J.E.; Little, J.P. Where does HIT Fit? An Examination of the Affective Response to High-Intensity Intervals in Comparison to Continuous Moderate- and Continuous Vigorous-Intensity Exercise in the Exercise Intensity-Affect Continuum. PLoS ONE 2014, 9, e114541. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, B.R.R.; Santos, T.M.; Kilpatrick, M.; Pires, F.O.; Deslandes, A.C. Affective and enjoyment responses in high intensity interval training and continuous training: A systematic review and meta-analysis. PLoS ONE 2018, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, A.A.; Williams, C.A.; Weston, K.L.; Barker, A.R. Perceptual Responses to High- and Moderate-Intensity Interval Exercise in Adolescents. Med. Sci. Sports Exerc. 2018, 50, 1021–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, L.H.; Roemmich, J.N. Reducing sedentary behavior: Role in modifying physical activity. Exerc. Sport Sci. Rev. 2001, 29, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Timbedake, W.; Farmer-Dougan, V.A. Reinforcement in Applied Settings: Figuring Out Ahead of Time What Will Work. Psychol. Bull. 1991, 110, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Destrebecqz, A.; Cleeremans, A. Can sequence learning be implicit? New evidence with the process dissociation procedure. Psychon. Bull. Rev. 2001, 8, 343–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gheysen, F.; Fias, W. Dissociable neural systems of sequence learning. Adv. Cogn. Psychol. 2012, 8, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Candler, C.; Meeuwsen, H. Implicit learning in children with and without developmental coordination disorder. Am. J. Occup. Ther. 2002, 56, 429–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bixby, W.R.; Spalding, T.W.; Hatfield, B.D. Temporal dynamics and dimensional specificity of the affective response to exercise of varying intensity: Differing pathways to a common outcome. J. Sport Exerc. Psychol. 2001, 23, 171–190. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Intervention Protocols Examples |
|---|---|
| Therapeutic Exercise | Each 50-minute class was divided into warm-up, training, and stretching:
|
| Pilates Method and Therapeutic Exercise | Each 50 minute-class was divided into warm-up, training, and stretching:
|
| Experimental Group | Control Group | p-Value | |
|---|---|---|---|
| Female (%) | 61.54 | 75 | - |
| Male (%) | 38.46 | 25 | - |
| Age (years), mean (SD) | 13 (1.6) | 11.17 (0.72) | < 0.01 |
| Time playing the instrument(months), mean(SD) | 23.53 (11.66) | 34 (16.84) | 0.6 |
| Time spent playing the instrument per week (Monday- Friday), mean expressed in hours (SD) | 4 (0.32) | 4 (0.35) | 1 |
| Years of experience playing the instruments in the music school, mean (SD) | 2 (0.24) | 3 (0.29) | 0.6 |
| Music initiation age, mean (SD) | 10.2 (0.65) | 8.5 (0.53) | 0.04 |
| String instrument played: | |||
| Violin/viola n. (%) | 5 (38.46) | 4 (33.33) | - |
| Cello n. (%) | 4 (30.77) | 4 (33.33) | - |
| Double bass n. (%) | 4 (30.77) | 4 (33.33) | - |
| Self-report outcome median (IQR) | |||
| VAS (0–10) | |||
| -Back pain before playing | 6 (0, 8) | 4.50 (0, 9) | 0.7 |
| -Back pain during practice | 6 (0, 8) | 6.50 (0, 9) | 0.9 |
| -Back pain after playing | 7 (0, 8) | 4.50 (0, 9) | 0.6 |
| Measured outcome | |||
| median (IQR) | |||
| Kinovea (movement angles, degrees º) | |||
| -Shoulders | 2 (0, 6) | 1 (0, 5) | 0.6 |
| -Hips | 2 (0, 6) | 1 (0, 5) | 0.6 |
| Self-Report Outcome Median (IQR) VAS (0–10) | Experimental Group Week 0 | Experimental Group Week 4 | p-Value | Control Group Week 0 | Control Group Week 4 | p-Value |
|---|---|---|---|---|---|---|
| Back pain before playing | 6 (0,8) | 0 (0, 8) | 0.04 * | 4.50 (0, 9) | 0 (0, 7) | 0.08 |
| Back pain during practice | 6 (0, 8) | 5 (0, 7) | 0.24 | 6.50 (0,9) | 5 (0, 7) | 0.34 |
| Back pain after playing | 7 (0, 8) | 0 (0, 7) | 0.01 * | 4.50 (0,9) | 4 (0, 7) | 0.46 |
| Measured Outcome Median (IQR) Kinovea (Movement Angles, Degreesº) | Experimental Group Week 0 | Experimental Group Week 4 | p-Value | Control Group Week 0 | Control Group Week 4 | p-Value |
|---|---|---|---|---|---|---|
| -Shoulders | 2 (0, 6) | 2 (1, 4) | 0.09 | 1 (0, 5) | 0 (0, 2) | 0.7 |
| -Hips | 2 (0, 6) | 2 (0, 5) | 0.57 | 1 (0, 4) | 0 (0, 3) | 0.1 |
| Experimental Group’s Post–Pre-Treatment Difference | Age | Time Playing the Instrument |
|---|---|---|
| Back pain before playing the instrument | −0.59 * | −0.05 |
| Back pain during playing the instrument | 0.04 | 0.11 |
| Back pain after playing the instrument | −0.35 | −0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poncela-Skupien, C.; Pinero-Pinto, E.; Martínez-Cepa, C.; Zuil-Escobar, J.C.; Romero-Galisteo, R.P.; Palomo-Carrión, R. How Does the Execution of the Pilates Method and Therapeutic Exercise Influence Back Pain and Postural Alignment in Children Who Play String Instruments? A Randomized Controlled Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 7436. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207436
Poncela-Skupien C, Pinero-Pinto E, Martínez-Cepa C, Zuil-Escobar JC, Romero-Galisteo RP, Palomo-Carrión R. How Does the Execution of the Pilates Method and Therapeutic Exercise Influence Back Pain and Postural Alignment in Children Who Play String Instruments? A Randomized Controlled Pilot Study. International Journal of Environmental Research and Public Health. 2020; 17(20):7436. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207436
Chicago/Turabian StylePoncela-Skupien, Carolina, Elena Pinero-Pinto, Carmen Martínez-Cepa, Juan Carlos Zuil-Escobar, Rita Pilar Romero-Galisteo, and Rocío Palomo-Carrión. 2020. "How Does the Execution of the Pilates Method and Therapeutic Exercise Influence Back Pain and Postural Alignment in Children Who Play String Instruments? A Randomized Controlled Pilot Study" International Journal of Environmental Research and Public Health 17, no. 20: 7436. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207436