Effectiveness of Non-Pharmacological Interventions for Overweight or Obese Infertile Women: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection Criteria
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.2. Search Strategy and Data Extraction
2.2.1. Search Strategy
2.2.2. Selection of Studies
2.2.3. Data Extraction
2.3. Risk of Bias Assessment
2.4. Statistical Analysis
3. Results
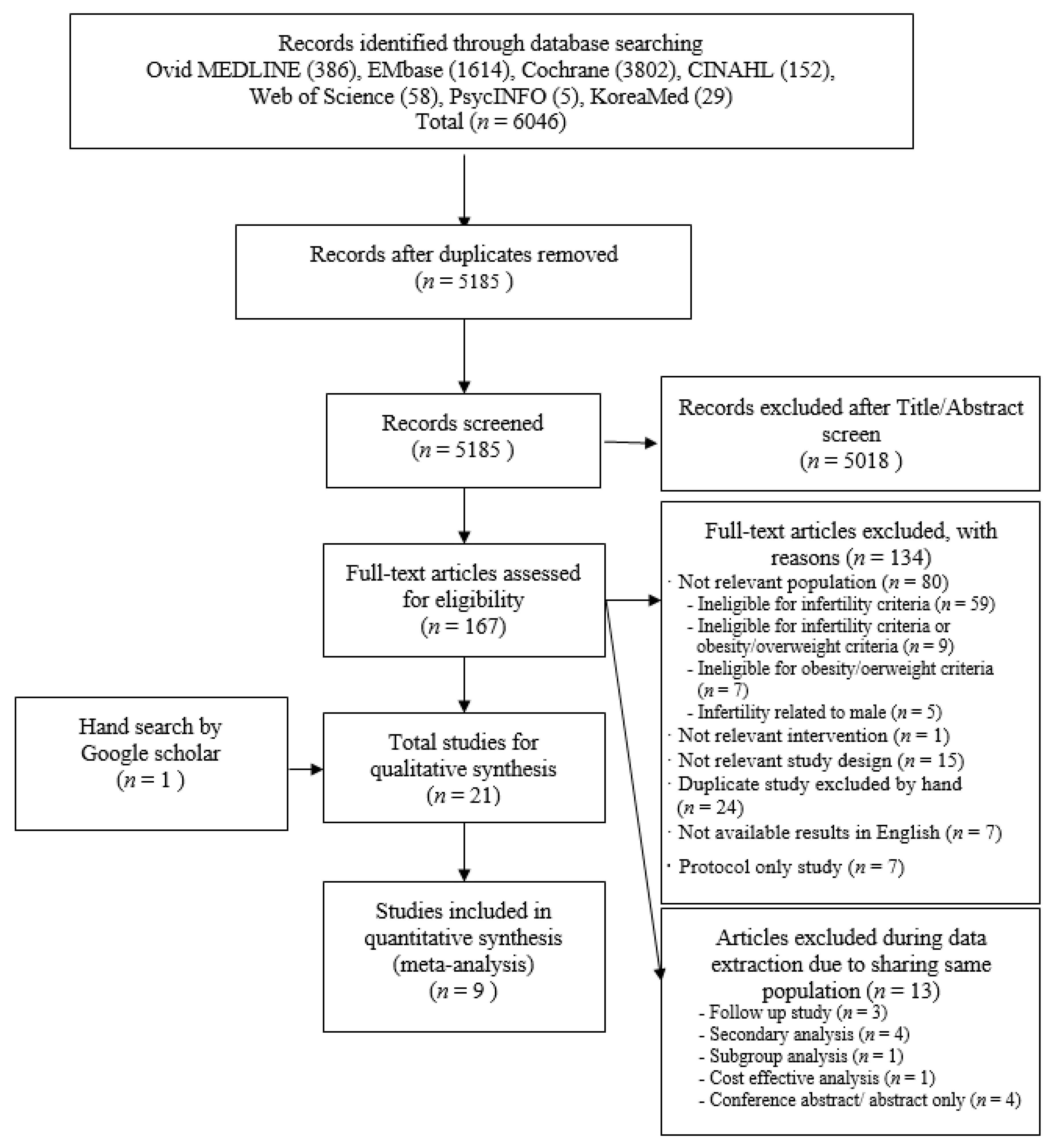
3.1. Selected Studies
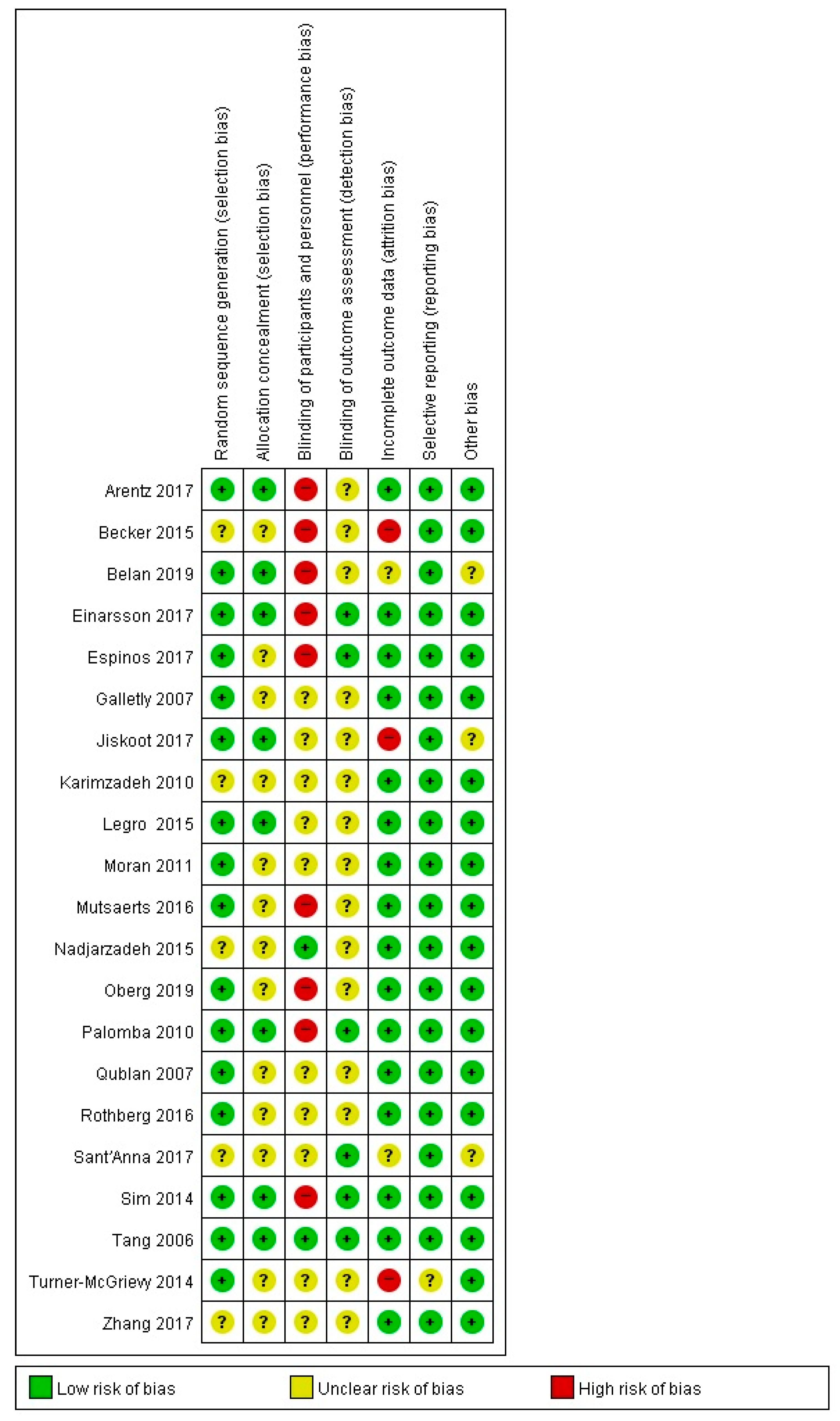
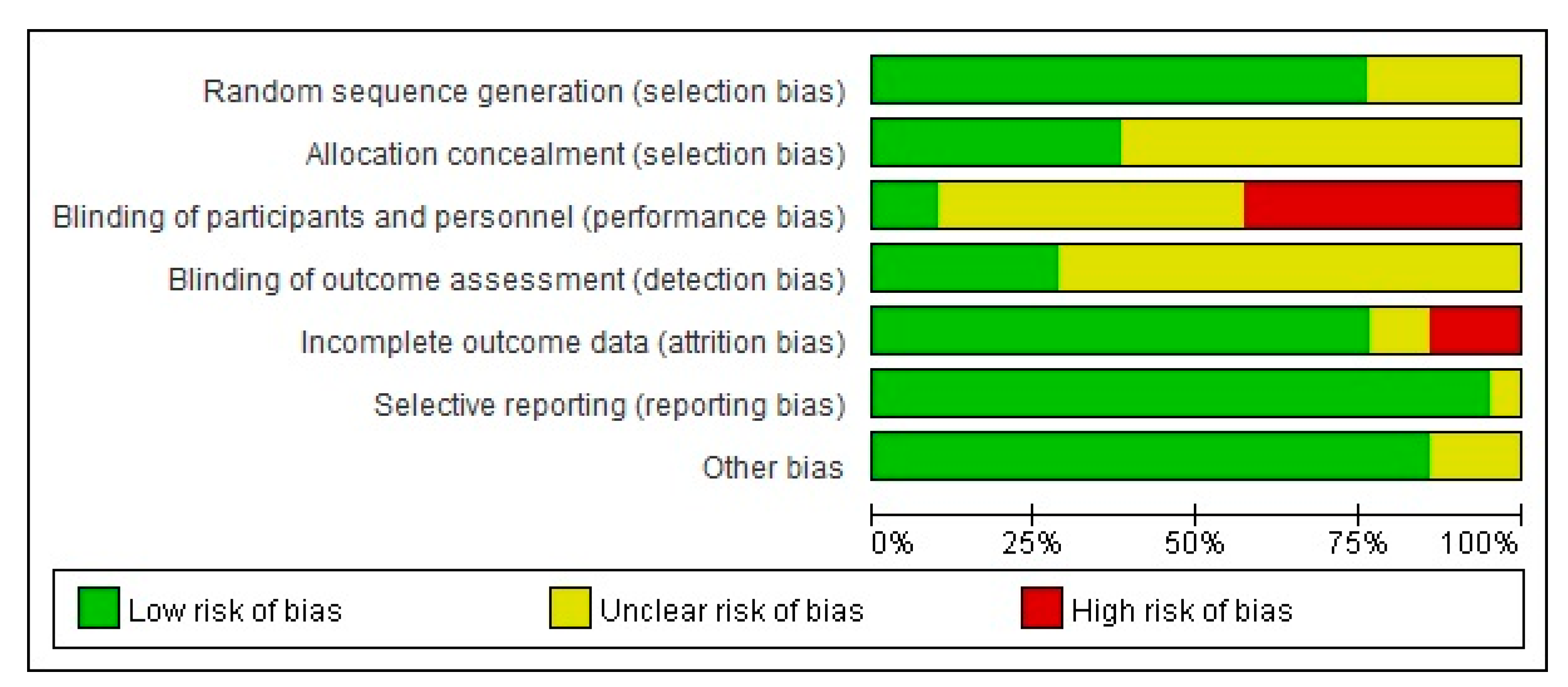
3.2. Risk of Bias Assessment
3.3. Characteristics of the Included Studies
3.3.1. General Characteristics of the Selected Studies
3.3.2. Characteristics of Nonpharmacological Interventions
3.3.3. Characteristics of Outcome Variables
3.4. Effects of the Nonpharmacological Interventions
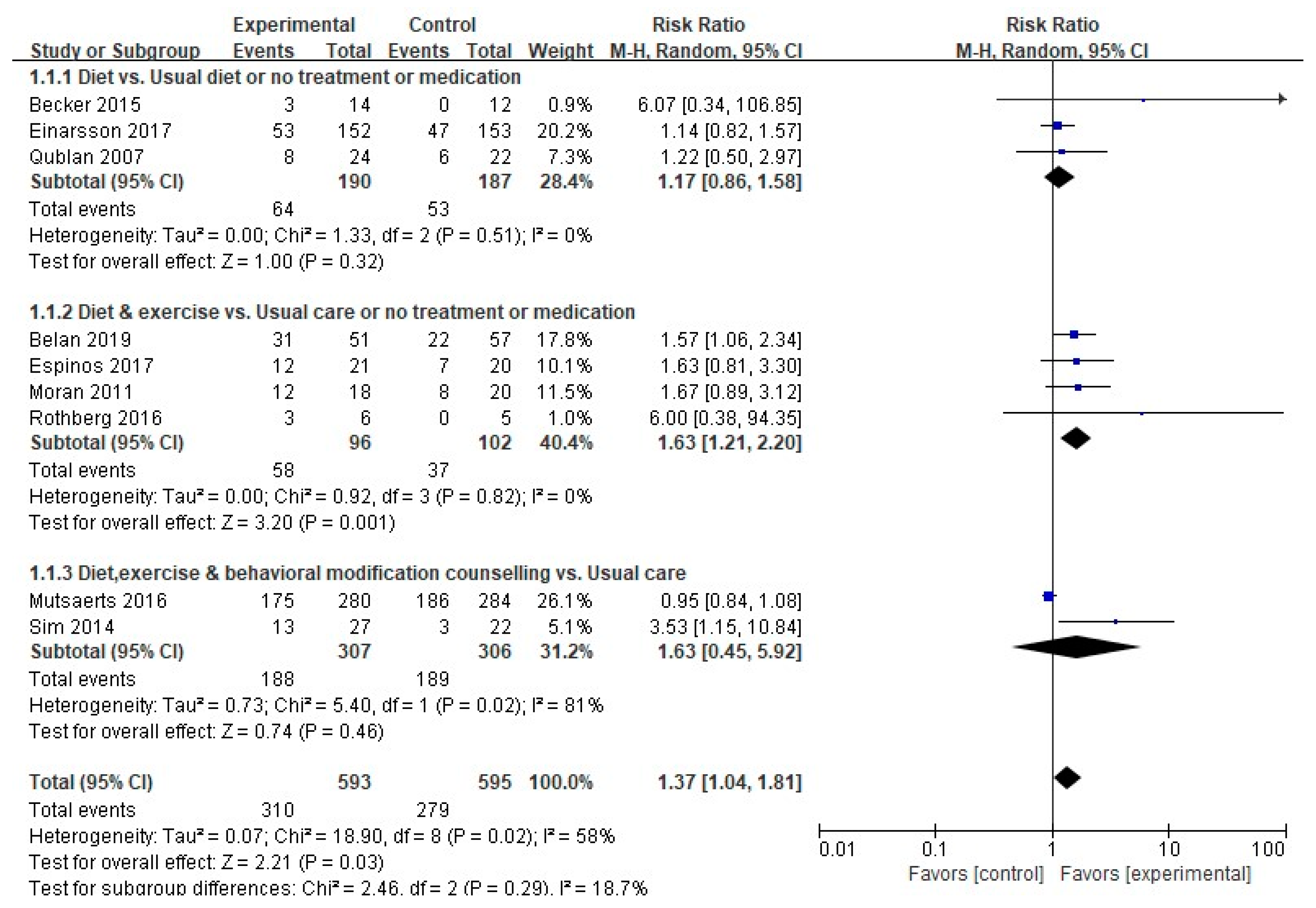
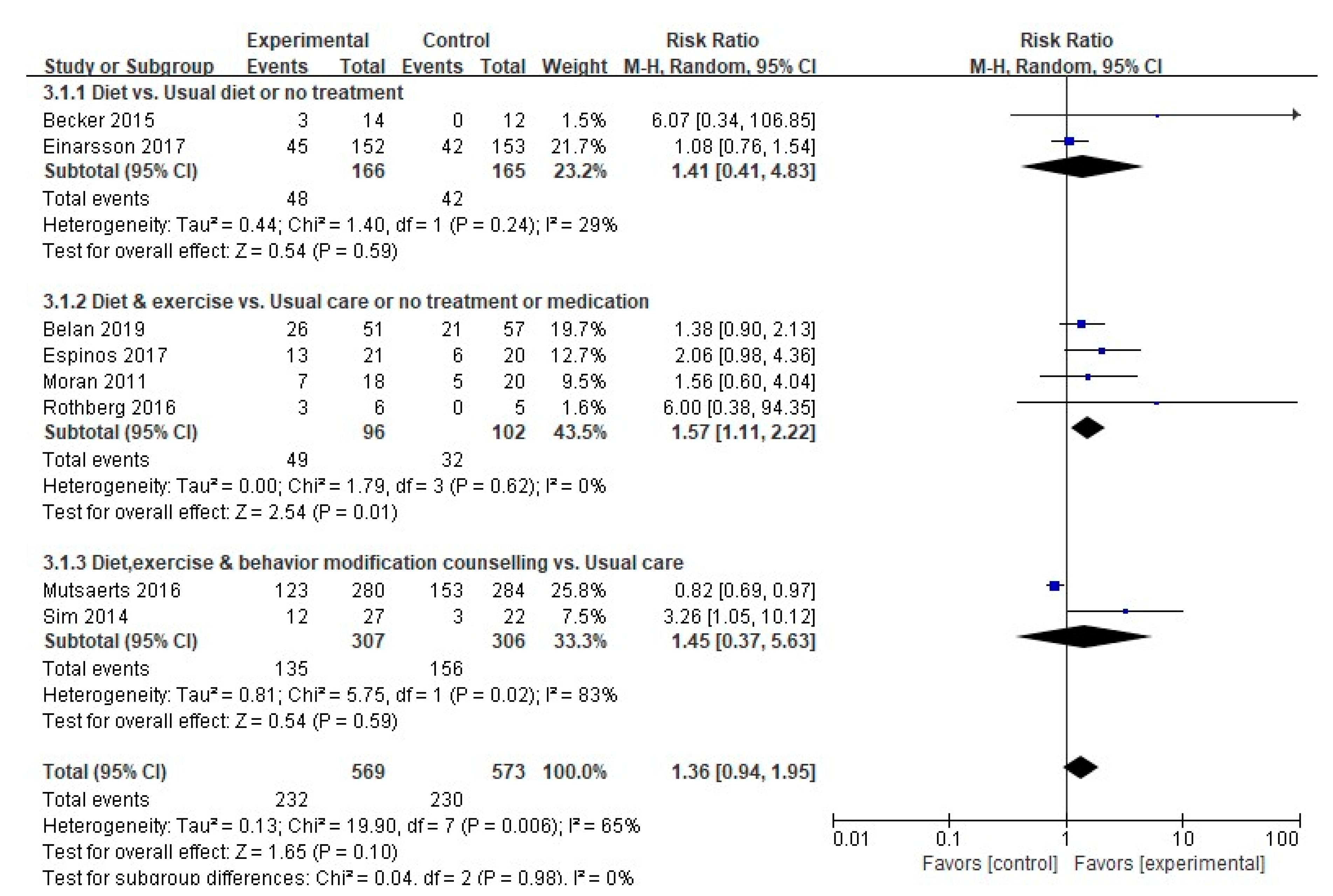
3.4.1. Pregnancy Rate
3.4.2. Natural Conception Rate
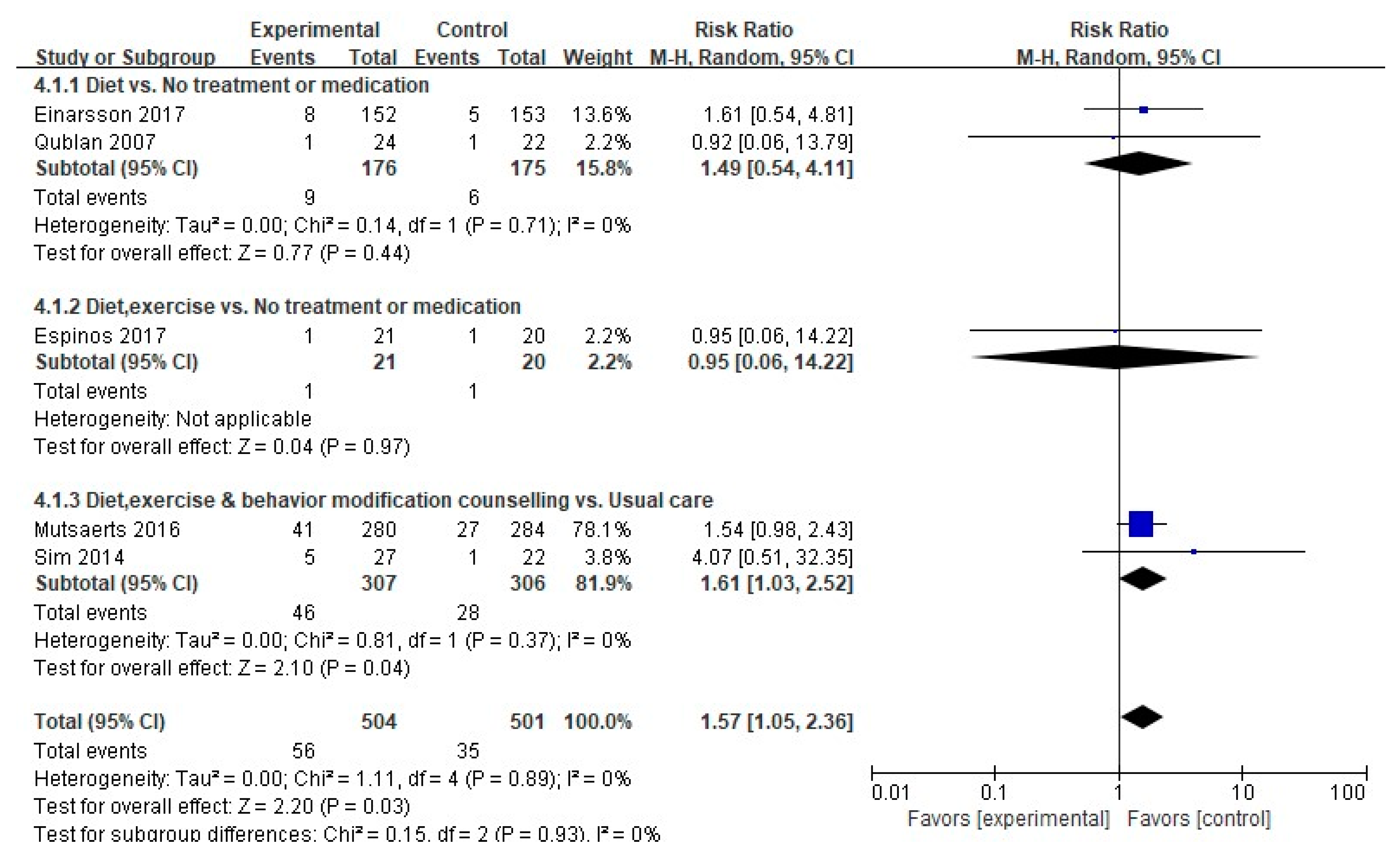
3.4.3. Live Birth Rate
3.4.4. Miscarriage Rate
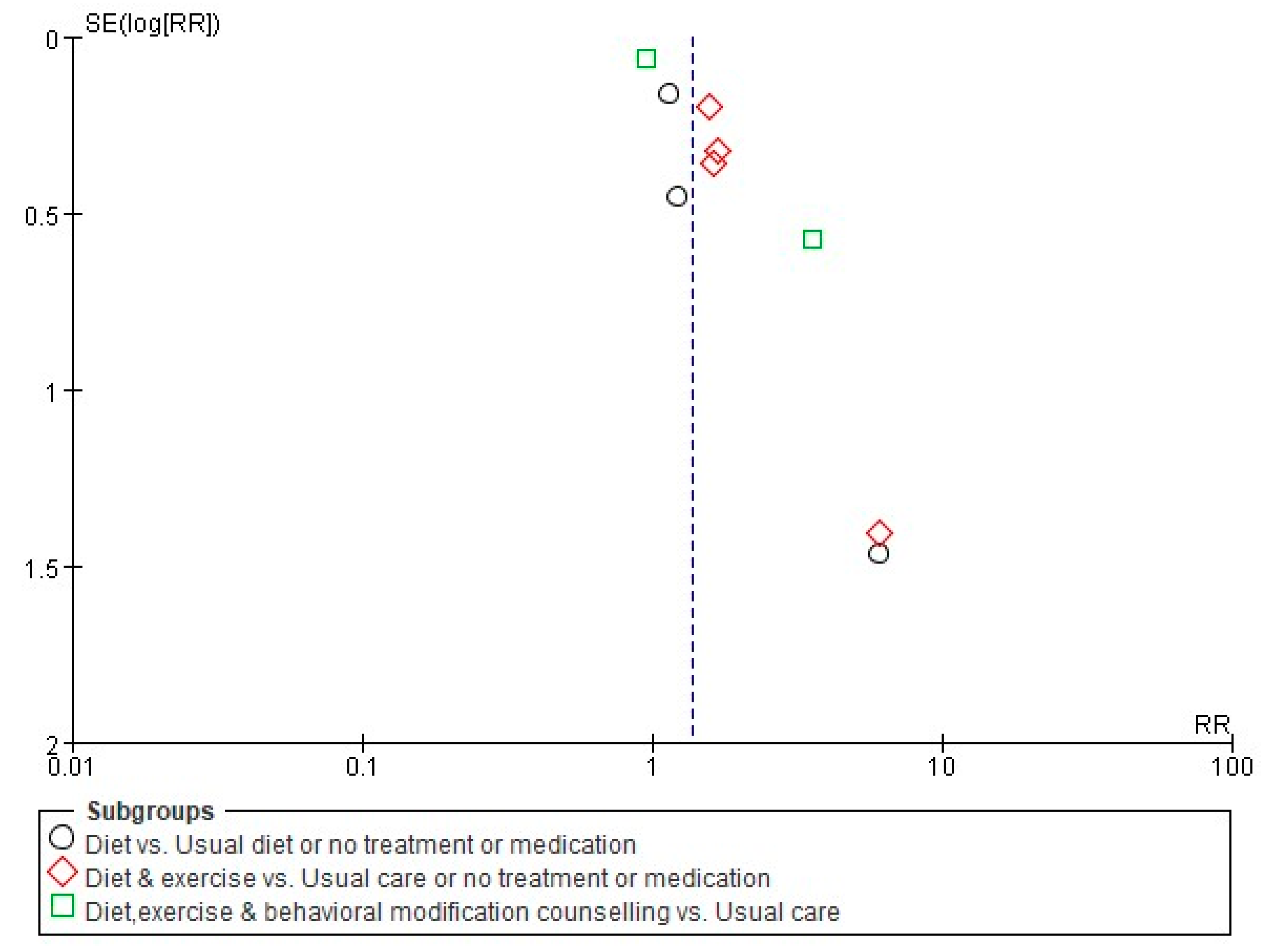
3.5. Publication Bias
4. Discussion
4.1. Characteristics and Quality Assessment of Nonpharmacological Studies on Overweight and Obese Infertile Women
4.2. Effects of Nonpharmacological Intervention Programs
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Vander Borght, M.; Wyns, C. Fertility and infertility: Definition and epidemiology. Clin. Biochem. 2018, 62, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Marchi, J.; Berg, M.; Dencker, A.; Olander, E.; Begley, C. Risks associated with obesity in pregnancy, for the mother and baby: A systematic review of reviews. Obes. Rev. 2015, 16, 621–638. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Saugstad, O.D.; Henriksen, T.; Tonstad, S. Maternal body mass index and the risk of fetal death, stillbirth, and infant death: A systematic review and meta-analysis. JAMA 2014, 311, 1536–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broughton, D.E.; Moley, K.H. Obesity and female infertility: Potential mediators of obesity’s impact. Fertil. Steril. 2017, 107, 840–847. [Google Scholar] [CrossRef] [Green Version]
- Silvestris, E.; de Pergola, G.; Rosania, R.; Loverro, G. Obesity as disruptor of the female fertility. Reprod. Biol. Endocrinol. 2018, 16, 22. [Google Scholar] [CrossRef]
- Lim, S.S.; Davies, M.; Norman, R.J.; Moran, L. Overweight, obesity and central obesity in women with polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. Update 2012, 18, 618–637. [Google Scholar] [CrossRef]
- Kupka, M.S.; Ferraretti, A.P.; De Mouzon, J.; Erb, K.; D’Hooghe, T.; Castilla, J.A.; Calhaz-Jorge, C.; De Geyter, C.; Goossens, V.; Strohmer, H. Assisted reproductive technology in Europe, 2010: Results generated from European registers by ESHRE. Hum. Reprod. 2014, 29, 2099–2113. [Google Scholar] [CrossRef]
- Pandey, S.; Pandey, S.; Maheshwari, A.; Bhattacharya, S. The impact of female obesity on the outcome of fertility treatment. J. Hum. Reprod. Sci. 2010, 3, 62. [Google Scholar] [CrossRef] [Green Version]
- Rittenberg, V.; Seshadri, S.; Sunkara, S.K.; Sobaleva, S.; Oteng-Ntim, E.; El-Toukhy, T. Effect of body mass index on IVF treatment outcome: An updated systematic review and meta-analysis. Reprod. Biomed. Online 2011, 23, 421–439. [Google Scholar] [CrossRef] [Green Version]
- Koning, A.; Mutsaerts, M.; Kuchenbecher, W.; Broekmans, F.; Land, J.; Mol, B.; Hoek, A. Complications and outcome of assisted reproduction technologies in overweight and obese women. Hum. Reprod. 2012, 27, 457–467. [Google Scholar] [CrossRef] [Green Version]
- Hollmann, M.; Runnebaum, B.; Gerhard, I. Effects of weight loss on the hormonal profile in obese, infertile women. Obstet. Gynecol. Surv. 1996, 11, 1884–1891. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.; Thornley, B.; Tomlinson, L.; Galletley, C.; Norman, R. Weight loss in obese infertile women results in improvement in reproductive outcome for all forms of fertility treatment. Hum. Reprod. 1998, 13, 1502–1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crosignani, P.G.; Colombo, M.; Vegetti, W.; Somigliana, E.; Gessati, A.; Ragni, G. Overweight and obese anovulatory patients with polycystic ovaries: Parallel improvements in anthropometric indices, ovarian physiology and fertility rate induced by diet. Hum. Reprod. 2003, 18, 1928–1932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kominiarek, M.A.; Jungheim, E.S.; Hoeger, K.M.; Rogers, A.M.; Kahan, S.; Kim, J.J. American Society for Metabolic and Bariatric Surgery position statement on the impact of obesity and obesity treatment on fertility and fertility therapy Endorsed by the American College of Obstetricians and Gynecologists and the Obesity Society. Surg. Obes. Relat. Dis. 2017, 13, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Johansson, K.; Cnattingius, S.; Näslund, I.; Roos, N.; Trolle Lagerros, Y.; Granath, F.; Stephansson, O.; Neovius, M. Outcomes of pregnancy after bariatric surgery. N. Engl. J. Med. 2015, 372, 814–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Källén, B.A. Antiobesity drugs in early pregnancy and congenital malformations in the offspring. Obes. Res. Clin. Pract. 2014, 8, e571–e576. [Google Scholar] [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine. Obesity and reproduction: A committee opinion. Fertil. Steril. 2015, 104, 1116–1126. [Google Scholar] [CrossRef] [Green Version]
- Brauer, P.; Gorber, S.C.; Shaw, E.; Singh, H.; Bell, N.; Shane, A.R.; Jaramillo, A.; Tonelli, M.; Canadian Task Force on Preventive Health Care. Recommendations for prevention of weight gain and use of behavioural and pharmacologic interventions to manage overweight and obesity in adults in primary care. CMAJ 2015, 187, 184–195. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Qublan, H.; Yannakoula, E.; Al-Qudah, M.; El-Uri, F. Dietary intervention versus metformin to improve the reproductive outcome in women with polycystic ovary syndrome. Saudi Med. J. 2007, 28, 1694–1698. [Google Scholar]
- Becker, G.F.; Passos, E.P.; Moulin, C.C. Short-term effects of a hypocaloric diet with low glycemic index and low glycemic load on body adiposity, metabolic variables, ghrelin, leptin, and pregnancy rate in overweight and obese infertile women: A randomized controlled trial. Am. J. Clin. Nutr. 2015, 102, 1365–1372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Einarsson, S.; Bergh, C.; Friberg, B.; Pinborg, A.; Klajnbard, A.; Karlström, P.O.; Kluge, L.; Larsson, I.; Loft, A.; Mikkelsen-Englund, A.L.; et al. Weight reduction intervention for obese infertile women prior to IVF: A randomized controlled trial. Hum. Reprod. 2017, 32, 1621–1630. [Google Scholar] [CrossRef] [Green Version]
- Turner-McGrievy, G.M.; Davidson, C.R.; Wingard, E.E.; Billings, D.L. Low glycemic index vegan or low-calorie weight loss diets for women with polycystic ovary syndrome: A randomized controlled feasibility study. Nutr. Res. 2014, 34, 552–558. [Google Scholar] [CrossRef]
- Galletly, C.M.; Moran, L.; Noakes, M.; Clifton, P.; Tomlinson, L.; Norman, R. Psychological benefits of a high-protein, low-carbohydrate diet in obese women with polycystic ovary syndrome-A pilot study. Appetite 2007, 49, 590–593. [Google Scholar] [CrossRef]
- Moran, L.; Tsagareli, V.; Norman, R.; Noakes, M. Diet and IVF pilot study: Short-term weight loss improves pregnancy rates in overweight/obese women undertaking IVF. Aust. N. Z. J. Obstet. Gynaecol. 2011, 51, 455–459. [Google Scholar] [CrossRef]
- Rothberg, A.; Lanham, M.; Randolph, J.; Fowler, C.; Miller, N.; Smith, Y. Feasibility of a brief, intensive weight loss intervention to improve reproductive outcomes in obese, subfertile women: A pilot study. Fertil. Steril. 2016, 106, 1212–1220. [Google Scholar] [CrossRef] [Green Version]
- Belan, M.; Carranza-Mamane, B.; Ainmelk, Y.; Pesant, M.-H.; Duval, K.; Jean-Denis, F.; Langlois, M.-F.; Baillargeon, J.-P. A Lifestyle Program Targeting Women with Obesity and Infertility Improves Their Fertility: A Randomized Controlled Trial. J. Endocr. Soc. 2019, 3 (Suppl. S1), OR11-2. [Google Scholar] [CrossRef]
- Espinos, J.J.; Polo, A.; Sanchez-Hernandez, J.; Bordas, R.; Pares, P.; Martinez, O.; Calaf, J. Weight decrease improves live birth rates in obese women undergoing IVF: A pilot study. Reprod. Biomed. Online 2017, 35, 417–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mutsaerts, M.A.; Van Oers, A.M.; Groen, H.; Burggraaff, J.M.; Kuchenbecker, W.K.; Perquin, D.A.; Koks, C.A.; Van Golde, R.; Kaaijk, E.M.; Schierbeek, J.M. Randomized trial of a lifestyle program in obese infertile women. N. Engl. J. Med. 2016, 374, 1942–1953. [Google Scholar] [CrossRef] [PubMed]
- Oberg, E.; Gidlof, S.; Jakson, I.; Mitsell, M.; Tollet Egnell, P.; Hirschberg, A.L. Improved menstrual function in obese women with polycystic ovary syndrome after behavioural modification intervention—A randomized controlled trial. Clin. Endocrinol. 2019, 90, 468–478. [Google Scholar] [CrossRef] [PubMed]
- Jiskoot, G.; Timman, R.; Beerthuizen, A.; de Loos, A.D.; Busschbach, J.; Laven, J. In the impact of a three-component lifestyle intervention on emotional well-being in women with PCOS. In Reproductive Sciences; SAGE Publication: Thousand Oaks, CA, USA, 2019; Volume 26, p. 283A. [Google Scholar]
- Sant’Anna, E.; Paiva, S.; Santos, R.; Rodrigues, A.; Nery, S.; Maia, F.; Ferreira, A.; Reis, F. Mindfulness-based intervention for lifestyle modification and weight loss in infertile women: Randomized controlled trial. In Proceedings of the 33rd Annual Meeting of the European Society of Human Reproduction and Embryology, Geneva, Switzerland, 2–5 July 2017; Oxford University Press: Oxford, UK, 2017; pp. i398–i399. [Google Scholar]
- Sim, K.A.; Dezarnaulds, G.M.; Denyer, G.S.; Skilton, M.R.; Caterson, I.D. Weight loss improves reproductive outcomes in obese women undergoing fertility treatment: A randomized controlled trial. Clin. Obes. 2014, 4, 61–68. [Google Scholar] [CrossRef]
- Zhang, J.; Si, Q.; Li, J. Therapeutic effects of metformin and clomiphene in combination with lifestyle intervention on infertility in women with obese polycystic ovary syndrome. Pak. J. Med. Sci. 2017, 33, 8–12. [Google Scholar] [CrossRef]
- Legro, R.S.D.; Dodson, W.C.; Kris-Etherton, P.M.; Kunselman, A.R.; Stetter, C.M.; Williams, N.I.; Gnatuk, C.L.; Estes, S.J.; Fleming, J.; Allison, K.C.; et al. Randomized controlled trial of preconception interventions in infertile women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2015, 100, 4048–4058. [Google Scholar] [CrossRef]
- Palomba, S.; Falbo, A.; Giallauria, F.; Russo, T.; Rocca, M.; Tolino, A.; Zullo, F.; Orio, F. Six weeks of structured exercise training and hypocaloric diet increases the probability of ovulation after clomiphene citrate in overweight and obese patients with polycystic ovary syndrome: A randomized controlled trial. Hum. Reprod. 2010, 25, 2783–2791. [Google Scholar] [CrossRef] [Green Version]
- Karimzadeh, M.A.; Javedani, M. An assessment of lifestyle modification versus medical treatment with clomiphene citrate, metformin, and clomiphene citrate-metformin in patients with polycystic ovary syndrome. Fertil. Steril. 2010, 94, 216–220. [Google Scholar] [CrossRef]
- Tang, T.; Glanville, J.; Hayden, C.J.; White, D.; Barth, J.H.; Balen, A.H. Combined lifestyle modification and metformin in obese patients with polycystic ovary syndrome: A randomized, placebo-controlled, double-blind multicentre study. Hum. Reprod. 2006, 21, 80–89. [Google Scholar] [CrossRef] [Green Version]
- Arentz, S.; Smith, C.A.; Abbott, J.; Fahey, P.; Cheema, B.S.; Bensoussan, A. Combined lifestyle and herbal medicine in overweight women with polycystic ovary syndrome (PCOS): A randomized controlled trial. Phytother. Res. 2017, 31, 1330–1340. [Google Scholar] [CrossRef] [PubMed]
- Nadjarzadeh, A.; Dehghani-Firouzabadi, R.; Daneshbodi, H.; Lotfi, M.H.; Vaziri, N. Mozaffari-Khosravi, H. Effect of omega-3 supplementation on visfatin, adiponectin, and anthropometric indices in women with polycystic ovarian syndrome. J. Reprod. Infertil. 2015, 16, 212–220. [Google Scholar] [PubMed]
- Stephenson, J.; Heslehurst, N.; Hall, J.; Schoenaker, D.A.; Hutchinson, J.; Cade, J.E.; Poston, L.; Barrett, G.; Crozier, S.R.; Barker, M. Before the beginning: Nutrition and lifestyle in the preconception period and its importance for future health. Lancet 2018, 391, 1830–1841. [Google Scholar] [CrossRef]
- Fleming, T.P.; Watkins, A.J.; Velazquez, M.A.; Mathers, J.C.; Prentice, A.M.; Stephenson, J.; Barker, M.; Saffery, R.; Yajnik, C.S.; Eckert, J.J. Origins of lifetime health around the time of conception: Causes and consequences. Lancet 2018, 391, 1842–1852. [Google Scholar] [CrossRef]
- Barker, M.; Dombrowski, S.U.; Colbourn, T.; Fall, C.H.; Kriznik, N.M.; Lawrence, W.T.; Norris, S.A.; Ngaiza, G.; Patel, D.; Skordis-Worrall, J. Intervention strategies to improve nutrition and health behaviours before conception. Lancet 2018, 391, 1853–1864. [Google Scholar] [CrossRef] [Green Version]
- Nolan, C.; Deehan, A.; Wylie, A.; Jones, R. Practice nurses and obesity: Professional and practice-based factors affecting role adequacy and role legitimacy. Prim. Health Care Res. Dev. 2012, 13, 353–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, H.; Stenlund, H.; Lundström, L.; Weinehall, L. Reorientation to more health promotion in health services–A study of barriers and possibilities from the perspective of health professionals. J. Multidiscip. Healthc. 2010, 3, 213–224. [Google Scholar] [CrossRef] [Green Version]
- Best, D.; Avenell, A.; Bhattacharya, S. How effective are weight-loss interventions for improving fertility in women and men who are overweight or obese? A systematic review and meta-analysis of the evidence. Hum. Reprod. Update 2017, 23, 681–705. [Google Scholar] [CrossRef] [Green Version]
- Laganà, A.S.; Garzon, S.; Casarin, J.; Franchi, M.; Ghezzi, F. Inositol in polycystic ovary syndrome: Restoring fertility through a pathophysiology-based approach. Trends Endocrinol. Metab. 2018, 29, 768–780. [Google Scholar] [CrossRef]
- Pundir, J.; Psaroudakis, D.; Savnur, P.; Bhide, P.; Sabatini, L.; Teede, H.; Coomarasamy, A.; Thangaratinam, S. Gynaecology, Inositol treatment of anovulation in women with polycystic ovary syndrome: A meta-analysis of randomised trials. BJOG 2018, 125, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Facchinetti, F.; Espinola, M.S.B.; Dewailly, D.; Ozay, A.C.; Prapas, N.; Vazquez-Levin, M.; Wdowiak, A.; Unfer, V.; Appetecchia, M.; Aragona, C. Metabolism, breakthroughs in the use of inositols for assisted reproductive treatment (ART). Trends Endocrinol. Metab. 2020. [Google Scholar] [CrossRef] [PubMed]
- Mahey, R.; Gupta, M.; Bansiwal, R.; Sethi, A. Successful IVF outcome after repeat laparoscopic ovarian drilling in a case of resistant PCOS. BMJ Case Rep. 2020, 13, e235628. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, H.R. Update on treatment strategies for obesity. J. Clin. Endocrinol. Metab. 2013, 98, 1299–1306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieuwenhuis-Ruifrok, A.; Kuchenbecker, W.; Hoek, A.; Middleton, P.; Norman, R. Insulin sensitizing drugs for weight loss in women of reproductive age who are overweight or obese: Systematic review and meta-analysis. Hum. Reprod. Update 2009, 15, 57–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morley, L.C.; Tang, T.; Yasmin, E.; Norman, R.J.; Balen, A.H. Insulin-sensitising drugs (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility. Cochrane Libr. 2017, 11. [Google Scholar] [CrossRef]
- Wang, F.F.; Wu, Y.; Zhu, Y.H.; Ding, T.; Batterham, R.; Qu, F.; Hardiman, P. Pharmacologic therapy to induce weight loss in women who have obesity/overweight with polycystic ovary syndrome: A systematic review and network meta-analysis. Obes. Rev. 2018, 19, 1424–1445. [Google Scholar] [CrossRef]
- Kocełak, P.; Chudek, J.; Naworska, B.; Bąk-Sosnowska, M.; Kotlarz, B.; Mazurek, M.; Madej, P.; Skrzypulec-Plinta, V.; Skałba, P.; Olszanecka-Glinianowicz, M. Psychological disturbances and quality of life in obese and infertile women and men. Int. J. Endocrinol. 2012, 2012. [Google Scholar] [CrossRef]
- Mahutte, N.; Kamga-Ngande, C.; Sharma, A.; Sylvestre, C. Obesity and reproduction. J. Obstet. Gynaecol. Can. 2018, 40, 950–966. [Google Scholar] [CrossRef] [Green Version]
- Kominiarek, M.A.; Chauhan, S.P. Obesity before, during, and after pregnancy: A review and comparison of five national guidelines. Am. J. Perinatol. 2016, 33, 433–441. [Google Scholar] [CrossRef]
- Cavalcante, M.B.; Sarno, M.; Peixoto, A.B.; Araujo Junior, E.; Barini, R. Obesity and recurrent miscarriage: A systematic review and meta-analysis. J. Obstet. Gynaecol. Res. 2019, 45, 30–38. [Google Scholar] [CrossRef]
- Radin, R.G.; Mumford, S.L.; Sjaarda, L.A.; Silver, R.M.; Wactawski-Wende, J.; Lynch, A.M.; Perkins, N.J.; Lesher, L.L.; Wilcox, B.D.; Hinkle, S.N. Recent attempted and actual weight change in relation to pregnancy loss: A prospective cohort study. BJOG 2018, 125, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Oxford, UK, 2019; pp. 349–370. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (year) | Country (Study Design) | Inclusion Criteria | Population | Intervention | Follow-Up Period | Main Outcome Variables | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention at Baseline | Control at Baseline | Description by Group (a~d) | Health Provider | Setting | Format (Individual/Group) | Duration | Number of Contacted | |||||
| I. Diet-based intervention | ||||||||||||
| I-1. Diet vs. Others | ||||||||||||
| Qublan et al. (2007) [24] | Jordan | Infertility Primary with PCOS CC-Resistant Age <36 BMI >29 | n = 24 Age: 31.5 BMI: 32.2 PCOS | N=22 Age: 30.8 BMI: 31.9 PCOS | a: Diet (a 1200-1400 kcal/Day; 25% Proteins; 25% Fat; 50% Carbohydrates per Week) b: Met (850mg Twice Daily) | NR | Hospital (Single Center) | In Person | 6 months | 6+ | 12 months | A: BMI B: Pregnancy, Miscarriage Rate C: Ovulation (Rate), Menstrual Cycle D: FSH, LH, T, A, DHEAS, Estradiol E: Fasting Glucose, Fasting Insulin |
| Becker et al. (2015) [25] | Brazil | Infertility Planning IVF BMI 25-40 | n = 14 Age:31.4 BMI:28.7 Multiple Factor | n = 12 Age: 31.3 BMI:28.8 Multiple factor | a: Diet (Hypocaloric Diet with Low-Glycemic Index/Low Glycemic Load Diet b: Usual Diet | Dietitian | Hospital (Single Center) | In Person (Individual) | 12 weeks | 3 | 24 months | A: BMI, BW, WC B: Pregnancy, Natural Conception, Live Birth Rate C: Oocytes Retrieved (No.) D: FSH, LH, T, SHBG, Estradiol E: Fasting Glucose, Fasting Insulin, HOMA-IR, Lipids G: Diet Intake |
| Einarsson et al. (2017) [26] | Nordic Countries | Infertility Planning IVF Age 18–38 BMI 30–34.9 | n = 152 Age:31.5 BMI:33.1 Multiple Factor | n = 153 Age: 31.7 BMI:33.0 Multiple Factor | a: LCD Liquid Formula Diet (880kcal/Day for 12 Weeks, Weight Maintenance for 2–5 Weeks) before IVF b: Only IVF | Health Professional, Dietitian | 9 Infertility Clinics | In Person (Individual) | 16 weeks | 6 | NR | A: BMI, BW B: Pregnancy, Natural Conception, Live Birth, Miscarriage Rate C: Oocytes Retrieved (No.) |
| I-2. Diet (Type of diet) | ||||||||||||
| Turner-McGrievy et al. (2014) [27] | USA (Pilot Study) | Infertility Due to PCOS Trying to Conceive over 6 mo Age 18–35 BMI 25–49.9 | n = 9 Age: 28.1 BMI: 42.7 PCOS | n = 9 Age: 27.4 BMI: 37.2 PCOS | a: Vegan Diet (a Low-Fat, Low–Glycemic Index Vegan Diet with no Caloric restriction) b: LCD ( 1200 kcal/Day, <90 kg; 1500 kcal/Day, >90kg) | Dietitian | Local Medical Clinic (Single Center) | In Person (Individual) + Email + Social Media | 6 months | 27+ | 6 months | A: BW B: Pregnancy Rate C: Ovulation (Detection), Menstrual Cycle F: QoL G: Diet Intake, Physical Activity |
| Galletly et al. (2007) [28] | Australia (Pilot Study) | Infertility Due to PCOS (Including Actively Try to Conceive) BW <140 kg | n = 12 Age: 33.0 BMI: 37.6 PCOS | n = 13 Age: 32.0 BMI:37.2 PCOS | Diet (6000KJ/Day for 12 Weeks, Weight Maintenance for 4 Weeks) + Exercise a: HPLC Diet (30% Protein, 40% Carbohydrate, 30% Fat) b: LPH Diet (15% Protein, 55% carbohydrate, 30% fat) | Dietitian | NR | In Person (Individual + Group) | 16 weeks | 16+ | 16 weeks | A: BMI, BW F: Depression and Anxiety G: Self-Esteem |
| I-3. Diet Plus Exercise Intervention | ||||||||||||
| Moran et al. (2011) [29] | Australia (Pilot Study) | Infertility Undergoing IVF (Previously had One Round of ART) Age 18–40 BMI 28–45 | n = 18 Age: 33.8 BMI:34 Multiple Factor | n = 20 Age: 32.5 BMI:33.9 Multiple Factor | a: Diet (One Liquid Meal Replacement + 200 ml Reduced Fat Milk (1057 kJ)) + Exercise b: Standard Advice on Diet and Lifestyle Factors | Dietitian | Hospital (Single Center) | In person (Individual) + Phone | 52.6 (14.0)/53.5 (16.6) Days | 3 | NR | A: BMI, BW, WC B: Pregnancy, Live Birth Rate |
| Rothberg et al. (2016) [30] | USA (Pilot Study) | Infertility due to Ovulation Dysfunction Age 18-40 BMI 35-45 | n = 6 Age: 33 BMI:41 Multiple Factor | n = 5 Age: 30 BMI:41 Multiple Factor | a: VLED (Liquid Meal Replacements, 800 Kcal/Day for 12 Weeks) + Low-Calorie Conventional Food-Based Diet (CFD) (for 4 Weeks) + Exercise Encouragement b: CFD (for 16 Weeks) | Dietitian, Physician | Academic Institution (Single Center) | In Person | 16 weeks | 12 | 12 months | A: BMI, BW, WC B: Pregnancy, Live Birth, Miscarriage Rate C: Ovulation (Induction, Detection), E: Fasting Glucose, Fasting Insulin, HOMA-IR, Lipids F: QoL, Depression |
| Belan et al. (2019) [31] | Canada | Infertility Age 18–40 Obesity with BMI ≥30 Overweight if PCOS, BMI ≥27 | n = 51 Multiple Factor (PCOS, Non-PCOS) | n = 57 Multiple Factor (PCOS, Non-PCOS) | a: Interdisciplinary Lifestyle Intervention (Diet + Exercise) before Infertility Treatment b: Standard Fertility Treatments | Dietitian, Kinesiologist, Psychologists | Academic Hospital (Single Center) | In person (Group + Individual) + Phone/Email | 18 months or Until the End of Pregnancy | 25 | 18 months or Until the End of Pregnancy | A: BW, WC B: Pregnancy, Natural Conception, live birth rate G: Diet Intake, Physical Activity |
| Espinos et al. (2017) [32] | Spain (Pilot Study) | Infertility Presenting First IVF Age 18–37 BMI 30-40 | n = 21 Age:32.0 BMI:34.6 Multiple Factor | n = 20 Age:32.9 BMI:34.0 Multiple Factor | a: Diet (Reduce Total Daily Calorie Intake by at least 500–800 kcal) + Exercise before Single IVF or ICSI b: No Intervention | Dietitian, Trained Staff | Hospital | In Person (Individual) | 12 weeks | 36+ | NR | A: BMI, BW, WC B: Pregnancy, Live Birth, Miscarriage Rate C: Oocytes Retrieved (No.) |
| II. Diet, Exercise plus behavioral modification intervention | ||||||||||||
| Mutsaerts et al. (2016) [33] | Netherlands | Infertility Age 18–39 BMI >29 | n = 280 Age:29.7 BMI: † 36.0 Multiple Factor | n = 284 Age:29.8 BMI: † 36.0 Multiple Factor | a: Diet, Exercise, Behavioral Change (Motivational Counselling) before Infertility Treatment b: Conventional Infertility Treatment (with Dutch Infertility Guideline) | Nurse | 6 University Medical Centers and 17 General Hospitals | In Person (Individual)+Phone/Email | 6 months | 10 | 24 months | A: BW, WC B: Pregnancy, natural conception, live birth, miscarriage rate, C: Ovulation (induction) H: Adverse outcome |
| Oberg, et al. (2019) [34] | Sweden (Pilot Study, Pre-Post design) | Infertility due to PCOS Aged 18–40 BMI ≥27 | n = 34 Age: 31.0 BMI:33.5 PCOS | n = 34 Age: 29.9 BMI:34.3 PCOS | a: Behavioral Modification (Information of Weight Control, Personal Leadership, Mindfulness and Physical Activity) b: Minimal Intervention (General Healthy Lifestyle Recommendations) | Lifestyle Coach (PhD in Endocrinology, Metabolism) and Midwife | Hospital | In Person (Small Groups + Individual) | 16 weeks | 16 | 12 months | A: BMI, BW B: Pregnancy, Natural Conception, live Birth, Miscarriage Rate C: Ovulation (Rate), Menstrual Cycle D: FSH, LH, T, A, SHBG, FAI, DHEAS, Estradiol E: Fasting Glucose, Fasting Insulin, HOMA-IR |
| Jiskoot et al. (2019) [35] | Netherlands | Infertility due to PCOS Trying to Conceive over 1 year Age 18–38 BMI > 25 | a: n = 72 PCOS | b: n = 77 c: n = 60 PCOS | a: CBT Lifestyle Intervention (Diet + Exercise) b: CBT +Short Message Service (SMS) c: (Control) Usual Care (Encouraged to Lose Weight by Publicly Available Services) | Mental Health Professional, Physical Therapist and Dietitian | Academic Hospital | In Person (Group + Individual) + Phone | 12 months | 25 | 12 months | A: BMI, BW F: Depression G: Self-Esteem, Body Image |
| Sant’Anna et al. (2017) [36] | NR | Infertility Age 18–48 BMI > 25 | n = 51 Age: † 37.0 | n = 49 Age: † 31.0 | a: Mindfulness based Stress Reduction Intervention b: No Intervention All Participants Received Dietary Plan and Physical Exercise | Trained Personnel | Hospital | NR | 8 weeks | 8 | 12 weeks | A: BW, WC B: QoL |
| Sim et al. (2014) [37] | Australia (Evaluator-Blinded) | Infertility Intending to Commence IVF, ICSI or Cryo-Stored Embryo Transfer Age18–37 BMI ≥ 30 | n = 27 Age:32.9 BMI:35.1 Multiple Factor | n = 22 Age:32.8 BMI:38.0 Multiple Factor | a: Diet (VLED for 6 Weeks then Hypocaloric Diet for 6 Weeks) Exercise and Psychological and Behavioral Advice then ART b: Standard Care (Advised to See their GP for Weight Loss) then ART | Fertility Fellow, Midwife, Fertility Counsellor, Dietitian | Hospital (Single Center) | In Person (Group + Individual) | 12 weeks | 13 | 12 months | A: BMI, BW, WC B: Pregnancy, Natural Conception, Live Birth, Miscarriage Rate H: Adverse Outcome |
| III. Lifestyle intervention combined medication | ||||||||||||
| Zhang, and Li (2017) [38] | China | Infertility due to PCOS Age 22–34 | n = 51 Age: 28.3 BMI: 23.0 PCOS | n = 50 Age: 27.8 BMI:23.4 PCOS | a: Lifestyle Intervention (Low-Fat Diet + Exercise Strengthening) with Met (500 mg, Three Times Daily, 3 Days of Menstruation) + CC (50–100 mg Once Daily, 1st–3rd Days of 3–5 days of Menstruation) b: Met + CC Same Above | NR | Hospital (Single Center) | In Person | 6 months | NR | 6 months | A: BMI, BW B: Pregnancy Rate C: Ovulation (Rate), Menstrual Cycle D: LH, T E: Fasting Insulin, Lipids (TG) |
| Legro et al. (2015) [39] | USA | Infertility due to PCOS Planning Pregnancy) Age 18–40 BMI 27–42 | a: n = 44 Age: a:28.6 BMI: a:35.1 PCOS | b: n = 43 c: n = 45 Age: b:28.7 c:29.8 BMI: b:35.5 c:35.1 PCOS | a: Lifestyle Intervention (Meal Replacements+ Exercise to Achieve >7% Weight Loss) + Weight Loss Medication (Sibutramine or Orlistat) before Ovulation Induction b: (Combined) a +c c: (Control) OCPs Only before Ovulation Induction | Trained Study Coordinators | Academic Health Centers (Two-Site) | In Person | 16 weeks | NR | 13 months | A: BW, WC B: Pregnancy Rate, Live Birth Rate, Miscarriage Rate C: Ovulation (Rate) D: T, SHBG E: Glucose (2 h, AUC), Insulin (2 h, AUC), Insulin Sensitivity Index F: QoL H: Adverse Outcome |
| Palomba et al. (2010) [40] | Italy (Assessor-Blinded) | Infertility due to PCOS with Anovulatory Infertility and Known CC Resistance Overweight (BMI 25–30), Obese (BMI > 30) | a: n=32 Age: a:27.5 BMI: a:31.3 PCOS | b: n = 32 c: n = 32 Age: b:28.4 c:26.5 BMI: b:31.1 c:32.3 PCOS | a: Lifestyle Intervention (Structured Exercise Training (SET) + Hypocaloric Diet) b: (Combined) Lifestyle Intervention + CC (One Cycle, for First 2 Weeks) c: (control) CC | Cardiologist | NR (Single Center) | In Person | 6weeks | 21+ | 6 weeks | A: BMI, BW, WC B: Pregnancy Rate C: Ovulation (rate) D: FSH, LH, T, SHBG, FAI, A, DHEAS, Estrogen E: Fasting Glucose, Fasting Insulin, HOMA-IR |
| Karimzadeh and Javedani (2010) [41] | Iran (Double-Blind) | Infertility Primary with PCOS Age 19–35 BMI 25–29.9 | a: n = 90 b: n = 90 Age: a:27.5 b:27.3 BMI: a:27.2 b:27.2 PCOS | c: n = 88 d: n = 75 Age: c:27.3 d:27.5 BMI:c:28.0 d:.27.9 PCOS | a: CC (100 mg on Days 3-7) b: Met (Initial dose of 500 mg Increased Until 1500 mg/day for 3–6 Months) c: CC + Met d: Lifestyle Modification (Low Calorie Diet + Exercise Advice) only | Dietician | University-Based infertility Clinic and Research Center | In Person | NR | 2+ | 8 months | A: BMI, WC B: Pregnancy Rate C: Menstrual Cycle D: T, SHBG E: Insulin, Lipids |
| Tang et al. (2006) [42] | UK (Double-Blind) | Infertility due to Anovulatory PCOS Including Desire to Conceive Age 18–39 BMI > 30 | n = 56 Age: 29.7 BMI:37.6 PCOS | n = 66 Age: 29.8 BMI:38.9 PCOS | a: Lifestyle Intervention (Hypocaloric Diet; Reduction in Daily Intake by 500 kcal, + Exercise Advice) + Met 850 mg Twice Daily b: Placebo + Lifestyle Intervention | Dietitian, Nurse and Medical Personnel | 8 Hospital Infertility Clinics | In Person (Individual) | 6 months | 6+ | 6 months | A: BMI, BW, WC B: Pregnancy Rate C: Menstrual Cycle D: T, SHBG, FAI E: Fasting Glucose, Fasting Insulin, QUICKI, Lipids |
| IV. Supplementation | ||||||||||||
| Arentz et al. (2017) [43] | Australia | Infertility due to PCOS) Including Desire to Conceive Age 18–44 BMI ≥ 24 | n = 60 Age: 29.2 BMI:34.1 PCOS | n = 62 Age: 28.9 BMI:35.2 PCOS | a: Herbal Medicine + Lifestyle Intervention (Dietary + Exercise Behaviors) b: Lifestyle Intervention | Dietitian, Exercise Physiologist, Herbal Practitioner | Community | In Person (Individual) | 12 weeks | 4+ | 12 weeks | A: BMI, BW, WC B: Pregnancy, Live Birth, Miscarriage Rate C: Menstrual Cycle D: FSH, LH, T, SHBG, FAI E: Fasting Glucose, Fasting Insulin, Insulin Sensitivity (QUICKI) F: QoL, Depression, Anxiety, and Stress |
| Nadjarzadeh et al. (2015) [44] | Iran (Double Blind) | Referred to Infertility Center Due to PCOS Age 20–40 BMI 25–40 | n = 39 Age: 26.9 BMI:31.5 PCOS | n = 39 Age: 26.9 BMI: 31.9 PCOS | a: Omega-3 (180 mg EPA and 120 mg DHA), 3 Capsules Daily) b: Placebo (1 g Paraffin, 3 Capsules Daily) | NR | Hospital | In Person (Individual) + Phone | 8 weeks | 10 | 8 weeks | A: BMI D: FSH, LH |
| Characteristics | Categories | n (%) |
|---|---|---|
| Year | 2005–2009 | 3 (14.3) |
| 2010–2014 | 5 (23.8) | |
| 2015–2019 | 13 (61.9) | |
| Country | Australia USA Netherland Nordic Countries (Sweden, Denmark, and Iceland) Iran Canada UK Italy Spain China Brazil Jordan Unclear | 4 (19.0) 3 (14.3) 2 (9.5) 2 (9.5) 2 (9.5) 1 (4.8) 1 (4.8) 1 (4.8) 1 (4.8) 1 (4.8) 1 (4.8) 1 (4.8) 1 (4.8) |
| Sample Size of Each Group | 5–29 30–49 50–99 100–149 150–200 200–284 | 8 (38.1) 4 (19.0) 6 (28.6) 1 (4.8) 1 (4.8) 1 (4.8) |
| Mean Age of Participants in Each Group (Year) | 25–29.9 30–37 Not reported | 9 (42.9) 10 (47.6) 2 (9.5) |
| Mean Body Mass Index of Participants in Each Group (kg/m2) | 23.0-29.9 30.0–34.9 35.0–42.7 Not reported | 3 (14.3) 8 (38.1) 7 (33.3) 3 (14.3) |
| Infertility Factor of Participants | Polycystic ovary symptom only Multiple Not reported | 12 (57.1) 8 (38.1) 1 (4.8) |
| Type of Intervention | Diet-based intervention Diet vs. Others Diet (Type of Diet) Diet plus exercise intervention Diet, exercise plus behavioral modification Lifestyle intervention combined medication Supplementation | 5 (23.8) 3 (14.3) 2 (9.5) 4 (19.0) 5 (23.8) 5 (23.8) 2 (9.5) |
| Health Provider Involvement † (n = 35) | Dietitian Physical professional (Physiologist or Kinesiologist or Physical Therapist) Nurse or Midwife Physician Metal health Professional Trained Personnel Not specified Health Professional Herbal Practitioner Counsellor Not Reported | 13 (37.1) 3 (8.6) 4 (11.4) 4 (11.4) 2 (5.7) 2 (5.7) 2 (5.7) 1 (2.9) 1 (2.9) 3 (8.6) |
| Setting | Hospitals or Infertility Clinics Academic Institution Community Not Reported | 16 (76.2) 2 (9.5) 1 (4.8) 2 (9.5) |
| Format † (n = 29) | In Person Individual Mixed (Individual + Group) Unclear Phone Social Media (Facebook) Not Reported | 20 (69.0) 9 (31.0) 5 (17.2) 6 (20.7) 4 (13.8) 3 (10.3) 1 (3.4) 1 (3.4) |
| Duration of Intervention (Weeks or Months) | 7.5 Weeks–12 Weeks 13 Weeks–6 Months 7–12 Months 13–18 Months Not Reported | 8 (38.1) 10 (47.6) 1 (4.8) 1 (4.8) 1 (4.8) |
| Follow-up period (Weeks or Months) | 6 Weeks–12 Weeks 13 Weeks–6 Months 7–12 Months 13–24 Months Not Reported | 4 (19.0) 4 (19.0) 6(28.6) 4 (19.0) 3(14.3) |
| Categories | Outcome Variables (Measurements) | n |
|---|---|---|
| Anthropometrics (n = 56) | Body weight | 18 |
| BMI | 16 | |
| Waist Circumference | 13 | |
| Hip Circumference | 2 | |
| WHR | 6 | |
| Ferriman-Gallwey score | 1 | |
| Pregnancy and Birth outcomes (n = 62) | Pregnancy rate | 17 |
| Natural conception | 6 | |
| Infertility treatments conception (IVF, ICSI, IUI, ovulation induction etc.) | 4 | |
| Multiple pregnancy | 7 | |
| Ectopic pregnancy | 3 | |
| Miscarriage | 9 | |
| Live birth | 11 | |
| Gestational age at delivery | 2 | |
| Infant birth weight | 2 | |
| Delivery mode | 1 | |
| Fertility-related outcomes (n = 45) | Ovulation - Ovulation rate - Ovulation detection | 5 2 |
| - Regularity of menstrual cycles | 7 | |
| Fertility treatment measures | ||
| - Number of oocytes retrieved | 3 | |
| - Number of medication-induced cycles of ovulation | 2 | |
| - Total dose of FSH used | 2 | |
| - Number of assisted conception cycles | 2 | |
| - Fertilization rate | 2 | |
| - Implantation rate1 | 2 | |
| - No. of good quality embryos | 2 | |
| - Fresh transfer (IVF or ICSI) | 3 | |
| - Cryo-stored embryo transfer | 3 | |
| - Cancelled cycle | 2 | |
| Ultrasound parameters | ||
| - Antral follicle count | 2 | |
| - Ovarian volume | 3 | |
| - Endometrial thickness | 3 | |
| Reproductive Hormone outcomes (n = 58) | Gonadotropin Hormone - FSH - LH - LH:FSH ratio | 6 7 3 |
| Prolactin | 4 | |
| Androgen Hormone - Testosterone - Androstenedione - DHT - DHEAS - Free Androgen Index | 9 3 1 3 4 | |
| Hirsutism | 1 | |
| SHBG | 7 | |
| Anti-Mullerian hormone | 2 | |
| Estrogens - Estrogen - Estradiol | 1 3 | |
| Progesterone | 2 | |
| 17-OHP | 2 | |
| Metabolic outcomes (n = 57) | Glucose - Fasting glucose - 2 h glucose - AUC glucose | 7 1 1 |
| Insulin - Fasting Insulin - 2 h insulin - AUC insulin - GIR (fasting glucose-to-insulin ratio) - Insulin sensitivity (QUICKI) - Insulin sensitivity Index - Insulin resistance (HOMA-IR) | 9 1 1 1 2 1 4 | |
| Lipid profile - Total cholesterol - Triglycerides - High-density lipoprotein (HDL) - Low-density lipoprotein (LDL) - Visfatin - Adiponectin | 3 4 2 3 1 1 | |
| Thyroid Hormone - TSH - Free T4 | 1 1 | |
| Others - Acylated ghrelin - Leptin - Hs-CRP | 1 1 1 | |
| Fat mass | 4 | |
| Blood pressure | 5 | |
| Heart rate | 1 | |
| Psychological outcomes (n = 9) | Quality of life - (PCOSQ) - (EQ-5D) - (PGWBI) | 3 1 1 |
| Depression - (BDI-II) - (IDS-SR) | 1 1 | |
| Depression and anxiety (HAD) Depression, anxiety, and stress (DASS21) | 1 1 | |
| Cognitive Behavioral outcomes (n = 9) | Self-esteem (SE) | 2 |
| Body image (FNAES) | 1 | |
| Physical activity - (PPAQ) - Accelerometer | 1 2 | |
| Dietary intake - (health eating index) - (ASA24) - Calculated by Nutribase7software (CyberSoft Incorporated, Phoenix, Arizona, USA) | 1 1 1 | |
| Adverse outcomes (n = 11) | During preconception (diarrhea, steatorrhea, breast pain, abdominal pain, dysmenorrhea, abnormal and uterine bleeding) | 2 |
| During infertility treatment (headache, OHSS, torsion, bleeding infection, etc.) | 2 | |
| During pregnancy (GDM, gestational HTN, pre-eclampsia, and Cesarean section) | 4 | |
| During postpartum Adverse postpartum outcome (PPH and total perineal rupture) Adverse neonatal outcome (congenital anomalies, premature birth, SGA, LGA, Apgar score <7 at 5 min, death, stillbirth, etc.) | 2 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.Y.; Park, E.-S.; Kim, H.W. Effectiveness of Non-Pharmacological Interventions for Overweight or Obese Infertile Women: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 7438. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207438
Kim SY, Park E-S, Kim HW. Effectiveness of Non-Pharmacological Interventions for Overweight or Obese Infertile Women: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(20):7438. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207438
Chicago/Turabian StyleKim, Seo Yun, Eun-Sun Park, and Hae Won Kim. 2020. "Effectiveness of Non-Pharmacological Interventions for Overweight or Obese Infertile Women: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 20: 7438. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207438