2.1. Data Collection: Study Area and Datasets
The geographical area covered by the analysis in this study includes 19 counties/cities and 349 towns on the main island of Taiwan. Information about board-certificated physiatrists was retrieved from the open data of Taiwan Academy of Physical Medicine and Rehabilitation in 2020 [
26]. Information about the population aged 65 and above in towns was retrieved from the database of Department of Household Registration, Ministry of the Interior, which was released in March 2020 [
27].
The convenience of transportation is an important factor that determines senior citizens’ access to community care resources. However, to examine the differences in convenience of transportation in counties/cities, we will have to consider the types of vehicles, frequencies of running and travel time, fare policies, as well as fare subsidy policies of counties/cities. Due to the scarcity or low credibility of relevant data, it is infeasible to include such information in the analysis of road network data. In the evaluation of factors that affect geographic accessibility, the study took reference from the research method of Page et al. [
28]. While retrieving data for the analysis of transportation influencing factors, the road network data in government open data representing actual route distances were adopted instead of the traditional map distances (the linear distance between two points) to reduce the error. As for map data, numerical maps were taken from the Ministry of Transportation and Communications [
29]. The ArcGIS application, which adopts geographic information systems, was used to calculate geographic accessibility by a geography information system (GIS)-based network analysis. As the geographic accessibility analysis focused on the convenience of users’ mobility, if the data of supply points in the main island and outlying islands of Taiwan are mixed and assessed collectively, the issues in traffic and geographic distance will produce deviations in resource accessibility assessment. Therefore, the study area was limited to the main island of Taiwan.
To define the searching area of physiatrist resources, registered specialist clinics were listed and filtered in this study, according to the Taiwan Academy of Physical Medicine and Rehabilitation. As these resource data only list service units, we had to search for the addresses of every service unit before converting the addresses to coordinates by geocoding applications. Next, with the use of the geography information system (GIS), the latitudes and longitudes of the locations of every resource were positioned in the TWD97 2-degree transverse Mercator coordinate system. Cartographic visualization was employed to test the accuracy of every coordinated point and reduce location error. Finally, the cartographic data of physiatrist resources were produced. As of March 2020, there were 688 physiatrist service points in the main island of Taiwan, while there were 1140 physiatrists in total.
Preliminary investigations in this study indicated that there were 3,618,878 people aged 65 and above on the main island of Taiwan as of March 2020. As there were 1140 physiatrists in total, it means that for every 10,000 elderly people there were 3.15 physiatrists on average. As the number is close to the population of towns, the weighted center point of towns (generated by the weighed calculation of population in villages) would represent the center point of people in demand for resources.
2.2. Measuring Geographic Accessibility to Elderly Physical Rehabilitation Resources
The geographic accessibility of resources is a critical basis for considering resource allocation. A main method to analyze resource accessibility is to calculate the ratio of resources allocated (amount and spatial distribution) to the population at demand.
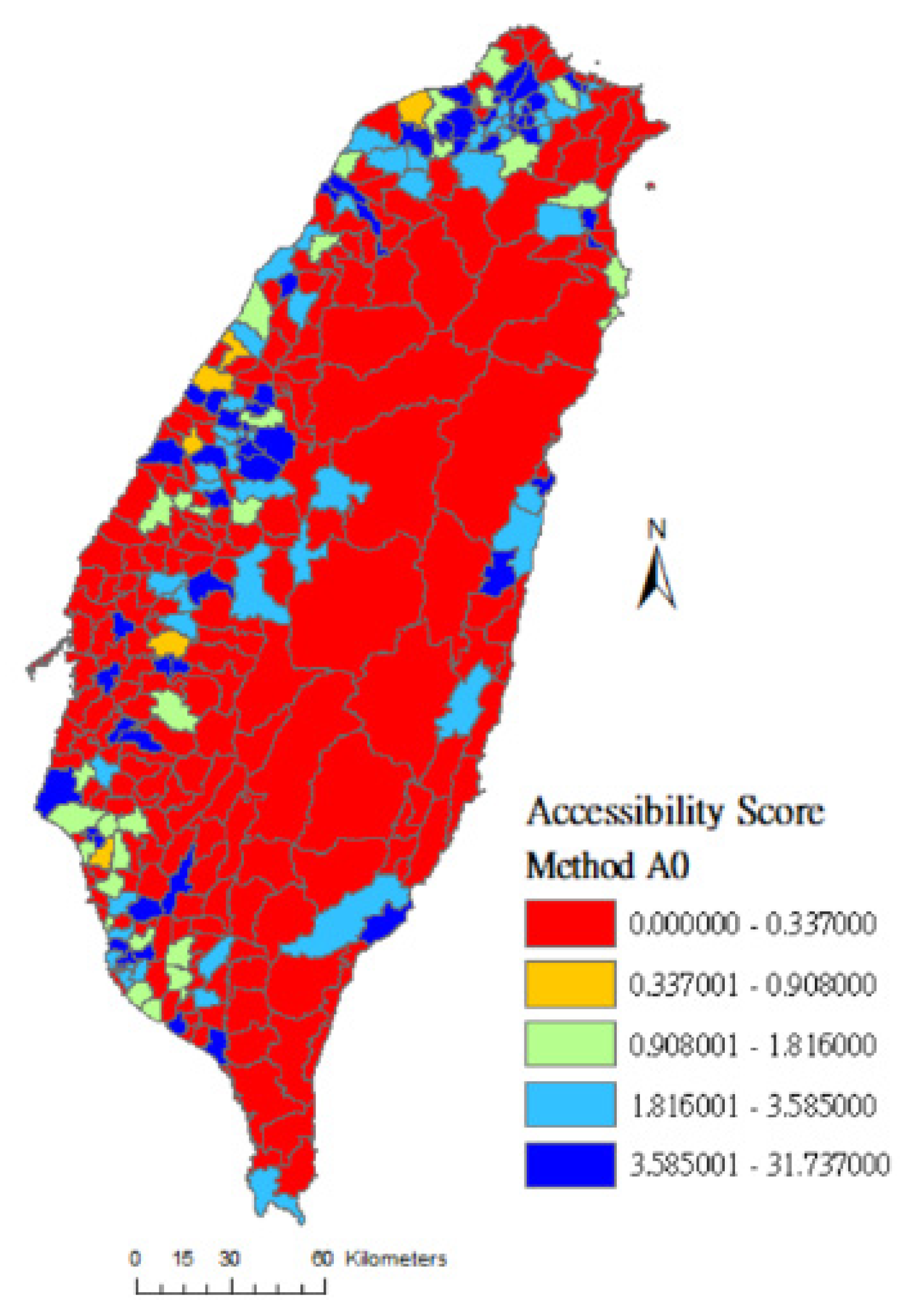
At present, Taiwan’s policy formulation relies on the regional average method in weighing medical resource accessibility. Taking each administrative region as a unit, the number of hospitals, medical personnel, and hospital beds per 10,000 (or per 100,000) people in the region is calculated and becomes a potential accessibility indicator for the framework of accessibility to medical resources [
30]. In terms of the assessment of medical resources, the method assumes that the administrative region equal to the activity space where people utilize medical resources and distances does not bring about differences in the usage of medical resources within the region. However, patients can seek treatments by crossing into different administrative regions in reality. This characteristic of spatial mobility is not taken into consideration in the regional average method, and this is where problems arise [
15]. The method was identified as method A0 in this study, with Equation (1) as follows:
where
Ai is the geographic accessibility score of a town
i and implies the average amount of supply point resources enjoyed by each person in demand in the region of the town
i;
represents the amount of supply point resources in region
i of the town;
Pi represents the population at demand aged 65 or above in the region
i of towns.
Luo and Wang [
14] proposed the two-step floating catchment area method, which breaks the aforementioned limitations caused by setting administrative regions as activity areas. Not only does the research method consider the possibilities of cross-region healthcare utilization by people, but it also sets a reasonable range of seeking treatment and, in turn, assesses the spatial accessibility of medical resources. The two-step floating catchment area method is primarily divided into two stages [
19,
21,
31]. In stage one, the service loads of each service provider of resources are calculated. In stage two, the ratios of resources that can be reached by each location of the population at demand are calculated to assess the geographic accessibility scores of resources [
20].
The three-step floating catchment area method [
32] is an advanced and improved search method derived from the two-step floating catchment area method. The new method evaluates different choice probabilities of the population at demand when people approach nearby locations of medical resources. The effects of hospitals’ capacities and travel distances on the utilization behavior of medical resources are specifically taken into consideration. The concept of this method is to calculate the probability of seeking treatment, which represents the probability of each patient to visit different hospitals through distance weighting and hospital capacities. The probability of seeking treatment is then used to estimate the average ability of the medical resource allocation of each hospital. In the same manner, with the hospitals’ capacities and distances from the served regions, the probability of each region in demand to visit different hospitals is calculated. According to the choice probabilities, the average ability of the medical resource allocation of each hospital will be allocated to the region in demand appropriately, wherein we obtain the distribution situation of geographical accessibility to medical resources in the research area.
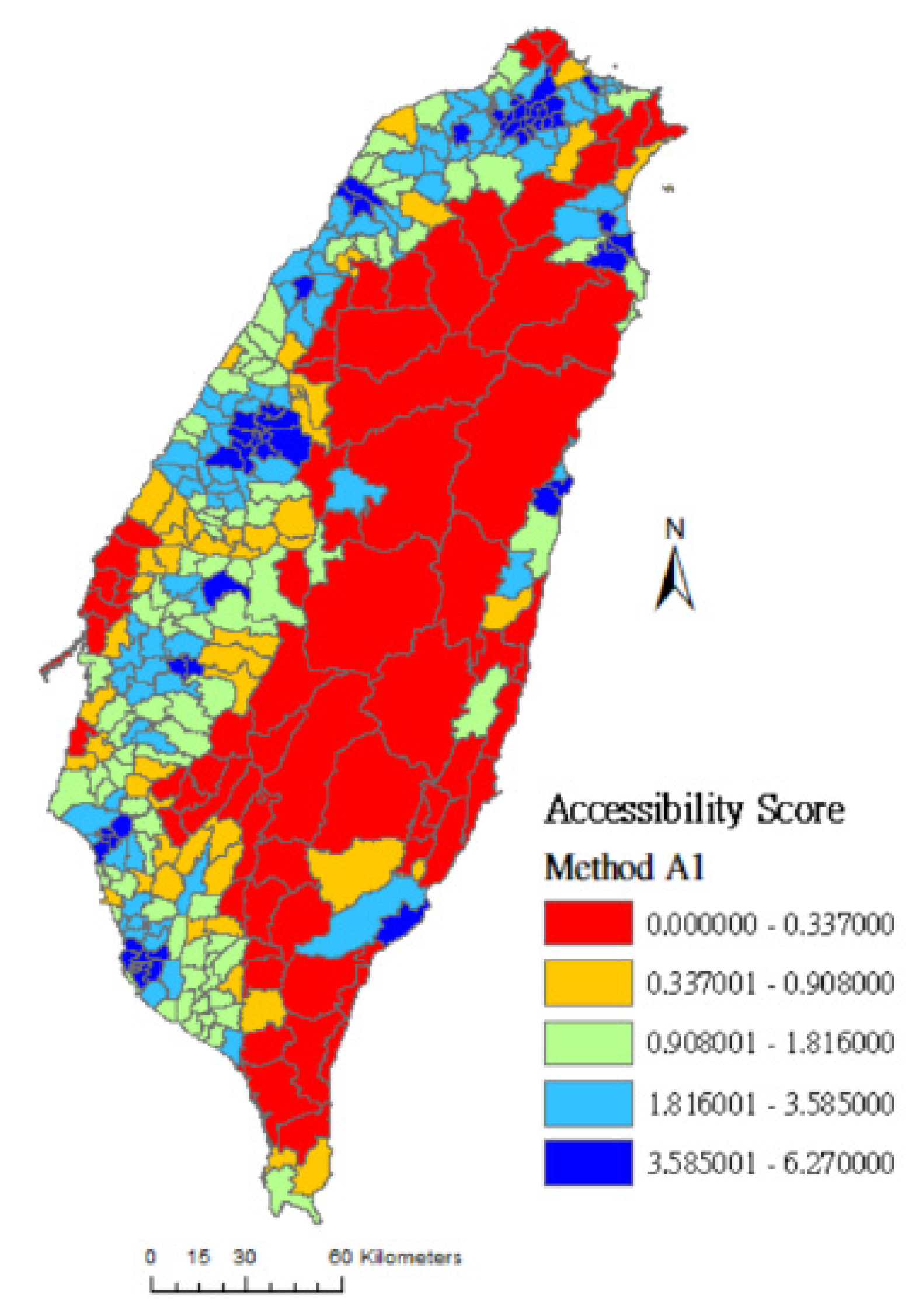
The calculation of geographical accessibility proposed in this study originates from the calculus concepts of the three-step floating catchment area method. Equations (2)–(5) are as follows:
where
Ai,1 is the simplest calculation of the geographical accessibility score of a location at demand
i and implies the average amount of supply point resources enjoyed by people at demand in the location at demand
i;
Sj represents the scale of supply at each service point (physiatrist)
j;
Pk represents the size of the elderly population in the location at demand
k;
dij is the route distance between the location at demand
i and the service point
j;
djk is the route distance between the service point
j and the location at demand
k. In the equations,
f(dij) is the distance-decay function, while the search radii of resources in this study are divided into three districts (
r = 1~3) according to the respective distance. The first district (
dij ≤ 3 km) is the area that the elderly can reach on foot in about an hour [
24]. The second district (3 km <
dij ≤ 15 km) is the area that the elderly can reach by driving for about half an hour. The third district (15 km <
dij ≤ 30 km) is the area that the elderly can reach by driving for about an hour.
f(dij) is shown in Equation (6):
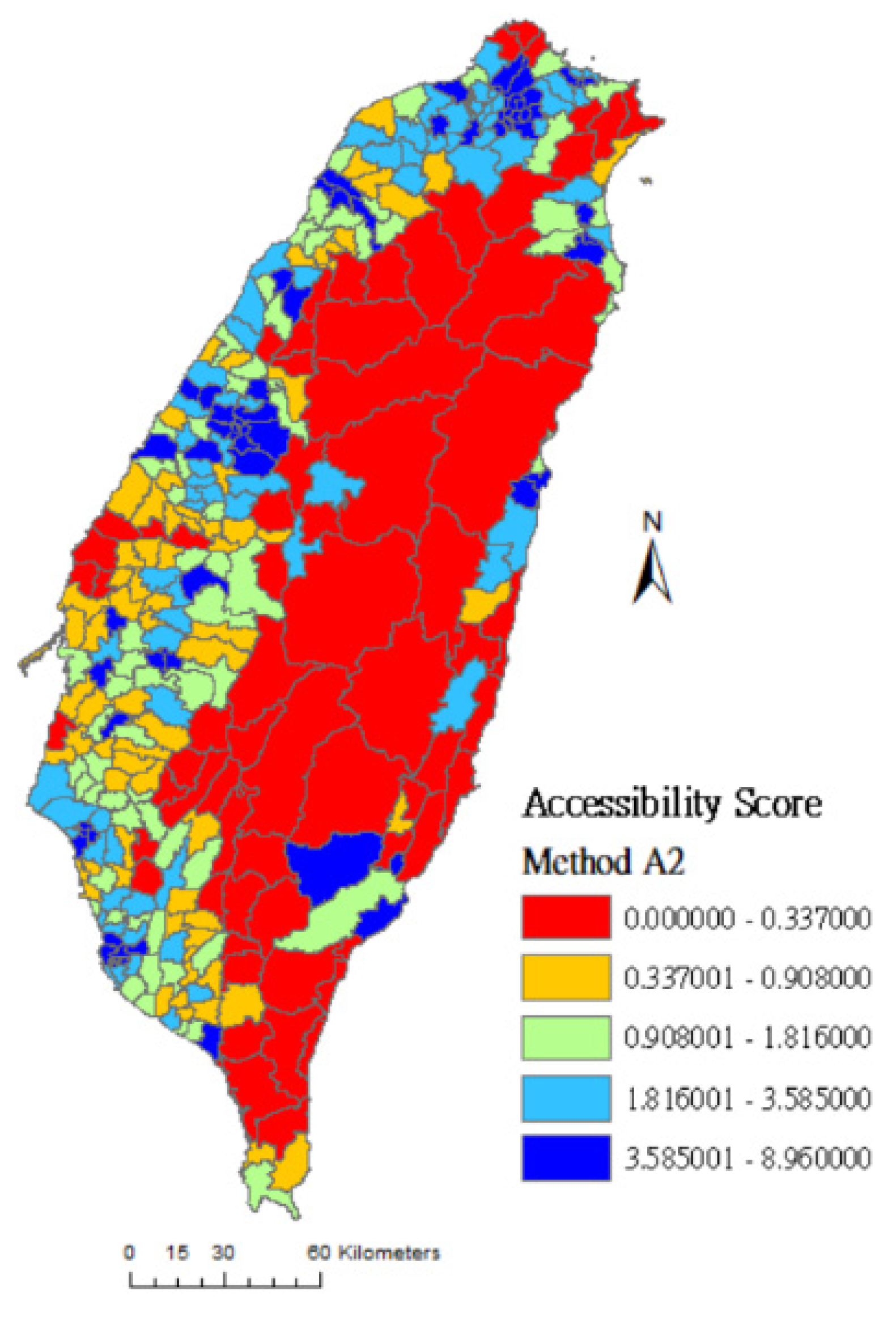
Ai,2 calculates the geographical accessibility score of a location at demand
i when
Kij, which is the different choice probabilities of the population at demand to approach various nearby service points, is taken into consideration. With considerations of the scale of supply at service points
Sj and distance decay
dij,
Kij represents the choice probabilities of the location at demand
i to service point
j and is expressed in Equation (7):
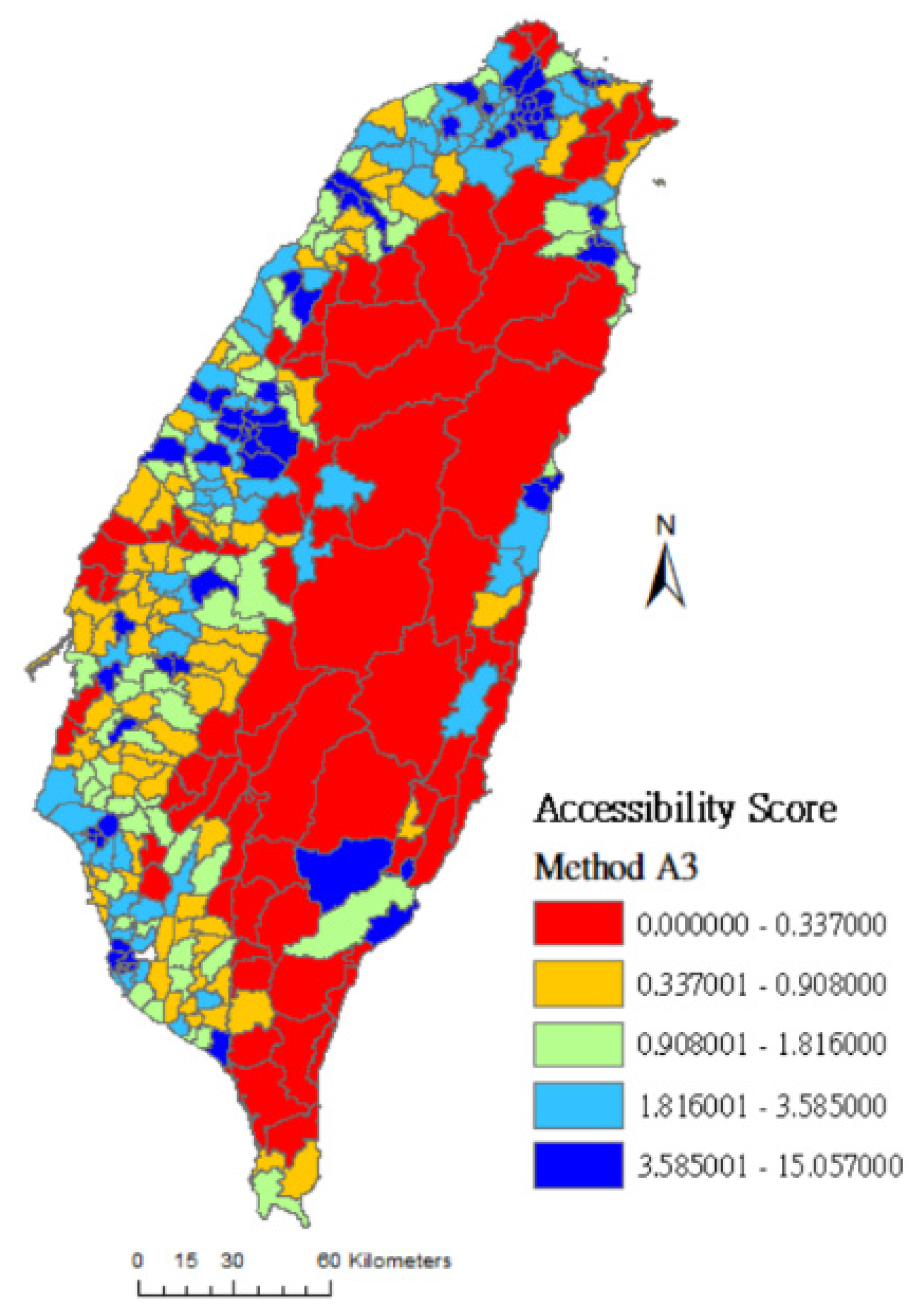
Ai,3 is a new method of calculation introduced in this study, which calculates the geographical accessibility score of a location at demand
i when
Vj, the overall rating of the location point
j summited to Google by ordinary users, is taken into consideration. It represents the crucial decision basis of people when they choose to visit a particular service point in reality. With considerations on rating
Vj and distance decay
dij,
Vij represents the choice probabilities of the location at demand
i to service point
j and is expressed in Equation (8):
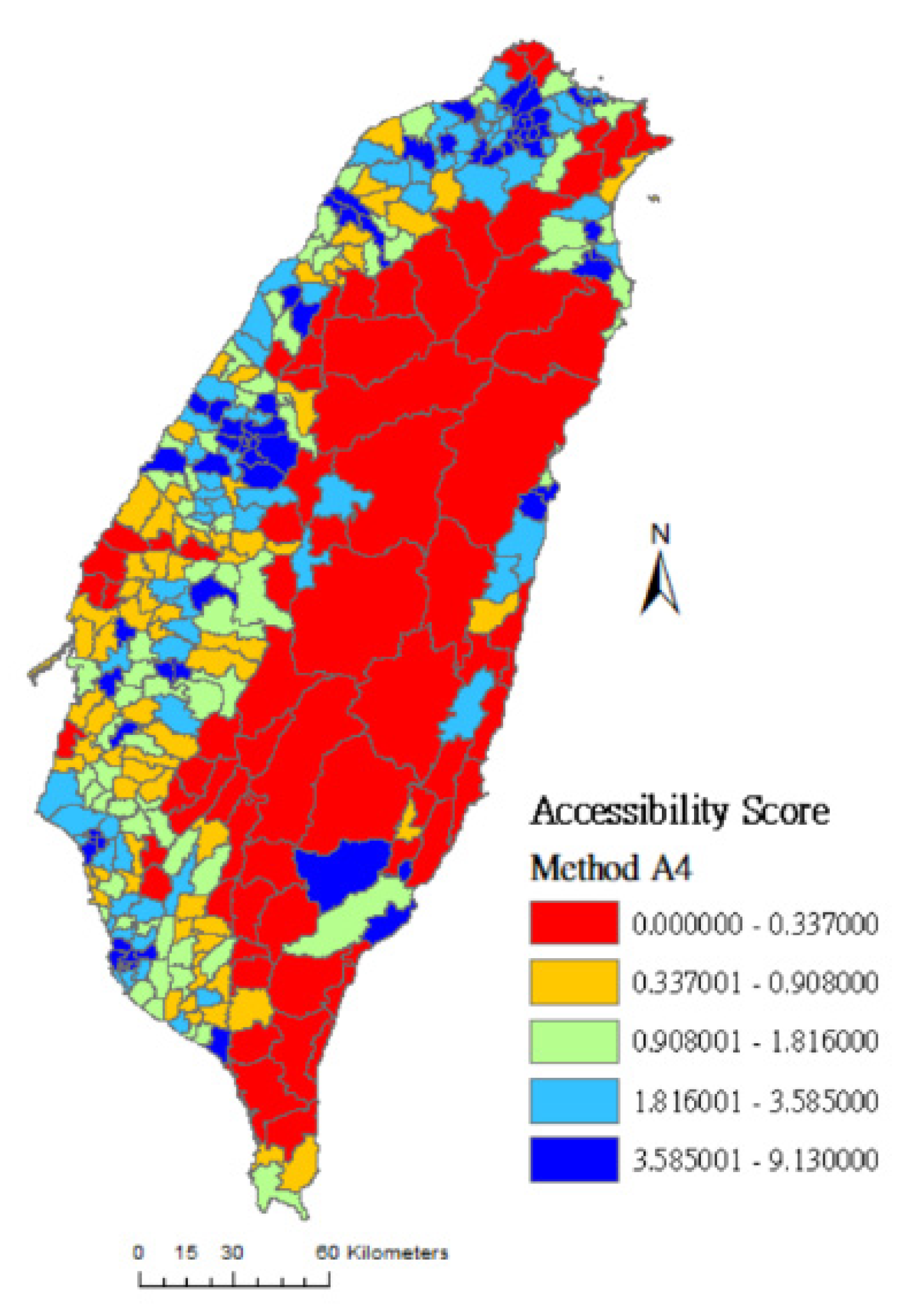
Ai,4 is another new method of calculation introduced in this study. It calculates the geographical accessibility score of a location at demand
i while integrating the factors of rating
Vj, the scale of supply at service points
Sj, distance decay
dij, and the different choice probabilities of the population at demand to approach various nearby service points
.
is expressed in Equation (9):
The flow of calculation follows Equations (1)–(8). First, we calculated the service load to be provided by each service point of physiatrists to the three districts divided by the distances and within a 30-km search radius of resources (the service load = the total population at demand in towns within a 30-km search radius/scale of service at the particular service point). Finally, we calculated the accumulated service load provided by the service points of physiatrists to each weighted center point of people at demand in towns, while the service points are within a 30-km search radius of the weighted center point. In this way, the accessible ratio of resources at the service points of physiatrists to the population at demand in towns was obtained, which is held to be the geographical accessibility score.
Table 1 shows the calculation equations used in this study to evaluate the geographic accessibility scores of physical rehabilitation resources.
2.3. Google Rating
In the era of Web 2.0, consumers increasingly rely on the rating mechanism of online service platforms as crucial factors for decision-making. The online rating mechanism has become an important asset in the digital “reputation” economy [
33]. For example, people who prepare to choose a hotel put a high value on the review scores left by tourists on travel information websites Agoda and Tripadvisor.
In 1995, Taiwan implemented the National Health Insurance policy, which provides convenient medical services to citizens. People are free to choose from various hospitals when they look for treatments. Faced with the competition in the free market, hospitals have adopted business models of marketing and branding to attract patients. Hospital rating mechanisms on online platforms, where people provide reviews voluntarily and freely, have emerged as crucial sources of references for patients’ healthcare-seeking decisions. Broadly speaking, rating mechanisms include blogging, Facebook, YouTube, and Google’s rating mechanism for businesses. Among them, Google Rating is the rating mechanism that performs best in structuring consumers’ feelings and is the most recognized by the public [
33,
34,
35]. Google Rating scores are divided into 1~5 points, representing evaluations ranging from least satisfied to most satisfied.
Based on the open competition in Taiwan’s medical market, the high degree of freedom enjoyed by people in seeking treatment, and the multiple choice factors in healthcare-seeking decisions, this study innovates and introduces new methods of calculating the geographic accessibility scores of physical rehabilitation resources, in which Google ratings for businesses is included as a choice factor in the calculation equations. The methods are detailed in the descriptions of methods A3 and A4 or Equations (7) and (8).
2.4. Gini Coefficient
The Gini coefficient was defined by Italian statistician Corrado Gini based on the Lorenz curve as a measure of income distribution equality within a society [
36]. The Gini coefficient can range from 1 to 0, wherein 1 represents complete inequality in people’s annual income distribution and 0 represents complete equality in income distribution. Generally speaking, a Gini coefficient below 0.2 indicates highly equitable income distribution, 0.2–0.3 represents equitable income distribution, 0.3–0.4 indicates bearable inequitable income distribution, 0.4–0.6 tends toward serious inequality in income distribution, and above 0.6 indicates high inequality in income distribution [
37]. Therefore, when the Gini coefficient is above 0.6, the ruling authority would usually be advised to be on the alert for excessive income inequality within the society, as the situation may lead to social conflicts. Due to its nature, the Gini coefficient is also called the inequality coefficient. With reference to the above-mentioned scaling of the coefficient, this study explains the disparity in the accessible ratio of resources at service points of physiatrists to the population at demand in counties/cities.
The Gini coefficient was used in this study to evaluate the equality of the accessible ratio of service point resources to the population at demand. Therefore, a higher Gini coefficient in a county/city represents a more inequitable distribution of resources at service points to the population at demand. Based on the definition of
y1 =
f(
x) of the Lorenz curve, the
y-axis measures the accumulated percentage of the accessible ratio of service point resources in each town, while the
x-axis measures the accumulated percentage of the population at demand in each town. The Gini coefficient is equal to the area between curve
y1 and line
y2, divided by the area below line
y2. The Equation (10) is as follows [
38]:









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}