The Psychometric Properties of the Patient Health Questionnaire-4 for Pregnant Women

Abstract
:1. Introduction
2. Materials and Methods
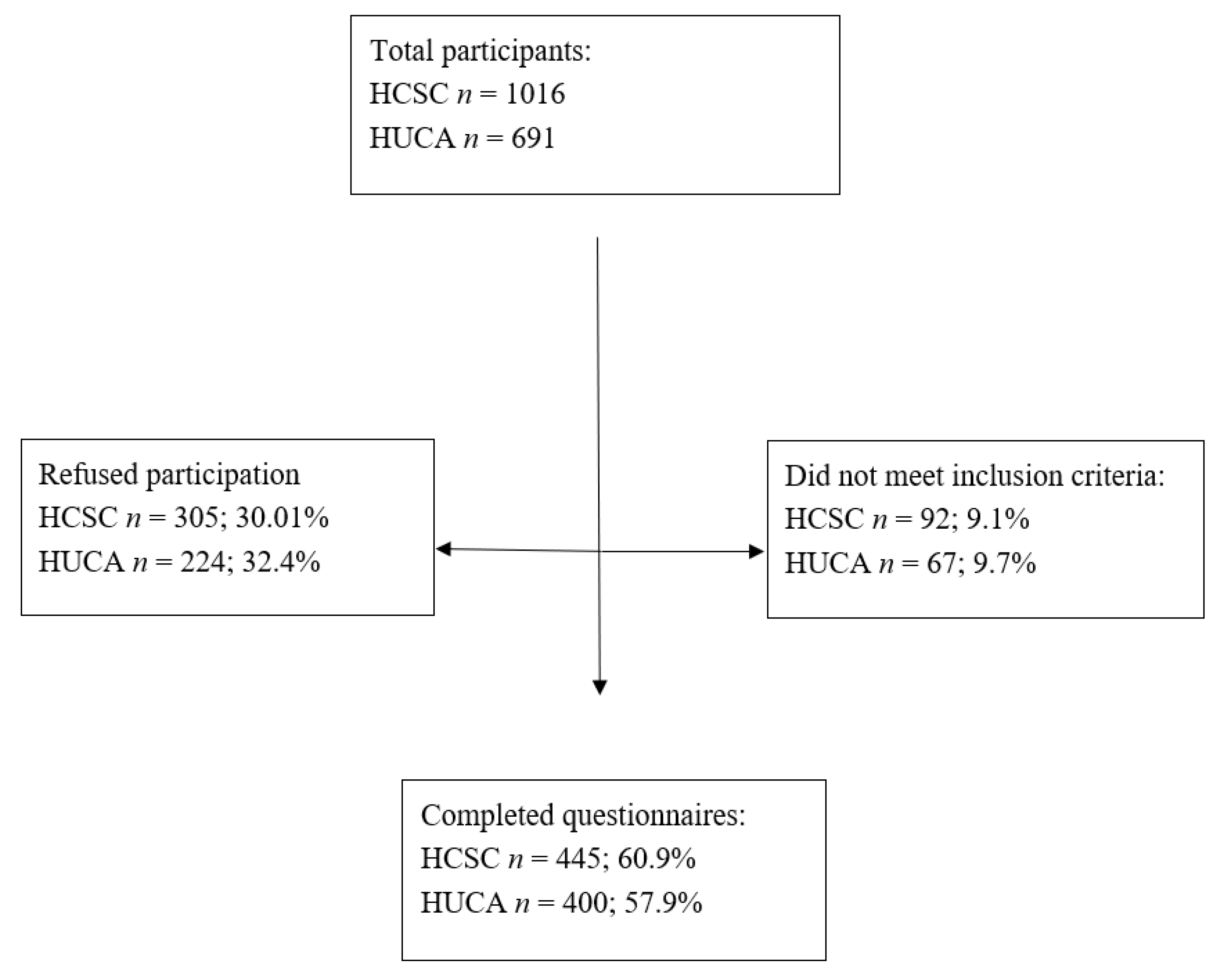
2.1. Study Population
2.2. Data Collection and Variable Specification
2.3. Instruments
2.3.1. The Patient Health Questionnaire (PHQ-2)
2.3.2. The Generalized Anxiety Disorder Scale (GAD-2)
2.3.3. The Patient Health Questionnaire (PHQ-4)
2.3.4. Statistical Analyses Overview
3. Results
3.1. Participant Characteristics
3.2. Reliability
3.3. Factor Analyses
3.4. Construct Validity
3.5. Analysis of Variance
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Caparrós-González, R.A.; Rodríguez Muñoz, M.F. Depresión posparto paterna: Visibilidad e influencia en la salud infantil. [Paternal postpartum depression: Visibility and influence on child health]. Clínica Salud 2020. [Google Scholar] [CrossRef]
- Bauer, A.; Knapp, M.; Parsonage, M. Lifetime costs of perinatal anxiety and depression. J. Affect. Disord. 2016, 192, 83–90. [Google Scholar] [CrossRef] [Green Version]
- Andersson, L.; Sundström-Poromaa, I.; Bixo, M.; Wulff, M.; Bondestam, K.; Åström, M. Point prevalence of psychiatric disorders during the second trimester of pregnancy: A population-based study. Am. J. Obstet. Gynecol. 2003, 189, 148–154. [Google Scholar] [CrossRef]
- Banti, S.; Mauri, M.; Oppo, A.; Borri, C.; Rambelli, C.; Ramacciotti, D.; Montagnani, M.; Camilleri, V.; Cortopassi, S.; Rucci, P.; et al. Prevalence, incidence, recurrence and new onset of depression durin pregnancy. Results from the perinatal depression-research & screening unit (PND-RESCU) study. Eur. Psychiatry 2010, 25, 1389. [Google Scholar]
- Escribà-Agüir, V.; Gonzalez-Galarzo, M.C.; Barona-Vilar, C.; Artazcoz, L. Factors related to depression during pregnancy: Are there gender differences? J. Epidemiol. Community Health 2008, 62, 410–414. [Google Scholar] [CrossRef]
- Rodríguez-Muñoz, M.F.; Le, H.N.; Vargas, I.; Olivares, M.E.; Izquierdo, N. Feasibility of screening and prevalence of prenatal depression in an obstetric setting in Spain. Eur. J. Obs. Gynecol. Reprod. Biol. 2017, 215, 101–105. [Google Scholar] [CrossRef]
- Dennis, C.L.; Kobra, F.H.; Shiri, R. Prevalence of antenatal and postnatal anxiety: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 210, 315–323. [Google Scholar] [CrossRef]
- Soto-Balbuena, C.; Rodríguez, M.F.; Escudero-Gomis, A.I.; Ferrer, F.J.; Le, H.N.; Grupo PMB-HUCA. Incidence, prevalence and risk factors related to anxiety symptoms during pregnancy. Psicothema 2018, 30, 257–263. [Google Scholar]
- Field, T. Prenatal depression effects on early development: A review. Infant Behav. Dev. 2011, 34, 1–14. [Google Scholar] [CrossRef]
- Zhong, Q.; Gelaye, B.; Zaslavsky, A.; Fann, J.; Ronden, M.; Sánchez, S.; Williams, M. Diagnostic validity of the generalized anxiety disorder-7 (GAD-7) among pregnant women. PLoS ONE 2015, 10, e0125096. [Google Scholar] [CrossRef]
- Vázquez, M.B.; Míguez, M.C. Spanish brief version of the Pregnancy Related Anxiety Questionnaire: PRAQ-20. Clínica Salud 2020. [Google Scholar] [CrossRef]
- Dunkel, C.; Tanner, L. Anxiety, depression and stress in pregnancy: Implications for mothers, children, research, and practice. Curr. Opin. Psychiatry 2012, 25, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Esteve, L.; Valdés, M. Manual de Psiquiatría Perinatal: Guía Para el Manejo de los Trastornos Mentales Durante el Embarazo, Postparto y Lactancia. [Perinatal Psychiatry Manual: Guide for the Management of Mental Disorders during Pregnancy, Postpartum and Lactation]; Panamericana: Madrid, Spain, 2017. [Google Scholar]
- Rodríguez-Muñoz, M.F.; Izquierdo, N.; Olivares, M.E.; Picos, M.C.; Rodríguez, M.I.; Herráiz, M.A.; Le, H.N.; Fonseca, J. Postpartum Depression Screening Scale Short Form: Is it possible to use it for antenatal depression? Clínica Salud 2018, 29, 147–150. [Google Scholar] [CrossRef] [Green Version]
- Marcos-Nájera, R.; Le, H.N.; Rodríguez-Muñoz, M.F.; Olivares, M.E.; Izquierdo, N. The structure of the Patient Health Questionnaire-9 in pregnant women in Spain. Midwifery 2018, 62, 36–41. [Google Scholar] [CrossRef]
- Lowë, B.; Kroenke, K.; Gräfe, K. Detecting and monitoring depression with a two-item questionnaire (PHQ-2). J. Psychosom. Res. 2005, 58, 163–171. [Google Scholar] [CrossRef]
- Rodríguez-Muñoz, M.F.; Castelao, P.C.; Olivares, M.E.; Soto, C.; Izquierdo, N.; Ferrer, J.; Le, H.N. PHQ-2 como primer instrumento de cribado de la depresión prenatal. Rev. Española Salud Pública 2017, 91, 1–8. [Google Scholar]
- Smith, M.; Gotman, N.; Lin, H.; Yonkers, K. Do the PHQ-8 and the PHQ-2 accurately screen for depressive disorders in a sample of pregnant women? Gen. Hosp. Psychiatry 2010, 32, 544–548. [Google Scholar] [CrossRef] [Green Version]
- Spitzer, R.L.; Kroenke, K.; Willians, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder, the GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Monahan, P.; Löwe, B. Anxiety disorders in primary care: Prevalence, impairment, comorbidity, and detection. Ann. Intern. Med. 2007, 146, 317–325. [Google Scholar] [CrossRef]
- Löwe, B.; Wahl, I.; Rose, M.; Spitzer, C.; Glaesmer, H.; Winterfeld, K.; Schneider, A.; Brähler, E. A 4-item measure of depression and anxiety: Validation and standardization of the patient health questionnaire-4 (PHQ-4) in the general population. J. Affect. Disord. 2010, 122, 86–95. [Google Scholar] [CrossRef]
- Penlington, C.; Araújo-Soares, V.; Durham, J. Predicting Persistent Orofacial Pain: The role of illness perceptions, anxiety, and depression. JDR Clin. Transl. Res. 2020, 5, 40–49. [Google Scholar] [CrossRef]
- Barrera, A.Z.; Moh, Y.S.; Nichols, A.; Le, H.N. The factor reliability and convergent validity of the patient health questionnaire-4 among an international sample of pregnant women. J. Womens Health 2020. [CrossRef]
- Kroenke, K.; Spitzer, R.; Williams, J.; Löwe, B. An ultra-brief screening scale for anxiety and depression: The PHQ-4. Psychosomatics 2009, 50, 613–621. [Google Scholar]
- Koncalevent, R.; Finck, C.; Jimenez-Leal, W.; Sautier, L.; Hinz, A. Standardization of the Colombian version of the PHQ-4 in the general population. BMC Psychiatry 2014, 14, 205. [Google Scholar]
- Mills, S.D.; Fox, R.S.; Pan, T.M.; Malcarne, V.L.; Roesch, S.C.; Robins Sadler, G. Psychometrics evaluation of the patient health questionnaire-4 in Hispanic Americans. Hisp. J. Behav. Sci. 2015, 37, 560–571. [Google Scholar] [CrossRef] [Green Version]
- Wubetu, A.D.; Habte, S.; Dagne, K. Prevalence of risky alcohol use behavior and associated factors in pregnant antenatal care attendees in Debre Berhan, Ethiopia, 2018. BMC Psychiatry 2019, 19, 250. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The Patient Health Questionnaire-2: Validity of a two-item depression screener. Med. Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef]
- Clout, D.; Brown, R. Sociodemographic, pregnancy, obstetric, and postnatal predictors of postpartum stress, anxiety and depression in new mothers. J. Affect. Disord. 2015, 188, 60–67. [Google Scholar] [CrossRef]
- Cano-Vindel, A.; Muñoz-Navarro, R.; Medrano, L.A.; Ruiz-Rodríguez, P.; González-Blanch, C.; Gómez-Castillo, M.D.; Capafons, A.; Chacón, F.; Santolaya, F. A computerized version of the Patient Health Questionnaire-4 as an ultra-brief screening tool to detect emotional disorders in primary care. J. Affect. Disord. 2018, 234, 247–255. [Google Scholar] [CrossRef]
- Biaggi, A.; Corno, S.; Pawlby, S.; Pariante, C. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef] [Green Version]
- Lancaster, C.A.; Gold, K.J.; Flynn, H.A.; Yoo, H.; Marcus, S.M.; Davis, M.M. Risk factors for depressive symptoms during pregnancy: A systematic review. J. Gen. Intern. Med. 2010, 202, 5–14. [Google Scholar] [CrossRef] [Green Version]
- NICE. Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance. 2014. Available online: https://www.nice.org.uk/guidance/cg192 (accessed on 1 September 2020).
- ACOG. Screening for Perinatal Depression. Obstet. Gynecol. 2015, 132, e208–e212. [Google Scholar] [CrossRef]
- Somerville, S.; Dedman, K.; Hagan, R. The Perinatal Anxiety Screening Scale: Development and preliminary validation. Arch. Womens Ment. Health 2014, 17, 443–454. [Google Scholar] [CrossRef]


{kind=link}
| n = 845 % | HCSC (n = 445) n (%) | HUCA (n = 400) n (%) | Χ2 | p-Value | |
|---|---|---|---|---|---|
| Age group | 1.166 | 0.125 | |||
| 16–25 years | 8.6 | 41 (10.0) | 29 (7.3) | ||
| 26–36 years | 60.0 | 234 (56.8) | 253 (63.4) | ||
| 36–45 years | 31.3 | 137 (33.3) | 117 (29.3) | ||
| Nationality | 68.239 | 0.000 | |||
| Spanish | 78.1 | 297 (66.9) | 361 (90.5) | ||
| Other | 21.9 | 147 (33.1) | 38 (9.5) | ||
| Education level | 18.163 | 0.000 | |||
| Primary | 17.3 | 55 (12.4) | 91 (22.9) | ||
| Secondary | 31.0 | 155 (34.8) | 106 (26.6) | ||
| University level | 51.7 | 235 (52.8) | 201 (50.5) | ||
| Employment status | 1.714 | 0.190 | |||
| Unemployed | 25.6 | 105 (23.8) | 110 (27.7) | ||
| Employed | 74.4 | 337 (76.2) | 287 (72.3) | ||
| Marital Status | 8.891 | 0.003 | |||
| Single | 11.5 | 65 (14.6) | 32 (8.1) | ||
| Partnered | 88.5 | 379 (85.4) | 365 (91.9) | ||
| History medical illness | 0.321 | 0.571 | |||
| No | 83.2 | 357 (82.4) | 334 (83.9) | ||
| Yes | 16.8 | 76 (14.6) | 64 (16.1) | ||
| Previous depression history | 0.170 | 0.680 | |||
| No | 97.5 | 420 (97.7) | 385 (97.2) | ||
| Yes | 2.5 | 10 (2.3) | 11 (2.8) | ||
| First-time mother | 0.130 | 0.719 | |||
| No | 54.2 | 232 (54.4) | 204 (51.1) | ||
| Yes | 45.8 | 211 (47.6) | 195 (48.9) |
| Item | n | M | SD | ra | α |
|---|---|---|---|---|---|
| Depression items (PHQ-2) | 824 | ||||
| Little interest or pleasure in doing things | 0.84 | 0.86 | 0.74 ** | ||
| Feeling down, depressed, or hopeless | 0.50 | 0.76 | 0.79 ** | ||
| lePHQ-2 sum score | 1.35 | 1.41 | 0.70 | ||
| Anxiety items (GAD-2) | 814 | ||||
| Feeling nervous, anxious or on edge | 0.67 | 0.80 | 0.75 ** | ||
| Not being able to stop or control worrying | 0.42 | 0.71 | 0.80 ** | ||
| GAD-2 sum score | 1.13 | 1.36 | 0.75 | ||
| Total scale score (PHQ-4) | 806 | 2.47 | 2.40 | 0.77 |
| One-Factor | Two-Factor | ||
|---|---|---|---|
| Item | Anxiety-Depression | Factor 1-Anxiety | Factor 2-Depression |
| 1. Little interest or pleasure in doing things | 0.714 | 0.909 | |
| 2. Feeling down, depressed, or hopeless | 0.799 | 0.769 | |
| 3. Feeling nervous, anxious or on edge | 0.753 | 0.906 | |
| 4. Not being able to stop or control worrying | 0.818 | 0.812 | |
| Model | X2 | X2/df | RMSEA | CFI | NFI | AIC | ECVI | PNFI |
|---|---|---|---|---|---|---|---|---|
| Two-factor | 5.006 | 5.006 | 0.069 | 0.99 | 0.91 | 31.006 | 0.037 | 0.09 |
| One-factor | 104.127 | 52.063 | 0.246 | 0.89 | 0.88 | 128.127 | 0.152 | 0.178 |
| PHQ-2, n = 824 | GAD-2, n = 814 | PHQ-4, n = 806 | ||||
|---|---|---|---|---|---|---|
| M (SD) | Group Differences p-Value | M (SD) | Group Differences p-Value | M (SD) | Group Differences p-Value | |
| Age group | 0.026 | 0.580 | 0.063 | |||
| 16–25 | 1.82 (1.67) | 1.29 (1.53) | 3.15 (2.78) | |||
| 26–35 | 1.32 (1.41) | 1.15 (1.36) | 2.47 (2.45) | |||
| 36–45 | 1.33 (1.37) | 1.09 (1.32) | 2.37 (2.45) | |||
| Education level | 0.000 | 0.017 | 0.000 | |||
| Primary | 1.59 (1.61) | 1.26 (1.48) | 2.83 (2.66) | |||
| Secondary | 1.60 (1.57) | 1.29 (1.45) | 2.90 (2.71) | |||
| University | 1.14 (1.22) | 1.00 (1.26) | 2.12 (2.07) | |||
| Employment status | 0.049 | 0.234 | 0.074 | |||
| Unemployed | 1.53 (1.60) | 1.23 (1.44) | 2.75 (2.73) | |||
| Employed | 1.29 (1.34) | 1.10 (1.33) | 2.37 (2.28) | |||
| Marital Status | 0.089 | 0.468 | 0.437 | |||
| Single | 1.63 (1.67) | 1.24 (1.51) | 2.86 (2.72) | |||
| Partnered | 1.32 (1.38) | 1.12 (1.34) | 2.42 (2.36) | |||
| History of medical illness | 0.031 | 0.268 | 0.059 | |||
| No | 1.30 (1.34) | 1.10 (1.31) | 2.38 (2.24) | |||
| Yes | 1.63 (1.70) | 1.26 (1.57) | 2.89 (2.99) | |||
| Smoking | 0.029 | 0.47 | 0.046 | |||
| No | 1.37 (1.43) | 1.26 (139) | 2.61 (2.41) | |||
| Yes | 1.80 (1.73) | 1.38 (1.49) | 3.20 (2.86) | |||
| Previous depression history | 0.013 | 0.001 | 0.01 | |||
| No | 1.31 (1.37) | 1.08 (1.30) | 2.37 (2.30) | |||
| Yes | 2.63 (2.09) | 2.78 (1.90) | 5.53 (3.33) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Muñoz, M.d.l.F.; Ruiz-Segovia, N.; Soto-Balbuena, C.; Le, H.-N.; Olivares-Crespo, M.E.; Izquierdo-Méndez, N. The Psychometric Properties of the Patient Health Questionnaire-4 for Pregnant Women. Int. J. Environ. Res. Public Health 2020, 17, 7583. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207583
Rodríguez-Muñoz MdlF, Ruiz-Segovia N, Soto-Balbuena C, Le H-N, Olivares-Crespo ME, Izquierdo-Méndez N. The Psychometric Properties of the Patient Health Questionnaire-4 for Pregnant Women. International Journal of Environmental Research and Public Health. 2020; 17(20):7583. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207583
Chicago/Turabian StyleRodríguez-Muñoz, María de la Fe, Natalia Ruiz-Segovia, Cristina Soto-Balbuena, Huynh-Nhu Le, María Eugenia Olivares-Crespo, and Nuria Izquierdo-Méndez. 2020. "The Psychometric Properties of the Patient Health Questionnaire-4 for Pregnant Women" International Journal of Environmental Research and Public Health 17, no. 20: 7583. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207583