Using Machines or Free Weights for Resistance Training in Novice Males? A Randomized Parallel Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Approach to the Problem
2.2. Participants
2.3. Procedures
2.3.1. RT Program
2.3.2. Outcome Measures
2.4. Statistical Analysis
3. Results
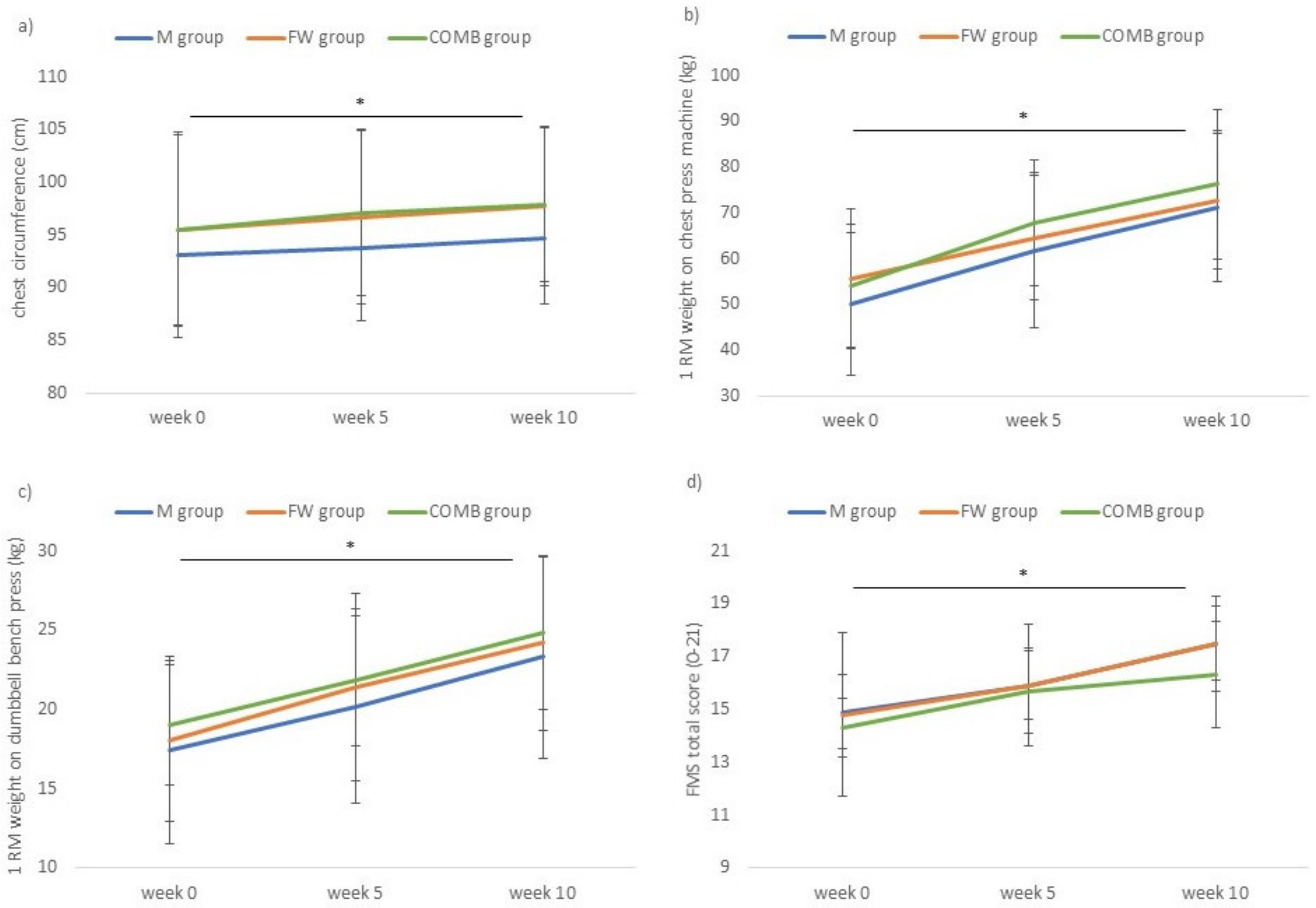
3.1. Anthropometrics
3.2. Strength
3.2.1. 1-RM Estimations on Machines
3.2.2. 1-RM Estimations on Free Weights
3.2.3. Standing Broad Jump
3.3. Functional Ability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine Position Stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [PubMed]
- Carroll, T.J.; Barry, B.; Riek, S.; Carson, R.G. Resistance training enhances the stability of sensorimotor coordination. Proc. R. Soc. B Biol. Sci. 2001, 268, 221–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiesel, K.; Plisky, P.J.; Voight, M.L. Can Serious Injury in Professional Football be Predicted by a Preseason Functional Movement Screen? North Am. J. Sports Phys. Ther. 2007, 2, 147–158. [Google Scholar]
- Peate, W.F.; Bates, G.; Lunda, K.; Francis, S.; Bellamy, K. Core strength: A new model for injury prediction and prevention. J. Occup. Med. Toxicol. 2007, 2, 3. [Google Scholar] [CrossRef] [Green Version]
- Ratamess, N.A.; Alvar, B.A.; Evetoch, T.K.; Housh, T.J.; Kibler, W.B.; Kraemer, W.J.; Triplett, N.T. American College of Sports Medicine Position Stand. Progression Models in Resistance Training for Healthy Adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar]
- Haff, G.G. Roundtable Discussion: Machines Versus Free Weights. Strength Cond. J. 2000, 22, 18. [Google Scholar] [CrossRef]
- Behm, D.G.; Anderson, K.G. The role of instability with resistance training. J. Strength Cond. Res. 2006, 20, 716–722. [Google Scholar]
- Schick, E.E.; Coburn, J.W.; Brown, L.E.; Judelson, D.A.; Khamoui, A.V.; Tran, T.T.; Uribe, B.P. A comparison of muscle activation between a Smith machine and free weight Bench Press. J. Strength Cond. Res. 2010, 24, 779–784. [Google Scholar] [CrossRef]
- Coratella, G.; Tornatore, G.; Longo, S.; Esposito, F.; Cè, E. Specific prime movers’ excitation during free-weight bench press variations and chest press machine in competitive bodybuilders. Eur. J. Sport Sci. 2020, 20, 571–579. [Google Scholar] [CrossRef]
- Schott, N.; Johnen, B.; Holfelder, B. Effects of free weight and machine training on muscular strength in high-functioning older adults. Exp. Geront. 2019, 122, 15–24. [Google Scholar] [CrossRef]
- Rossi, F.E.; Schoenfeld, B.J.; Ocetnik, S.; Young, J.; Vigotsky, A.; Contreras, B.; Krieger, J.; Miller, M.; Cholewa, J. Strength, body composition, and functional outcomes in the squat versus leg press exercises. J. Sports Med. Phys. Fit. 2018, 58, 263–270. [Google Scholar]
- Schwartz, N.A.; Harper, S.P.; Waldhelm, A.; McKinley-Barnard, S.K.; Holden, S.L.; Kovaleski, J.E. A comparison of machine versus free-weight squats for the enhancement of lower-body power, speed, and the change-of-direction ability during an initial training phase of recreationally-active women. Sports 2019, 7, 215. [Google Scholar] [CrossRef] [Green Version]
- Kraemer, W.J.; Ratamess, N.A. Hormonal responses and adaptations to resistance exercise and training. Sports Med. 2005, 35, 339–361. [Google Scholar] [CrossRef] [PubMed]
- Herbst, K.L.; Bhasin, S. Testosterone action on skeletal muscle. Curr. Opin. Clin. Nutr. Metab. Care 2004, 7, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Lavallee, M.E.; Balam, T. An overview of strength training injuries: Acute and chronic. Curr. Sports Med. Rep. 2010, 9, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Barnett, M.L.; Ross, D.; Schmidt, R.A.; Todd, B. Motor Skills Learning and the Specificity of Training Principle. Research Quarterly. Res. Q. Am. Assoc. Health Phys. Educ. Recreat. 1973, 44, 440–447. [Google Scholar]
- Boyer, B.T. A comparison of the effects of three strength training programs on women. J. Appl. Sports Sci. Res. 1990, 4, 88–94. [Google Scholar]
- Stone, M.H.; Collins, D.; Plisk, S.; Haff, G.; Stone, M.E. Training Principles: Evaluation of Modes and Methods of Resistance Training. Strength Cond. J. 2004, 22, 65–76. [Google Scholar] [CrossRef]
- Seynnes, O.R.; de Boer, M.; Narici, M.V. Early skeletal muscle hypertrophy and architectural changes in response to high-intensity resistance training. J. Appl. Physiol. 2006, 102, 368–373. [Google Scholar] [CrossRef]
- Cadore, E.L.; González-Izal, M.; Pallarés, J.G.; Rodriguez-Falces, J.; Häkkinen, K.; Kraemer, W.J.; Pinto, R.S.; Izquierdo, M. Muscle conduction velocity, strength, neural activity, and morphological changes after eccentric and concentric training. Scand. J. Med. Sci. Sports 2014, 24, 343–352. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Correa Mesa, J.F.; Cruz Martinez, L.E.; Correa Morales, J.C.; Rojas Valencia, J.T. Maximum Heart Rate during exercise: Reliability of the 220-age and Tanaka formulas in healthy young people at a moderate altitude. Rev. Fac. Med. 2015, 62, 579–585. [Google Scholar] [CrossRef]
- Marfell-Jones, M.; Olds, T.; De Ridder, J. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Potchefstroom, South Africa, 2011; 137p. [Google Scholar]
- Flegal, K.M.; Shepherd, J.A.; Looker, A.C.; Graubard, B.I.; Borrud, L.G.; Ogden, C.L.; Harris, T.B.; Everhart, J.E.; Schenker, N. Comparisons of percentage body fat, body mass index, waist circumference, and waist-stature ratio in adults. Am. J. Clin. Nutr. 2009, 89, 500–508. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines of Exercise Testing and Prescription, 9th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2014; p. 96. [Google Scholar]
- Hertling, D.; Kessler, R.M. Management of Common Musculoskeletal Disorders: Physical Therapy Principles and Methods, 4th ed.; Lippincot Williams & Wilkins: Philadelphia, PA, USA, 2006; pp. 307–308. [Google Scholar]
- Kraus, K.; Schütz, E.; Taylor, W.R.; Doyscher, R. Efficacy of the Functional Movement Screen. A Review. J. Strength Cond. Res. 2014, 28, 3571–3584. [Google Scholar] [CrossRef]
- Cook, G. Movement: Functional Movement Systems: Screening, Assessment, Corrective Strategies; Lotus Publishing: Chichester, UK, 2011; 416p. [Google Scholar]
- Campos, G.E.R.; Luecke, T.J.; Wendeln, H.K.; Toma, K.; Hagerman, F.C.; Murray, T.F.; Ragg, K.E.; Ratamess, N.A.; Kraemer, W.J.; Staron, R.S. Muscular adaptations in response to three different resistance-training regimens: Specificity of repetition maximum training zones. Eur. J. Appl. Physiol. 2002, 88, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.J.; Churchward-Venne, T.A.; West, D.W.; Burd, N.A.; Breen, L.; Baker, S.K.; Philips, S.M. Resistance exercise load does not determine training-mediated hypertrophic gains in young men. J. Appl. Physiol. 2012, 113, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Moro, T.; Marcolin, G.; Bianco, A.; Bolzetta, F.; Berton, L.; Sergi, G.; Paoli, A. Effects of 6 weeks of traditional resistance training or high intensity interval resistance training on body composition, aerobic power and strength in healthy young subjects: A randomized parallel trial. Int. J. Environ. Res. Public Health 2020, 17, 4093. [Google Scholar] [CrossRef]
- Buckner, S.L.; Jessee, M.B.; Mouser, J.G.; Dankel, S.J.; Mattocks, K.T.; Bell, Z.W.; Abe, T.; Loenneke, J.P. The basics of training for muscle size and strength: A brief review on the theory. Med. Sci. Sports Exerc. 2020, 52, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Baechle, T.; Earle, R.; Wathen, D. Essentials of Strength and Conditioning; Human Kinetics: Leeds, UK, 2000; pp. 395–425. [Google Scholar]
- McCaw, S.T.; Friday, J.J. A comparison of muscle activity between a free weight and machine bench press. J. Strength Cond. Res. 1994, 8, 259–264. [Google Scholar]
- Lee, S.Y.; Gallagher, D. Assessment methods in human body composition. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 566–572. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Machine Exercise | Free Weight Exercise | Primary Movers |
|---|---|---|
| Leg press | Squat (barbell) | M. Quadriceps femoris + M. Hamstrings + M. Glutei |
| Chest press | Bench press (dumbbells) | M. Pectoralis major and minor + M. Triceps brachii + M. Deltoideus pars clavicularis |
| Hip extension | Deadlift (barbell) | M. Hamstrings + M. Glutei + M. Erector spinae |
| Seated row | Bent over row (dumbbells) | M. Latissimus dorsi + M. Trapezius |
| Shoulder press | Standing shoulder press (dumbbells) | M. Deltoideus + M. Triceps brachii |
| Pre Tests | Week 1–5 | Mid Tests | Week 6–10 | Post Tests | |
|---|---|---|---|---|---|
| Using machines in RT program | M + COMB | M | |||
| Using free weights in RT program | FW | FW + COMB | |||
| 1-RM test for machines + free weights | M + FW + COMB | ||||
| 1-RM test for free weights + 1-RM machines derived from preceding training | M + COMB | M | |||
| 1-RM test for machines + 1-RM free weights derived from preceding training | FW | FW + COMB | |||
| Anthropometric tests + SBJ + Functional Movement ScreenTM | M + FW + COMB | M + FW + COMB | M + FW + COMB |
| Anthropometric Outcomes | RT Group | Pre-Intervention (0 Weeks) | Mid-Intervention (5 Weeks) | Post-Intervention (10 Weeks) | Univariate p-Value and (ηp2) of the Interaction Effect |
|---|---|---|---|---|---|
| Body weight (kg) | M | 78.3 ± 9.0 | 77.7 ± 9.2 | 78.4 ± 8.9 | 0.465 |
| FW | 80.6 ± 11.1 | 80.4 ± 10.8 | 80.1 ± 10.7 | (0.05) | |
| COMB | 80.4 ± 9.1 | 80.1 ± 8.9 | 80.5 ± 9.3 | ||
| Total | 79.7 ± 9.5 | 79.4 ± 9.4 | 79.7 ± 9.4 | ||
| Upper arm circumference relaxed (cm) | M | 30.5 ± 2.7 | 31.1 ± 2.6 | 31.7 ± 2.6 | 0.044 |
| FW | 30.5 ± 3.1 | 31.0 ± 2.9 | 31.1 ± 2.9 | (0.146) | |
| COMB | 30.4 ± 2.0 | 31.4 ± 2.2 | 32.0 ± 2.4 | ||
| Total | 30.4 ± 2.6 | 31.2 ± 2.5 | 31.6 ± 2.7 | ||
| Upper arm circumference flexed (cm) | M | 33.0 ± 2.7 | 33.5 ± 3.0 | 33.9 ± 3.0 | 0.757 |
| FW | 33.1 ± 2.6 | 33.6 ± 2.8 | 34.1 ± 3.2 | (0.022) | |
| COMB | 33.1 ± 2.8 | 33.8 ± 2.8 | 34.3 ± 3.0 | ||
| Total | 33.0 ± 2.7 | 33.6 ± 2.8 | 34.1 ± 3.0 | ||
| Thigh circumference (cm) | M | 51.6 ± 3.7 | 52.5 ± 3.1 | 53.1 ± 2.8 | 0.386 |
| FW | 53.8 ± 2.9 | 54.0 ± 2.4 | 54.2 ± 2.2 | (0.057) | |
| COMB | 52.7 ± 1.8 | 53.4 ± 1.6 | 54.0 ± 1.8 | ||
| Total | 52.7 ± 2.9 | 53.3 ± 2.4 | 53.8 ± 2.3 | ||
| Chest circumference (cm) | M | 93.1 ± 7.8 | 93.8 ± 7.0 | 94.7 ± 6.2 | 0.728 |
| FW | 95.5 ± 9.2 | 96.7 ± 8.2 | 97.7 ± 7.6 | (0.024) | |
| COMB | 95.5 ± 9.0 | 97.1 ± 7.9 | 97.9 ± 7.3 | ||
| Total | 94.7 ± 8.5 | 95.9 ± 7.6 | 96.7 ± 7.0 | ||
| Waist circumference (cm) | M | 86.1 ± 12.0 | 85.4 ± 12.4 | 85.6 ± 11.2 | 0.657 |
| FW | 85.6 ± 8.0 | 84.9 ± 7.7 | 84.8 ± 7.8 | (0.037) | |
| COMB | 83.2 ± 8.4 | 83.0 ± 8.5 | 83.4 ± 8.1 | ||
| Total | 85.0 ± 9.4 | 84.4 ± 9.5 | 84.6 ± 9.0 |
| Strength Outcomes | RT Group | Pre-Intervention (0 Weeks) | Mid-Intervention (5 Weeks) | Post-Intervention (10 Weeks) | Univariate p -Value and (ηp2) of the Interaction Effect |
|---|---|---|---|---|---|
| Leg press (kg) a | M | 117.8 ± 47.6 | 132.3 ± 46.2 | 153.2 ± 48.3 | 0.756 |
| FW | 128.6 ± 56.8 | 150.1 ± 61.3 | 167.5 ± 67.5 | (0.021) | |
| COMB | 124.8 ± 32.2 | 150.2 ± 36.3 | 166.5 ± 44.9 | ||
| Total | 123.7 ± 45.6 | 144.2 ± 48.3 | 162.4 ± 54.6 | ||
| Squat (kg) b | M | 50.9 ± 20.6 | 61.0 ± 20.7 | 76.0 ± 18.6 | 0.481 |
| FW | 53.8 ± 23.2 | 65.9 ± 24.8 | 74.8 ± 25.7 | (0.047) | |
| COMB | 50.6 ± 9.6 | 59.9 ± 9.6 | 70.1 ± 14.1 | ||
| Total | 51.7 ± 18.3 | 62.3 ± 19.1 | 73.6 ± 19.6 | ||
| Chest press (kg) a | M | 50.0 ± 15.5 | 61.8 ± 17.0 | 71.1 ± 16.2 | 0.657 |
| FW | 55.6 ± 15.1 | 64.5 ± 13.5 | 72.8 ± 15.1 | (0.033) | |
| COMB | 53.9 ± 13.5 | 67.8 ± 13.7 | 76.2 ± 16.3 | ||
| Total | 53.2 ± 14.5 | 64.7 ± 14.6 | 73.4 ± 15.6 | ||
| Dumbbell bench press (kg) b | M | 17.4 ± 5.9 | 20.2 ± 6.1 | 23.3 ± 6.4 | 0.974 |
| FW | 18.0 ± 5.1 | 21.4 ± 5.9 | 24.2 ± 5.5 | (0.005) | |
| COMB | 19.0 ± 3.8 | 21.8 ± 4.1 | 24.8 ± 4.8 | ||
| Total | 18.1 ± 4.9 | 21.1 ± 5.3 | 24.1 ± 5.5 | ||
| Hip extension (kg) a | M | 46.6 ± 13.7 | 55.6 ± 13.6 | 65.6 ± 16.5 | 0.724 |
| FW | 55.7 ± 18.1 | 66.9 ± 17.9 | 73.0 ± 14.7 | (0.025) | |
| COMB | 48.9 ± 18.0 | 62.7 ± 19.8 | 70.5 ± 21.3 | ||
| Total | 50.4 ± 16.7 | 61.7 ± 18.5 | 60.0 ± 18.8 | ||
| Deadlift (kg) b | M | 44.9 ± 17.4 | 51.4 ± 18.8 | 59.9 ± 18.8 | 0.446 |
| FW | 50.6 ± 23.6 | 62.4 ± 28.4 | 73.3 ± 28.3 | (0.051) | |
| COMB | 45.3 ± 15.1 | 51.4 ± 16.3 | 63.2 ± 22.8 | ||
| Total | 46.9 ± 28.3 | 55.0 ± 21.7 | 65.5 ± 23.7 | ||
| Seated row (kg) a | M | 53.6 ± 15.3 | 61.7 ± 14.2 | 71.6 ± 17.8 | 0.753 |
| FW | 62.5 ± 14.0 | 71.1 ± 12.0 | 77.3 ± 14.5 | (0.021) | |
| COMB | 59.2 ± 19.5 | 68.1 ± 14.3 | 73.1 ± 14.9 | ||
| Total | 58.4 ± 16.4 | 67.0 ± 13.8 | 74.0 ± 15.6 | ||
| Dumbbell bent over row (kg) b | M | 16.7 ± 5.4 | 19.2 ± 4.7 | 21.2 ± 5.8 | 0.935 |
| FW | 18.6 ± 5.4 | 21.7 ± 5.6 | 23.0 ± 5.5 | (0.008) | |
| COMB | 16.1 ± 3.6 | 19.1 ± 4.7 | 21.2 ± 4.8 | ||
| Total | 17.1 ± 4.8 | 20.0 ± 5.0 | 21.8 ± 5.3 | ||
| Shoulder press (kg) a | M | 35.3 ± 13.4 | 40.2 ± 12.7 | 47.6 ± 15.2 | 0.662 |
| FW | 36.5 ± 8.8 | 42.9 ± 11.6 | 50.3 ± 13.4 | (0.029) | |
| COMB | 43.0 ± 17.0 | 52.0 ± 20.3 | 56.3 ± 20.9 | ||
| Total | 38.3 ± 12.6 | 45.1 ± 15.8 | 51.4 ± 16.7 | ||
| Standing dumbbell shoulder press (kg) b | M | 11.7 ± 2.8 | 14.1 ± 2.9 | 15.8 ± 3.1 | 0.832 |
| FW | 12.1 ± 3.3 | 14.5 ± 3.0 | 16.1 ± 3.1 | (0.015) | |
| COMB | 12.0 ± 3.2 | 13.8 ± 3.6 | 15.5 ± 3.8 | ||
| Total | 11.9 ± 3.0 | 14.1 ± 3.1 | 15.8 ± 3.3 | ||
| Standing broad jump (cm) | M | 179.7 ± 28.2 | 184.0 ± 28.6 | 185.5 ± 28.2 | 0.108 |
| FW | 184.4 ± 29.9 | 193.1 ± 32.3 | 198.2 ± 31.8 | (0.115) | |
| COMB | 200.7 ± 22.5 | 213.7 ± 17.9 | 217.1 ± 20.9 | ||
| Total | 188.2 ± 27.8 | 196.9 ± 29.1 | 200.3 ± 29.6 | ||
| FMS total score | M | 14.9 ± 1.4 | 15.9 ± 1.3 | 17.5 ± 1.4 | 0.578 |
| FW | 14.8 ± 3.1 | 15.9 ± 2.3 | 17.5 ± 1.8 | (0.041) | |
| COMB | 14.3 ± 1.1 | 15.7 ± 1.6 | 16.3 ± 2.0 | ||
| Total | 14.6 ± 2.0 | 15.9 ± 1.7 | 17.1 ± 1.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aerenhouts, D.; D’Hondt, E. Using Machines or Free Weights for Resistance Training in Novice Males? A Randomized Parallel Trial. Int. J. Environ. Res. Public Health 2020, 17, 7848. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217848
Aerenhouts D, D’Hondt E. Using Machines or Free Weights for Resistance Training in Novice Males? A Randomized Parallel Trial. International Journal of Environmental Research and Public Health. 2020; 17(21):7848. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217848
Chicago/Turabian StyleAerenhouts, Dirk, and Eva D’Hondt. 2020. "Using Machines or Free Weights for Resistance Training in Novice Males? A Randomized Parallel Trial" International Journal of Environmental Research and Public Health 17, no. 21: 7848. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217848