Profile of Mothers of Children with Fetal Alcohol Spectrum Disorder: A Population-Based Study in Canada

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Maternal Interview
2.2. Prenatal Alcohol Exposure
2.3. Statistical Analysis
2.4. Ethics
3. Results
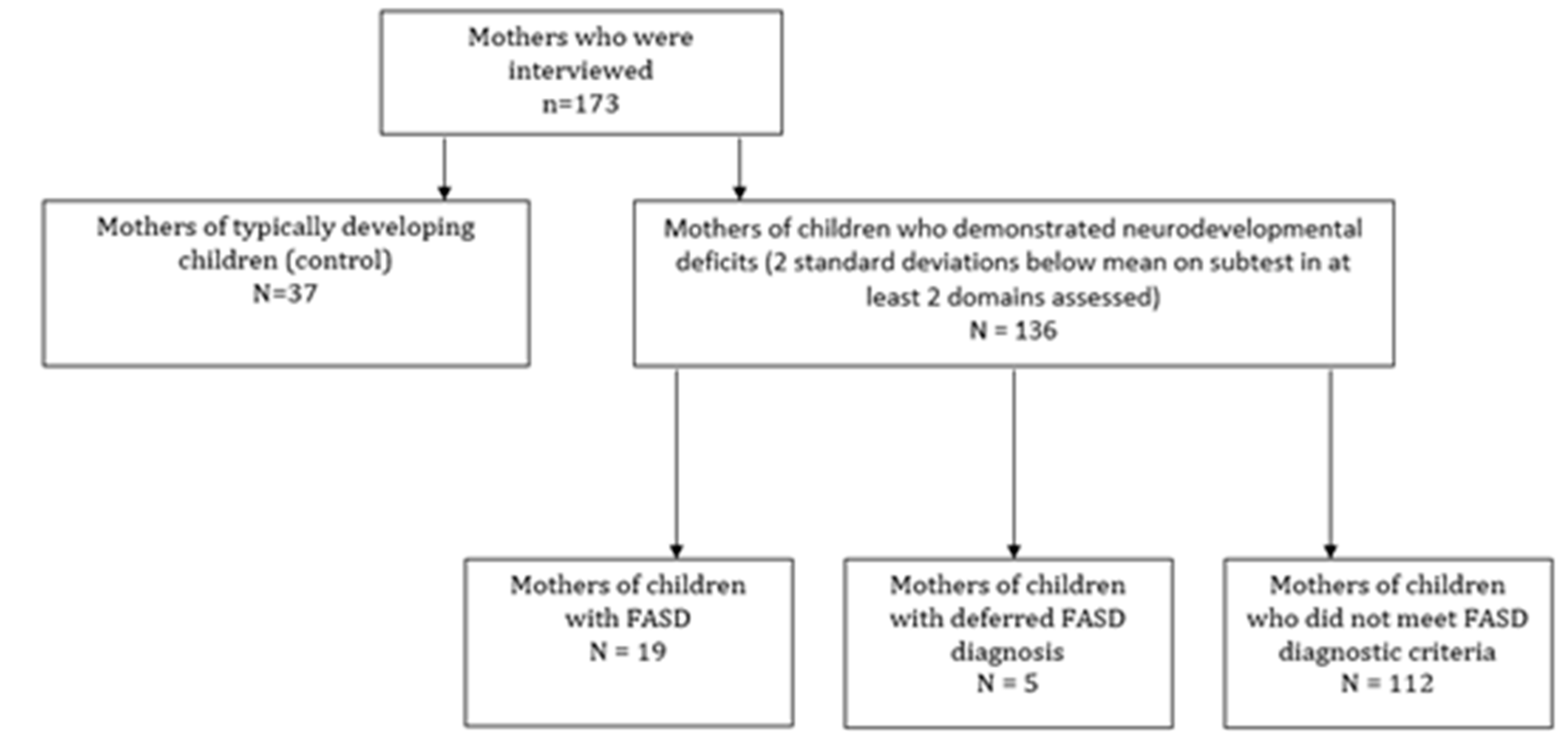
3.1. Total Sample of Interviewed Mothers
3.2. Mothers of Children with FASD Compared with Mothers of Typically Developing Control Children
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Role of the Funders
References
- Burd, L.; Popova, S. Fetal Alcohol Spectrum Disorders: Fixing Our Aim to Aim for the Fix. Int. J. Environ. Res. Public Health 2019, 16, 3978. [Google Scholar] [CrossRef] [Green Version]
- Forray, A. Substance use during pregnancy. F1000Research 2016, 5, 887. [Google Scholar] [CrossRef] [PubMed]
- Popova, S.; Lange, S.; Probst, C.; Gmel, G.; Rehm, J. Estimation of national, regional, and global prevalence of alcohol use during pregnancy and fetal alcohol syndrome: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e290–e299. [Google Scholar] [CrossRef] [Green Version]
- Jones, K.; Smith, D. Recognition of the Fetal Alcohol Syndrome in Early Infancy. Lancet 1973, 302, 999–1001. [Google Scholar] [CrossRef]
- Burd, L. Drinking at the end of pregnancy: Why don’t we see it? Pediatr. Res. 2020, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Chambers, C.D.; Coles, C.D.; Kable, J.; Akshoomoff, N.; Xu, R.; Zellner, J.A.; Honerkamp-Smith, G.; Manning, M.A.; Adam, M.P.; Jones, K.L. Fetal Alcohol Spectrum Disorders in a Pacific Southwest City: Maternal and Child Characteristics. Alcohol. Clin. Exp. Res. 2019, 43, 2578–2590. [Google Scholar] [CrossRef]
- May, P.A.; Hasken, J.; Baete, A.; Russo, J.; Elliott, A.J.; Kalberg, W.O.; Buckley, D.; Brooks, M.; Ortega, M.A.; Hedrick, D.M.; et al. Fetal alcohol spectrum disorders in a midwestern city: Child characteristics, maternal risk traits, and prevalence. Alcohol. Clin. Exp. Res. 2020, 16, 1332–1337. [Google Scholar] [CrossRef]
- May, P.A.; Hasken, J.M.; Bozeman, R.; Jones, J.-V.; Burns, M.K.; Goodover, J.; Kalberg, W.O.; Buckley, D.; Brooks, M.; Ortega, M.A.; et al. Fetal Alcohol Spectrum Disorders in a Rocky Mountain Region City: Child Characteristics, Maternal Risk Traits, and Prevalence. Alcohol. Clin. Exp. Res. 2020, 44, 900–918. [Google Scholar] [CrossRef] [PubMed]
- Bakhireva, L.N.; Sharkis, J.; Shrestha, S.; Miranda-Sohrabji, T.J.; Williams, S.; Miranda, R.C. Prevalence of Prenatal Alcohol Exposure in the State of Texas as Assessed by Phosphatidylethanol in Newborn Dried Blood Spot Specimens. Alcohol. Clin. Exp. Res. 2017, 41, 1004–1011. [Google Scholar] [CrossRef]
- Lange, S.; Probst, C.; Gmel, G.; Rehm, J.; Burd, L.; Popova, S. Global Prevalence of Fetal Alcohol Spectrum Disorder Among Children and Youth: A systematic review and meta-analysis. JAMA Pediatr. 2017, 171, 948–956. [Google Scholar] [CrossRef]
- Popova, S.; Lange, S.; Chudley, A.E.; Reynolds, J.N.; Rehm, J.; May, P.A.; Riley, E.P. World Health Organization International Study on the Prevalence of Fetal Alcohol Spectrum Disorder (FASD): Canadian Component; Centre for Addiction and Mental Health: Toronto, ON, Canada, 2018; Available online: https://www.camh.ca/-/media/files/pdfs%2D%2D-reports-and-books%2D%2D-research/who-fasd-report-english-april2018-pdf.pdf?la=en&hash=347373E4C8C362E1F746C28BB063C7DA9E2987AE (accessed on 15 July 2020).
- National Autism Spectrum Disorder Surveillance (NASS). Autism Spectrum Disorder among Children and Youth in Canada 2018. A Report of the National Autism Spectrum Disorder Surveillance System. Available online: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/autism-spectrum-disorder-children-youth-canada-2018.html (accessed on 8 September 2019).
- Popova, S.; Lange, S.; Shield, K.; Burd, L.; Rehm, J. Prevalence of fetal alcohol spectrum disorder among special subpopulations: A systematic review and meta-analysis. Addiction 2019, 114, 1150–1172. [Google Scholar] [CrossRef]
- Li, Q.; Fisher, W.W.; Peng, C.-Z.; Williams, A.D.; Burd, L. Fetal alcohol spectrum disorders: A population based study of premature mortality rates in the mothers. Matern. Child Health J. 2012, 16, 1332–1337. [Google Scholar] [CrossRef]
- Schwartz, M.; Hart, B.; Weyrauch, D.; Benson, P.; Klug, M.G.; Burd, L. The Hidden Face of Fetal Alcohol Spectrum Disorder. Curr. Womens Health Rev. 2017, 13, 96–102. [Google Scholar] [CrossRef]
- Burd, L.; Klug, M.G.; Bueling, R.; Martsolf, J.; Olson, M.; Kerbeshian, J. Mortality rates in subjects with fetal alcohol spectrum disorders and their siblings. Birth Defects Res. Part A Clin. Mol. Teratol. 2008, 82, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Burd, L. Maternal alcohol use increases risk of infant mortality. Evid. Based Med. 2013, 19, 27. [Google Scholar] [CrossRef]
- Greenmyer, J.R.; Klug, M.G.; Kambeitz, C.; Popova, S.; Burd, L. A Multicountry Updated Assessment of the Economic Impact of Fetal Alcohol Spectrum Disorder: Costs for children and adults. J. Addict. Med. 2018, 12, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Greenmyer, J.R.; Popova, S.; Klug, M.G.; Burd, L. Fetal alcohol spectrum disorder: A systematic review of the cost of and savings from prevention in the United States and Canada. Addiction 2019, 115, 409–417. [Google Scholar] [CrossRef]
- Popova, S.; Dozet, D.; Burd, L. Fetal Alcohol Spectrum Disorder: Can We Change the Future? Alcohol. Clin. Exp. Res. 2020, 44, 815–819. [Google Scholar] [CrossRef]
- Abel, E. An update on the incidence of FAS: FAS is not an equal opportunity birth defect. Neurotoxicol. Teratol. 1995, 17, 437–443. [Google Scholar] [CrossRef]
- Coles, C.D.; Brown, R.T.; Smith, I.E.; Platzman, K.A.; Erickson, S.; Falek, A. Effects of prenatal alcohol exposure at school age: I. Physical and cognitive development. Neurotoxicol. Teratol. 1991, 13, 357–367. [Google Scholar] [CrossRef]
- May, P.A.; Gossage, J.P.; Brooke, L.E.; Snell, C.L.; Marais, A.S.; Hendricks, L.S.; Coxford, J.A.; Viljoen, D.L. Maternal risk factors for FAS in the Western Cape Province of South Africa: A population based study. Am. J. Public Health 2005, 95, 1190–1199. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Population and Dwelling Counts, for Canada, Provinces and Territories, and Census Divisions, 2016 and 2011 Censuses—100% Data; Statistics Canada: Ottawa, ON, Canada, 2017. Available online: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/hlt-fst/pd-pl/Table.cfm?Lang=Eng&T=101&S=50&O=A (accessed on 17 May 2019).
- Chudley, A.E.; Conry, J.; Cook, J.L.; Loock, C.; Rosales, T.; Leblanc, N. Fetal alcohol spectrum disorder: Canadian guidelines for diagnosis. Can. Med Assoc. J. 2005, 172 (Suppl. 5), S1–S21. [Google Scholar] [CrossRef] [Green Version]
- Cook, J.L.; Green, C.R.; Lilley, C.M.; Anderson, S.M.; Baldwin, M.E.; Chudley, A.E.; Conry, J.L.; Leblanc, N.; Loock, C.A.; Lutke, J.; et al. Fetal alcohol spectrum disorder: A guideline for diagnosis across the lifespan. Can. Med Assoc. J. 2016, 188, 191–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stata Corporation. Statistical Software: Release 15; Stata Corporation: College Station, TX, USA, 2017. [Google Scholar]
- Odendaal, H.J.; Steyn, D.W.; Elliott, A.; Burd, L. Combined Effects of Cigarette Smoking and Alcohol Consumption on Perinatal Outcome. Gynecol. Obstet. Investig. 2009, 67, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Popova, S.; Lange, S.; Probst, C.; Parunashvili, N.; Rehm, J. Prevalence of alcohol consumption during pregnancy and Fetal Alcohol Spectrum Disorders among the general and Aboriginal populations in Canada and the United States. Eur. J. Med. Genet. 2017, 60, 32–48. [Google Scholar] [CrossRef] [Green Version]
- Czeizel, A.E. Ten years of experience in periconceptual care. Eur. J. Obstet. Gynecol. Reprod. Biol. 1999, 84, 43–49. [Google Scholar] [CrossRef]
- Russell, M.; Skinner, J.B. Early Measures of Maternal Alcohol Misuse as Predictors of Adverse Pregnancy Outcomes. Alcohol. Clin. Exp. Res. 1988, 12, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Canadian Cannabis Survey 2017—Summary. Ottawa, ON, Canada. Available online: https://www.canada.ca/en/health-canada/services/publications/drugs-health-products/canadian-cannabis-survey-2017-summary.html (accessed on 17 May 2019).
- Schreiber, S.; Pick, C. Cannabis use during pregnancy: Are we at the verge of defining a “fetal cannabis spectrum disorder”? Med. Hypotheses 2019, 124, 53–55. [Google Scholar] [CrossRef]
- Young-Wolff, K.C.; Sarovar, V.; Tucker, L.-Y.; Conway, A.; Alexeeff, S.; Weisner, C.; Armstrong, M.A.; Goler, N. Self-reported Daily, Weekly, and Monthly Cannabis Use Among Women Before and During Pregnancy. JAMA Netw. Open 2019, 2, e196471. [Google Scholar] [CrossRef]
- May, P.A.; Hasken, J.M.; Stegall, J.M.; Mastro, H.A.; Kalberg, W.O.; Buckley, D.; Brooks, M.; Hedrick, D.M.; Ortega, M.A.; Elliott, A.J.; et al. Fetal Alcohol Spectrum Disorders in a Southeastern County of the United States: Child Characteristics and Maternal Risk Traits. Alcohol. Clin. Exp. Res. 2020, 44, 939–959. [Google Scholar] [CrossRef]
- Chang, J.C.; Tarr, J.A.; Holland, C.L.; De Genna, N.M.; Richardson, G.A.; Rodriguez, K.L.; Sheeder, J.; Kraemer, K.L.; Day, N.L.; Rubio, D.; et al. Beliefs and attitudes regarding prenatal marijuana use: Perspectives of pregnant women who report use. Drug Alcohol Depend. 2019, 196, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Jarlenski, M.P.; Tarr, J.A.; Holland, C.L.; Farrell, D.; Chang, J.C. Pregnant Women’s Access to Information About Perinatal Marijuana Use: A Qualitative Study. Women’s Health Issues 2016, 26, 452–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aliyu, M.H.; Wilson, R.E.; Zoorob, R.; Brown, K.; Alio, A.P.; Clayton, H.; Salihu, H.M. Prenatal alcohol consumption and fetal growth restriction: Potentiation effect by concomitant smoking. Nicotine Tob. Res. 2009, 11, 36–43. [Google Scholar] [CrossRef]
- Astley, S.J.; Bailey, D.; Talbot, C.; Clarren, S.K. Fetal Alcohol Syndrome (FAS) Primary Prevention through Fas Diagnosis: II. A comprehensive profile of 80 birth mothers of children with FAS. Alcohol. Alcohol. 2000, 35, 509–519. [Google Scholar] [CrossRef] [Green Version]
- Singal, D.; Brownell, M.D.; Chateau, D.; Hanlon-Dearman, A.; Longstaffe, S.; Roos, L.L. The Psychiatric Morbidity of Women Who Give Birth to Children with Fetal Alcohol Spectrum Disorder (FASD): Results of the Manitoba Mothers and FASD Study. Can. J. Psychiatry 2017, 62, 531–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singal, D.; Brownell, M.; Chateau, D.; Wall-Wieler, E.; Longstaffe, S.; Hanlon-Dearman, A.; Roos, L.L. Suicide and suicide attempts among women in the Manitoba Mothers and Fetal Alcohol Spectrum Disorder cohort: A retrospective matched analysis using linked administrative data. CMAJ Open 2017, 5, E646–E652. [Google Scholar] [CrossRef] [PubMed]
- Lange, S.; Shield, K.; Koren, G.; Rehm, J.; Popova, S. A comparison of the prevalence of prenatal alcohol exposure obtained via maternal self-reports versus meconium testing: A systematic literature review and meta-analysis. BMC Pregnancy Childbirth 2014, 14, 127. [Google Scholar] [CrossRef] [Green Version]
- May, P.A.; Baete, A.; Russo, J.; Elliott, A.J.; Blankenship, J.; Kalberg, W.O.; Buckley, D.; Brooks, M.; Hasken, J.; Abdul-Rahman, O.; et al. Prevalence and Characteristics of Fetal Alcohol Spectrum Disorders. Pediatrics 2014, 134, 855–866. [Google Scholar] [CrossRef] [Green Version]
- Ortega-García, J.A.; Gutierrez-Churango, J.E.; Sánchez-Sauco, M.F.; Martínez-Aroca, M.; Delgado-Marín, J.L.; Sánchez-Solis, M.; Parrilla-Paricio, J.J.; Claudio, L.; Martínez-Lage, J.F. Head circumference at birth and exposure to tobacco, alcohol and illegal drugs during early pregnancy. Childs Nerv Syst. 2012, 28, 433–439. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Demographics | All Interviewed Mothers (n = 173) | Mothers of Children with FASD (n = 19) | Mothers of Children Considered Deferred Cases (n = 5) | Mothers of Control Children (n = 37) | Statistical Test a | p Value |
|---|---|---|---|---|---|---|
| Current age (years)—mean (SD) | 40.9 (5.0) | 41.7 (6.0) | 42.6 (5.0) | 41.4 (4.9) | t = 0.188 | 0.851 |
| Range | 26–56 | 32–49 | 38–51 | 30–56 | ||
| Ethnicity—n (%) | X = 7.933 | 0.160 | ||||
| Caucasian | 85 (49.1) | 14 (73.7) | 2 (40.0) | 29 (78.4) | ||
| Aboriginal | 1 (0.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| African Canadian/Caribbean | 11 (6.4) | 1 (5.3) | 0 (0.0) | 0 (0.0) | ||
| Eastern European | 12 (6.9) | 0 (0.0) | 1 (20.0) | 3 (8.1) | ||
| Western European | 23 (13.3) | 4 (21.1) | 1 (20.0) | 2 (5.4) | ||
| Chinese/Southeast Asian | 16 (9.3) | 0 (0.0) | 1 (20.0) | 2 (5.4) | ||
| South Asian | 8 (4.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Other | 16 (9.3) | 0 (0.0) | 0 (0.0) | 1 (2.7) | ||
| Marital status when pregnant—n (%) | X = 0.482 | 0.786 | ||||
| Single | 6 (4.5) | 1 (5.3) | 0 (0.0) | 1 (2.7) | ||
| Married, living with husband | 137 (79.2) | 14 (73.7) | 4 (80.0) | 30 (81.1) | ||
| Not married, but living with partner | 29 (16.8) | 4 (21.1) | 1 (20.0) | 6 (16.2) | ||
| Separated from spouse | 1 (0.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Employment status 12 months before pregnancy—n (%) | X = 0.090 | 0.764 | ||||
| Employed | 141 (81.5) | 17 (89.5) | 5 (100.0) | 34 (91.9) | ||
| Unemployed | 32 (18.5) | 2 (10.5) | 0 (0.0) | 3 (8.1) | ||
| Highest level of education completed by pregnancy—n (%) | X = 15.220 | 0.004 | ||||
| Less than 9 years | 3 (1.7) | 1 (5.3) | 0 (0.0) | 0 (0.0) | ||
| Uncompleted high school diploma | 3 (1.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| High school diploma | 22 (12.7) | 5 (26.3) | 0 (0.0) | 0 (0.0) | ||
| College diploma | 56 (32.4) | 6 (31.6) | 1 (20.0) | 9 (24.3) | ||
| University degree | 77 (44.5) | 6 (31.6) | 4 (80.0) | 21 (56.8) | ||
| Graduate degree | 11 (6.4) | 1 (5.3) | 0 (0.0) | 7 (18.9) |
| Paternal Characteristics | Based on All Maternal Interviews (n =173) | Children with FASD (n =19) | Children Considered Deferred Cases (n =5) | Control Children (n = 37) | Statistical Test a | p Value |
|---|---|---|---|---|---|---|
| Employment status 12 months before partner’s pregnancy—n (%) | X = 0.496 | 0.780 | ||||
| Employed | 162 (93.6) | 17 (89.5) | 5 (100.0) | 35 (94.6) | ||
| Unemployed | 5 (2.9) | 1 (5.3) | 0 (0.0) | 1 (2.7) | ||
| Highest level of education completed at time of partner’s pregnancy—n (%) | ||||||
| Less than 9 years | 1 (1.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | X = 9.043 | 0.107 |
| Uncompleted high school diploma | 10 (5.8) | 3 (15.8) | 0 (0.0) | 2 (5.4) | ||
| High school diploma | 40 (23.1) | 4 (21.1) | 2 (40.0) | 2 (5.4) | ||
| College diploma | 46 (26.6) | 6 (31.6) | 2 (40.0) | 12 (32.4) | ||
| University degree | 58 (33.5) | 3 (15.8) | 0 (0.0) | 16 (43.2) | ||
| Graduate degree | 9 (5.2) | 1 (5.3) | 1 (20.0) | 4 (10.8) |
| Pregnancy-Related Characteristics | All Interviewed Mothers (n = 173) | Mothers of Children with FASD (n = 19) | Mothers of Children Considered Deferred cases (n = 5) | Mothers of Control Children (n = 37) | Statistical Test a | p Value |
|---|---|---|---|---|---|---|
| Received financial support during pregnancy from relative and/or non-relative | 21 (12.1) | 3 (15.8) | 2 (40.0) | 2 (5.4) | X = 3.801 | 0.149 |
| Received financial support was at least half of respondent’s income | 14 (8.1) | 3 (15.8) | 2 (40.0) | 0 (0.0) | X = 6.187 | 0.045 |
| Financial supported provided by: | ||||||
| Child’s grandmother or grandfather | 7 (4.1) | 2 (10.5) | 0 (0.0) | 0 (0.0) | X = 6.587 | 0.086 |
| Child’s father | 6 (3.5) | 1 (5.3) | 2 (40.0) | 0 (0.0) | ||
| Other relative | 3 (1.7) | 0 (0.0) | 0 (0.0) | 1 (2.7) | ||
| Other non-relative | 1 (0.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Planned pregnancy—n (%) | 126 (72.8) | 12 (63.2) | 5 (100.0) | 31 (83.8) | X = 5.242 | 0.155 |
| Number of pregnancies—mean (SD) | 2.8 (1.3) | 3.5 (2.3) | 2.8 (1.3) | 2.7 (1.2) | t = 1.809 | 0.076 |
| Range | 1–11 | 1–11 | 1–4 | 1–7 | ||
| Number of live births—mean (SD) | 2.3 (0.9) | 2.5 (1.6) | 2.0 (0.7) | 2.2 (0.6) | t = 0.873 | 0.387 |
| Range | 1–8 | 1–8 | 1–3 | 1–4 | ||
| Any children born prematurely (yes)—n (%) | 28 (16.2) | 3 (15.8) | 0 (0.0) | 4 (10.8) | X = 0.285 | 0.594 |
| Any children with a birth defect (yes)—n (%) | 20 (11.6) | 4 (21.1) | 0 (0.0) | 2 (5.4) | X = 3.213 | 0.073 |
| Point of pregnancy recognition (weeks)—Mean (SD) | 4.6 (2.3) | 4.1 (1.2) | 4.4 (2.6) | 4.9 (1.8) | t = 1.717 | 0.092 |
| Range | 1–20 | 1–6 | 1–8 | 2–9 |
| Alcohol Use | All Interviewed Mothers (n = 173) | Mothers of Children with FASD (n = 19) | Mothers of Children Considered Deferred Cases (n = 5) | Mothers of Control Children (n = 37) | Statistical Test a | p Value |
|---|---|---|---|---|---|---|
| Lifetime abstainer—n (%) | 17 (9.8) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Age of first drink (years)—mean (SD) | 17.7 (3.0) | 16.6 (2.0) | 18 (1.4) | 17.0 (2.0) | t = 0.692 | 0.492 |
| Age when began to drink regularly (years)—mean (SD) | 20.7 (5.3) | 18.2 (1.7) | 20.3 (2.5) | 19.4 (3.3) | t = 1.381 | 0.174 |
| Current drinking problem—n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Ever sought help for a drinking problem—n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Ever felt they should cut down their drinking—n (%) | 4 (2.3) | 0 (0.0) | 0 (0.0) | 1 (2.7) | X = 1.065 | 0.587 |
| Alcohol use prior to pregnancy recognition—n (%) | X = 31.605 | < 0.001 | ||||
| High risk | 19 (11.0) | 12 (63.2) | 4 (80.0) | 0 (0.0) | ||
| Some risk | 110 (63.6) | 7 (36.8) | 1 (20.0) | 25 (67.6) | ||
| No risk (no use) | 44 (25.4) | 0 (0.0) | 0 (0.0) | 12 (32.4) | ||
| Beverage preference of mothers who used alcohol prior to pregnancy recognition—n (%) | X = 8.509 | 0.075 | ||||
| Beer | 28 (16.2) | 5 (26.3) | 1 (20.0) | 5 (13.5) | ||
| Wine | 76 (43.9) | 11 (57.9) | 4 (80.0) | 15 (40.5) | ||
| Wine coolers or champagne | 13 (7.5) | 2 (10.5) | 0 (0.0) | 2 (5.4) | ||
| Liquor/cocktails | 13 (7.5) | 1 (5.3) | 0 (0.0) | 4 (10.8) | ||
| Alcohol use following pregnancy recognition—n (%) | X = 0.496 | 0.481 | ||||
| High risk | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Some risk | 11 (6.4) | 2 (10.5) | 1 (20.0) | 2 (5.4) | ||
| No risk (no use) | 162 (93.6) | 17 (89.5) | 4 (80.0) | 35 (94.6) | ||
| Beverage preference of mothers who used alcohol following pregnancy recognition—n (%) | X = 2.469 | 0.291 | ||||
| Beer | 3 (1.7) | 0 (0.0) | 0 (0.0) | 2 (5.4) | ||
| Wine | 8 (4.6) | 2 (10.5) | 1 (20.0) | 0 (0.0) | ||
| Wine coolers or champagne | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Liquor/cocktails | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Tobacco/Drug Use | All Interviewed Mothers (n = 173) | Mothers of Children with FASD (n = 19) | Mothers of Children Considered Deferred Cases (n = 5) | Mothers of Control Children (n = 37) | Statistical Test a | p Value |
|---|---|---|---|---|---|---|
| Ever smoked in their lifetime—n (%) | 81 (47.1) | 14 (73.7) | 3 (60.0) | 17 (46.0) | X = 6.525 | 0.038 |
| Current smoker—n (%) | ||||||
| Daily | 21 (12.1) | 4 (21.1) | 0 (0.0) | 2 (5.4) | X = 0.278 | 0.598 |
| Occasionally | 6 (3.5) | 2 (10.5) | 1 (20.0) | 2 (5.4) | ||
| Does not smoke | 146 (84.4) | 13 (68.4) | 4 (80.0) | 33 (89.2) | ||
| Tobacco use prior to pregnancy recognition—n (%) | X = 17.233 | < 0.001 | ||||
| Daily | 42 (24.3) | 11 (57.9) | 2 (40.0) | 3 (8.1) | ||
| Occasionally | 17 (9.8) | 2 (10.5) | 1 (20.0) | 4 (10.8) | ||
| Did not smoke | 114 (65.9) | 6 (31.6) | 2 (40.0) | 30 (81.1) | ||
| Number of cigarettes smoked per day prior to pregnancy recognition (daily smokers)—mean (SD) | 6.9 (4.5) | 8.1 (6.4) | 4.5 (0.7) | 4.4 (3.2) | t = 1.207 | 0.248 |
| Range | 1–25 | 1–25 | 4–5 | 1–8 | ||
| Tobacco use following pregnancy recognition—n (%) | X = 0.496 | 0.481 | ||||
| Daily | 8 (4.6) | 2 (10.5) | 0 (0.0) | 2 (5.4) | ||
| Occasionally | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Did not smoke | 165 (95.4) | 17 (89.5) | 5 (100.0) | 35 (94.6) | ||
| Number of cigarettes smoked per day following pregnancy recognition (daily smokers)—mean (SD) | 4.5 (3.6) | 2.5 (0.7) | 0 (0.0) | 3.0 (1.4) | t = 0.447 | 0.699 |
| Range | 1–12 | 2–3 | 2–4 | |||
| Drug Use | ||||||
| Drug use during pregnancy (prior to pregnancy recognition)—n (%) | ||||||
| Anabolic steroids | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Club drugs (ecstasy, GHB, rohypnol) | 7 (4.1) | 1 (5.3) | 0 (0.0) | 2 (5.4) | X = 0.001 | 0.982 |
| Crack/cocaine | 1 (0.6) | 1 (5.3) | 0 (0.0) | 0 (0.0) | X = 1.983 | 0.159 |
| Dissociative drugs (PCP, ketamine, salvia, DXM) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Hallucinogens (LSD, mushrooms, peyote) | 11 (6.4) | 3 (15.8) | 0 (0.0) | 3 (8.1) | X = 0.774 | 0.379 |
| Heroin or opium | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Marijuana or hashish | 48 (28.6) | 13 (68.4) | 2 (40.0) | 10 (27.0) | X = 8.887 | 0.003 |
| Methamphetamines/amphetamines | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popova, S.; Lange, S.; Temple, V.; Poznyak, V.; Chudley, A.E.; Burd, L.; Murray, M.; Rehm, J. Profile of Mothers of Children with Fetal Alcohol Spectrum Disorder: A Population-Based Study in Canada. Int. J. Environ. Res. Public Health 2020, 17, 7986. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217986
Popova S, Lange S, Temple V, Poznyak V, Chudley AE, Burd L, Murray M, Rehm J. Profile of Mothers of Children with Fetal Alcohol Spectrum Disorder: A Population-Based Study in Canada. International Journal of Environmental Research and Public Health. 2020; 17(21):7986. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217986
Chicago/Turabian StylePopova, Svetlana, Shannon Lange, Valerie Temple, Vladimir Poznyak, Albert E. Chudley, Larry Burd, Margaret Murray, and Jürgen Rehm. 2020. "Profile of Mothers of Children with Fetal Alcohol Spectrum Disorder: A Population-Based Study in Canada" International Journal of Environmental Research and Public Health 17, no. 21: 7986. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217986