Acute Effects of High-Intensity Interval Training on Brain-Derived Neurotrophic Factor, Cortisol and Working Memory in Physical Education College Students


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Approach
2.3. Exercise-Related Measurements
2.3.1. VO2 Peak
2.3.2. HIIT HR and RPE Assessment
2.4. Neurophysiological Assessment
2.4.1. BDNF
2.4.2. CORT
2.5. WM Task
2.6. Statistical Analysis
3. Results
3.1. Graded Exercise Test: refErence Data
3.2. Cardiovascular and RPE Responses to HIIT
3.3. BDNF and CORT Assessment
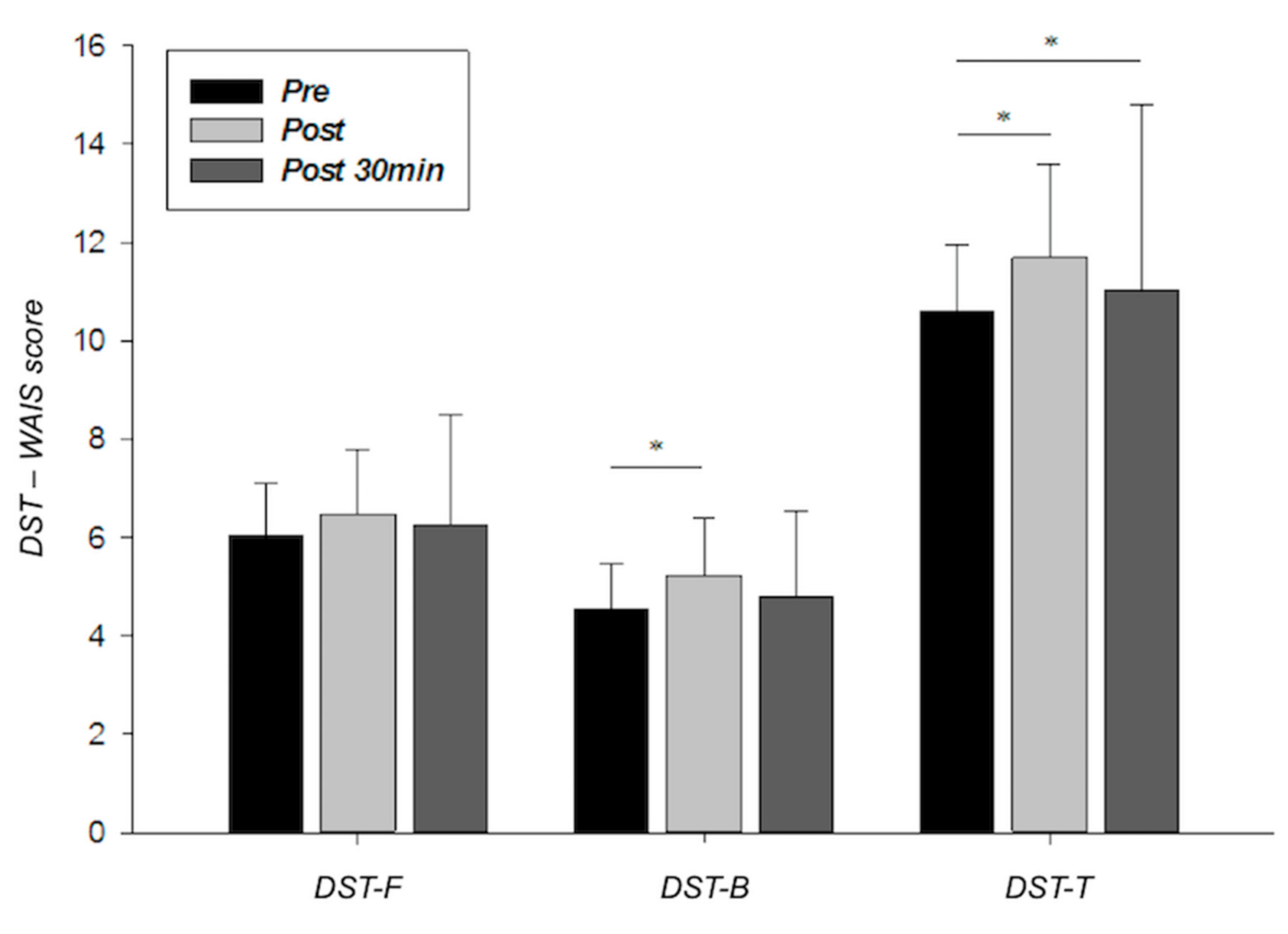
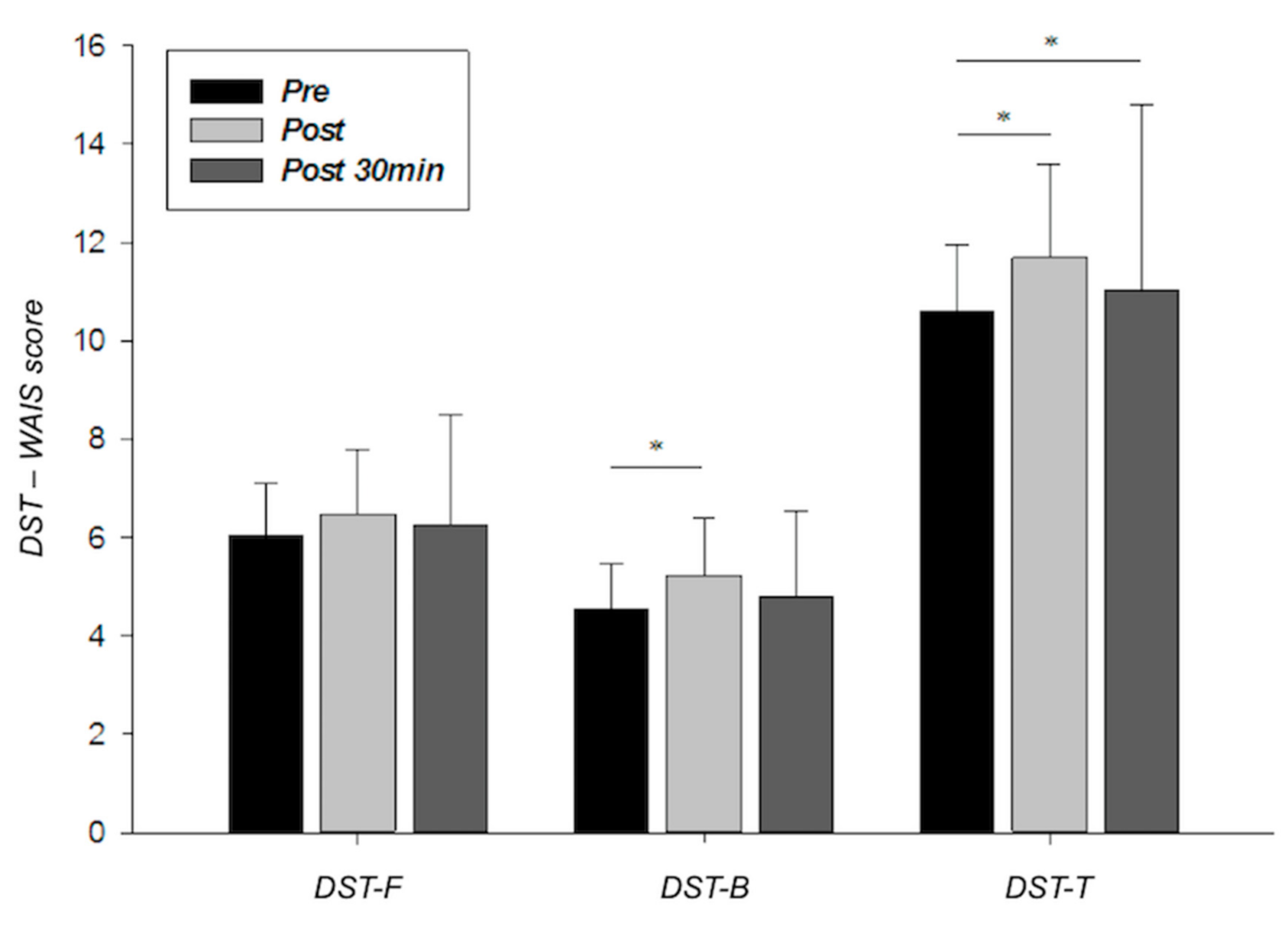
3.4. WM Evaluation
3.5. Relationship Between Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gibala, M.J.; Little, J.P.; MacDonald, M.J.; Hawley, J.A. Physiological adaptations to low volume, high intensity interval training in health and disease. J. Physiol. 2012, 590, 1077–1084. [Google Scholar] [CrossRef]
- Helgerud, J.; Høydal, K.; Wang, E.; Karlsen, T.; Berg, P.; Bjeerkaas, M.; Simonsen, T.; Helsegen, T.; Hjorth, N.; Bach, R.; et al. Aerobic high-intensity intervals improve VO2max more than moderate training. Med. Sci. Sports Exerc. 2007, 39, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Buchheit, M.; Laursen, P. High-intensity interval training, solutions to the programming puzzle. Sports Med. 2013, 43, 313–338. [Google Scholar] [CrossRef] [PubMed]
- Kessler, H.S.; Sisson, S.B.; Short, K.R. The potential for high-intensity interval training to reduce cardiometabolic disease risk. Sports Med. 2012, 42, 489–509. [Google Scholar] [CrossRef] [PubMed]
- Weston, M.; Taylor, K.L.; Batterham, A.M.; Hopkins, W.G. Effects of low-volume highintensity interval training (HIT) on fitness in adults: A meta-analysis of controlled and non-controlled trials. Sports Med. 2014, 44, 1005–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerber, M.; Firth, J.; Hallgren, M.; Firth, J.; Veronese, N.; Solmi, M.; Kahl, K.G. EPA guidance on physical activity as a treatment for severe mentalillness: A meta-review of the evidence and Position Statement from theEuropean Psychiatric Association (EPA), supported by the InternationalOrganization of Physical Therapists in Mental. Eur. Psychiatry 2018, 54, 124–144. [Google Scholar] [CrossRef] [Green Version]
- Martland, R.; Morelli, V.; Gaughran, F.; Stubbs, B. Can high-intensity interval training improve physical and mental health outcomes? A metareview of 33 systematic reviews across the lifespan. J. Sports Sci. 2020, 38, 430–469. [Google Scholar] [CrossRef] [PubMed]
- Coetsee, C.; Terblanche, E. Cerebral oxygenation during cortical activation: The differential influence of three exercise training modalities. A randomized controlled trial. Eur. J. Appl. Physiol. 2017, 117, 1617–1627. [Google Scholar] [CrossRef]
- Santos-Concejero, J.; Billaut, F.; Grobler, L.; Olivan, J.; Noakes, T.D.; Tucker, R. Brain oxygenation declines in elite Kenyan runners during a maximal interval training session. Eur. J. Appl. Physiol. 2017, 117, 1017–1024. [Google Scholar] [CrossRef]
- So, J.H.; Huang, C.; Ge, M.; Cai, G.; Zhang, L.; Lu, Y.; Mu, Y. Intense exercise promotes adult hippocampal neurogenesis but not spatial discrimination. Front. Cell. Neurosci. 2017, 11, 13. [Google Scholar] [CrossRef] [Green Version]
- Freitas, D.A.; Rocha-Vieira, E.; Soares, B.A.; Nonato, L.F.; Fonseca, S.R.; Martins, J.B.; Mendonça, V.A.; Lacerda, A.C.; Massensini, A.R.; Poortamns, J.R.; et al. High intensity interval training modulates hippocampal oxidative stress, BDNF and inflammatory mediators in rats. Physiol. Behav. 2018, 184, 6–11. [Google Scholar] [CrossRef]
- Robinson, M.M.; Lowe, V.J.; Nair, K.S. Increased brain glucose uptake after 12 weeks of aerobic high-intensity interval training in young and older adults. J. Clin. Endocrinol. Metab. 2018, 103, 221–227. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Maldonado, A.; Rentería, I.; García-Suárez, P.; Moncada-Jiménez, J.; Freire-Royes, L.F. The impact of high-intensity interval training on brain dervied neurotrophic factor in brain: A mini-review. Front. Neurosci. 2018, 12, 839. [Google Scholar] [CrossRef]
- Fernandes, J.; Arida, R.M.; Gomez-Pinilla, F. Physical exercise as an epigenetic modulator of brain plasticity and cognition. Neurosci. Biobehav. Rev. 2017, 80, 443–456. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, G.; Lira, C.M.; Johansson, J.; Wisén, A.; Wohlfart, B.; Ekman, R.; Westrin, A. The acute response of plasma brain-derived neurotrophic factor as a result of exercise in major depression. Psychiatry Res. 2009, 94, 1159–1160. [Google Scholar] [CrossRef]
- Rasmussen, P.; Brassard, P.; Adser, H. Evidence for a release of brain-derived neurotrophic factor from the brain during exercise. Exp. Physiol. 2009, 94, 1062–1069. [Google Scholar] [CrossRef]
- Schmolesky, M.T.; Webb, D.L.; Hansen, R.A. The effects of aerobic exercise intensity and duration on levels of brain-derived neurotrophic factor in healthy men. J. Sports Sci. Med. 2013, 12, 502–511. [Google Scholar]
- Winter, B.; Breitenstein, C.; Mooren, F.C.; Voelker, K.; Fobker, M.; Lechtermann, A.; Krueger, K.; Fromme, A.; Korsukewitz, C.; Floel, A.; et al. High impact running improves learning. Neurobiol. Learn. Mem. 2007, 87, 597–609. [Google Scholar] [CrossRef]
- Laske, C.; Banschcach, S.; Stransky, E.; Bosch, S.; Straten, G.; Machann, J.; Fritsche, A.; Hipp, A.; Niess, A.; Eschweiler, G.W. Exercise-induced normalization of decreased BDNF serum concentration in elderly women with remitted major depression. Int. J. Neuropsychopharmacol. 2010, 13, 595–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rentería, I.; García-Suárez, P.C.; Martínez-Corona, D.O.; Moncada-Jiménez, J.; Plaisance, E.P.; Jiménez-Maldonado, A. Short-term high-Intensity interval training increases systemic brain-derived neurotrophic factor (BDNF) in healthy women. Eur. J. Sport Sci. 2020, 20, 516–524. [Google Scholar] [CrossRef]
- Rojas-Vega, S.; Struder, H.K.; Wahrmann, B.V.; Schmidt, A.; Bloch, W.; Hollmann, W. Acute BDNF and cortisol response to low intensity exercise and following ramp incremental exercise to exhaustion in humans. Brain Res. 2006, 1121, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Lu, B.; Gottschalk, W. Modulation of hippocampal synaptic transmission and plasticity by neurotrophins. Prog Brain Res. 2000, 128, 231–241. [Google Scholar] [CrossRef]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Men, W.W.; Chang, Y.K.; Fan, M.X.; Ji, L.; Wei, G.X. Acute aerobic exercise increases cortical activity during working memory: A functional RMI study in female college students. PLoS ONE 2014, 9, e99222. [Google Scholar] [CrossRef]
- Smith, P.J.; Blumenthal, J.A.; Hoffman, B.M.; Cooper, H.; Strauman, T.A.; Welsh-Bohmer, K.; Browndyke, J.; Sherwood, A. Aerobic exercise and neurocognitive performance: A meta-analytic review of randomized controlled trials. Psychosom. Med. 2010, 72, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, H.; Suga, T.; Takenaka, S.; Tanaka, D.; Takeuchi, T.; Hamaoka, T.; Isaka, T.; Hashimoto, T. Greater impact of acute high-intensity interval exercise on post-exercise executive function compared to moderate-intensity continuous exercise. Physiol. Behav. 2016, 155, 224–230. [Google Scholar] [CrossRef]
- Verbickas, V.; Baranauskiene, N.; Eimantas, N.; Kamandulis, S.; Rutkauskas, S.; Satkunskiene, D.; Sadauskas, S.; Brazaitis, M.; Skurvydas, A. Effects of sprint cycling and stretch-shortening cycle exercises on the neuromuscular, immune and stress indicators in young men. J. Physiol. Pharmacol. 2017, 68, 125–132. [Google Scholar] [CrossRef] [Green Version]
- Ferris, L.T.; Williams, J.S.; Shen, C.L. The effect of acute exercise on serum brain-derived neurotrophic factor levels and cognitive function. Med. Sci. Sports Exerc. 2007, 39, 728–734. [Google Scholar] [CrossRef]
- Chang, Y.K.; Alderman, B.L.; Chu, C.H.; Wang, C.C.; Song, T.F.; Chen, F.T. Acute exercise has a general facilitative effect on cognitive function: A combined ERP temporal dynamics and BDNF study. Psychophysiology 2017, 54, 289–300. [Google Scholar] [CrossRef]
- Henckens, M.J.; Wingen, G.A.; Joels, M.; Fernandez, G. Time-dependent effects of cortisol on selective attention and emotional interference: A functional MRI study. Front. Integr. Neurosci. 2012, 6, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fragala, M.S.; Kraemer, W.J.; Denegar, C.R.; Maresh, C.M.; Mastro, A.M.; Volek, J.S. Neuroendocrine-immune interactions and responses to exercise. Sports Med. 2011, 41, 621–639. [Google Scholar] [CrossRef]
- Lupien, S.J.; McEwen, B.S. The acute effects of corticosteroids on cognition: Integration of animal and human model studies. Brain Res. Rev. 1997, 24, 1–27. [Google Scholar] [CrossRef]
- Blair, C.; Granger, D.; Razza, R.P. Cortisol reactivity is positively related to executive function in preschool children attending head start. Child Dev. 2005, 76, 554–567. [Google Scholar] [CrossRef]
- Heaney, J.L.J.; Carroll, D.; Phillips, A.C. DHEA, DHEA-S and cortisol responses to acute exercise in older adults in relation to exercise training status and sex. Age 2013, 35, 395–405. [Google Scholar] [CrossRef] [Green Version]
- Ludyga, S.; Gerberg, M.; Brand, S.; Holsboer-Traschsler, E.; Püshe, U. Acute effects of moderate aerobic exercise on specific aspects of executive function in different age and fitness groups: A meta-analyis. Psychophysiology 2016, 53, 1611–1626. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Vega, S.; Hollmann, W.; Vera-Wahrmann, B.; Struder, H.K. pH buffering does not influence BDNF responses to exercise. Int. J. Sports Med. 2012, 33, 8–12. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki ethical principles for medical research involving human subjects. JAMA J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- American College of Sport Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 7th ed.; Lippincott, Williams, and Wilkins: Baltimore, MD, USA, 2005. [Google Scholar]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Wechler, D. Escala de Inteligencia de Wechsler Para Adultos-III. Manual Técnico; TEA Ediciones: Madrid, Spain, 1999. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Earlbaum Associates: Hillsdale, MI, USA, 1988. [Google Scholar]
- Rozenek, R.; Salassi, J.W., III; Mier, N.M.; Fleming, J. Acute cadiopulmonary and metabolic responses to high-intensity interval training (HIIT) protocols using 60 s of work and 60 s recovery. J. Strength Cond. Res. 2016, 30, 3014–3023. [Google Scholar] [CrossRef] [PubMed]
- Nofuji, Y.; Suwa, M.; Moriyama, Y.; Nakano, H.; Ichimiya, A.; Nishichi, R.; Sasaki, H.; Radak, Z.; Kumagai, S. Decreased serum brain-derived neurotrophic factor in trained men. Neurosci. Lett. 2008, 437, 29–32. [Google Scholar] [CrossRef]
- Tang, S.W.; Chu, E.; Hui, T.; Helmeste, D.; Law, C. Influence of exercise on serum brain-derived neurotrophic factor concentrations in healthy human subjects. Neurosci. Lett. 2008, 431, 62–65. [Google Scholar] [CrossRef]
- Knaepen, K.; Goekint, M.; Heymann, E.M.; Meeusen, R. Neuroplasticity: Exercise-induced response of peripheral brain-derivied neurotrophic factor. Sports Med. 2010, 40, 765–801. [Google Scholar] [CrossRef]
- Tamayo, F.; Casals-Coll, M.; Sánchez-Benavides, G.; Quintana, M.; Manero, R.M.; Rognoni, T.; Calvo, L.; Palomo, R.; Aranciba, F.; Peña-Casanova, J. Estudios normativos españoles en población adulta joven (Proyecto NEURONORMA jóvenes): Normas para las pruebas span verbal, span visuoespacial, Letter-Number Sequencing, Trail Making Test y Symbol Digit Modalities Test. Neurología 2012, 27, 319–329. [Google Scholar] [CrossRef]
- Kashihara, K.; Maruyama, T.; Murota, M.; Nakahara, Y. Positive effects of acute and moderate physical exercise on cognitive function. J. Physiol. Anthropol. 2009, 28, 155–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oweis, P.; Spinks, W. Biopsychological, affective and cognitive responses to acute physical activity. J. Sports Med. Phys. Fit. 2001, 41, 528–538. [Google Scholar]
- Quesada, A.A.; Wiemers, U.S.; Schoofs, D.; Wolf, O.T. Psychosocial stress exposure impairs memory retrieval in children. Psychoneuroendocrinology 2012, 37, 125–136. [Google Scholar] [CrossRef]
- Northey, J.M.; Pumpa, K.L.; Quinlan, C.; Ikin, A.; Tookey, K.; Smee, D.J.; Rattray, B. Cognition in breast cancer survivors: A pilot study of interval and continuous exercise. J. Sci. Med. Sport 2019, 22, 580–585. [Google Scholar] [CrossRef]
- Hough, J.P.; Papacosta, E.; Wraith, E.; Gleeson, M. Plasma and salivary steroid hormone response of men to high-intensity cycling and resistance exercise. J. Strength Cond. Res. 2011, 25, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Vuorimaa, T.; Ahotupa, M.; Hakkinen, K.; Vasankari, T. Different hormonal response to continuous and intermittent exercise in middle-distance and maratón runners. Scand. J. Med. Sci. Sports 2008, 18, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Tanner, A.V.; Nielsen, B.V.; Allgrove, J. Salivary and plasma cortisol and testosterone responses to interval and tempo runs and a bodyweight-only circuit sesión in endurance-trained men. J. Sports Sci. 2014, 32, 680–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraemer, W.J.; Ratamess, N.A. Hormonal responses and adaptations to resistance exercise and training. Sports Med. 2005, 35, 339–361. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, L.; Kindermann, W. Beta-endorphin, adrenocorticotropic hormone, cortisol and catecholamines during aerobic and anaerobic exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 61, 165–171. [Google Scholar] [CrossRef]
- Ratamess, N.A.; Kraemer, W.J.; Volek, J.S.; Maresh, C.M.; VanHeest, J.L.; Sharman, M.J.; Rubin, M.R.; French, D.N.; Vescovi, J.D.; Silvestre, R.; et al. Androgen receptor content following heavy resistance exercise in men. J. Steroid Biochem. Mol. Biol. 2005, 93, 35–42. [Google Scholar] [CrossRef]
- Jeon, Y.K.; Ha, C.H. Expression of brain-derived neurothropic factor, IGF-1, and cortisol elicited by a regular aerobic exercise in adolescents. J. Phys. Ther. Sci. 2015, 27, 737–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, K.; Shea, P.Y.; Le, L.; Xiao-Xiang, Z.; Kai-Yu, T. The effects of voluntary, involuntary, and forced exercise on Brain-Derived Neurotrophic Factor and Motor function recovery: A rat brain ischemia model. PLoS ONE 2010, 6, e16643. [Google Scholar] [CrossRef] [Green Version]
- Tsai, C.L.; Wang, C.H.; Pan, C.Y.; Chen, F.C.; Huang, T.H.; Chou, F. Executive function and endocrinological responses to acute resistance exercise. Front. Behav. Neurosci. 2014, 8, 1–12. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Variable | Mean ± SD |
|---|---|
| Age (years) | 21.7 ± 2.1 |
| Height (m) | 1.77 ± 0.06 |
| BMI (Kg/m2) | 23.1 ± 1.4 |
| Time to exhaustion (min) | 13.6 ± 1.8 |
| VO2max (mL/kg/min) | 47.1 ± 10.1 |
| VT2 (mL/kg/min) | 30.3 ± 9.9 |
| VT2 (% VO2max) | 64.6 ± 14.6 |
| HRmax (bpm) | 181.5 ± 8.4 |
| VO2 peak (mL/kg/min) | 45.3 ± 9.3 |
| pVO2 peak (W) | 275.0 ± 48.9 |
| Effect Size (r) | |||||||
|---|---|---|---|---|---|---|---|
| Pre Mean (SD) | Post Mean (SD) | Post 30 min Mean (SD) | Friedman Test (p) | Pre vs. Post | Post vs. Post 30 min | Pre vs. Post 30 min | |
| BDNF (pg/mL) | 424.66 (91.05) | 1271.07 * (342.93) | 437.04 (101.32) | <0.001 | 0.775 | 0.714 | 0.006 |
| CORT (ng/mL) | 132.33 (35.88) | 181.41 ‡ (107.26) | 234.45 † (109.63) | <0.001 | 0.716 | 0.425 | 0.828 |
| Pre—Post | Post—Post 30 min | Pre—Post 30 min | |
|---|---|---|---|
| BDNF | 0.768 *** | 0.567 ** | 0.652 *** |
| CORT | 0.645 *** | 0.737 *** | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Díaz, I.C.; Escobar-Muñoz, M.C.; Carrasco, L. Acute Effects of High-Intensity Interval Training on Brain-Derived Neurotrophic Factor, Cortisol and Working Memory in Physical Education College Students. Int. J. Environ. Res. Public Health 2020, 17, 8216. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218216
Martínez-Díaz IC, Escobar-Muñoz MC, Carrasco L. Acute Effects of High-Intensity Interval Training on Brain-Derived Neurotrophic Factor, Cortisol and Working Memory in Physical Education College Students. International Journal of Environmental Research and Public Health. 2020; 17(21):8216. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218216
Chicago/Turabian StyleMartínez-Díaz, Inmaculada C., María C. Escobar-Muñoz, and Luis Carrasco. 2020. "Acute Effects of High-Intensity Interval Training on Brain-Derived Neurotrophic Factor, Cortisol and Working Memory in Physical Education College Students" International Journal of Environmental Research and Public Health 17, no. 21: 8216. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218216