“There Is No Link Between Resource Allocation and Use of Local Data”: A Qualitative Study of District-Based Health Decision-Making in West Bengal, India

 , and
, and
Abstract
:1. Introduction
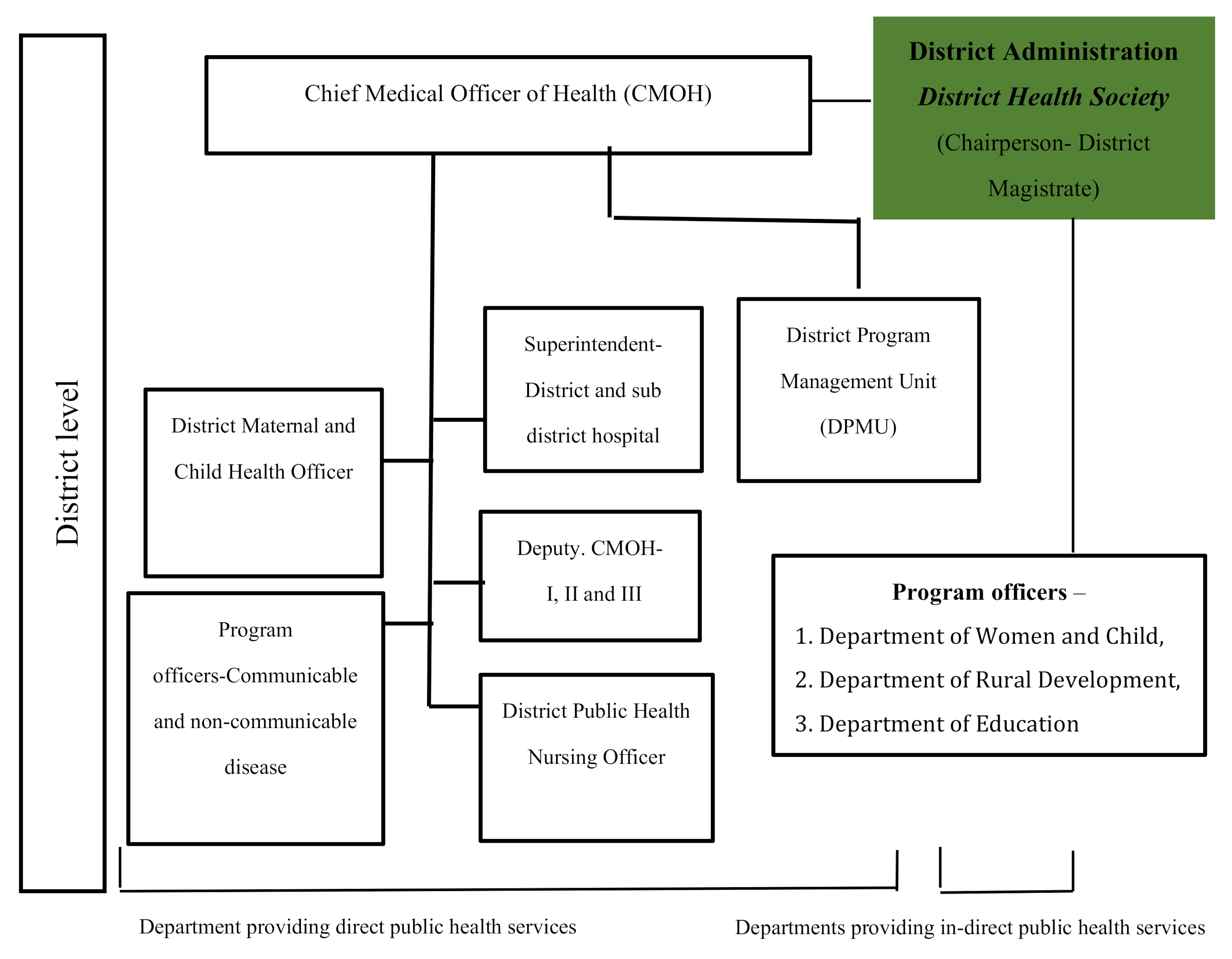
Context: Health System Connectivity at the District Level
2. Methods
2.1. Data Collection
2.2. Data Analysis
3. Results
3.1. The Health Decision-Making Process in Districts
“Bottom-up approach should be adopted while making district health plans… Suggestions from the community can be considered and discussed …But we have to adhere to the priorities set by (the) Government of India and State Government.”(Health Department Representative)
“Sometimes, issues related to funds shortage for implementing programmes can be taken care (of) by DHS… District specific useful ideas which need funds can be decided at the DHS.”(Health Department Representative)
“Interactions with other departments is only need based … otherwise, there are no such regular interactions other than DHS forum.”(Health Department Representative)
“Our department is not getting much importance in DHS meetings. One representative from our end just attends the meeting and is not aware of DHS functions... and the health department is also not taking the initiative to motivate us… Our role is poorly defined.”(Other department Representative)
3.2. Use of Data for Decision-Making
“HMIS is a structured format with (a) specific set of columns (indicators)... all data coming from different divisions can’t be uploaded on HMIS… MCTS are specifically reproductive and child health-based data portal, rather than for other public health programmes.....”(Health Department Representative)
“Data sharing between Health and the Department of Women and Child is a major challenge. There is no concordance between these two departments. At the district level, data sharing should be mandatory at DHS.”(other department Representative)
3.3. Extent of Data Use for Planning and Decision-Making
“Yes data is useful for planning (e.g., bed occupancy rate). When (the) Mission Director of NHM (National Health Mission) visited this hospital found bed occupancy rate at 130%. Then we send the proposal of increasing beds in maternity ward from 85 to 120 and was discussed in DHS meeting...”(Health Department Representative)
“We are not monitoring our programmes on the basis of our own data... we are not utilising the data... in fact, we are not benefiting from the large volume of data that we are collecting.“(Health Department Representative)
“Data is very much useful while preparing (the) district health plan. Data supports us every time, but it is also true that due to lack of time and inadequate manpower... it is not utilised. Data is a fascinating tool if we use it properly.”(Health Department Representative)
“There is no such link between funding and data; in my personal opinion, funding is particular (predefined state guideline) and never linked with data.”(other department Representative)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| VHND | Village Health Nutrition Days organised once a month aimed at promoting Reproductive Maternal Newborn Child Health initiatives. |
| ASHA | Accredited Social Health Activists are community health workers recruited under National Rural Health Mission who work as health promoters in the community. |
| Anganwadi workers | Anganwadi is the basic unit of the Integrated Child Development Services scheme and covers a population of 1000. The workers are females recruited from the local community and trained in non-formal pre-school education, nutrition and health. |
| JSSK Nischay Yan | Provision of free referral transport to pregnant women under Janani Shishu Suraksha Karyakram |
References
- Talukder, N.; Rob, U.; Mahabub-Ul-Anwar, U. Lessons Learned from Health Sector Reform: A Four-Country Comparison. Int. Q. Community Health Educ. 2008, 28, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Bossert, T.J.; Beauvais, J.C. Decentralization of health systems in Ghana, Zambia, Uganda and the Philippines: A comparative analysis of decision space. Health Policy Plan. 2002, 17, 14–31. [Google Scholar] [CrossRef] [PubMed]
- Somanji, H.; Barry, S.; Dram, B. Health systems strengthening: Improving district health service delivery and community ownership and participation. Afr. Health Monit. 2017, 15, 48–54. [Google Scholar]
- La Vincente, S.; Aldaba, B.; Firth, S.; Kraft, A.; Jimenez-Soto, E.; Clark, A. Supporting local planning and budgeting for maternal, neonatal and child health in the Philippines. Health Res. Policy Syst. 2013, 11, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mutemwa, R.I. HMIS and decision-making in Zambia: Re-thinking information solutions for district health management in decentralized health systems. Health Policy Plan. 2005, 21, 40–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maluka, S.; Kamuzora, P.; SanSebastian, M.; Byskov, J.; Ndawi, B.; Olsen, O.E.; Hurtig, A.K. Implementing accountability for reasonableness framework at district level in Tanzania: A realist evaluation. Implement. Sci. 2011, 6, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maluka, S.; Kamuzora, P.; Sebastian, M.S.; Byskov, J.; Olsen, O.E.; Shayo, E.; Ndawi, B.; Hurtig, A.K. Decentralized health care priority-setting in Tanzania: Evaluating against the accountability for reasonableness framework. Soc. Sci. Med. 2010, 71, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Roman, T.E.; Cleary, S.; McIntyre, D. Exploring the Functioning of Decision Space: A Review of the Available Health Systems Literature. Int. J. Health Policy Manag. 2017, 6, 365–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liwanag, H.J.; Wyss, K. Optimising decentralisation for the health sector by exploring the synergy of decision space, capacity and accountability: Insights from the Philippines. Health Res. Policy Syst. 2019, 17, 4. [Google Scholar] [CrossRef] [Green Version]
- Seshadri, S.R.; Parab, S.; Kotte, S.; Latha, N.; Subbiah, K. Decentralization and decision space in the health sector: A case study from Karnataka, India. Health Policy Plan. 2016, 31, 171–181. [Google Scholar] [CrossRef] [Green Version]
- Barros, A.J.D.; Victora, C.G. Measuring Coverage in MNCH: Determining and Interpreting Inequalities in Coverage of Maternal, Newborn, and Child Health Interventions. PLoS Med. 2013, 10, e1001390. [Google Scholar] [CrossRef] [Green Version]
- Pelletier, D.L.; Frongillo, E.A.; Gervais, S.; Hoey, L.; Menon, P.; Ngo, T.; Stoltzfus, R.J.; Ahmed, A.M.S.; Ahmed, T. Nutrition agenda setting, policy formulation and implementation: Lessons from the Mainstreaming Nutrition Initiative. Health Policy Plan. 2011, 27, 19–31. [Google Scholar] [CrossRef] [Green Version]
- Panda, B.; Thakur, H.P. Decentralization and health system performance—A focused review of dimensions, difficulties, and derivatives in India. BMC Health Serv. Res. 2016, 16, 561. [Google Scholar] [CrossRef] [Green Version]
- Mutale, W.; Chintu, N.; Amoroso, C.; Awoonor-Williams, K.; Phillips, J.; Baynes, C.; Michel, C.; Taylor, A.; Sherr, K. Population Health Implementation and Training-Africa Health Initiative Data Collaborative Improving health information systems for decision making across five sub-Saharan African countries: Implementation strategies from the African Health Initiative. BMC Health Serv. Res. 2013, 5, 9. [Google Scholar]
- Bhattacharyya, K.; Murray, J. Community Assessment and Planning for Maternal and Child Health Programs: A Participatory Approach in Ethiopia. Soc. Appl. Anthropol. 2000, 59, 255–266. [Google Scholar] [CrossRef]
- Garrib, A.; Stoops, N.; McKenzie, A.; Dlamini, L.; Govender, T.; Rohde, J.; Herbst, K. An evaluation of the District Health Information System in rural South Africa. S. Afr. Med. J. 2008, 98, 7. [Google Scholar]
- Gething, P.W.; Noor, A.M.; Gikandi, P.W.; Ogara, E.A.A.; Hay, S.I.; Nixon, M.S.; Snow, R.W.; Atkinson, P.M. Improving Imperfect Data from Health Management Information Systems in Africa Using Space–Time Geostatistics. PLoS Med. 2006, 3, e271. [Google Scholar] [CrossRef] [Green Version]
- Mate, K.S.; Bennett, B.; Mphatswe, W.; Barker, P.; Rollins, N. Challenges for Routine Health System Data Management in a Large Public Programme to Prevent Mother-to-Child HIV Transmission in South Africa. PLoS ONE 2009, 4, e5483. [Google Scholar] [CrossRef] [Green Version]
- Ronveaux, O.; Rickert, D.; Hadler, S.; Groom, H.; Lloyd, J.; Bchir, A.; Birmingham, M. The immunization data quality audit: Verifying the quality and consistency of immunization monitoring systems. Bull. World Health Organ. 2005, 83, 503–510. [Google Scholar]
- Wordl Health Organization. Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes-WHO’s Framework for Action; Word Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Ministry of Health and Family Welfare. National Rural Health Mission: Meetings People’s Health Needs in Rural Areas-Framework for Implementation 2005–2012; Ministry of Health and Family Welfare: New Delhi, India, 2020. [Google Scholar]
- Prasad, A.M.; Chakraborty, G.; Yadav, S.S.; Bhatia, S. Addressing the social determinants of health through health system strengthening and inter-sectoral convergence: The case of the Indian National Rural Health Mission. Glob. Health Action 2013, 6, 1–11. [Google Scholar] [CrossRef]
- Bhattacharyya, S.; Berhanu, D.; Taddesse, N.; Srivastava, A.; Wickremasinghe, D.; Schellenberg, J.; Iqbal Avan, B. District decision-making for health in low-income settings: A case study of the potential of public and private sector data in India and Ethiopia. Health Policy Plan. 2016, 31, 25–34. [Google Scholar] [CrossRef]
- Registrar General of India. Sample Registration System Bulletin 2014; Registrar General of India: New Delhi, India, 2014. [Google Scholar]
- Office of the Registrar General & Census Commissioner. Special Bulletian on Maternal Mortaliry in India 2010–12; Office of the Registrar General & Census Commissioner: New Delhi, India, 2020. [Google Scholar]
- Department of Health & Family Welfare. Governance; Department of Health & Family Welfare: New Delhi, India, 2017. [Google Scholar]
- Department of Health & Family Welfare. Health Management Information System State Dashboard-2015–16; Department of Health & Family Welfare: New Delhi, India, 2017. [Google Scholar]
- Creswell, J.W. Qualitative Inquiry and Research Design: Choosing among Five Approaches; Sage Publications: London, UK, 2007. [Google Scholar]
- Khaleghian, P. Decentralization and public services: The case of immunization. Soc. Sci. Med. 2004, 59, 163–183. [Google Scholar] [CrossRef] [Green Version]
- Nyamtema, A.S. Bridging the gaps in the Health Management Information System in the context of a changing health sector. BMC Med. Inform. Decis. Mak. 2010, 10, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abajebel, S.; Jira, C.; Beyene, W. Utilization of health information system at district level in jimma zone oromia regional state, South west ethiopia. Ethiop. J. Health Sci. 2011, 21, 65–76. [Google Scholar] [PubMed]
- Akaco, E.; Erastus, M.; Edward, K.; Scott, M. Data Demand and Use in the Health Sector in Central and Eastern Kenya; Measure Evaluation: Chapel Hill, NC, USA, 2015. [Google Scholar]
- Murthy, L.; Shepperd, S.; Clarke, M.J.; Garner, S.E.; Lavis, J.N.; Perrier, L.; Roberts, N.W.; Straus, S.E. Interventions to improve the use of systematic reviews in decision-making by health system managers, policy makers and clinicians. Cochrane Database of Syst. Rev. 2012, 9. [Google Scholar] [CrossRef]
- Gill, Z.; Bailey, P.E. Bottom up and top down: A comprehensive approach to improve care and strengthen the health system. J. Pak. Med. Assoc. 2010, 60, 927–935. [Google Scholar]
- Qazi, M.S.; Ali, M. Health Management Information System utilization in Pakistan: Challenges, pitfalls and the way forward. BioSci. Trends 2011, 5, 245–254. [Google Scholar] [CrossRef] [Green Version]
- Chitama, D.; Baltussen, R.; Ketting, E.; Kamazima, S.; Nswilla, A.; Mujinja, P.G. From papers to practices: District level priority setting processes and criteria for family planning, maternal, newborn and child health interventions in Tanzania. BMC Women’s Health 2011, 11, 46. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Methods | Source of Data | Sample in Two Districts |
|---|---|---|
| Observations | District decision-making meetings. | 4 |
| In-depth interviews | Respondents from the Health Department | 16 |
| Respondents from government departments that provide indirect public health services | 6 | |
| Respondents from the district administration | 2 | |
| Collection of data templates, which contribute to HMIS |
| |
| Health System Categories | Type of Maternal and Child Health Issues Discussed | Use of Data (Yes/No) * | Availability of Data (Yes/No) # | Availability of Indicators in HMIS # (per Month) |
|---|---|---|---|---|
| Service delivery | 1. Immunisation coverage: sub-district percentage | Y | Y | Number of infants 0–11 months who received: OPV1,2,3; BCG; DPT |
| 2. Institutional delivery: sub-district and facility-based | Y | Y | Number of facility deliveries (including C-sections); number of women discharged under 48 h after delivery | |
| 3. Deliveries: empanelment of private nursing homes under public private partnership scheme | Y | Y | Number of deliveries | |
| 4. Home births: sub-district | N | Y | Number of home deliveries | |
| 5. C-sections: number performed at facility | N | Y | Number of C-Section deliveries | |
| 6. Use of partograph | N | N | Not available | |
| 7. Information Education Communication (IEC), Behaviour Change Communication (BCC) activities conducted for malaria and dengue fever | N | Y | IEC/BCC activities conducted; available, usable etc. | |
| Health outcome | 8. Child malnutrition: proportion of underweight children in the district | Y | Y | A number of children with severe acute malnutrition (SAM). Of children weighed, numbers found to be: moderately underweight/severely underweight |
| 9. Childhood diseases prevalence: sub-district | N | Y | Number of cases of childhood diseases reported | |
| 10. Malnutrition among pregnant women | N | Y | Pregnant women with anaemia: number having Hb level <11, <7 Deaths of mothers due to anaemia, during pregnancy or delivery | |
| 11. Birth weight of newborn | N | Y | Number of newborns weighed at birth; weighing less than 2.5 kg | |
| 12. Maternal mortality rate | N | Y | Mortality details: name, age, sex, village, causes | |
| 13. Newborn and child death rate | N | Y | Mortality details: name, age, sex, village, causes | |
| Human Resouces | 14. Shortage of staff, e.g., at sub-district: Accrediated Social Health Activist (ASHA) Facilitator and data entry operators | Y | Y | Number of staff in post, vacancies etc. |
| 15. Arranging joint home-visits by ASHA and Anganwadi workers (AWW) to pregnant women near their expected delivery date: sub-district | Y | Y | Number of Village Health and Nutrition day (VHNDs) where Auxiliary Nurse and Midwife (ANM), AWW, ASHA present | |
| 16. Data maintenance skills of frontline workers | N | Y | Number of ASHAs fully trained (5 modules—23 days) | |
| 17. Counselling skills, inter-personal communication skills of Frontline workers | N | Y | Number of trained/skilled staff | |
| Infrastructure and Supplies | 18. Construction and renovation of primary health centre, requirement of additional beds | Y | Y | Construction of new primary health centres, staff quarters, new MCH complex, neonatal ward |
| 19. Operationalising new delivery points | Y | Y | Number of facilities where deliveries take place (delivery points). Number of children referred from health facility/delivery point | |
| 20. Referral transport under the Janani Sishu Suraksha Karaykram (JSSK): Nischay Jan ambulance scheme, including three-wheeler motorised vehicles | Y | Y | Number of sub-districts where referral transport service is available. Ambulance type. Number of sick infants transported by referral transport services | |
| 21. Stock out of medicine | N | Y | Stock position: drugs and medical commodities/consumables. Number of ASHAs having regular supplies for drug kits |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhattacharyya, S.; Issac, A.; Girase, B.; Guha, M.; Schellenberg, J.; Iqbal Avan, B. “There Is No Link Between Resource Allocation and Use of Local Data”: A Qualitative Study of District-Based Health Decision-Making in West Bengal, India. Int. J. Environ. Res. Public Health 2020, 17, 8283. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218283
Bhattacharyya S, Issac A, Girase B, Guha M, Schellenberg J, Iqbal Avan B. “There Is No Link Between Resource Allocation and Use of Local Data”: A Qualitative Study of District-Based Health Decision-Making in West Bengal, India. International Journal of Environmental Research and Public Health. 2020; 17(21):8283. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218283
Chicago/Turabian StyleBhattacharyya, Sanghita, Anns Issac, Bhushan Girase, Mayukhmala Guha, Joanna Schellenberg, and Bilal Iqbal Avan. 2020. "“There Is No Link Between Resource Allocation and Use of Local Data”: A Qualitative Study of District-Based Health Decision-Making in West Bengal, India" International Journal of Environmental Research and Public Health 17, no. 21: 8283. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218283