Octopus Watch Fosters Family Resilience by Enhancing Occupational Engagement for Children with Spina Bifida and/or Hydrocephalus: Pilot Study





Abstract
:1. Introduction
2. Methods
2.1. Pilot Research Design
2.2. Participants
2.3. Equipment
HeyJoy Octopus Watch v2
2.4. Procedure
2.5. Measures
2.5.1. Demographic Survey
2.5.2. Short Semi-Structured Interviews
2.5.3. Childhood Executive Functioning Inventory (CHEXI)
2.5.4. Canadian Occupational Performance Measure (COPM)
2.5.5. Activity Measure (HeyJoy Octopus Watch v2)
2.6. Quantitative Analyses
2.7. Qualitative Analyses
2.7.1. Focus Groups
2.7.2. Semi-Structured Interviews
3. Results
3.1. Quantitative Results
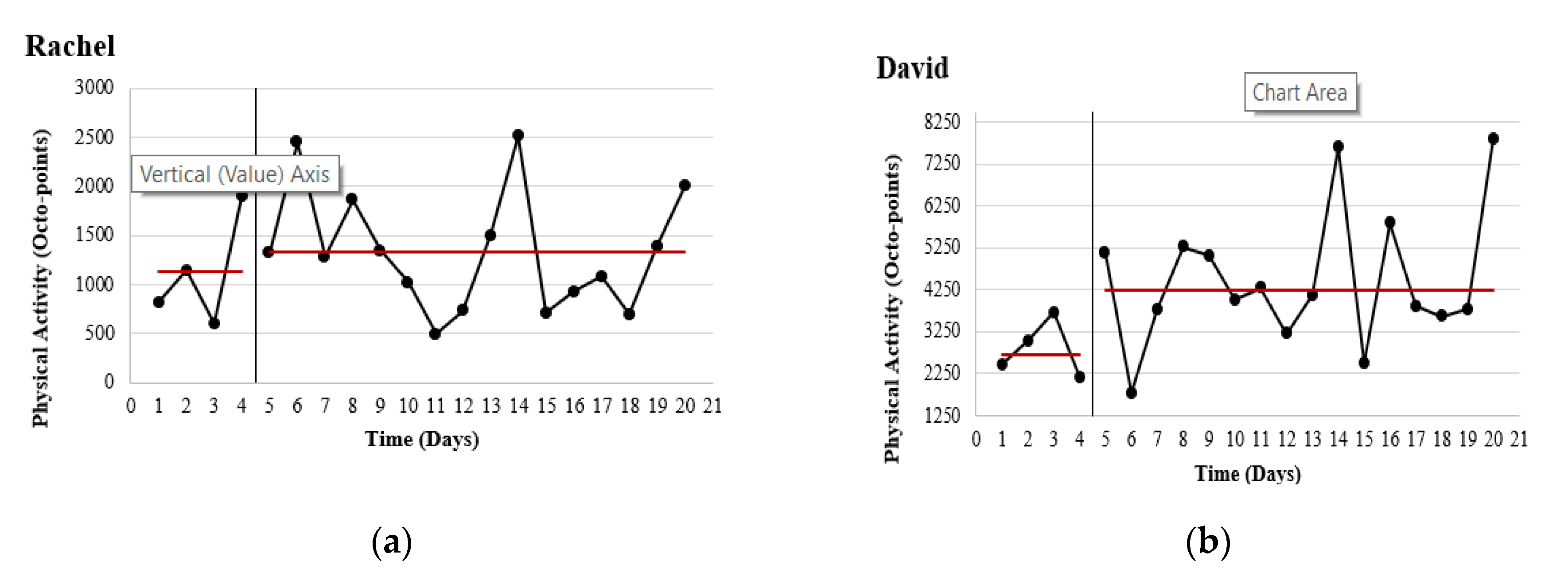
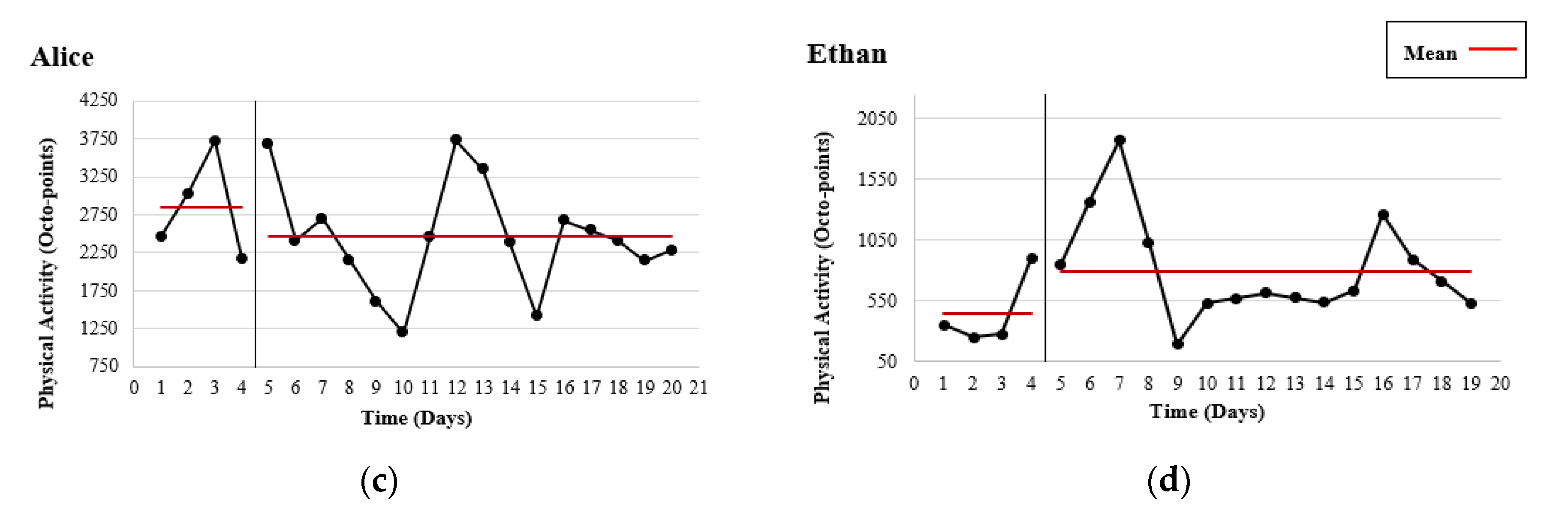
3.1.1. Physical Activity
3.1.2. CHEXI
3.1.3. COPM
3.2. Qualitative Findings
3.2.1. Rachel
“For her…to say I want to brush my teeth or to wash my hands, you know to get her feeding as well, to finish her breakfast with the rest of us, you know, that kind of a way. For her to become more independent”.
3.2.2. David
“I suppose I hope that our morning routine might get a bit better, definitely, and you know, that we’re not just going to have battles every morning trying to get things achieved, especially with other kids in the house…it’s just mayhem in the mornings”.
3.2.3. Alice
3.2.4. Ethan
3.3. Themes Identified
3.3.1. Developing a Routine
“Before, David was up and down and had no concentration at breakfast-time…now David sits and eats. He doesn’t need to use the timer anymore”.
3.3.2. Encouraging Independence
“The timer would go off and David would have task completed. He asks why it is going off if he had done task already”.
“Daniel got lost one day about 2 years ago, he was crying, he was very upset. Now he tells me that he can go up to somebody and tell them to ring mammy or daddy and show them the watch”.
“At the start, there was a lot of coaxing to go out and I would have to go with her or she wouldn’t stay out for long but by the end of the third week…she would look for me to open the door and she would go out herself—not for long but we are building it every day. I’m delighted to see her achieve this”.
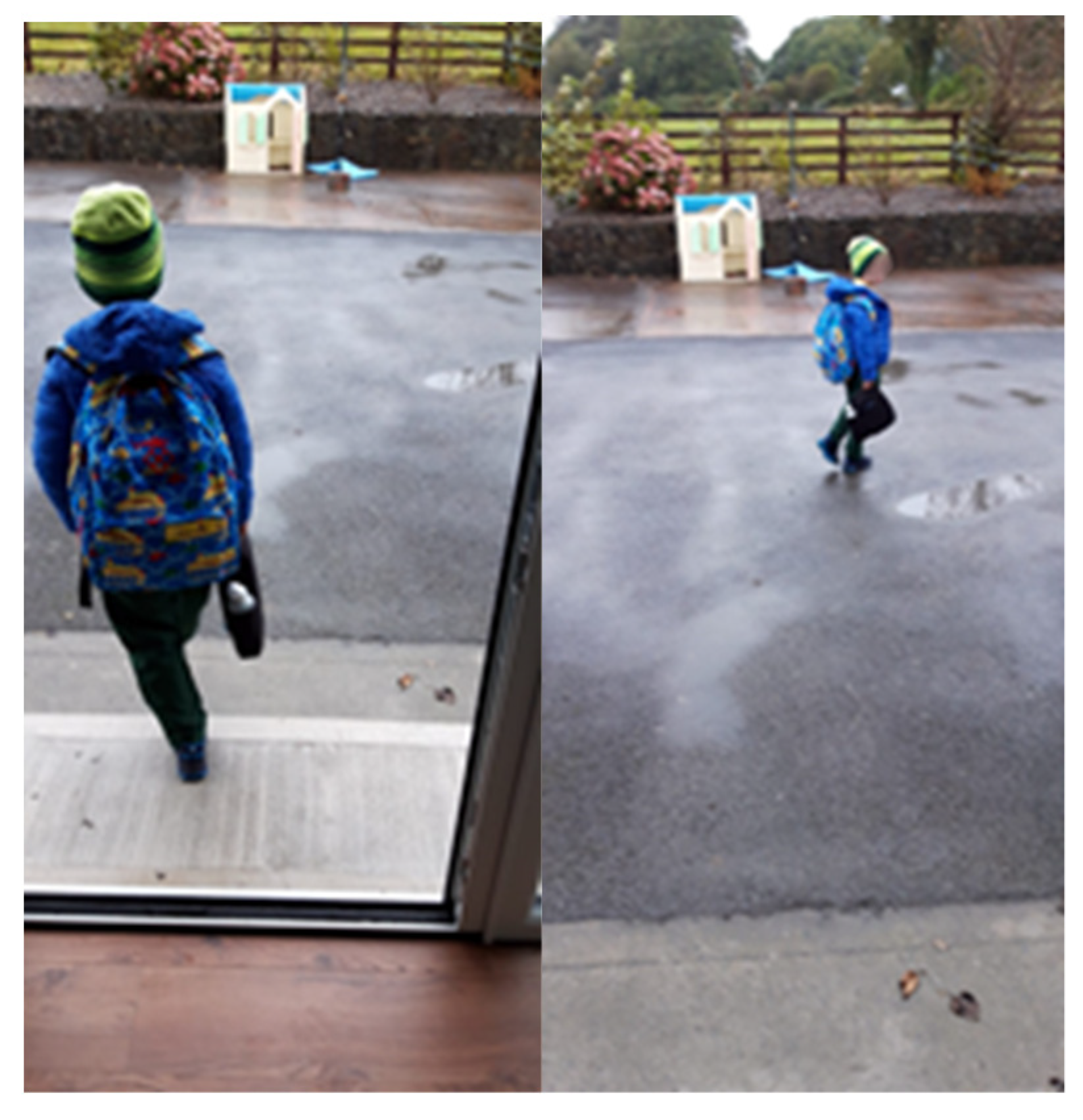
3.3.3. Showing Off the Watch
“This one was her going into play school in the morning and wanting to show the boys her watch” (in reference to Picture 3 in Supplementary Materials)
“Ethan was excited to go back to his sports group…after the summer break and show his friends his watch”.
4. Discussion
4.1. Limitations
4.2. Future Research and Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kondo, A.; Kamihira, O.; Ozawa, H. Neural tube defects: Prevalence, etiology and prevention. Int. J. Urol. 2008, 16, 49–57. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, R.; Delany, V.; O’Mahony, M.T.; Mullaney, C.; Lee, B.; Turner, M.J. Neural tube defects in the Republic of Ireland in 2009–11. J. Public Health 2015, 37, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloemen, M.; Verschuren, O.; Van Mechelen, C.; Borst, H.E.; De Leeuw, A.J.; Van Der Hoef, M.; De Groot, J.F. Personal and environmental factors to consider when aiming to improve participation in physical activity in children with Spina Bifida: A qualitative study. BMC Neurol. 2015, 15, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barkovich, A.J.; Fitz, C.R. Pediatric Neuroimaging. J. Comput. Assist. Tomogr. 1991, 15, 179. [Google Scholar] [CrossRef]
- Barker, E.; Saulino, M.; Caristo, A.M. Spina bifida. RN 2002, 65, 33–39. [Google Scholar] [PubMed]
- Kahle, K.T.; Kulkarni, A.V.; Limbrick, D.D.; Warf, B.C. Hydrocephalus in children. Lancet 2016, 387, 788–799. [Google Scholar] [CrossRef]
- Vinck, A.; Maassen, B.; Mullaart, R.; Rotteveel, J. Arnold-Chiari-II malformation and cognitive functioning in spina bifida. J. Neurol. Neurosurg. Psychiatry 2006, 77, 1083–1086. [Google Scholar] [CrossRef] [Green Version]
- Singh, D.K. Families of Children with Spina Bifida: A Review. J. Dev. Phys. Disabil. 2003, 15, 37–55. [Google Scholar] [CrossRef]
- Governey, S.; Culligan, E.; Leonard, J. The Health and Therapy Needs of Children with Spina Bifida in Ireland; Temple Street Childrens University Hospital: Dublin, Ireland, 2014. [Google Scholar]
- Strömfors, L.; Wilhelmsson, S.; Falk, L.; Höst, G.E. Experiences among children and adolescents of living with spina bifida and their visions of the future. Disabil. Rehabil. 2016, 39, 261–271. [Google Scholar] [CrossRef] [Green Version]
- Dennis, M.; Landry, S.H.; Barnes, M.; Fletcher, J.M. A model of neurocognitive function in spina bifida over the life span. J. Int. Neuropsychol. Soc. 2006, 12, 285–296. [Google Scholar] [CrossRef] [Green Version]
- Stubberud, J.; Langenbahn, D.; Elevine, B.; Stanghelle, J.; Schanke, A.-K. Goal Management Training of Executive Functions in Patients with Spina Bifida: A Randomized Controlled Trial. J. Int. Neuropsychol. Soc. 2013, 19, 672–685. [Google Scholar] [CrossRef] [PubMed]
- Kelly, N.C.; Ammerman, R.T.; Rausch, J.R.; Ris, M.D.; Yeates, K.O.; Oppenheimer, S.G.; Enrile, B.G. Executive functioning and psychological adjustment in children and youth with spina bifida. Child Neuropsychol. 2012, 18, 417–431. [Google Scholar] [CrossRef] [PubMed]
- Stuss, D.T. Traumatic brain injury: Relation to executive dysfunction and the frontal lobes. Curr. Opin. Neurol. 2011, 24, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Peny-Dahlstrand, M.; Bergqvist, L.; Hofgren, C.; Himmelmann, K.; Öhrvall, A.-M. Potential benefits of the cognitive orientation to daily occupational performance approach in young adults with spina bifida or cerebral palsy: A feasibility study. Disabil. Rehabil. 2018, 42, 228–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowman, R.M.; McLone, D.G.; Grant, J.A.; Tomita, T.; Ito, J.A. Spina Bifida Outcome: A 25-Year Prospective. Pediatr. Neurosurg. 2001, 34, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, D.; Dicianno, B.E.; Bellin, M. Self-management, preventable conditions and assessment of care among young adults with myelomeningocele. Child Care Health Dev. 2011, 37, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Vanderbom, K.A.; Driver, S.; Nery-Hurwit, M. A systematic framework to classify physical activity research for individuals with spina bifida. Disabil. Health J. 2014, 7, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Greene, C.M.; Bellgrove, M.A.; Gill, M.; Robertson, I.H. Noradrenergic genotype predicts lapses in sustained attention. Neuropsychologia 2009, 47, 591–594. [Google Scholar] [CrossRef]
- Paul, L.; Brewster, S.; Wyke, S.; McFadyen, A.K.; Sattar, N.; Gill, J.M.; Dybus, A.; Gray, C.M. Increasing physical activity in older adults using STARFISH, an interactive smartphone application (app); a pilot study. J. Rehabil. Assist. Technol. Eng. 2017, 4. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Benefits of Physical Activity. 2020. Available online: https://www.cdc.gov/physicalactivity/basics/pa-health/index.htm (accessed on 4 January 2020).
- De Groot, J.F.; Takken, T.; Van Brussel, M.; Gooskens, R.; Schoenmakers, M.; Versteeg, C.; Vanhees, L.; Helders, P. Randomized Controlled Study of Home-Based Treadmill Training for Ambulatory Children With Spina Bifida. Neurorehabil. Neural Repair 2011, 25, 597–606. [Google Scholar] [CrossRef]
- Shaw, E.J.; Stokes, T.; Camosso-Stefinovic, J.; Baker, R.; Baker, G.A.; Jacoby, A.; Camosso-Stefinovic, J. Self-management education for adults with epilepsy. Cochrane Database Syst. Rev. 2007, 2. [Google Scholar] [CrossRef] [Green Version]
- Du, S.; Yuan, C. Evaluation of patient self-management outcomes in health care: A systematic review. Int. Nurs. Rev. 2010, 57, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Berg-Emons, H.J.V.D.; Bussmann, J.B.; Brobbel, A.S.; Roebroeck, M.E.; Van Meeteren, J.; Stam, H.J. Everyday physical activity in adolescents and young adults with meningomyelocele as measured with a novel activity monitor. J. Pediatr. 2001, 139, 880–886. [Google Scholar] [CrossRef] [PubMed]
- Giarelli, E.; Bernhardt, B.A.; Mack, R.; Pyeritz, R.E. Adolescents’ Transition to Self-Management of a Chronic Genetic Disorder. Qual. Health Res. 2008, 18, 441–457. [Google Scholar] [CrossRef]
- Kingsnorth, S.; Healy, H.; MacArthur, C. Preparing for Adulthood: A Systematic Review of Life Skill Programs for Youth with Physical Disabilities. J. Adolesc. Health 2007, 41, 323–332. [Google Scholar] [CrossRef]
- Lindsay, S.; Kingsnorth, S.; Hamdani, Y. Barriers and facilitators of chronic illness self-management among adolescents: A review and future directions. J. Nurs. Health Chronic Illn. 2011, 3, 186–208. [Google Scholar] [CrossRef]
- Goracke, E.; Jacobs, K.; Pilney, E.; Shephard, K. Goal-Directed Leg Movements and Kicks in Infants with Spina Bifida. Ph.D. Thesis, St. Catherine University, St. Paul, MN, USA, 2016. [Google Scholar]
- Salah, H.; MacIntosh, E.; Rajakulendran, N. Wearable Tech: Leveraging Canadian Innovation to Improve Health; MaRS Discovery District: Toronto, ON, Canada, 2014. [Google Scholar]
- Puri, A.; Kim, B.; Nguyen, O.; Stolee, P.; Tung, J.; Lee, J. User Acceptance of Wrist-Worn Activity Trackers Among Community-Dwelling Older Adults: Mixed Method Study. JMIR mHealth uHealth 2017, 5, e173. [Google Scholar] [CrossRef] [Green Version]
- Bove, L.A. Increasing Patient Engagement Through the Use of Wearable Technology. J. Nurse Pract. 2019, 15, 535–539. [Google Scholar] [CrossRef] [Green Version]
- Rosser, B.A.; Vowles, K.E.; Keogh, E.; Eccleston, C.; Mountain, G.A. Technologically-assisted behaviour change: A systematic review of studies of novel technologies for the management of chronic illness. J. Telemed. Telecare 2009, 15, 327–338. [Google Scholar] [CrossRef]
- Lansing, A.H.; Berg, C.A. Topical Review: Adolescent Self-Regulation as a Foundation for Chronic Illness Self-Management. J. Pediatr. Psychol. 2014, 39, 1091–1096. [Google Scholar] [CrossRef] [Green Version]
- Dicianno, B.E.; Fairman, A.D.; McCue, M.; Parmanto, B.; Yih, E.; McCoy, A.; Pramana, G.; Yu, D.X.; McClelland, J.; Collins, D.M.; et al. Feasibility of Using Mobile Health to Promote Self-Management in Spina Bifida. Am. J. Phys. Med. Rehabil. 2016, 95, 425–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bratton, S.C.; Ray, D.; Rhine, T.; Jones, L. The Efficacy of Play Therapy With Children: A Meta-Analytic Review of Treatment Outcomes. Prof. Psychol. Res. Pract. 2005, 36, 376–390. [Google Scholar] [CrossRef]
- Webster-Stratton, C. The Incredible Years: Use of Play Interventions and Coaching for Children with Externalizing Difficulties. Am. Psychol. Assoc. 2015. [Google Scholar] [CrossRef]
- Nwokah, E.; Hsu, H.C.; Gulker, H. The Use of Play Materials in Early Intervention: The Dilemma of Poverty. Am. J. Play 2013, 5, 187–218. [Google Scholar]
- Joy Familytech. Octopus by JOY, the First Icon-Based Watch™ that Empowers Kids. 2020. Available online: https://www.heyjoy.io/ (accessed on 7 January 2020).
- Lynch, H.; Moore, A. Play as an occupation in occupational therapy. Br. J. Occup. Ther. 2016, 79, 519–520. [Google Scholar] [CrossRef] [Green Version]
- McKim, C.A. The value of mixed methods research: A mixed methods study. J. Mix. Methods Res. 2017, 11, 202–222. [Google Scholar] [CrossRef]
- Ha, V.S.; Whittaker, A. ‘Closer to my world’: Children with autism spectrum disorder tell their stories through photovoice. Glob. Public Health 2016, 11, 546–563. [Google Scholar] [CrossRef]
- Allmark, P.; Stevenson, K.J.; Stotzer, T. Having a Voice and Being Heard: Photography and Children’s Communication through Photovoice; ECU Research Online: 2017. Refereed Proceedings of the Australian and New Zealand Communication Association Conference 2017—Communication Worlds: Access, Voice, Diversity, Engagement, Sydney. This Conference Proceeding Is Posted at Research Online. Available online: https://ro.ecu.edu.au/ecuworkspost2013/5056 (accessed on 15 January 2020).
- Tickle, S. Engaging young people through photovoice in coastal resorts. Qual. Res. J. 2019, 20, 103–115. [Google Scholar] [CrossRef]
- Naughton, F.; Johnston, D. A starter kit for undertaking n-of-1 trials. Eur. Health Psychol. 2014, 16, 196–205. [Google Scholar]
- Kwasnicka, D.; Naughton, F. N-of-1 methods: A practical guide to exploring trajectories of behaviour change and designing precision behaviour change interventions. Psychol. Sport Exerc. 2020, 47, 101570. [Google Scholar] [CrossRef]
- Hoffer, M.M.; Feiwell, E.; Perry, R.; Perry, J.; Bonnett, C. Functional Ambulation in Patients with Myelomeningocele. J. Bone Jt. Surg.-Am. Vol. 1973, 55, 137–148. [Google Scholar] [CrossRef]
- Schoenmakers, M.A.G.C.; Gulmans, V.A.M.; Gooskens, R.H.J.M.; Pruijs, J.E.H.; Helders, P.J.M. Spinal fusion in children with spina bifida: Influence on ambulation level and functional abilities. Eur. Spine J. 2004, 14, 415–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawson, S.; Manderson, L.; Tallo, V.L. A Manual for the Use of Focus Groups; International Nutrition Foundation for Developing Countries: Boston, MA, USA, 1993. [Google Scholar]
- Rabiee, F. Focus-group interview and data analysis. Proc. Nutr. Soc. 2004, 63, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Burris, M.A. Photovoice: Concept, Methodology, and Use for Participatory Needs Assessment. Health Educ. Behav. 1997, 24, 369–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trost, S.G.; Pate, R.R.; Freedson, P.S.; Sallis, J.F.; Taylor, W.C. Using objective physical activity measures with youth: How many days of monitoring are needed? Med. Sci. Sports Exerc. 2000, 32, 426–431. [Google Scholar] [CrossRef] [PubMed]
- WhatsApp. WhatsApp Security. 2020. Available online: https://www.whatsapp.com/security/ (accessed on 6 March 2020).
- Vanderbom, K.A. Exploring Physical Activity Behaviors in Adults with Spina Bifida: A Mixed Methods Approach. Ph.D. Thesis, Oregon State University, Corvallis, OR, USA, 2013. [Google Scholar]
- Carswell, A.; McColl, M.A.; Baptiste, S.; Law, M.; Polatajko, H.; Pollock, N. The Canadian Occupational Performance Measure: A Research and Clinical Literature Review. Can. J. Occup. Ther. 2004, 71, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Thorell, L.B.; Nyberg, L. The Childhood Executive Functioning Inventory (CHEXI): A New Rating Instrument for Parents and Teachers. Dev. Neuropsychol. 2008, 33, 536–552. [Google Scholar] [CrossRef]
- Thorell, L.B.; Eninger, L.; Brocki, K.C.; Bohlin, G. Childhood Executive Function Inventory (CHEXI): A promising measure for identifying young children with ADHD? J. Clin. Exp. Neuropsychol. 2010, 32, 38–43. [Google Scholar] [CrossRef]
- Camerota, M.; Willoughby, M.T.; Kuhn, L.J.; Blair, C. The Childhood Executive Functioning Inventory (CHEXI): Factor structure, measurement invariance, and correlates in US preschoolers. Child Neuropsychol. 2016, 24, 322–337. [Google Scholar] [CrossRef]
- Law, M.; Baptiste, S.; Carswell, A.; McColl, M.A.; Polatajko, H.; Pollock, N. Canadian Occupational Performance Measure, 2nd ed.; CAOT Publications ACE: Toronto, ON, Canada, 1994. [Google Scholar]
- Yang, S.-Y.; Lin, C.-Y.; Lee, Y.-C.; Chang, J.-H. The Canadian occupational performance measure for patients with stroke: A systematic review. J. Phys. Ther. Sci. 2017, 29, 548–555. [Google Scholar] [CrossRef] [Green Version]
- Kazdin, A.E. Single-Case Research Designs: Methods for Clinical and Applied Settings, 2nd ed.; Oxford University Press: New York, NY, USA, 2011. [Google Scholar]
- McDonald, S.; Quinn, F.; Vieira, R.; O’Brien, N.; White, M.; Johnston, D.W.; Sniehotta, F.F. The state of the art and future opportunities for using longitudinal n-of-1 methods in health behaviour research: A systematic literature overview. Health Psychol. Rev. 2017, 11, 307–323. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, J.A.; Kronish, I.M.; Falzon, L.; Cheung, Y.K.; Davidson, K.W. N-of-1 Randomized Intervention Trials in Health Psychology: A Systematic Review and Methodology Critique. Ann. Behav. Med. 2018, 52, 731–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyman, S.R.; Goodwin, K.; Kwasnicka, D.; Callaway, A. Increasing walking among older people: A test of behaviour change techniques using factorial randomised N-of-1 trials. Psychol. Health 2015, 31, 313–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power for the Behavioural Sciences; Lawrence Erlbaum: Hilsdale, NY, USA, 1988. [Google Scholar]
- Lambert, V.; Glacken, M.; McCarron, M. Employing an ethnographic approach: Key characteristics. Nurse Res. 2011, 19, 17–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- QSR International. NVivo Qualitative Data Analysis Software Version 12; QSR International: Burlington, MA, USA, 2018. [Google Scholar]
- Graneheim, U.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- Patton, M.Q. Enhancing the quality and credibility of qualitative analysis. Health Serv. Res. 1999, 34, 1189–1208. [Google Scholar]
- Graneheim, U.H.; Lindgren, B.-M.; Lundman, B. Methodological challenges in qualitative content analysis: A discussion paper. Nurse Educ. Today 2017, 56, 29–34. [Google Scholar] [CrossRef]
- Bejerholm, U.; Eklund, M. Occupational Engagement in Persons With Schizophrenia: Relationships to Self-Related Variables, Psychopathology, and Quality of Life. Am. J. Occup. Ther. 2007, 61, 21–32. [Google Scholar] [CrossRef] [Green Version]
- Poulin, V.; Korner-Bitensky, N.; Bherer, L.; Lussier, M.; Dawson, D.R. Comparison of two cognitive interventions for adults experiencing executive dysfunction post-stroke: A pilot study. Disabil. Rehabil. 2016, 39, 1–13. [Google Scholar] [CrossRef]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, B.; Schweizer, T.A.; O’Connor, C.; Turner, G.; Gillingham, S.; Stuss, D.T.; Manly, T.; Robertson, I.H. Rehabilitation of executive functioning in patients with frontal lobe brain damage with goal management training. Front. Hum. Neurosci. 2011, 5, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiese, M.S.; Ronna, B.; Ott, U. P value interpretations and considerations. J. Thorac. Dis. 2016, 8, E928–E931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cott, C.A. Client-centred rehabilitation: Client perspectives. Disabil. Rehabil. 2004, 26, 1411–1422. [Google Scholar] [CrossRef]
- Hammell, K.W. Dimensions of Meaning in the Occupations of Daily Life. Can. J. Occup. Ther. 2004, 71, 296–305. [Google Scholar] [CrossRef]
- Hitch, D.; Pepin, G.; Stagnitti, K. In the Footsteps of Wilcock, Part Two: The Interdependent Nature of Doing, Being, Becoming, and Belonging. Occup. Ther. Health Care 2014, 28, 247–263. [Google Scholar] [CrossRef]
- Tong, A.; Jones, J.; Craig, J.C.; Singh-Grewal, D. Children’s experiences of living with juvenile idiopathic arthritis: A thematic synthesis of qualitative studies. Arthritis Care Res. 2012, 64, 1392–1404. [Google Scholar] [CrossRef]
- Lindsay, S. A Qualitative Synthesis of Adolescents’ Experiences of Living with Spina Bifida. Qual. Health Res. 2014, 24, 1298–1309. [Google Scholar] [CrossRef]
- Bakaniene, I.; Žiukienė, L.; Vasiliauskienė, V.; Prasauskienė, A. Participation of Children with Spina Bifida: A Scoping Review Using the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) as a Reference Framework. Medicina 2018, 54, 40. [Google Scholar] [CrossRef] [Green Version]
- Van Der Slot, W.; Nieuwenhuijsen, C.; Berg-Emons, R.V.D.; Wensink-Boonstra, A.; Stam, H.; Roebroeck, M. Participation and health-related quality of life in adults with spastic bilateral cerebral palsy and the role of self-efficacy. J. Rehabil. Med. 2010, 42, 528–535. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. The evolution of social cognitive theory. In Great Minds in Management; Smith, K.G., Hitt, M.A., Eds.; Oxford University Press: Oxford, UK, 2005; pp. 9–35. [Google Scholar]
- Peny-Dahlstrand, M.; Åhlander, A.-C.; Krumlinde-Sundholm, L.; Gosman-Hedström, G. Quality of performance of everyday activities in children with spina bifida: A population-based study. Acta Paediatr. 2009, 98, 1674–1679. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, T.D.; Noyes, J.; Spencer, L.H.; Kubis, H.-P.; Hastings, R.P.; Whitaker, R. Systematic review of physical activity and exercise interventions to improve health, fitness and well-being of children and young people who use wheelchairs. BMJ Open Sport Exerc. Med. 2016, 2, e000109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kriemler, S.; Meyer, U.; Martin, E.; Van Sluijs, E.M.F.; Andersen, L.B.; Martin, B.W. Effect of school-based interventions on physical activity and fitness in children and adolescents: A review of reviews and systematic update. Br. J. Sports Med. 2011, 45, 923–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biddle, S.J.H.; Mutrie, N. Psychology of Physical Activity: Determinants, Well-Being and Interventions, 2nd ed.; Routledge: London, UK, 2008. [Google Scholar]
- Mercer, K.; Giangregorio, L.M.; Schneider, E.; Chilana, P.; Li, M.; Grindrod, K. Acceptance of Commercially Available Wearable Activity Trackers Among Adults Aged Over 50 and With Chronic Illness: A Mixed-Methods Evaluation. JMIR mHealth uHealth 2016, 4, e7. [Google Scholar] [CrossRef] [PubMed]
- Chantry, J.; Dunford, C. How do Computer Assistive Technologies Enhance Participation in Childhood Occupations for Children with Multiple and Complex Disabilities? A Review of the Current Literature. Br. J. Occup. Ther. 2010, 73, 351–365. [Google Scholar] [CrossRef]
- Vaquero, E.; Urrea, A.; Mundet, A. Promoting resilience through technology, art and a child rights-based approach. Rev. Cercet. Interv. Soc. 2014, 45, 144. [Google Scholar]
- Holmbeck, G.N.; Devine, K.A. Psychosocial and family functioning in spina bifida. Dev. Disabil. Res. Rev. 2010, 16, 40–46. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Developmental Milestone | Typically Developing Infant | Infant with SB |
|---|---|---|
| Sitting | 6–7 months | 1–2 years |
| Crawling | 7–11 months | 1–2 years |
| Standing | 9–13 months | 3 years |
| Walking | 12–15 months | 3–7 years |
| Level of Functional Mobility | Description |
|---|---|
| Normal ambulation | Independent and unrestricted ambulation without use of assisted devices. |
| Community ambulation | Independent outdoor ambulation with/without use of brace and/or assisted devices; using wheelchair for longer distances. |
| Household ambulation | Using braces or assisted devices for indoor ambulation; using wheelchair for outdoor locomotion. |
| Non-functional ambulation | Walking only in therapeutic situations. |
| Functional wheelchair user | Wheelchair for mobility but can self-propel the wheelchair. |
| Age | Sex | Ethnicity | Assistive Devices | Independently Walking | |
|---|---|---|---|---|---|
| Rachel | 4 | F | Irish | Wheelchair | No |
| David | 7 | M | Irish | None | Yes |
| Alice | 3.5 | F | Irish | Braces (full-time) Wheelchair (Part-time) | Yes (short distance) |
| Ethan | 7 | M | Irish | Wheelchair (full-time) Braces (full-time) | No |
| Physical Activity (Octo-Points) | |
|---|---|
| Rachel | |
| r2 | 0.003 |
| p-value | 0.833 |
| David | |
| r2 | 0.28 |
| p-value | 0.021 * |
| Alice | |
| r2 | 0.042 |
| p-value | 0.397 |
| Ethan | |
| r2 | 0.004 |
| p-value | 0.796 |
| Pre-Test | Post-Test | Difference | % Change | |
|---|---|---|---|---|
| Rachel | ||||
| Working memory | 41 | 40 | −1 | −2.4 |
| Inhibition | 35 | 29 | −6 | −17.1 |
| David | ||||
| Working memory | 46 | 45 | −1 | −2.2 |
| Inhibition | 43 | 37 | −6 | −14 |
| Alice | ||||
| Working memory | 38 | 41 | 3 | 7.9 |
| Inhibition | 49 | 37 | −12 | −24.5 |
| Ethan | ||||
| Working memory | 44 | 41 | −3 | −6.8 |
| Inhibition | 50 | 45 | −5 | −10 |
| Pre-Test | Post-Test | Mean Difference | Individual Goals | |
|---|---|---|---|---|
| Rachel | Feeding/mealtime Washing hands Brushing teeth Independence Outside play | |||
| Performance | 3.8 | 5.4 | 1.6 | |
| Satisfaction | 4.4 | 5.8 | 1.4 | |
| David | Toileting Storytime Homework Medication Morning routine | |||
| Performance | 3.2 | 7.6 | 4.4 | |
| Satisfaction | 3.4 | 7.2 | 3.8 | |
| Alice | Feeding/mealtime Daily routine Toileting Clean-up Walking | |||
| Performance | 5.0 | 6.6 | 1.6 | |
| Satisfaction | 4.6 | 7.4 | 2.8 | |
| Ethan | Brushing teeth Medication Toileting Outings (school) Homework | |||
| Performance | 4.6 | 5.4 | 0.8 | |
| Satisfaction | 4.4 | 5.8 | 1.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jennings, M.; Guilfoyle, A.; Green, J.; Cleary, Y.; Gowran, R.J. Octopus Watch Fosters Family Resilience by Enhancing Occupational Engagement for Children with Spina Bifida and/or Hydrocephalus: Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 8316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228316
Jennings M, Guilfoyle A, Green J, Cleary Y, Gowran RJ. Octopus Watch Fosters Family Resilience by Enhancing Occupational Engagement for Children with Spina Bifida and/or Hydrocephalus: Pilot Study. International Journal of Environmental Research and Public Health. 2020; 17(22):8316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228316
Chicago/Turabian StyleJennings, Mark, Aoife Guilfoyle, James Green, Yvonne Cleary, and Rosemary Joan Gowran. 2020. "Octopus Watch Fosters Family Resilience by Enhancing Occupational Engagement for Children with Spina Bifida and/or Hydrocephalus: Pilot Study" International Journal of Environmental Research and Public Health 17, no. 22: 8316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228316