The Relationship between Health Status and Social Activity of Perimenopausal and Postmenopausal Women (Health Status and Social Relationships in Menopause)



Abstract
:1. Introduction
- (1)
- Are there differences in the level of physical activity between the participants of U3A and the group not participating in any formal groups and possibly to what extent?
- (2)
- Are there differences in the number of climacteric symptoms between the examined groups?
- (3)
- What is the level of depression in the examined groups and are there differences between the examined groups?
- (4)
- Is there a relationship between the level of physical activity and depression?
2. Materials and Methods
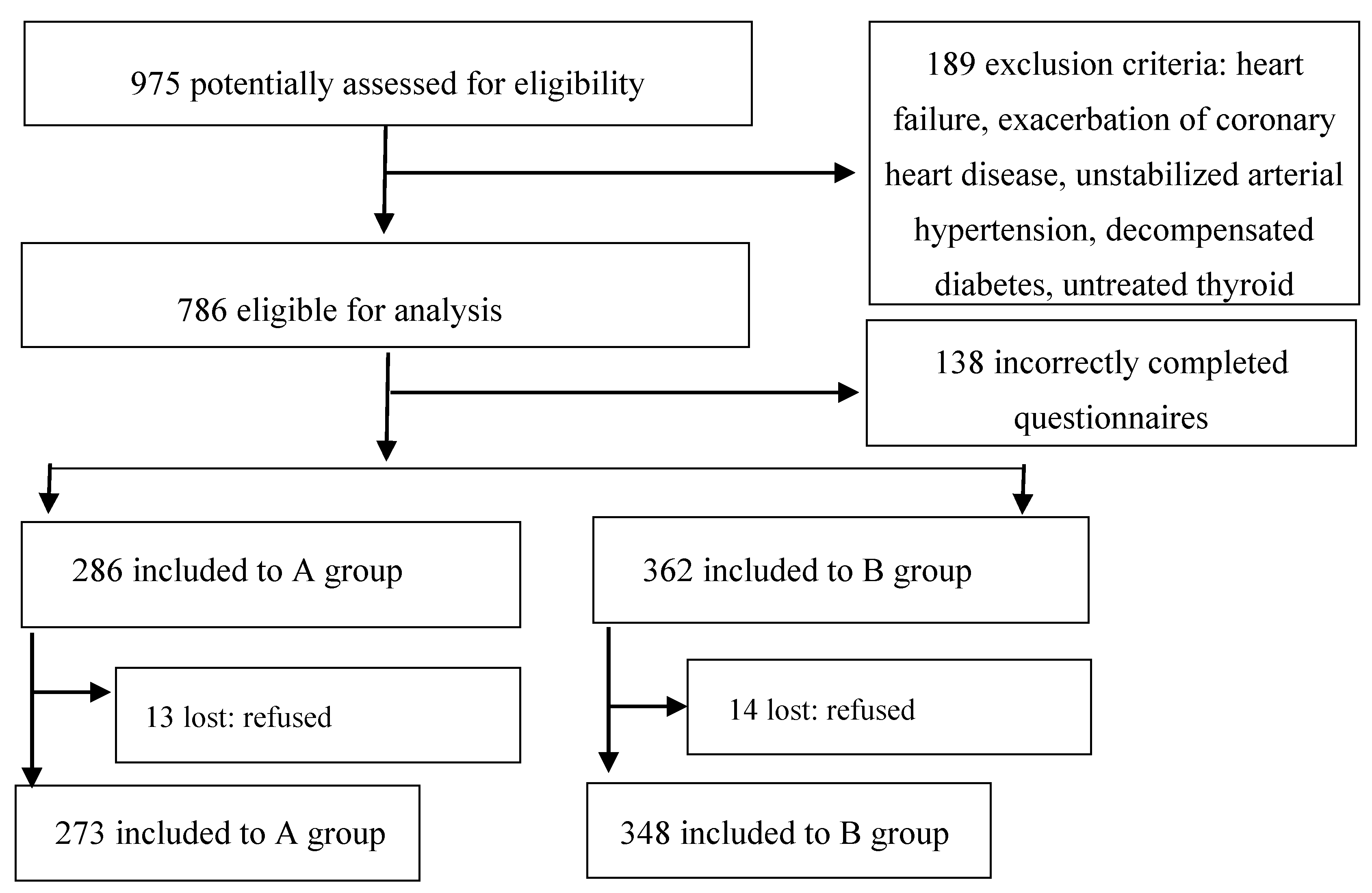
2.1. Material Status
2.2. Method
2.3. Organization of the Study
2.4. Ethical Considerations
2.5. Statistical Analysis
3. Results
3.1. Physical Activity
3.2. Climacteric Symptoms
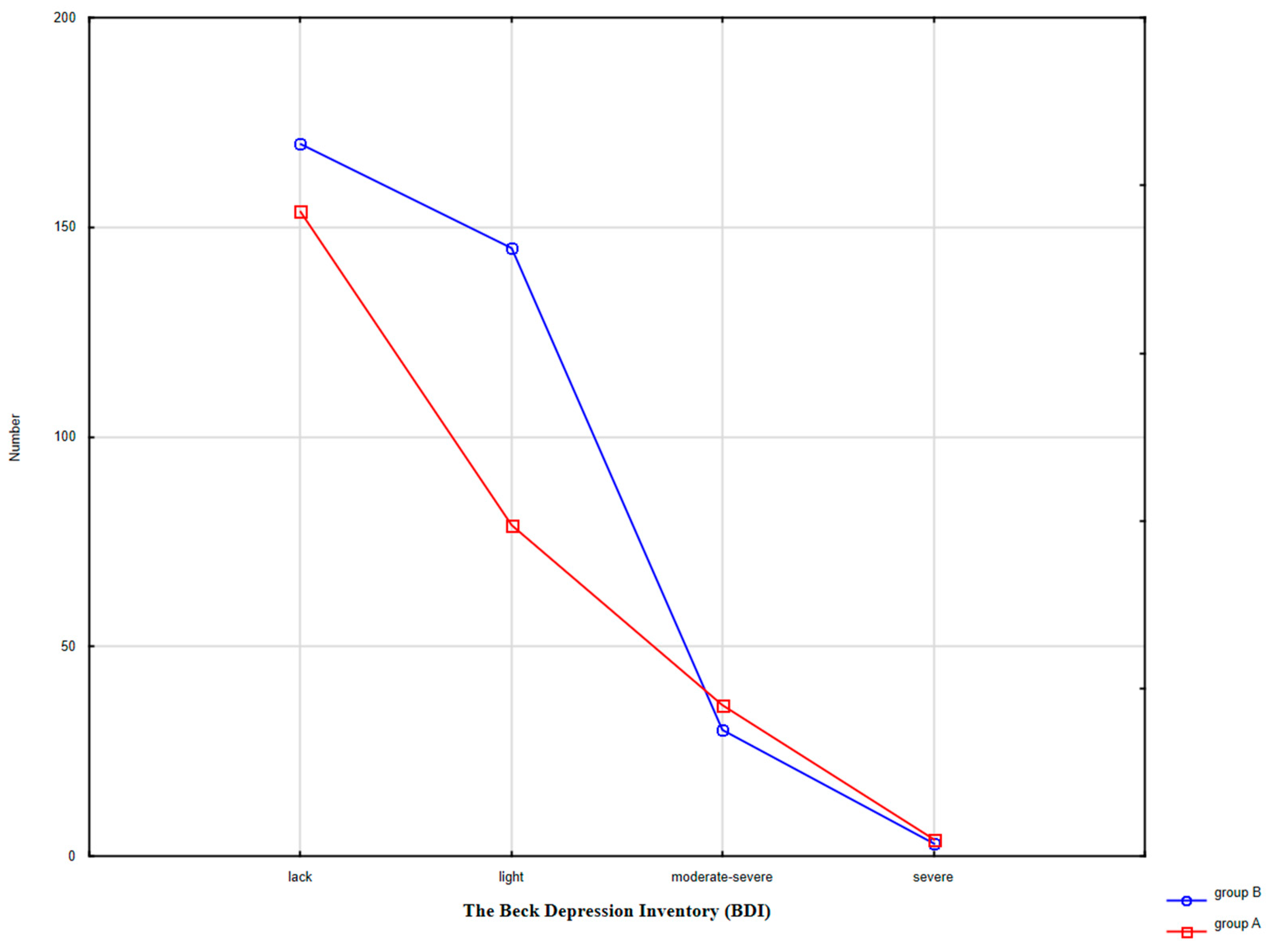
3.3. Depressive Symptoms
4. Discussion
4.1. The University of the Third Age (U3A)
4.2. Climacteric Symptoms
4.3. Depressive Symptoms
4.4. Physical Activity
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Research on the menopause in the 1990s. In WHO Technical Report Series 866; Report of a WHO Scientific Group; WHO: Geneva, Switzerland, 1996. [Google Scholar]
- Skrzypulec, V.; Naworska, B.; Drosdzol, A. The impact of climacteric symptoms on functioning and quality of life among women in perimenopausal stage. Przegląd Menopauzalny 2007, 2, 96–101. Available online: https://www.termedia.pl/The-impact-of-climacteric-symptoms-on-functioning-and-quality-of-life-among-women-in-perimenopausal-stage,4,8102,1,1.html (accessed on 25 April 2007).
- Santoro, N.; Epperson, C.N.; Mathews, S.B. Menopausal symptoms and their management. Endocrinol. Metab. Clin. N. Am. 2015, 44, 3, 497–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llaneza, P.; Garcia-Portilla, M.P.; Llaneza-Suarez, D.; Armott, B.; Perez-Lopez, F.R. Depressive disorders and the menopause transition. Maturitas 2012, 71, 120–130. [Google Scholar] [CrossRef] [PubMed]
- MacLennan, A.H.; Broadbent, J.L.; Lester, S.; Moore, V. Oral estrogen and combined estrogen/progestagen therapy versus placebo for hot flushes. Cochrane Database Syst. Rev. 2004, 4, CD002978. [Google Scholar] [CrossRef]
- Gencel, V.B.; Benjamin, M.M.; Bahou, S.N.; Khail, R.A. Vascular effects of phytoestrogens and alternative menopausal hormone therapy in cardiovascular disease. Mini Rev. Med. Chem. 2012, 12, 149–174. [Google Scholar] [CrossRef] [PubMed]
- Freeman, E.W.; Samuel, M.D.; Lin, H.; Nelson, D.B. Association of hormones and menopausal status with depressed mood in women with no history of depression. Arch. Gen. Psychiatry 2006, 63, 375–382. [Google Scholar] [CrossRef]
- Gibbs, Z.; Lee, S.; Kulkarni, J. Factors associated with depression during the perimenopausal transition. Women Health Issues 2013, 23, 301–307. [Google Scholar] [CrossRef]
- Umberson, D.; Montez, J.K. Social Relationships and Health: A Flashpoint for Health Policy. J. Health Soc. Behav. 2010, 51 (Suppl. 1), 54–66. [Google Scholar] [CrossRef] [Green Version]
- Scocco, P.; Nassuato, M. The role of social relationships among elderly community-dwelling and nursing-home residents: Findings from a quality of life study. Psychogeriatrics 2017, 17, 231–237. [Google Scholar] [CrossRef]
- Blümel, J.E.; Castelo-Branco, C.; Cancelo, M.J.; Córdova, A.T.; Binfa, L.E.; Bonilla, H.G.; Muñoz, I.G.; Vergara, V.G.; Sarrá, S.C. Relationship between psychological complaints and vasomotor symptoms during climacteric. Maturitas 2004, 49, 205–210. [Google Scholar] [CrossRef]
- Deeks, A.A. Psychological aspects of menopause Management. Best Practice and Research. Clinical Endocrinol. Metab. 2003, 17, 17–31. [Google Scholar] [CrossRef]
- Antonucci, T.C.; Lansford, J.E.; Akiyama, H.; Smith, J.; Baltes, M.M.; Takahashi, K.; Fuhrer, R.; Dartigues, J.-F. Differences Between Men and Women in Social Relations, Resource Deficits, and Depressive Symptomatology During Later Life in Four Nations. J. Soc. Issue 2002, 58, 767–783. [Google Scholar] [CrossRef] [Green Version]
- Zając-Gawlak, I.; Pośpiech, D.; Kroemeke, A.; Mossakowska, M.; Gába, A.; Pelclová, J.; Přidalová, M.; Kłapcińska, B. Physical activity, body composition and general health status of physically active students of the University of the Third Age (U3A). Arch. Gerontol. Geriatr. 2016, 64, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Krzepota, J.; Biernat, E.; Florkiewicz, B. The Relationship between Levels of Physical Activity and Quality of Life among Students of the University of the Third Age. Cent. Eur. J. Public Health. 2015, 23, 335–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maniecka-Bryła, I.; Gajewska, O.; Burzyńska, M.; Bryła, M. Factors Associated with Self-Rated Health (SRH) of a University of the Third Age (U3A) Class Participants. Arch. Gerontol. Geriatr. 2013, 57, 156–161. [Google Scholar] [CrossRef]
- Mitchell, R.A.; Legge, V.; Sinclair-Legge, G. Membership of the University of the Third Age (U3A) and perceived well-being. Disabil. Rehabil. 1997, 19, 244–248. [Google Scholar] [CrossRef]
- Hughes, M.E.; Waite, L.J. Marital biography and health at mid-life. J. Health Soc. Behav. 2009, 50, 344–358. [Google Scholar] [CrossRef] [Green Version]
- Avis, N.E.; Brockwell, S.; Colvin, A.A. Universal menopausal syndrome? Am. J. Med. 2005, 11, 37–46. [Google Scholar] [CrossRef]
- Sherman, S.; Miller, H.; Nerurkar, L.; Schiff, I. Research opportunities for reducing the burden of menopause-related symptoms. Am. J. Med. 2005, 118, 166–171. [Google Scholar] [CrossRef]
- Sternfeld, B.; Dugan, S. Physical Activity and Health During the Menopausal Transition. Obstet. Gynecol. Clin. N. Am. 2011, 3, 537–566. [Google Scholar] [CrossRef] [Green Version]
- Avis, N.E.; Colvin, A.; Bromberger, J.T.; Hess, R.; Matthews, K.A.; Ory, M.; Schocken, M. Change in health-related quality of life over the menopausal transition in a multiethnic cohort of middle-aged women: Study of Women’s Health Across the Nation. Menopause 2009, 16, 860–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.F.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12 country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasińska, Z.; Tracz, E. Universities of the Third Age and their role in the active aging process. Soc. Sci. Pol. 2013, 1, 102–110, ISSN 2080-6019. [Google Scholar]
- Grzanka-Tykwińska, A.; Chudzińska, M.; Podhorecka, M.; Kędziora-Kornatowska, K. Universities of the Third Age yesterday, today and tomorrow. Gerontol. Pol. 2015, 4, 165–168. [Google Scholar]
- Santos, T.R.; Pereira, S.V.M.; Santos, R.L. Intensity of climacteric symptoms in postmenopausal women. Rev. Rede Enferm. Nord. 2016, 17, 225–232. [Google Scholar] [CrossRef]
- McNeil, M. Menopausal Hormone Therapy: Understanding Long-term Risks and Benefits. JAMA 2017, 318, 911–913. [Google Scholar] [CrossRef]
- Genazzani, A.R.; Schneider, H.P.G.; Nijland, E. The European Menopause Survey 2005: What do women think right now about menopause and HRT? Climacteric 2005, 8, 96. [Google Scholar] [CrossRef]
- Vivian-Taylor, J.; Hickey, M. Menopause and depression: Is there a link? Maturitas 2014, 79, 142–146. [Google Scholar] [CrossRef]
- DiBonaventura, M.; Wagner, J.S.; Alvir, J.; Whiteley, J. Depression, Quality of Life, Work Productivity, Resource Use, and Costs among Women Experiencing Menopause and Hot Flashes: A Cross-Sectional Study. Prim. Care Companion CNS Disord. 2012, 14. [Google Scholar] [CrossRef] [Green Version]
- Bromberger, J.T.; Kravitz, H.M. Mood and menopause: Findings from the Study of Women’s Health Across the Nation (SWAN) over 10 years. Obstet. Gynecol. Clin. N. Am. 2011, 38, 609–625. [Google Scholar] [CrossRef] [Green Version]
- Worsley, R.; Bell, R.J.; Gartoulla, P.; Robinson, P.J.; Davis, S.R. Moderate-Severe Vasomotor Symptoms Are Associated with Moderate-Severe Depressive Symptoms. J. Women Health 2017, 26, 712–718. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.J.; Joffe, H.; Bromberger, T.; Thurston, R.C.; Lewis, T.T.; Khalil, N.; Matthews, K.A. Mood symptoms after natural menopause and hysterectomy with and without bilateral oophorectomy among women in midlife. Obstet. Gynecol. 2012, 119, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Conroy, D.E.; Hyde, A.L.; Doerksen, S.E.; Ribeiro, N.F. Implicit attitudes and explicit motivation prospectively predict physical activity. Ann. Behav. Med. 2010, 39, 112–118. [Google Scholar] [CrossRef] [PubMed]
- McArthur, D.; Dumas, A.; Woodend, K.; Beach, S.; Stacey, D. Factors influencing adherence to regular exercise in middle-aged women: A qualitative study to inform clinical practice. BMC Women Health 2014, 14, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skrzypulec, V.; Dąbrowska, J.; Drosdzol, A. The influence of physical activity level on climacteric symptoms in menopausal women. Climacteric 2010, 13, 355–361. [Google Scholar] [CrossRef]
- Freeman, E.W. Associations of depression with the transition to menopause. Menopause 2010, 17, 823–827. [Google Scholar] [CrossRef]
- Cabral, P.U.; Canário, A.C.; Spyrides, M.H.; Uchôa, S.A.; Eleutério Júnior, J.; Giraldo, P.C.; Gonçalves, A.K. Physical activity and sexual function in middle-aged women. Rev. Assoc. Med. Bras. 2014, 60, 47–52. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.J.; Yim, G.; Park, H.Y. Vasomotor and physical menopausal symptoms are associated with sleep quality. PLoS ONE 2018, 13, e0192934. [Google Scholar] [CrossRef]
- Reed, S.D.; Guthrie, K.A.; Newton, K.M.; Anderson, G.L.; Booth-LaForce, C.; Caan, B.; Carpenter, J.S.; Cohen, L.S.; Dunn, A.L.; Ensrud, K.E. Menopausal quality of life: RCT of yoga, exercise, and omega-3 supplements. Am. J. Obstet. Gynecol. 2014, 210, 244.e1–244.e11. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Archana, E.; Pai, A.; Nayak, G.; Shenoy, R.; Anjali, A.R. Serum mineral status and climacteric symptoms in perimanopausal women before and after Yoga therapy, an ongoing study. J. Midlife Health 2013, 4, 225–229. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Group A N (%) | Group B N (%) | X2 | |
|---|---|---|---|---|
| Education | High | 52 (19.05) | 81 (23.28) | 2.95 |
| Secondary | 146 (53.48) | 173 (49.71) | ||
| Primary | 75 (27.47) | 94 (27.01) | ||
| Work | Yes | 141 (51.65) | 156 (44.83) | 2.85 |
| No | 132 (48.35) | 192 (55.17) | ||
| Material Status | High | 48 (17.58) | 51 (14.66) | 8.51 * |
| Medium | 158 (57.88) | 192 (55.17) | ||
| Low | 67 (24.55) | 105 (30.17) | ||
| Marital Status | Married | 220 (80.59) | 260 (74.71) | 3.03 |
| Widowed | 33 (12.09) | 55 (15.80) | ||
| Divorced | 20 (7.33) | 33 (9.48) | ||
| Children | Yes | 212 (77.66) | 222 (63.79) | 14.22 ** |
| No | 61 (22.34) | 126 (36.21) | ||
| Group | Group A | Group B | T-Student |
|---|---|---|---|
| IPAQ Domains | Average ± SD (MET-min/week) | Average ± SD (MET-min/week) | |
| Job-Related | 4780.3 ± 7723.19 | 2464.89 ± 3485.43 | 3.66 ** |
| Housework | 2138.01 ± 2990.12 | 1822.2 ± 3047.27 | 1.29 |
| Transportation | 798.29 ± 2050.6 | 1060.63 ± 2420.41 | 1.43 |
| Leisure Time | 2072.42 ± 2954.84 (60–18,480) | 1984.8 ± 3077.32 (0–18,480) | 2.66 ** |
| Sitting Time | 174.61 ± 138.79 | 197.83 ± 132.14 | 2.12 * |
| Total | 3484.2 ± 4871.38 | 3914.35 ± 5573.89 | 1.01 |
| Group | Climacteric Symptoms | ||||
|---|---|---|---|---|---|
| Lack | Light | Medium | Severe | ||
| Group A | NM N = 244 | 64.81% | 12.96% | 4.81% | 6.67% |
| MHT N = 9 | 2.59% | 0.37% | 0.37% | 0.0 % | |
| PEs N = 20 | 5.19% | 1.85/% | 0.0 % | 0.37% | |
| X2; df; p | 5.18; 6; >0.52 | ||||
| Group B | NM N = 275 | 52.89% | 9.25% | 8.09% | 8.09% |
| MHT N = 30 | 6.65% | 0.58% | 0.87% | 0.58% | |
| PEs N = 43 | 9.25% | 2.31% | 1.16% | 0.29% | |
| X2; df; p | 6.23; 6; >0.39 | ||||
| Symptoms of Depression | IPAQ Level | Group A | Group B | X2 |
|---|---|---|---|---|
| N (%) | N (%) | |||
| Yes | High | 42 (15.61) | 51 (14.70) | 1.63 |
| Moderate | 64 (23.79) | 107 (30.84) | ||
| Low | 11 (4.09) | 19 (5.48) | ||
| No | High | 36 (13.38) | 61 (17.58) | 11.76 * |
| Moderate | 108 (40.15) | 90 (25.94) | ||
| Low | 8 (2.97) | 19 (5.48) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naworska, B.; Brzęk, A.; Bąk-Sosnowska, M. The Relationship between Health Status and Social Activity of Perimenopausal and Postmenopausal Women (Health Status and Social Relationships in Menopause). Int. J. Environ. Res. Public Health 2020, 17, 8388. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228388
Naworska B, Brzęk A, Bąk-Sosnowska M. The Relationship between Health Status and Social Activity of Perimenopausal and Postmenopausal Women (Health Status and Social Relationships in Menopause). International Journal of Environmental Research and Public Health. 2020; 17(22):8388. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228388
Chicago/Turabian StyleNaworska, Beata, Anna Brzęk, and Monika Bąk-Sosnowska. 2020. "The Relationship between Health Status and Social Activity of Perimenopausal and Postmenopausal Women (Health Status and Social Relationships in Menopause)" International Journal of Environmental Research and Public Health 17, no. 22: 8388. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228388