Environmental Characteristics Associated with Older Adults’ Social Participation: The Contribution of Sociodemography and Transportation in Metropolitan, Urban, and Rural Areas




Abstract
:1. Introduction
Social Participation According to Living Area in Quebec
2. Materials and Methods
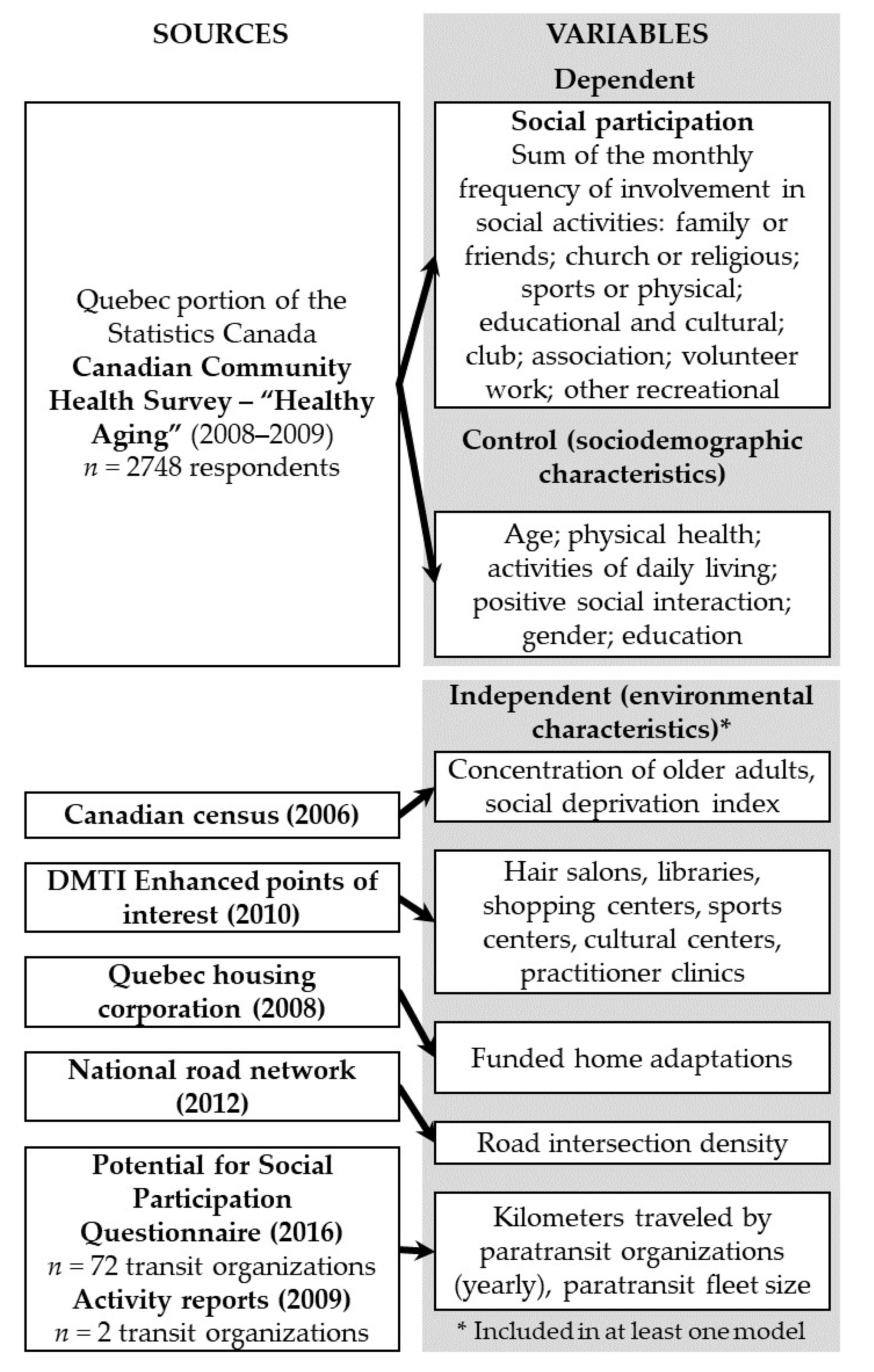
2.1. Design and Participants
2.2. Variables
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Living Area’s Age Composition
4.2. Transportation
4.3. Strengths and Weaknesses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Government of Quebec. Plan D’action 2018–2023 Un Québec Pour tous les Âges [Action Plan 2018–2023 A Quebec for All Ages]; Ministère de la santé et des Services sociaux du Québec: Sainte-Foy, QC, Canada, 2018.
- Statistics Canada. Canadian Survey on Disability; Statistics Canada: Ottawa, ON, Canada, 2012.
- Levasseur, M.; Lefebvre, H.; Levert, M.-J.; Lacasse-Bédard, J.; Desrosiers, J.; Therriault, P.-Y.; Tourigny, A.; Couturier, Y.; Carbonneau, H. Personalized citizen assistance for social participation (APIC): A promising intervention for increasing mobility, accomplishment of social activities and frequency of leisure activities in older adults having disabilities. Arch. Gerontol. Geriatr. 2016, 64, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. World Report on Ageing and Health; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Levasseur, M.; Richard, L.; Gauvin, L.; Raymond, É. Inventory and analysis of definitions of social participation found in the aging literature: Proposed taxonomy of social activities. Soc. Sci. Med. 2010, 71, 2141–2149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lund, R.; Nilsson, C.J.; Avlund, K. Can the higher risk of disability onset among older people who live alone be alleviated by strong social relations? A longitudinal study of non-disabled men and women. Age Ageing 2010, 39, 319–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glass, T.A.; De Leon, C.F.M.; Bassuk, S.S.; Berkman, L.F. Social engagement and depressive symptoms in late life longitudinal findings. J. Aging Health 2006, 18, 604–628. [Google Scholar] [CrossRef]
- Glei, D.A.; A Landau, D.; Goldman, N.; Chuang, Y.-L.; Rodríguez, G.; Weinstein, M. Participating in social activities helps preserve cognitive function: An analysis of a longitudinal, population-based study of the elderly. Int. J. Epidemiol. 2005, 34, 864–871. [Google Scholar] [CrossRef]
- Newall, N.E.G.; McArthur, J.; Menec, V.H. A Longitudinal Examination of Social Participation, Loneliness, and Use of Physician and Hospital Services. J. Aging Health 2014, 27, 500–518. [Google Scholar] [CrossRef]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and Social Isolation as Risk Factors for Mortality A Meta-Analytic Review. Perspect. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef] [Green Version]
- Fougeyrollas, P. La Funambule, le fil et la Toile: Transformations Réciproques du sens du Handicap [The Tightrope Walker, Wire and Canvas. Reciprocal Transformations of the Meaning of Disability]; Presses de l’Université Laval: Sainte-Foy, QC, Canada, 2010. [Google Scholar]
- Bowling, A. Ageing Well: Quality of Life in Old Age; McGraw-Hill Education (UK): London, UK, 2005. [Google Scholar]
- Levasseur, M.; Cohen, A.A.; Dubois, M.-F.; Généreux, M.; Richard, L.; Therrien, F.-H.; Payette, H. Environmental Factors Associated With Social Participation of Older Adults Living in Metropolitan, Urban, and Rural Areas: The NuAge Study. Am. J. Public Health 2015, 105, 1718–1725. [Google Scholar] [CrossRef]
- Pigeon, C.; Boulianne, R.; Levasseur, M. Accompagnement-citoyen personnalisé d’intégration communautaire (APIC) et changements de la mobilité chez des aînés en perte d’autonomie. Rev. Francophone Recherche Ergothér. 2019, 5, 65–86. [Google Scholar]
- Buffel, T.; De Donder, L.; Phillipson, C.; Dury, S.; De Witte, N.; Verté, D. Social participation among older adults living in medium-sized cities in Belgium: The role of neighbourhood perceptions. Health Promot. Int. 2013, 29, 655–668. [Google Scholar] [CrossRef] [PubMed]
- Leyden, K.M. Social Capital and the Built Environment: The Importance of Walkable Neighborhoods. Am. J. Public Health 2003, 93, 1546–1551. [Google Scholar] [CrossRef] [PubMed]
- Bowling, A.; Stafford, M. How do objective and subjective assessments of neighbourhood influence social and physical functioning in older age? Findings from a British survey of ageing. Soc. Sci. Med. 2007, 64, 2533–2549. [Google Scholar] [CrossRef] [PubMed]
- Turcotte, M. Social Engagement and Civic Participation: Are Rural and Small Town Populations Really at an Advantage? Statistics Canada, Agriculture Division: Ottawa, ON, Canada, 2005.
- PPampalon, R.; Hamel, D.; Gamache, P. Recent changes in the geography of social disparities in premature mortality in Québec. Soc. Sci. Med. 2008, 67, 1269–1281. [Google Scholar] [CrossRef] [PubMed]
- Brooke, J.; Jackson, D. Older people and COVID-19: Isolation, risk and ageism. J. Clin. Nurs. 2020, 29, 2044–2046. [Google Scholar] [CrossRef]
- Naud, D.; Généreux, M.; Bruneau, J.-F.; Alauzet, A.; Levasseur, M. Social participation in older women and men: Differences in community activities and barriers according to region and population size in Canada. BMC Public Health 2019, 19, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Therrien, F.-H.; Desrosiers, J. Participation of metropolitan, urban and rural community-dwelling older adults. Arch. Gerontol. Geriatr. 2010, 51, e52–e56. [Google Scholar] [CrossRef]
- Richard, L.; Gauvin, L.; Gosselin, C.; Laforest, S. Staying connected: Neighbourhood correlates of social participation among older adults living in an urban environment in Montreal, Quebec. Health Promot. Int. 2009, 24, 46–57. [Google Scholar] [CrossRef] [Green Version]
- Legh-Jones, H.; Moore, S. Network social capital, social participation, and physical inactivity in an urban adult population. Soc. Sci. Med. 2012, 74, 1362–1367. [Google Scholar] [CrossRef]
- Julien, D.; Gauvin, L.; Richard, L.; Kestens, Y.; Payette, H. The Role of Social Participation and Walking in Depression among Older Adults: Results from the VoisiNuAge Study. Can. J. Aging La Rev. Can. Vieil. 2013, 32, 1–12. [Google Scholar] [CrossRef]
- Richard, L.; Gauvin, L.; Kestens, Y.; Shatenstein, B.; Payette, H.; Daniel, M.; Moore, S.; Levasseur, M.; Mercille, G. Neighborhood Resources and Social Participation Among Older Adults Results From the VoisiNuage Study. J. Aging Health 2013, 25, 296–318. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Census Metropolitan Area and Census Agglomeration Definitions; Statistics Canada: Ottawa, ON, Canada, 2010.
- Levasseur, M.; Naud, D.; Routhier, S.; Généreux, M.; Bruneau, J.-F.; Alauzet, A.; Vanasse, A.; Cohen, A.; Kestens, Y.; Trottier, L.; et al. Caractéristiques environnementales favorisant la participation sociale: Développement d’un outil d’intervention adapté aux particularités de la population québécoise vieillissante. In Rapport de Recherche Présenté au Fonds de Recherche du Québec Société Culture (FRQSC; Actions Concertées # 2015-465); FRQSC: Québec, QC, Canada, 2017. [Google Scholar]
- Naud, D.; Hamel, M.; Caron, M.; Cardin, V.; Roux, M.-H.D.; Levasseur, M. Caractéristiques environnementales favorisant la participation sociale: Une enquête auprès d’aînés québécois. Can. J. Aging 2019, 39, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Levasseur, M.; Généreux, M.; Bruneau, J.-F.; Vanasse, A.; Chabot, É.; Beaulac, C.; Bédard, M.-M. Importance of proximity to resources, social support, transportation and neighborhood security for mobility and social participation in older adults: Results from a scoping study. BMC Public Health 2015, 15, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levasseur, M.; Naud, D.; Routhier, S.; Bruneau, J.-F. Comparaison des caractéristiques des organismes de transport en commun du Québec selon la ruralité: Vers l’identification de nouvelles opportunités pour favoriser la participation sociale des aînés. Popul. Vulnérables 2020, in press. [Google Scholar]
- Kirkland, S.A.; Griffith, L.E.; Menec, V.; Wister, A.; Payette, H.; Wolfson, C.; Raina, P.S. Mining a Unique Canadian Resource: The Canadian Longitudinal Study on Aging. Can. J. Aging 2015, 34, 366–377. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Canadian Community Health Survey (CCHS)-Healthy Aging-User Guide, Health Statistics Division ed.; Statistics Canada: Ottawa, ON, Canada, 2010.
- World Health Organization. International Classification of Functioning, Disability and Health; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Levasseur, M.; Routhier, S.; Naud, D.; Allostry, J.; Généreux, M.; Vanasse, A.; Alauzet, A. Public transit characteristics according to living areas: Toward improving social participation in older adults. In Proceedings of the Entretiens Jacques-Cartier, La mobilité Sous Toutes ses Formes au Service des Collectivités et des Citoyens, Québec, QC, Canada, 16–17 October 2018. [Google Scholar]
- Statistics Canada. Dissemination Area (DA); Statistics Canada: Ottawa, ON, Canada, 2010.
- Levasseur, M.; Gauvin, L.; Richard, L.; Kestens, Y.; Daniel, M.; Payette, H. Associations between perceived proximity to neighborhood resources, disability, and social participation among community-dwelling older adults: Results from the VoisiNuAge Study. Arch. Phys. Med. Rehabil. 2011, 92, 1979–1986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levasseur, M.; Roy, M.; Michallet, B.; St-Hilaire, F.; Maltais, D.; Généreux, M. Associations Between Resilience, Community Belonging, and Social Participation Among Community-Dwelling Older Adults: Results From the Eastern Townships Population Health Survey. Arch. Phys. Med. Rehabil. 2017, 98, 2422–2432. [Google Scholar] [CrossRef]
- Ministère des Transports du Québec. Transport Adapté pour une Meilleure Accessibilité des Services: Révision du Cadre Organisationnel et Financier: Document de Consultation; Ministère des Transports: Québec, QC, Canada, 2003.
- Ministère des Transports du Québec. Politique D’admissibilité au Transport Adapté; Ministère des Transports: Québec, QC, Canada, 1998.
- Hallisey, E.; Tai, E.; Berens, A.; Wilt, G.; Peipins, L.; Lewis, B.; Graham, S.; Flanagan, B.; Lunsford, N.B. Transforming geographic scale: A comparison of combined population and areal weighting to other interpolation methods. Int. J. Health Geogr. 2017, 16, 29. [Google Scholar] [CrossRef] [Green Version]
- Fillenbaum, G.G. OARS Multidimensional Functional Assessment Questionnaire; Springer: New York, NY, USA, 1987. [Google Scholar]
- Sherbourne, C.D.; Stewart, A.L. The MOS social support survey. Soc. Sci. Med. 1991, 32, 705–714. [Google Scholar] [CrossRef]
- Pampalon, R.; Hamel, D.; Gamache, P. Health inequalities in urban and rural Canada: Comparing inequalities in survival according to an individual and area-based deprivation index. Health Place 2010, 16, 416–420. [Google Scholar] [CrossRef]
- Coxe, S.; West, S.G.; Aiken, L.S. The analysis of count data: A gentle introduction to Poisson regression and its alternatives. J. Personal. Assess. 2009, 91, 121–136. [Google Scholar] [CrossRef] [PubMed]
- Hox, J.J.; Moerbeek, M.; Schoot, R.V.D. Multilevel Analysis: Techniques and Applications, 3rd ed.; Routledge: London, UK, 2018; p. 393. [Google Scholar]
- Kianoush, F.; Masoomehni, K. Application REML model and determining cut off of ICC by multi-level model based on Markov Chains simulation in health. Indian J. Fundam. Appl. Life Sci. 2015, 5, 1432–1448. [Google Scholar]
- Louviere, J.J.; Hensher, D.A.; Swait, J.D. Stated Choice Methods: Analysis and Applications; Cambridge University Press: Cambridge, UK, 2000. [Google Scholar]
- Enzmann, D. NB_ADJUST: Stata Module to Identify and Adjust Outliers of a Variable Assumed to Follow a Negative Binomial Distribution; Boston College Department of Economics: Boston, MA, USA, 2015. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 15; StataCorp LP: College Station, TX, USA, 2017. [Google Scholar]
- Institut de la Statistique du Québec. Données Sociales du Québec. Conditions de vie; L’Institut de la Statistique du Québec: Sainte-Foy, QC, Canada, 2009.
- Statistics Canada. Working Seniors in Canada: Census in Brief; Branch, A.S., Ed.; Statistics Canada: Ottawa, ON, Canada, 2017.
- Van Groenou, M.I.B.; Deeg, D.J.H. Formal and informal social participation of the ‘young-old’ in The Netherlands in 1992 and 2002. Ageing Soc. 2010, 30, 445–465. [Google Scholar] [CrossRef]
- Statistics Canada. Retirement Age by Class of Worker, Annual; Canada, S., Ed.; Statistics Canada: Ottawa, ON, Canada, 2018.
- Rijs, K.J.; Cozijnsen, R.; Deeg, D.J.H. The effect of retirement and age at retirement on self-perceived health after three years of follow-up in Dutch 55–64-year-olds. Ageing Soc. 2012, 32, 281–306. [Google Scholar] [CrossRef] [Green Version]
- Galenkamp, H.; Gagliardi, C.; Principi, A.; Golinowska, S.; Moreira, A.; Schmidt, A.E.; Winkelmann, J.; Sowa, A.; Van Der Pas, S.; Deeg, D.J.H. Predictors of social leisure activities in older Europeans with and without multimorbidity. Eur. J. Ageing 2016, 13, 129–143. [Google Scholar] [CrossRef] [Green Version]
- Moulaert, T. Quebec’s Vieillir et vivre ensemble Policy on Ageing: A critical outside analysis. Can. Rev. Soc. Policy 2012, 68/69, 125. [Google Scholar]
- Hunter, B.D.; Neiger, B.; West, J. The importance of addressing social determinants of health at the local level: The case for social capital. Health Soc. Care Community 2011, 19, 522–530. [Google Scholar] [CrossRef]
- Heath, G.W.; Brownson, R.C.; Kruger, J.; Miles, R.; Powell, K.E.; Ramsey, L.T. The Effectiveness of Urban Design and Land Use and Transport Policies and Practices to Increase Physical Activity: A Systematic Review. J. Phys. Act. Heal. 2006, 3, S55–S76. [Google Scholar] [CrossRef]
- Fisher, K.J.; Li, F.; Michael, Y.; Cleveland, M. Neighborhood-Level Influences on Physical Activity among Older Adults: A Multilevel Analysis. J. Aging Phys. Act. 2004, 12, 45–63. [Google Scholar] [CrossRef]
- Moore, S.; Gauvin, L.; Daniel, M.; Kestens, Y.; Böckenholt, U.; Dubé, L.; Richard, L. Associations among Park Use, Age, Social Participation, and Neighborhood Age Composition in Montreal. Leis. Sci. 2010, 32, 318–336. [Google Scholar] [CrossRef]
- Dahan-Oliel, N.; Mazer, B.; Gélinas, I.; Dobbs, B.; Lefebvre, H. Transportation Use in Community-Dwelling Older Adults: Association with Participation and Leisure Activities. Can. J. Aging La Rev. Can. Vieil. 2010, 29, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Fordham, L.; Grisé, E.; Elgeneidy, A.M. When I’m 64: Assessing Generational Differences in Public Transit Use of Seniors in Montreal, Quebec, Canada. Transp. Res. Rec. J. Transp. Res. Board 2017, 2651, 31–41. [Google Scholar] [CrossRef]
- Mercado, R.; Páez, A.; Newbold, K.B. Transport policy and the provision of mobility options in an aging society: A case study of Ontario, Canada. J. Transp. Geogr. 2010, 18, 649–661. [Google Scholar] [CrossRef]
- Burkhardt, J.E. Mobility Changes: Their Nature, Effects, and Meaning for Elders Who Reduce or Cease Driving. Transp. Res. Rec. J. Transp. Res. Board 1999, 1671, 11–18. [Google Scholar] [CrossRef]
- Lord, S.; Cloutier, M.-S.; Garnier, B.; Christoforou, Z. Crossing road intersections in old age—With or without risks? Perceptions of risk and crossing behaviours among the elderly. Transp. Res. Part F Traffic Psychol. Behav. 2018, 55, 282–296. [Google Scholar] [CrossRef]
- Romoser, M.R.E.; Pollatsek, A.; Fisher, D.L.; Williams, C.C. Comparing the glance patterns of older versus younger experienced drivers: Scanning for hazards while approaching and entering the intersection. Transp. Res. Part F Traffic Psychol. Behav. 2013, 16, 104–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turcotte, M. Profile of seniors’ transportation habits. Can. Soc. Trends 2012, 93, 1–16. [Google Scholar]
- Baum, F.; Palmer, C. ‘Opportunity structures’: Urban landscape, social capital and health promotion in Australia. Health Promot. Int. 2002, 17, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Fotheringham, A.S.; Wong, D.W. The modifiable areal unit problem in multivariate statistical analysis. Environ. Plan. A 1991, 23, 1025–1044. [Google Scholar] [CrossRef]
- Turcotte, M. The city/suburb contrast: How canF we measure it. Can. Soc. Trends 2008, 85, 11-008. [Google Scholar]


{kind=link}
| Variable | Quebec n = 2748 | Large Metro n = 1283 | Regular Metro n = 440 | Urban n = 426 | Rural n = 599 | |
|---|---|---|---|---|---|---|
| Continuous Variables | ||||||
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | p-Value 1 | |
| [95% CI] | [95% CI] | [95% CI] | [95% CI] | [95% CI] | ||
| Age (years) | 74.3 (8.8) | 74.5 a (9.1) | 74.6 a (8.9) | 73.5 a (8.8) | 74.0 a (8.1) | 0.18 |
| [74.1, 74.4] | [74.1, 75.0] | [73.8, 75.4] | [72.8, 74.3] | [73.4, 74.6] | ||
| Social participation (number of community activities/month) | 14.9 (17.5) | 14.0 a (18.5) | 14.9 ab (16.1) | 18.4 b (19.7) | 14.0 a (14.4) | <0.01 |
| [14.0; 15.7] | [11.3, 17.4] | [12.0, 18.6] | [14.8; 23.0] | [13.0, 15.2] | ||
| Positive social interaction [0 (low)–16 (high)] | 13.2 (4.7) | 13.0 a (4.9) | 13.3 a (4.9) | 13.5 a (4.4) | 13.5 a (4.4) | 0.13 |
| [13.1, 13.4] | [12.7, 13.3] | [12.9, 13.8] | [13.1, 13.9] | [13.1, 13.9] | ||
| Activities of Daily Living (1 [total]–5 [no impairment]) | 4.7 (0.9) | 4.6 a (1.0) | 4.7 a (0.8) | 4.7 a (0.8) | 4.6 a (0.9) | 0.17 |
| [4.4, 4.9] | [4.6, 4.7] | [4.6, 4.8] | [4.7, 4.8] | [4.6, 4.7] | ||
| Mobility [1 (cannot walk)–6 (no restriction)] | 5.7 (1.1) | 5.7 ab (1.2) | 5.7 a (1.2) | 5.8 ab (0.9) | 5.7 ab (1.0) | <0.05 |
| [5.7, 5.8] | [5.6, 5.7] | [5.6, 5.8] | [5.7, 5.9] | [5.6, 5.8] | ||
| Mental health (0 [poor]–4 [excellent]) | 3.1 (1.2) | 3.1 a (1.2) | 3.2 b (1.1) | 3.0 a (1.2) | 3.0 a (1.1) | <0.05 |
| [3.0, 3.1] | [3.0, 3.2] | [3.1, 3.3] | [2.9, 3.2] | [2.9, 3.1] | ||
| Physical health (0 [poor]–4 [excellent]) | 3.3 (1.3) | 3.4 b (1.4) | 3.2 ab (1.3) | 3.3 ab (1.3) | 3.2 a (1.2) | 0.05 |
| [3.3, 3.4] | [3.3, 3.5] | [3.1, 3.4] | [3.2, 3.5] | [3.1, 3.3] | ||
| Categorical Variables | ||||||
| Percentage | Percentage | Percentage | Percentage | Percentage | p-Value 2 | |
| [95% CI] | [95% CI] | [95% CI] | [95% CI] | [95% CI] | ||
| Homeowner | 66.5 | 60.8 b | 64.2 b | 66.7 ab | 78.6 a | <0.001 |
| [63.1, 69.9] | [55.6, 66.0] | [54.5, 73.9] | [56.6, 76.8] | [73.8, 83.5] | ||
| Income < low income cut-off (yes) | 12.0 | 15.4 | 8.9 | 9.9 | 15.4 | 0.13 |
| [9.9, 14.2] | [8.1, 16.4] | [6.1, 11.8] | [5.8, 14.0] | [10.6, 20.2] | ||
| In a couple | 60.7 | 56.8 b | 62.6 ab | 64.4 ab | 64.6 a | <0.05 |
| [58.4, 63.0] | [53.0, 60.5] | [56.5, 68.7] | [57.7, 71.0] | [60.6, 68.6] | ||
| Retired | 94.2 | 94.0 a | 94.7 a | 94.3 a | 94.2 a | 0.99 |
| [92.8, 95.5] | [91.8, 96.2] | [91.8, 97.6] | [90.8, 97.7] | [91.8, 96.5] | ||
| [Education] No diploma | 54.7 | 52.0 b | 48.2 b | 53.6 b | 64.6 a | 0.001 |
| [51.5, 57.8] | [47.4, 56.6] | [40.5, 56.0] | [46.4, 60.8] | [59.3, 69.8] | ||
| [Education] High school diploma | 10.9 | 12.1 a | 12.5 a | 10.2 a | 7.8 a | 0.17 |
| [9.1, 12.7] | [9.5, 14.8] | [7.5, 17.5] | [6.0, 14.4] | [4.9, 10.8] | ||
| [Education] Postsecondary diploma | 34.5 | 35.9 b | 39.3 b | 36.2 b | 27.6 a | <0.05 |
| [31.9, 37.1] | [31.8, 39.9] | [32.4, 46.1] | [29.3, 43.2] | [23.2, 31.9] | ||
| Has a driver’s license | 71.0 | 63.1 b | 77.0 a | 80.7 a | 76.2 a | <0.001 |
| [68.7, 73.4] | [58.7, 67.5] | [71.7, 82.3] | [76.3, 85.0] | [72.5, 80.0] | ||
| Immigrant | 11.8 | 22.2 b | 3.3 a | 3.2 a | 3.0 a | <0.001 |
| [9.2, 14.4] | [17.5, 26.9] | [1.3, 5.3] | [0.2, 6.2] | [1.2, 4.8] | ||
| Variable | Model 1 (n = 1184) | Model 2 (n = 1097) | ||||
|---|---|---|---|---|---|---|
| exp(b) | exp(b) 95% CI | exp(b) | exp(b) 95% CI | |||
| Concentration of older adults # (vs. Quartile 1 (Q1)) | ||||||
| Q2 | 1.075 | 0.892 | 1.295 | 1.071 | 0.897 | 1.278 |
| Q3 | 1.530 *** | 1.227 | 1.909 | 1.411 ** | 1.129 | 1.765 |
| Q4 | 2.272 *** | 1.600 | 3.226 | 2.172 *** | 1.600 | 2.948 |
| Km traveled by paratransit organizations † (CSD) (vs. Q1) | ||||||
| Q2 | 1.729 *** | 1.330 | 2.246 | 1.744 *** | 1.349 | 2.255 |
| Q3 | 1.514 ** | 1.142 | 2.008 | 1.504 *** | 1.139 | 1.987 |
| Q4 | 1.585 ** | 1.193 | 2.107 | 1.714 *** | 1.286 | 2.285 |
| Hair salons/km2 (DA) (vs. Q1) Q2 | 1.130 | 0.990 | 1.289 | |||
| At least one general practitioner clinic (DA) | 0.698 ** | 0.563 | 0.866 | 0.730 * | 0.574 | 0.930 |
| Funded home adaptations/km2 (CSD) | 1.208 ** | 1.070 | 1.365 | 1.170 * | 1.036 | 1.320 |
| (Funded home adaptations/km2) squared | 0.960 * | 0.929 | 0.991 | 0.972 | 0.940 | 1.005 |
| Age | 1.001 | 0.992 | 1.009 | |||
| Physical health | 1.065 * | 1.002 | 1.131 | |||
| Activities of daily living | 1.213 ** | 1.083 | 1.360 | |||
| Positive social interaction | 1.058 *** | 1.041 | 1.074 | |||
| Man (vs. woman) | 0.905 | 0.784 | 1.046 | |||
| Education (vs. no diploma) | ||||||
| High school diploma | 1.084 | 0.882 | 1.333 | |||
| Postsecondary diploma | 1.135 | 0.989 | 1.301 | |||
| McFadden’s pseudo R2 | 0.011 | 0.025 | ||||
| Prob > F | <0.001 | <0.001 | ||||
| Variable | Model 1 (n = 436) | Model 2 (n = 403) | ||||
|---|---|---|---|---|---|---|
| exp(b) | exp(b) 95% CI | exp(b) | exp(b) 95% CI | |||
| Paratransit fleet size # (CSD) | 1.394 ** | 1.137 | 1.710 | 1.368 * | 1.044 | 1.791 |
| Paratransit fleet size # squared | 0.866 ** | 0.795 | 0.944 | 0.866 * | 0.775 | 0.969 |
| Road intersection density (DA) | 0.835 ** | 0.749 | 0.931 | 0.862 * | 0.756 | 0.982 |
| Age | 0.995 | 0.982 | 1.009 | |||
| Physical health | 0.976 | 0.887 | 1.075 | |||
| Activities of daily living | 1.237 | 0.994 | 1.539 | |||
| Positive social interaction | 1.042 ** | 1.017 | 1.068 | |||
| Man (vs. woman) | 0.921 | 0.772 | 1.100 | |||
| Education (vs. no diploma) | ||||||
| High school diploma | 1.188 | 0.830 | 1.702 | |||
| Postsecondary diploma | 1.050 | 0.894 | 1.234 | |||
| McFadden’s pseudo R2 | 0.002 | 0.015 | ||||
| Prob > F | 0.002 | <0.001 | ||||
| Variable | Model 1 (n = 277) | Model 2 (n = 243) | ||||
|---|---|---|---|---|---|---|
| exp(b) | exp(b) 95% CI | exp(b) | exp(b) 95% CI | |||
| Paratransit fleet size # (CSD) (vs. Q1) | ||||||
| Q2 | 1.443 | 0.902 | 2.309 | 1.333 | 0.798 | 2.228 |
| Q3 | 0.576 *** | 0.483 | 0.686 | 0.862 | 0.607 | 1.225 |
| Q4 | n/a | n/a | ||||
| Paratransit fleet size# x social deprivation index (vs. Q1) | ||||||
| Q2 | 0.471 | 0.187 | 1.188 | 0.355 * | 0.160 | 0.787 |
| Q3 | 0.822 | 0.632 | 1.069 | 0.883 | 0.735 | 1.061 |
| Q4 | n/a | n/a | ||||
| Stores (DA) (vs. Q1) | ||||||
| Q2 | 1.088 | 0.837 | 1.415 | |||
| Q3 | 1.370 * | 1.021 | 1.838 | |||
| Q4 | n/a | n/a | ||||
| Social deprivation index (worst to best) (DA) | 1.204 * | 1.017 | 1.425 | 1.162 * | 1.025 | 1.318 |
| Age | 1.011 | 0.989 | 1.032 | |||
| Physical health | 1.017 | 0.923 | 1.122 | |||
| Activities of daily living | 1.562 *** | 1.232 | 1.981 | |||
| Positive social interaction | 1.042 * | 1.010 | 1.075 | |||
| Man (vs. woman) | 0.737 | 0.537 | 1.012 | |||
| Education (vs. no diploma) | ||||||
| High school diploma | 1.096 | 0.676 | 1.775 | |||
| Postsecondary diploma | 1.444 ** | 1.110 | 1.880 | |||
| McFadden’s pseudo R2 | 0.010 | 0.036 | ||||
| Prob > F | <0.001 | <0.001 | ||||
| Variable | Model 1 (n = 592) | Model 2 (n = 518) | ||||
|---|---|---|---|---|---|---|
| exp(b) | exp(b) 95% CI | exp(b) | exp(b) 95% CI | |||
| Concentration of older adults # (vs. Q1) | ||||||
| Q2 | 2.430 *** | 2.030 | 2.909 | 2.370 *** | 1.700 | 3.304 |
| Q3 | 2.148 *** | 1.884 | 2.448 | 2.386 *** | 1.817 | 3.133 |
| Q4 | n/a | n/a | ||||
| Libraries/km2 (DA) (vs. Q2) Q3 | 0.738 * | 0.581 | 0.939 | 0.707 * | 0.545 | 0.919 |
| At least one leisure resource (DA) (vs. none) | 1.205 * | 1.018 | 1.425 | |||
| At least one shopping center (DA) (vs. none) | 1.535 * | 0.998 | 2.361 | |||
| Age | 1.011 | 0.997 | 1.024 | |||
| Physical health | 1.082 | 0.990 | 1.184 | |||
| Activities of daily living | 1.289 ** | 1.097 | 1.514 | |||
| Positive social interaction | 1.045 *** | 1.021 | 1.069 | |||
| Man (vs. woman) | 0.924 | 0.774 | 1.104 | |||
| Education (vs. no diploma) | ||||||
| High school diploma | 1.517 ** | 1.180 | 1.950 | |||
| Postsecondary diploma | 1.135 | 0.924 | 1.394 | |||
| McFadden’s pseudo R2 | 0.005 | 0.018 | ||||
| Prob > F | <0.001 | <0.001 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levasseur, M.; Naud, D.; Bruneau, J.-F.; Généreux, M. Environmental Characteristics Associated with Older Adults’ Social Participation: The Contribution of Sociodemography and Transportation in Metropolitan, Urban, and Rural Areas. Int. J. Environ. Res. Public Health 2020, 17, 8399. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228399
Levasseur M, Naud D, Bruneau J-F, Généreux M. Environmental Characteristics Associated with Older Adults’ Social Participation: The Contribution of Sociodemography and Transportation in Metropolitan, Urban, and Rural Areas. International Journal of Environmental Research and Public Health. 2020; 17(22):8399. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228399
Chicago/Turabian StyleLevasseur, Mélanie, Daniel Naud, Jean-François Bruneau, and Mélissa Généreux. 2020. "Environmental Characteristics Associated with Older Adults’ Social Participation: The Contribution of Sociodemography and Transportation in Metropolitan, Urban, and Rural Areas" International Journal of Environmental Research and Public Health 17, no. 22: 8399. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228399