Quality of Life in a Cohort of 1078 Women Diagnosed with Breast Cancer in Spain: 7-Year Follow-Up Results in the MCC-Spain Study

 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Health-Related QoL Assessment
2.3. Study Variables
2.4. Statistical Analysis
2.5. Ethics
3. Results
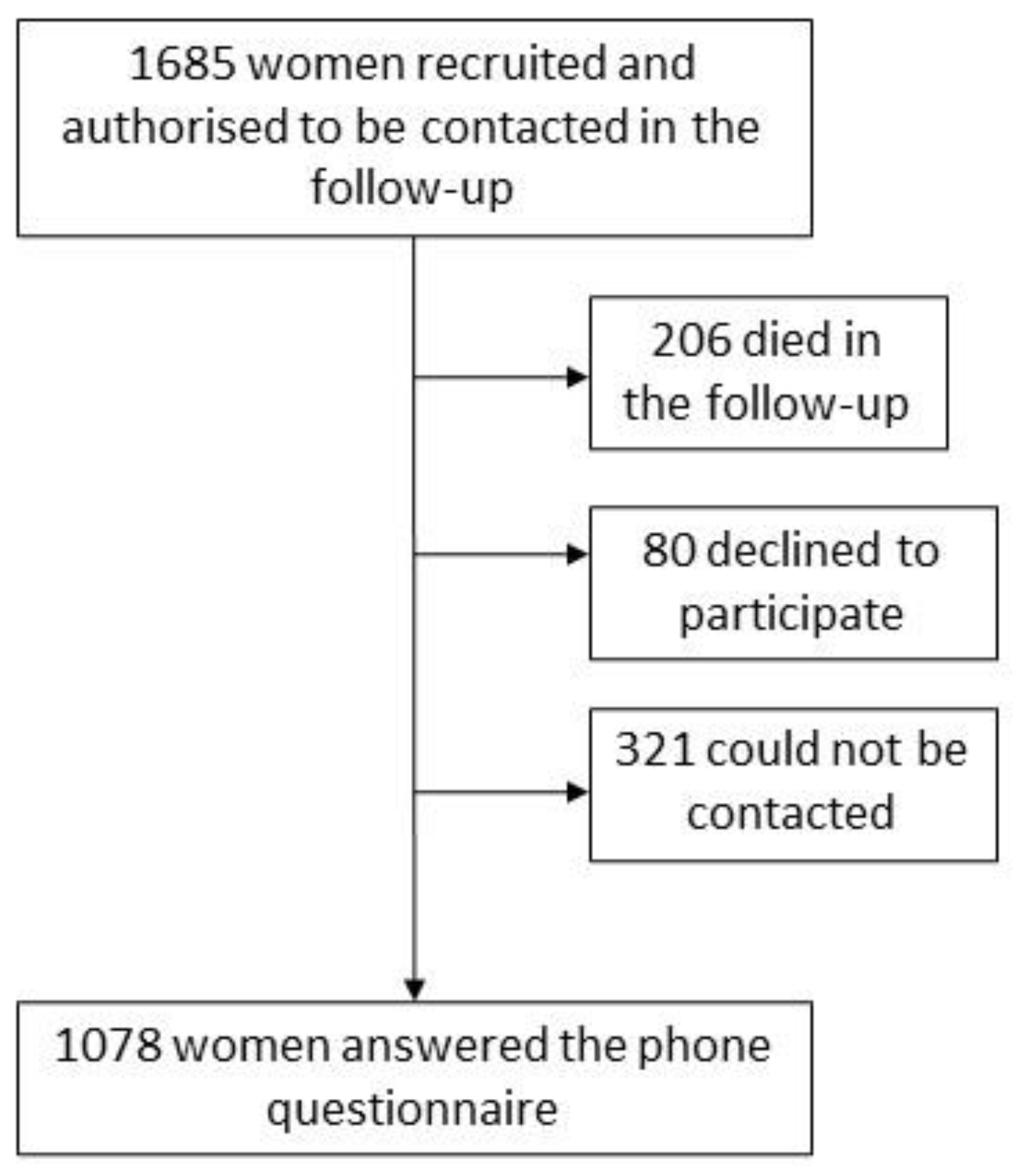
3.1. Recruitment and Response
3.2. General Description about HR-QoL Scores
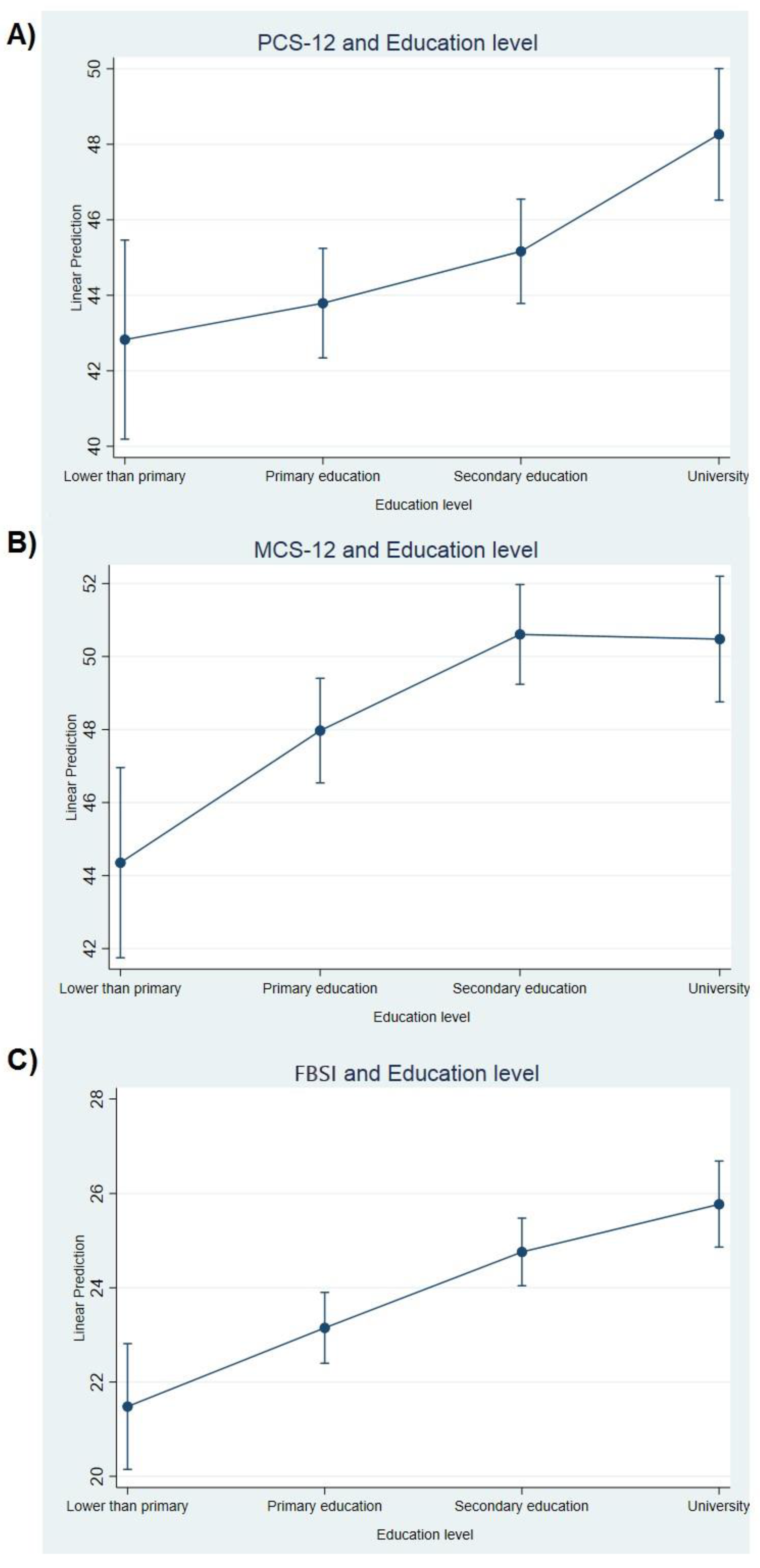
3.3. Socio-Demographic Variables
3.4. Tumor Characteristics
3.5. Treatment Received
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allemani, C.; Weir, H.K.; Carreira, H.; Harewood, R.; Spika, D.; Bannon, F.; Ahn, J.V.; Johnson, C.J.; Bonaventure, A.; Stiller, C.; et al. Global surveillance of cancer survival 1995–2009: Analysis of individual data for 25 676 887 patients from 279 population- based registries in 67 countries (CONCORD-2) Claudia. Lancet 2015, 385, 977–1010. [Google Scholar] [CrossRef] [Green Version]
- Chirlaque, M.D.; Salmerón, D.; Ardanaz, E.; Galceran, J.; Martínez, R.; Marcos-Gragera, R.; Sánchez, M.J.; Mateos, A.; Torrella, A.; Capocaccia, R.; et al. Cancer survival in Spain: Estimate for nine major cancers. Ann. Oncol. 2010, 21, iii21–iii29. [Google Scholar] [CrossRef] [PubMed]
- Guevara, M.; Molinuevo, A.; Salmerón, D.; Marcos-Gragera, R.; Chirlaque, M.D.; Quirós, J.R.; Alemán, A.; Rojas, D.; Sabater, C.; Chico, M.; et al. Supervivencia de cáncer en españa, 2002–2013. Red Esp. Regist. Cáncer 2019. [Google Scholar]
- Alonso-Molero, J.; Molina, A.J.; Jiménez-Moleón, J.J.; Pérez-Gómez, B.; Martin, V.; Moreno, V.; Amiano, P.; Ardanaz, E.; De Sanjose, S.; Salcedo, I.; et al. Cohort profile: The MCC-Spain follow-up on colorectal, breast and prostate cancers: Study design and initial results. BMJ Open 2019, 9, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Chu, W.; Dialla, P.O.; Roignot, P.; Bone-Lepinoy, M.C.; Poillot, M.L.; Coutant, C.; Arveux, P.; Dabakuyo-Yonli, T.S. Determinants of quality of life among long-term breast cancer survivors. Qual. Life Res. 2016, 25, 1981–1990. [Google Scholar] [CrossRef]
- Moro-Valdezate, D.; Buch-Villa, E.; Peiró, S.; Morales-Monsalve, M.D.; Caballero-Gárate, A.; Martínez-Agulló, Á.; Checa-Ayet, F.; Ortega-Serrano, J.; Dolores Morales-Monsalve, M.; Caballero-Gárate, A.; et al. Factors associated with health-related quality of life in a cohort of Spanish breast cancer patients. Breast Cancer 2014, 21, 442–452. [Google Scholar] [CrossRef]
- Syrowatka, A.; Motulsky, A.; Kurteva, S.; Hanley, J.A.; Dixon, W.G.; Meguerditchian, A.N.; Tamblyn, R. Predictors of distress in female breast cancer survivors: A systematic review. Breast Cancer Res. Treat. 2017, 165, 229–245. [Google Scholar] [CrossRef]
- Wang, S.-Y.; Hsu, S.H.; Gross, C.P.; Sanft, T.; Davidoff, A.J.; Ma, X.; Yu, J.B. Association Between Time Since Cancer Diagnosis and Health- Related Quality of Life: A Population-Level Analysis. Value Health 2016, 19, 631–638. [Google Scholar] [CrossRef] [Green Version]
- Hsu, T.; Ennis, M.; Hood, N.; Graham, M.; Goodwin, P.J. Quality of life in long-term breast cancer survivors. J. Clin. Oncol. 2013, 31, 3540–3548. [Google Scholar] [CrossRef]
- Vacek, P.M.; Winstead-Fry, P.; Secker-Walker, R.H.; Hooper, G.J.; Plante, D.A. Factors influencing quality of life in breast cancer survivors. Qual. Life Res. 2003, 12, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Koch, L.; Jansen, L.; Herrmann, A.; Stegmaier, C.; Holleczek, B.; Singer, S.; Brenner, H.; Arndt, V. Quality of life in long-term breast cancer survivors-a 10-year longitudinal population-based study. Acta Oncol. 2013, 52, 1119–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saadatmand, S.; Bretveld, R.; Siesling, S.; Tilanus-Linthorst, M.M.A. Influence of tumour stage at breast cancer detection on survival in modern times: Population based study in 173 797 patients. BMJ 2015, 351, h4901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez-Acebo, I.; Dierssen-Sotos, T.; Palazuelos-Calderón, C.; Pérez-Gómez, B.; Amiano, P.; Guevara, M.; Molina, A.J.A.J.; Domingo, L.; Fernández-Ortiz, M.; Moreno, V.; et al. Tumour characteristics and survivorship in a cohort of breast cancer: The MCC-Spain study. Breast Cancer Res. Treat. 2020, 181, 667–678. [Google Scholar] [CrossRef] [PubMed]
- Castaño-Vinyals, G.; Aragonés, N.; Pérez-Gómez, B.; Martín, V.; Llorca, J.; Moreno, V.; Altzibar, J.M.; Ardanaz, E.; de Sanjosé, S.; Jiménez-Moleón, J.J.; et al. Population-based multicase-control study in common tumors in Spain (MCC-Spain): Rationale and study design. Gac. Sanit. 2015, 29, 308–315. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.; Kosinki, M.; Turner-Bowker, D.; Gandek, B. How to Score Version 2 of the SF-12 Health Survey; Quality Metric. Incorporated: Lincoln, RI, USA, 2004. [Google Scholar]
- Vilagut, G.; Valderas, J.M.; Ferrer, M.; Garin, O.; López-García, E.; Alonso, J. Interpretation of SF-36 and SF-12 questionnaires in Spain: Physical and mental components. Med. Clin. 2008, 130, 726–735. [Google Scholar] [CrossRef] [Green Version]
- Brady, M.J.; Cella, D.F.; Mo, F.; Bonomi, A.E.; Tulsky, D.S.; Lloyd, S.R.; Deasy, S.; Cobleigh, M.; Shiomoto, G. Reliability and validity of the Functional Assessment of Cancer Therapy-Breast quality-of-life instrument. J. Clin. Oncol. Am. Soc. Clin. Oncol. 1997, 15, 974–986. [Google Scholar] [CrossRef]
- Lee, C.F.; Ng, R.; Wong, N.S.; Luo, N.; Yap, Y.S.; Lo, S.K.; Chia, W.K.; Yee, A.; Krishna, L.; Wong, C.; et al. Measurement properties of the eight-item abbreviated functional assessment of cancer therapy—Breast symptom index and comparison with its 37-item parent measure. J. Pain Symptom Manag. 2013, 45, 782–791. [Google Scholar] [CrossRef]
- Cella, D.; Paul, D.; Yount, S.; Winn, R.; Chang, C.H.; Banik, D.; Weeks, J. What are the most important symptom targets when treating advanced cancer? A survey of providers in the National Comprehensive Cancer Network (NCCN). Cancer Investig. 2003, 21, 526–535. [Google Scholar] [CrossRef]
- Garcia, S.F.; Rosenbloom, S.K.; Beaumont, J.L.; Merkel, D.; Von Roenn, J.H.; Rao, D.; Cella, D. Priority symptoms in advanced breast cancer: Development and initial validation of the national comprehensive cancer Network-Functional Assessment of Cancer Therapy-Breast Cancer Symptom Index (NFBSI-16). Value Health 2012, 15, 183–190. [Google Scholar] [CrossRef] [Green Version]
- Alonso, J. IMIM-IMAS CUESTIONARIO DE SALUD SF-12. 2002. Available online: http://www.ser.es/wp-content/uploads/2015/03/SF12_CUESTIONARIO.pdf (accessed on 13 November 2020).
- Martínez, R.B.; Boronat, O.G.; Badía, M.S.; Latiesas, J.S.; Navarro, E.M.; Fores, M.F. Validación de la versión española. Med. Clin. 2011, 137, 685–688. [Google Scholar] [CrossRef]
- Alfonse, M.M.; Aref, M.; Salem, A.-B.M. An Ontology-Based System for Cancer Diseases Knowledge Management. Int. J. Inf. Eng. Electron. Bus. 2014, 6, 55–63. [Google Scholar] [CrossRef]
- Eton, D.T.; Cella, D.; Yost, K.J.; Yount, S.E.; Peterman, A.H.; Neuberg, D.S.; Sledge, G.W.; Wood, W.C. A combination of distribution-and anchor-based approaches determined minimally important differences (MIDs) for four endpoints in a breast cancer scale. J. Clin. Epidemiol. 2004, 57, 898–910. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Schwartz, C.E. Data mining for response shift patterns in multiple sclerosis patients using recursive partitioning tree analysis. Qual. Life Res. 2011, 20, 1543–1553. [Google Scholar] [CrossRef] [PubMed]
- Monteagudo Piqueras, O.; Hernando Arizaleta, L.; Palomar Rodríguez, J.A. Normas poblacionales de referencia de la versión española del SF-12V2 para la Región de Murcia. Gac. Sanit. 2011, 25, 50–61. [Google Scholar] [CrossRef] [Green Version]
- Graells-Sans, A.; Serral, G.; Puigpinós-Riera, R. Social inequalities in quality of life in a cohort of women diagnosed with breast cancer in Barcelona (DAMA Cohort). Cancer Epidemiol. 2018, 54, 38–47. [Google Scholar] [CrossRef]
- Yan, B.; Yang, L.-M.; Hao, L.-P.; Yang, C.; Quan, L.; Wang, L.-H.; Wu, Z.; Li, X.-P.; Gao, Y.-T.; Sun, Q.; et al. Determinants of Quality of Life for Breast Cancer Patients in Shanghai, China. PLoS ONE 2016, 11, e0153714. [Google Scholar] [CrossRef] [Green Version]
- Lu, W.; Cui, Y.; Chen, X.; Zheng, Y.; Gu, K.; Cai, H.; Zheng, W.; Shu, X.O. Changes in quality of life among breast cancer patients three years post-diagnosis. Breast Cancer Res. Treat. 2009, 114, 357–369. [Google Scholar] [CrossRef]
- Neumer, J.M.; Zokoe, N.; McGinley, E.L.E.L.; Pezzin, L.E.L.E.L.E.; Ten, T.W.F.; Schapira, M.M.M.M.; Nattinger, A.B.A.B.; Neuner, J.M.; Zokoe, N.; McGinley, E.L.E.L.; et al. Quality of Life Among a Population-Based Cohort of Older Patients with Breast Cancer. Breast 2014, 23, 609–616. [Google Scholar] [CrossRef]
- Zebrack, B.J.; Jaehee, Y.; Petersen, L.; Gans, P.A. The impact of cancer and quality of life for long-term survivors. Psychooncology 2009, 17, 891–900. [Google Scholar] [CrossRef] [PubMed]
- Mogal, H.D.; Howard-McNatt, M.; Dodson, R.; Fino, N.F.; Clark, C.J. Quality of life of older African American breast cancer survivors: A population-based study. Support. Care Cancer 2017, 25, 1431–1438. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-Y.Y.; Tsai, W.-C.C.; Chou, W.-Y.Y.; Hung, Y.-C.C.; Liu, L.-C.C.; Huang, K.-F.F.; Wang, W.-C.C.; Leung, K.-W.W.; Hsieh, R.-K.K.; Kung, P.-T.T. Quality of life of breast and cervical cancer survivors. BMC Womens Health 2017, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- López-García, E.; Banegas, J.R.; Graciani Pérez-Regadera, A.; Gutiérrez-Fisac, J.L.; Alonso, J.; Rodríguez-Artalejo, F. Valores de referencia de la versión española del Cuestionario de Salud SF-36 en población adulta de más de 60 años. Med. Clin. 2003, 120, 568–573. [Google Scholar] [CrossRef]
- Hawley, S.T.; Janz, N.; Griffith, K.; Jagsi, R.; Friese, C.; Kurian, A.; Hamilton, A.; Ward, K.; Morrow, M.; Wallner, L.; et al. Recurrence Risk Perception and Quality of Life Following Treatment of Breast Cancer. Breast Cancer Res. Treat. 2017, 161, 557–565. [Google Scholar] [CrossRef] [Green Version]
- Dialla, P.O.; Chu, W.O.; Roignot, P.; Bone-Lepinoy, M.C.; Poillot, M.L.; Coutant, C.; Arveux, P.; Dabakuyo-Yonli, T.S. Impact of age-related socio-economic and clinical determinants of quality of life among long-term breast cancer survivors. Maturitas 2015, 81, 362–370. [Google Scholar] [CrossRef]
- Matteo-Ciccone, M.; Aquilino, A.; Cortese, F.; Scicchitano, P.; Sassara, M.; Mola, E.; Rollo, R.; Caldarola, P.; Giorgino, F.; Pomo, V.; et al. Feasibility and effectiveness of a disease and care management model in the primary health care system for patients with heart failure and diabetes (Project Leonardo). Vasc. Health Risk Manag. 2010, 6, 297–305. [Google Scholar] [CrossRef] [Green Version]
- Fann, J.R.; Fan, M.Y.; Unützer, J. Improving primary care for older adults with cancer and depression. J. Gen. Intern. Med. 2009, 24, 417–424. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Socio-Demographic and Clinical Variables | PCS-12 1 | MCS-12 2 | FBSI 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Mean (95% CI) | p-Value | N | Mean (95% CI) | p-Value | N | Mean (95% CI) | p-Value | ||
| Menopausal status | Postmenopausal * | 642 | 45.22 (43.93, 46.51) | 0.92 | 642 | 49.19 (47.92, 50.46) | 0.78 | 663 | 23.92 (23.25, 24.59) | 0.51 |
| Premenopausal | - | 45.10 (43.48, 46.72) | - | - | 48.84 (47.24, 50.44) | - | - | 24.34 (23.50, 25.18) | - | |
| Breast cancer family history | None * | 639 | 45.05 (44.12, 45.99) | 0.82 | 639 | 48.97 (48.05, 49.89) | 0.8 | 660 | 23.86 (23.38, 24.34) | 0.08 |
| First degree | - | 45.16 (43.02, 47.30) | - | - | 48.96 (46.85, 51.08) | - | - | 24.16 (23.05, 25.26) | ||
| Second degree | - | 45.82 (43.59, 48.05) | - | - | 49.78 (47.57, 51.98) | - | - | 25.29 (24.12, 26.45) | - | |
| Educational level | No schooling * | 642 | 42.83 (40.19, 45.46) | <0.001 | 642 | 44.35 (41.75, 46.96) | <0.001 | 663 | 21.48 (20.15, 22.82) | <0.001 |
| Primary education | - | 43.79 (42.34, 45.24) | - | - | 47.97 (46.54, 49.41) | - | - | 23.15 (22.40, 23.90) | - | |
| Secondary education | - | 45.17 (43.78, 46.55) | - | - | 50.61 (49.24, 51.97) | - | - | 24.76 (24.04, 25.48) | - | |
| University | - | 48.26 (46.52, 50.01) | - | - | 50.48 (48.76, 52.20) | - | - | 25.77 (24.86, 26.68) | - | |
| Civil status | Single * | 641 | 44.59 (42.41, 46.78) | 0.95 | 641 | 49.78 (47.61, 51.94) | 0.06 | 662 | 24.45 (23.31, 25.60) | 0.53 |
| Married | - | 45.34 (44.36, 46.31) | - | - | 49.13 (48.16, 50.09) | - | - | 24.02 (23.51, 24.52) | - | |
| Cohabitation | - | 45.23 (42.59, 47.87) | - | - | 45.79 (43.18, 48.40) | - | - | 23.56 (22.19, 24.92) | - | |
| Widowed | - | 45.28 (42.52, 48.04) | - | -- | 50.34 (47.61, 53.07) | - | - | 24.87 (23.43, 26.32) | - | |
| Smoking | Non-smoker at diagnosis * | 642 | 45.40 (44.27, 46.54) | 0.09 | 642 | 49.64 (48.52, 50.76) | 0.05 | 663 | 24.34 (23.75, 24.92) | 0.04 |
| Former smoker at diagnosis | - | 45.91 (44.38, 47.45) | - | - | 49.26 (47.74, 50.78) | - | - | 24.39 (23.58, 25.19) | - | |
| Smoker at diagnosis | - | 43.25 (41.32, 45.19) | - | - | 46.90 (44.99, 48.81) | - | - | 22.92 (21.93, 23.92) | - | |
| Body Mass Index | <18.5 * | 642 | 46.05 (40.35, 51.74) | 0.14 | 642 | 49.35 (43.71, 55.00) | 0.73 | 663 | 25.01 (22.11, 27.91) | 0.17 |
| 18.5–24.9 | - | 46.16 (44.95, 47.37) | - | - | 49.54 (48.34, 50.74) | - | - | 24.54 (23.91, 25.17) | - | |
| 25–29.9 | - | 43.89 (42.47, 45.30) | - | - | 48.46 (47.06, 49.86) | - | - | 23.45 (22.73, 24.18) | - | |
| ≥30 | - | 44.83 (42.89, 46.76) | - | - | 48.78 (46.86, 50.70) | - | - | 24.05 (23.05, 25.06) | - | |
| Age at diagnosis (continuous, per year) | (results are beta (95% CI) instead of marginal means | 642 | −0.11 (−0.19, −0.03) | <0.01 | 642 | 0.05 (−0.03, 0.13) | 0.22 | 663 | 0.03 (−0.01, 0.07) | 0.12 |
| Age at diagnosis | 35–44 * | 642 | 47.30 (45.25, 49.36) | 0.11 | 642 | 47.62 (45.60, 49.65) | 0.38 | 663 | 23.83 (22.75, 24.90) | 0.50 |
| - | 45–54 | - | 45.20 (43.71, 46.68) | - | - | 48.30 (46.84, 49.77) | - | - | 23.61 (22.85, 24.38) | - |
| - | 55–64 | - | 45.34 (43.86, 46.83) | - | - | 50.10 (48.64, 51.57) | - | - | 24.16 (23.39, 24.92) | - |
| - | 65–74 | - | 44.07 (41.96, 46.17) | - | - | 49.22 (47.15, 51.29) | - | - | 24.86 (23.76, 25.95) | - |
| - | ≥75 | - | 40.57 (36.78, 44.36) | - | 49.98 (46.24, 53.72) | - | 25.36 (23.42, 27.31) | - | ||
| Tumor Characteristics | Tumor Characteristics | PCS-12 | MCS-12 | FBSI | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Category | N | Mean (95% CI) | p-Value | N | Mean (95% CI) | p-Value | N | Mean (95% CI) | p-Value | |
| Tumor size | T0 | 619 | 47.19 (37.97, 56.41) | 0.77 | 619 | 48.22 (39.15, 57.29) | 0.10 | 640 | 23.09 (18.25, 27.93) | 0.40 |
| T1 * | - | 44.73 (43.60, 45.85) | - | - | 48.75 (47.64, 49.85) | - | - | 23.77 (23.19, 24.36) | - | |
| T2 | - | 46.27 (44.26, 48.28) | - | - | 50.39 (48.41, 52.37) | - | - | 25.03 (24.00, 26.07) | - | |
| T3 | - | 44.43 (39.65, 49.21) | - | - | 47.06 (42.36, 51.77) | - | - | 23.65 (21.14, 26.16) | - | |
| T4 | - | 45.60 (37.08, 54.11) | - | 39.72 (31.35, 48.10) | - | - | 23.64 (19.47, 27.80) | - | ||
| Node infiltration | N0 | 632 | 45.80 (44.46, 47.15) | 0.65 | 632 | 49.14 (47.81, 50.46) | 0.99 | 652 | 24.36 (23.68, 25.04) | 0.81 |
| N1 * | - | 45.05 (43.24, 46.85) | - | - | 49.15 (47.38, 50.93) | - | - | 23.97 (23.04, 24.90) | - | |
| N2 | - | 41.06 (34.05, 48.07) | - | - | 48.54 (41.65, 55.44) | - | - | 22.79 (19.27, 26.31) | - | |
| N3 | - | 41.31 (32.92, 49.70) | - | - | 49.51 (41.25, 57.77) | - | - | 22.64 (18.35, 26.93) | - | |
| Complete clinical remission | No * | 628 | 45.14 (39.52, 50.76) | 0.99 | 628 | 50.03 (44.47, 55.60) | 0.69 | 649 | 24.31 (21.46, 27.16) | 0.85 |
| Yes | - | 45.13 (44.31, 45.95) | - | - | 48.89 (48.08, 49.70) | - | - | 24.06 (23.63, 24.48) | - | |
| Recurrence | No * | 611 | 45.38 (44.55, 46.21) | 0.01 | 611 | 48.76 (47.94, 49.58) | 0.17 | 631 | 24.16 (23.73, 24.59) | 0.12 |
| Yes | - | 39.92 (35.65, 44.18) | - | - | 51.78 (47.58, 55.98) | - | - | 22.43 (20.28, 24.59) | - | |
| Pathological TNM stage | I * | 642 | 45.53 (44.41, 46.64) | 0.30 | 642 | 48.44 (47.34, 49.54) | 0.40 | 663 | 24.12 (23.54, 24.70) | 0.45 |
| II | - | 44.88 (43.56, 46.20) | - | 49.91 (48.60, 51.21) | - | - | 24.26 (23.58, 24.94) | - | ||
| III | - | 44.90 (42.42, 47.38) | - | - | 49.07 (46.62, 51.52) | - | - | 23.57 (22.28, 24.87) | - | |
| IV | - | 34.61 (22.88, 46.34) | - | - | 46.64 (35.04, 58.23) | - | - | 19.90 (13.72, 26.08) | - | |
| Histological grade | Well differentiated * | 642 | 45.10 (43.64, 46.56) | 0.86 | 642 | 50.76 (49.32, 52.20) | 0.001 | 663 | 24.82 (24.07, 25.57) | 0.07 |
| Moderately differentiated | - | 45.42 (44.15, 46.68) | - | - | 47.32 (46.08, 48.57) | - | - | 23.83 (23.17, 24.48) | - | |
| Poorly differentiated | - | 44.88 (43.34, 46.41) | - | - | 49.63 (48.12, 51.15) | - | - | 23.65 (22.85, 24.46) | - | |
| Intrinsic subtype | Luminal A * | 634 | 44.98 (43.97, 45.99) | 0.72 | 634 | 49.03 (48.04, 50.03) | 0.90 | 655 | 23.98 (23.46, 24.50) | 0.27 |
| Luminal B | - | 45.67 (43.73, 47.60) | - | - | 50.03 (48.12, 51.94) | - | - | 24.30 (23.30, 25.31) | - | |
| Her2 | - | 46.08 (42.15, 50.02) | - | - | 48.37 (44.49, 52.25) | - | - | 25.16 (23.10, 27.22) | - | |
| Basal-like | - | 44.66 (41.35, 47.97) | - | - | 48.04 (44.78, 51.31) | - | - | 23.16 (21.41, 24.92) | - | |
| Luminal ONI ** | - | 48.07 (43.77, 52.38) | - | - | 48.63 (44.39, 52.88) | - | - | 26.27 (24.07, 28.48) | - | |
| Non-luminal ONI ** | - | 41.97 (31.61, 52.32) | - | 49.62 (39.41, 59.83) | - | - | 23.86 (18.45, 29.28) | - | ||
| Treatment | Treatment | PCS-12 | MCS-12 | FBSI | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Category | N | Mean (95% CI) | p-Value | N | Mean (95% CI) | p-Value | N | Mean (95% CI) | p-Value | |
| Immunotherapy | No * | 642 | 45.17 (44.32, 46.01) | 0.99 | 642 | 48.93 (48.10, 49.77) | 0.46 | 663 | 24.05 (23.61, 24.49) | 0.53 |
| Yes | - | 45.16 (42.70, 47.62) | - | - | 49.92 (47.49, 52.34) | - | - | 24.48 (23.19, 25.77) | - | |
| Hormone therapy | No * | 642 | 44.86 (43.20, 46.53) | 0.68 | 642 | 47.90 (46.25, 49.54) | 0.12 | 663 | 23.55 (22.69, 24.42) | 0.16 |
| Yes | - | 45.28 (44.32, 46.25) | - | - | 49.47 (48.52, 50.42) | - | - | 24.30 (23.80, 24.80) | - | |
| Chemotherapy | No * | 642 | 45.06 (43.61, 46.50) | 0.85 | 642 | 48.82 (47.40, 50.25) | 0.72 | 663 | 24.26 (23.51, 25.00) | 0.61 |
| Yes | - | 45.24 (44.13, 46.35) | - | - | 49.18 (48.09, 50.28) | - | - | 23.99 (23.42, 24.57) | - | |
| HER2-targeted therapy | No * | 607 | 44.98 (44.11, 45.85) | 0.53 | 607 | 49.06 (48.21, 49.90) | 0.51 | 627 | 23.96 (23.51, 24.40) | 0.22 |
| Yes | - | 45.88 (43.26, 48.49) | - | - | 49.96 (47.41, 52.50) | - | - | 24.86 (23.51, 26.22) | - | |
| Radiotherapy | No * | 642 | 44.96 (42.91, 47.01) | 0.98 | 642 | 49.09 (47.06, 51.11) | 0.85 | 663 | 23.95 (22.89, 25.02) | 0.91 |
| Yes | - | 45.21 (44.31, 46.11) | - | 48.97 (48.08, 49.86) | - | - | 24.10 (23.64, 24.57) | - | ||
| Surgery | Conservative * | 642 | 45.28 (44.35, 46.21) | 0.64 | 642 | 49.31 (48.39, 50.23) | 0.28 | 663 | 24.08 (23.60, 24.56) | 0.92 |
| Mastectomy | - | 44.81 (43.13, 46.50) | - | - | 48.23 (46.56, 49.89) | - | - | 24.14 (23.26, 25.02) | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso-Molero, J.; Dierssen-Sotos, T.; Gomez-Acebo, I.; Fernandez de Larrea Baz, N.; Guevara, M.; Amiano, P.; Castaño-Vinyals, G.; Fernandez-Villa, T.; Moreno, V.; Bayo, J.; et al. Quality of Life in a Cohort of 1078 Women Diagnosed with Breast Cancer in Spain: 7-Year Follow-Up Results in the MCC-Spain Study. Int. J. Environ. Res. Public Health 2020, 17, 8411. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228411
Alonso-Molero J, Dierssen-Sotos T, Gomez-Acebo I, Fernandez de Larrea Baz N, Guevara M, Amiano P, Castaño-Vinyals G, Fernandez-Villa T, Moreno V, Bayo J, et al. Quality of Life in a Cohort of 1078 Women Diagnosed with Breast Cancer in Spain: 7-Year Follow-Up Results in the MCC-Spain Study. International Journal of Environmental Research and Public Health. 2020; 17(22):8411. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228411
Chicago/Turabian StyleAlonso-Molero, Jéssica, Trinidad Dierssen-Sotos, Ines Gomez-Acebo, Nerea Fernandez de Larrea Baz, Marcela Guevara, Pilar Amiano, Gemma Castaño-Vinyals, Tania Fernandez-Villa, Victor Moreno, Juan Bayo, and et al. 2020. "Quality of Life in a Cohort of 1078 Women Diagnosed with Breast Cancer in Spain: 7-Year Follow-Up Results in the MCC-Spain Study" International Journal of Environmental Research and Public Health 17, no. 22: 8411. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228411