Predicting Postpartum Depressive Symptoms from Pregnancy Biopsychosocial Factors: A Longitudinal Investigation Using Structural Equation Modeling



Abstract
:1. Introduction
2. Materials and Methods
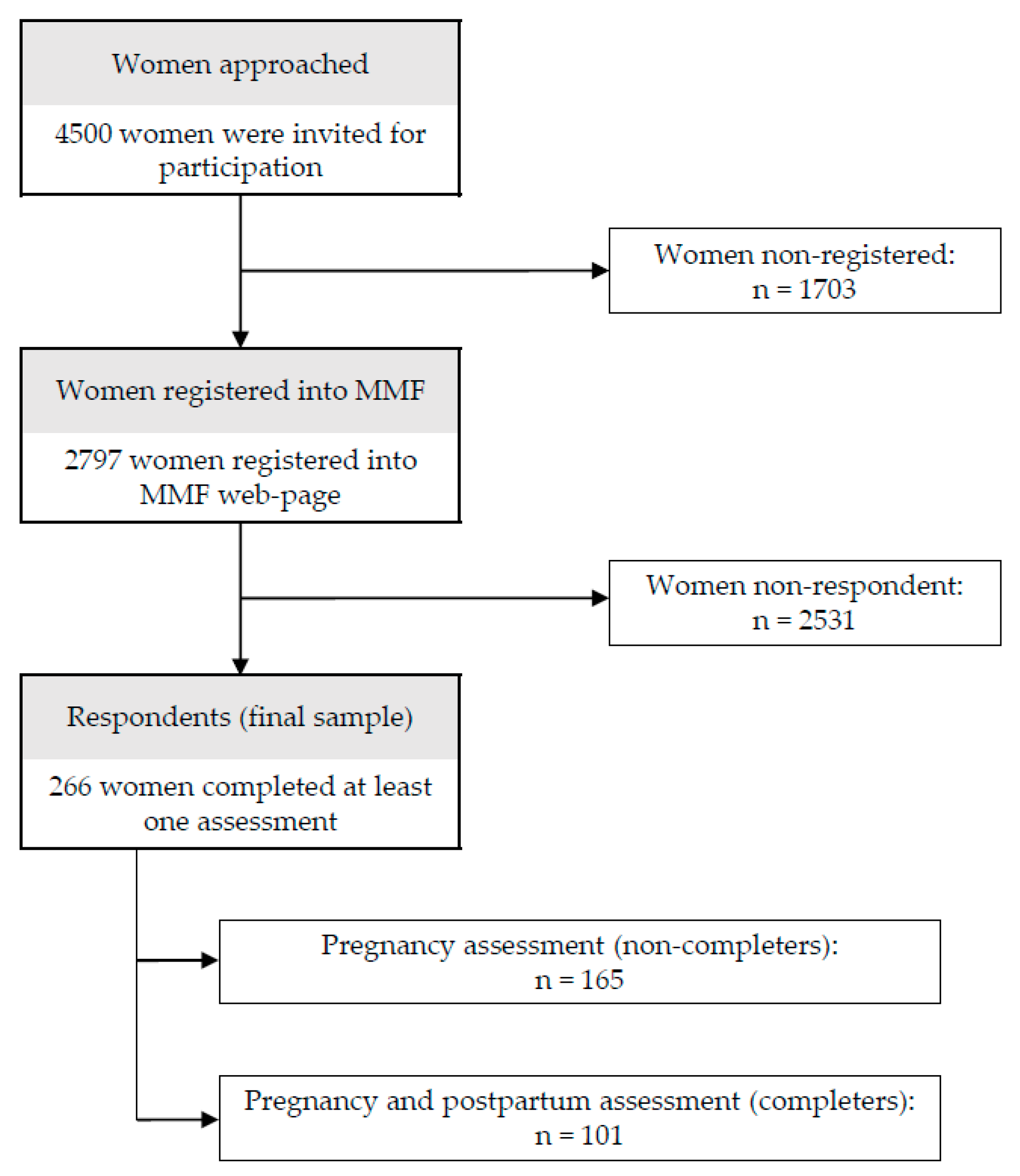
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Demographic and Biologic
2.3.2. Psychological
2.3.3. Social
2.4. Data Analysis
3. Results
3.1. Demographic and Biopsychosocial Characteristics of the Participants: Comparison between Completers and Non-Completers
3.2. Cross-Sectional and Longitudinal Bivariate Associations between Pregnancy Biopsychosocial Factors and Pregnancy and Postpartum Depressive Symptoms in the Sample of Completers
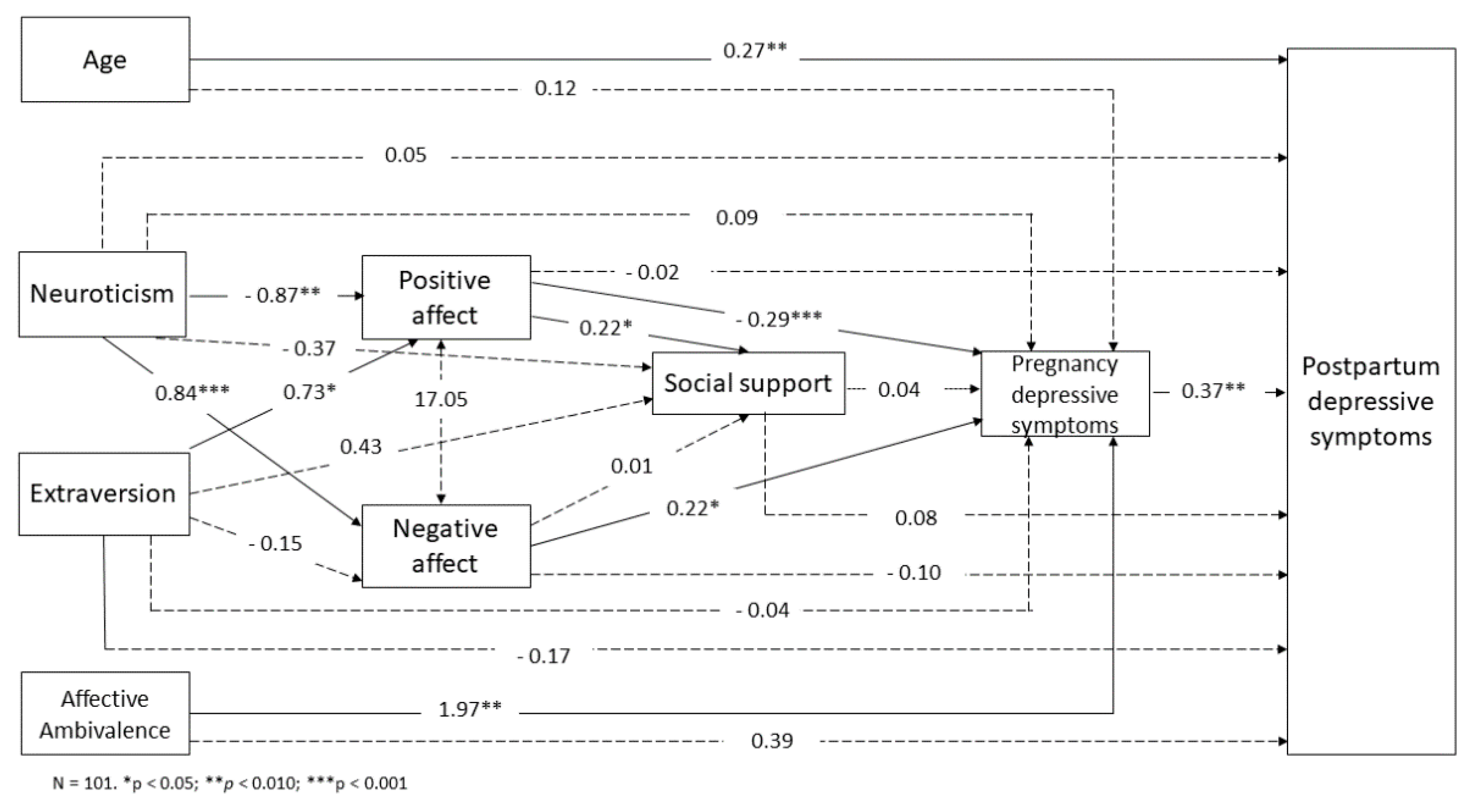
3.3. Structural Equation Model Predicting Postpartum Depressive Symptoms from Prenatal Biopsychosocial Factors in the Sample of Completers
4. Discussion
4.1. Factors Cross-Sectionally Associated with Prenatal Depressive Symptoms
4.2. Factors Predicting Postpartum Depressive Symptoms
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Woody, C.A.; Ferrari, A.J.; Siskind, D.J.; Whiteford, H.A.; Harris, M.G. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J. Affect. Disord. 2017, 219, 86–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Hara, M.; Wisner, K. Perinatal mental illness: Definition, description and aetiology. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Maternal and Child Mental Health. Available online: http://www.who.int/mental_health/maternal-child/maternal_mental_health/en/ (accessed on 17 February 2020).
- Badon, S.E.; Hedderson, M.M.; Hyde, R.J.; Quesenberry, C.P.; Avalos, L.A. Pre- and Early Pregnancy Onset Depression and Subsequent Rate of Gestational Weight Gain. J. Women’s Health 2019, 28, 1237–1245. [Google Scholar] [CrossRef] [PubMed]
- Danaher, B.G.; Milgrom, J.; Seeley, J.R.; Stuart, S.; Schembri, C.; Tyler, M.S.; Ericksen, J.; Lester, W.; Gemmill, A.W.; Kosty, D.B.; et al. MomMoodBooster web-based intervention for postpartum depression: Feasibility trial results. J. Med. Internet Res. 2013, 15, e242. [Google Scholar] [CrossRef]
- Byatt, N.; Carter, D.; Deligiannidis, K.M.; Epperson, C.N.; Meltzer-Brody, S.; Payne, J.L.; Robinson, G.; Silver, N.E.; Stowe, Z.; Van Niel, M.S.; et al. Position Statement on Screening and Treatment of Mood and Anxiety Disorders During Pregnancy and Postpartum. APA Off. Actions 2018. Available online: https://www.psychiatry.org/File%20Library/About-APA/Organization-Documents-Policies/Policies/Position-Screening-and-Treatment-Mood-Anxiety-Disorders-During-Pregnancy-Postpartum.pdf (accessed on 14 November 2020).
- Milgrom, J.; Martin, P.; Negri, L. Treating Postnatal Depression: A Psychological Approach for Health Care Practicionaers; John Wiley & Sons, Ltd.: Chichester, UK, 1999. [Google Scholar]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef] [Green Version]
- Norhayati, M.N.; Nik Hazlina, N.H.; Asrenee, A.R.; Wan Emilin, W.M.A. Magnitude and risk factors for postpartum symptoms: A literature review. J. Affect. Disord. 2015, 175, 34–52. [Google Scholar] [CrossRef] [Green Version]
- Chatillon, O.; Even, C. Antepartum depression: Prevalence, diagnosis and treatment. Encephale 2010, 36, 443–451. [Google Scholar] [CrossRef]
- Peñacoba-Puente, C.; Marín-Morales, D.; Carmona-Monge, F.J.; Velasco Furlong, L. Post-Partum Depression, Personality, and Cognitive-Emotional Factors: A Longitudinal Study on Spanish Pregnant Women. Health Care Women Int. 2016, 37, 97–117. [Google Scholar] [CrossRef]
- Bos, S.C.; Macedo, A.; Marques, M.; Pereira, A.T.; Maia, B.R.; Soares, M.J.; Valente, J.; Gomes, A.A.; Azevedo, M.H. Is positive affect in pregnancy protective of postpartum depression? Rev. Bras. Psiquiatr. 2013, 35, 5–12. [Google Scholar] [CrossRef] [Green Version]
- Míguez, C.; Fernández, V.; Pereira, B. Depresión postparto y factores asociados en mujeres con embarazos de riesgo 1. Behav. Psychol./Psicol. Conduct. 2017, 25, 47–64. [Google Scholar]
- Hetherington, E.; McDonald, S.; Williamson, T.; Patten, S.B.; Tough, S.C. Social support and maternal mental health at 4 months and 1 year postpartum: Analysis from the All Our Families cohort. J. Epidemiol. Community Health 2018, 72, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Yim, I.S.; Tanner Stapleton, L.R.; Guardino, C.M.; Hahn-Holbrook, J.; Dunkel Schetter, C. Biological and psychosocial predictors of postpartum depression: Systematic review and call for integration. Annu. Rev. Clin. Psychol. 2015, 11, 99–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adamu, A.F.; Adinew, Y.M. Domestic Violence as a Risk Factor for Postpartum Depression Among Ethiopian Women: Facility Based Study. Clin. Pract. Epidemiol. Ment. Health 2018, 14, 109–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, M.; Brain, U.; Grunau, R.; Diamond, A.; Oberlander, T. Maternal depression trajectories from pregnancy to 3 years postpartum are associated with children’s behavior and executive functions at 3 and 6 years. Arch. Womens. Ment. Health 2018, 21, 353–363. [Google Scholar] [CrossRef]
- Lara, M.A.; Navarrete, L.; Nieto, L.; Berenzon, S. Acceptability and barriers to treatment for perinatal depression. An exploratory study in Mexican women. Salud Ment. 2014, 37, 293–301. [Google Scholar] [CrossRef] [Green Version]
- Clout, D.; Brown, R. Sociodemographic, pregnancy, obstetric, and postnatal predictors of postpartum stress, anxiety and depression in new mothers. J. Affect. Disord. 2015, 188, 60–67. [Google Scholar] [CrossRef]
- Bennett, H.A.; Einarson, A.; Taddio, A.; Koren, G.; Einarson, T.R. Prevalence of depression during pregnancy: Systematic review. Obstet. Gynecol. 2004, 103, 698–709. [Google Scholar] [CrossRef]
- Takehara, K.; Tachibana, Y.; Yoshida, K.; Mori, R.; Kakee, N.; Kubo, T. Prevalence trends of pre- and postnatal depression in Japanese women: A population-based longitudinal study. J. Affect. Disord. 2018, 225, 389–394. [Google Scholar] [CrossRef]
- Qandil, S.; Jabr, S.; Wagler, S.; Collin, S.M. Postpartum depression in the Occupied Palestinian Territory: A longitudinal study in Bethlehem. BMC Pregnancy Childbirth 2016, 16, 375. [Google Scholar] [CrossRef] [Green Version]
- Harris, R. A Primer of Multivariate Statistics, 3rd ed.; LEA: Mahwah, NJ, USA, 2001. [Google Scholar]
- Harrell, F. Regression Modeling Strategies: With Applications to Linear Models, Logistic Regression, and Survival Analysis; Springer: New York, NY, USA, 2001. [Google Scholar]
- Beck, A.; Steer, R.; Brown, G. Manual for the Beck Depression Inventory-II.; Psychological Corporation: San Antonio, TX, USA, 1996; ISBN 0158018389. [Google Scholar]
- Sanz, J.; Perdigón, A.; Vázquez, C. Adaptación Española del inventario para la depresión de Beck-II (BDI-II): 2. Propiedades psicométricas en población general. Clínica y Salud 2003, 14, 249–280. [Google Scholar]
- Sanz, J.; Gutiérrez, S.; Gesteira, C.; García-Vera, M. Criteria and norms for interpreting the Beck Depression Inventory-II (BDI-II). Behav. Psychol. Psicol. Conduct. 2014, 22, 37–59. [Google Scholar]
- Sandín, B.; Chorot, P.; Lostao, L.; Joiner, T.; Santed, M.; Valiente, R. Escalas PANAS de afecto positivo y negativo: Validación factorial y convergencia transcultural. Psicothema 1999, 11, 37–51. [Google Scholar]
- Watson, D.; Clark, L.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Eysenck, H.; Eysenck, S. Manual of Eysenck Personality Questionnaire; Hodder & Stoughton: London, UK, 1975. [Google Scholar]
- Ortet, G.; Ibáñez, M.; Moro, M.; Silva, F. Cuestionario Revisado de Personalidad de Eysenck: Versiones Completa (EPQ-R) y Abreviada (EPQ-RS); TEA Ediciones: Madrid, Spain, 2001. [Google Scholar]
- Landeta, O.; Calvete, E. Adaptación y validación de la escala multidimensional de apoyo social percibido. Ansiedad y Estrés 2002, 8, 173–182. [Google Scholar]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Pers. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Hooper, D.; Coughlan, J.; Mullen, M. Structural equation modelling: Guidelines for determining model fit. Electron. J. Bus. Res. Methods 2008, 6, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Cupani, M. Análisis de Ecuaciones Estructurales: Conceptos, etapas de desarrollo y un ejemplo de aplicación. Tesis 2012, 1, 186–199. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- DiStefano, C.; Morgan, G.B. A Comparison of Diagonal Weighted Least Squares Robust Estimation Techniques for Ordinal Data. Struct. Equ. Model. Multidiscip. J. 2014, 21, 425–438. [Google Scholar] [CrossRef]
- Rubin, M. Do p values lose their meaning in exploratory analyses? It depends how you define the familywise error rate. Rev. Gen. Psychol. 2017, 21, 269–275. [Google Scholar] [CrossRef] [Green Version]
- Beck, C. Predictors of postpartum depression: An update. Nurs. Res. 2001, 50, 275–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strelow, B.; Fellows, N.; Fink, S.R.; O’Laughlin, D.J.; Radke, G.; Stevens, J.; Tweedy, J.M. Postpartum depression in older women. J. Am. Acad. Physician Assist. 2018, 31, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Moeller, S.B.; Lars Kessing, P.B.; Mortensen, E.L. A Psychometric Validation Analysis of Eysenck’s Neuroticism and Extraversion Scales in a Sample of First Time Depressed Patients. J. Depress. Anxiety 2015, 4, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Guardino, C.M.; Dunkel-Schetter, C. Coping during pregnancy: A systematic review and recommendations. Health Psychol. Rev. 2014, 8, 70–94. [Google Scholar] [CrossRef] [Green Version]
- Milgrom, J.; Hirshler, Y.; Reece, J.; Charlene, C.H.; Gemmill Alan, A.W. Social support—A protective factor for depressed perinatal women? Int. J. Environ. Res. Public Health 2019, 16, 1426. [Google Scholar] [CrossRef] [Green Version]
- Doraiswamy, S.; Jithesh, A.; Chaabane, S.; Abraham, A.; Chaabna, K.; Cheema, S. Perinatal mental illness in the middle east and North Africa region—A systematic overview. Int. J. Environ. Res. Public Health 2020, 17, 5487. [Google Scholar] [CrossRef]
- Leahy-Warren, P.; Newham, J.; Alderdice, F. Perinatal social support: Panacea or a pitfall. J. Reprod. Infant Psychol. 2018, 36, 219–221. [Google Scholar] [CrossRef]
- Saeed Abbasi, I.; Rattan, N.; Kousar, T.; Khalifa Elsayed, F. Neuroticism and Close Relationships: How Negative Affect is Linked with Relationship Disaffection in Couples. Am. J. Fam. Ther. 2018, 46, 139–152. [Google Scholar] [CrossRef]
- Hain, S.; Oddo-Sommerfeld, S.; Bahlmann, F.; Louwen, F.; Schermelleh-Engel, K. Risk and protective factors for antepartum and postpartum depression: A prospective study. J. Psychosom. Obstet. Gynecol. 2016, 37, 119–129. [Google Scholar] [CrossRef]
- Maloni, J.A.; Przeworski, A.; Damato, E.G. Web recruitment and internet use and preferences reported by women with postpartum depression after pregnancy complications. Arch. Psychiatr. Nurs. 2013, 27, 90–95. [Google Scholar] [CrossRef]
- O’Neill, P.; Cycon, A.; Friedman, L. Seeking social support and postpartum depression: A pilot retrospective study of perceived changes. Midwifery 2019, 71, 56–62. [Google Scholar] [CrossRef] [PubMed]
- McMahon, C.A.; Boivin, J.; Gibson, F.L.; Hammarberg, K.; Wynter, K.; Fisher, J.R.W. Older maternal age and major depressive episodes in the first two years after birth: Findings from the Parental Age and Transition to Parenthood Australia (PATPA) study. J. Affect. Disord. 2015, 175, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Nassar, A.H.; Usta, I.M. Advanced Maternal Age. Part II: Long-Term Consequences. Am. J. Perinatol. 2009, 26, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Lara-Cinisomo, S.; Clark, C.T.; Wood, J. Increasing Diagnosis and Treatment of Perinatal Depression in Latinas and African American Women: Addressing Stigma Is Not Enough. Women’s Health Issues 2018, 28, 201–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parvin, S.; Sakineh, N.; Seyed, M.; Bahram, G.; Hashem, A. Comparing postpartum stressors and social support level in primiparous and multiparous women. J. Midwifery Reprod. Health 2014, 2, 71–77. [Google Scholar]
- Hung, C.H. The psychosocial consequences for primiparas and multiparas. Kaohsiung J. Med. Sci. 2007, 23, 352–360. [Google Scholar] [CrossRef] [Green Version]
- Donker, T.; Cuijpers, P.; Stanley, D.; Danaher, B. The Future of Perinatal Depression Identification Can Information and Communication Technology Optimize Effectiveness? In Identifying Perinatal Depression and Anxiety: Evidence-Based Practice in Screening, Psychosocial Assessment, and Management; Wiley-Blackwell: Oxford, UK, 2015; pp. 240–255. ISBN 978-1-118-50969-2. [Google Scholar]
- Martínez-Borba, V.; Suso-ribera, C.; Osma, J. The Use of Information and Communication Technologies in Perinatal Depression Screening: A Systematic Review. Cyberpsychol. Behav. Soc. Netw. 2018, 21, 741–752. [Google Scholar] [CrossRef] [Green Version]
- Suso-Ribera, C.; Castilla, D.; Zaragozá, I.; Ribera-Canudas, M.V.; Botella, C.; García-Palacios, A. Validity, reliability, feasibility, and usefulness of Pain Monitor. A multidimensional smartphone app for daily monitoring of adults with heterogeneous chronic pain. Clin. J. Pain 2018, 34, 900–908. [Google Scholar] [CrossRef]
- Čuržik, D.; Nataša Begić, J. The utility of BDI-II in assessment of pre-and postpartum depression symptoms and their relation to labor pain. Psychiatr. Danub. 2012, 24, 167–174. [Google Scholar]
- Carvalho Bos, S.; Pereira, A.T.; Marques, M.; Maia, B.; Soares, M.J.; Valente, J.; Gomes, A.; Macedo, A.; Azevedo, M.H. The BDI-II factor structure in pregnancy and postpartum: Two or three factors? Eur. Psychiatry 2009, 24, 334–340. [Google Scholar] [CrossRef]
- Darius Tandon, S.; Cluxton-Keller, F.; Leis, J.; Le, H.-N.; Perry, D.F. A comparison of three screening tools to identify perinatal depression among low-income African American women. J. Affect. Disord. 2012, 136, 155–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, D.; Gay, C.; Torres, R.; Lee, K. Shortening day length: A potential risk factor for perinatal depression. J. Behav. Med. 2018, 41, 690–702. [Google Scholar] [CrossRef] [PubMed]
- Barlow, D.H.; Farchione, T.J.; Fairholme, C.P.; Ellard, K.K.; Boisseau, C.L.; Allen, L.B.; Ehrenreich-May, J.; Fairholme, C.P.; Farchione, T.J.; Boisseau, C.L.; et al. Unified Protocol for Transdiagnostic Treatment of Emotional Disorders: Therapist Guide; Treatments that work; Oxford University Press: New York, NY, USA, 2011; ISBN 978-0-19-977266-7. (Paperback). [Google Scholar]
- Crespo-Delgado, E.; Martínez-Borba, V.; Osma, J. The Unified Protocol for Transdiagnostic Treatment of Perinatal Depression: A Case Study. Clin. Case Stud. 2020, 19, 491–508. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inclusion | Exclusion |
|---|---|
| Being pregnant (weeks 16 to 36) | Not being able to read and answer questions in Spanish |
| Over 18 years of age | |
| Having internet access | |
| Signing the informed consent form |
| Variable | Non-Completers | Completers | Comparison | |||
|---|---|---|---|---|---|---|
| Mean (SD; Range) | N | Mean (SD; Range) | N | U | p | |
| Age | 32.59 (4.39; 18–42) | 165 | 33.54 (3.88; 23–42) | 101 | 7474.00 | 0.157 |
| Affective Ambivalence | 0.93 (0.73; 0–3) | 165 | 0.86 (0.74; 0–3) | 101 | ||
| No | 26.1% | 43 | 30.7% | 31 | 7869.00 | 0.390 |
| Yes | 73.9% | 122 | 69.3% | 70 | ||
| Neuroticism | 3.77(3.43; 0–12) | 165 | 3.69 (2.99; 0–12) | 101 | 8191.00 | 0.815 |
| Extraversion | 8.10 (2.93; 0–12) | 165 | 8.54 (2.67; 1–12) | 101 | 7678.00 | 0.279 |
| Positive Affect | 29.70 (9.78; 0–50) | 139 | 29.68 (8.92; 0–50) | 101 | 6735.00 | 0.592 |
| Negative Affect | 16.50 (7.00; 0–40) | 139 | 15.88 (5.82; 0–32) | 101 | 6754.40 | 0.617 |
| Social Support | 75.13 (10.92; 12–84) | 123 | 76.97 (7.84; 42–82) | 101 | 5927.00 | 0.551 |
| Pregnancy Depressive Symptoms | 11.37 (7.40; 2–33) | 134 | 10.21 (5.49; 1–26) | 101 | 6499.50 | 0.603 |
| Minimal | 73.9% | 99 | 72.3% | 73 | 3446.00 | 0.602 |
| Mild | 11.2% | 15 | 23.7% | 24 | 169.50 | 0.765 |
| Moderate | 9.7% | 13 | 4% | 4 | 21.00 | 0.563 |
| Severe | 5.2% | 7 | 0 | |||
| Postpartum Depressive Symptoms | 8.54 (5.53; 0–25) | 101 | ||||
| Minimal | 82.2% | 83 | ||||
| Mild | 14.8% | 15 | ||||
| Moderate | 3% | 3 | ||||
| Severe | 0 | |||||
| Variable | Non-Completers | Completers | Comparison | |
|---|---|---|---|---|
| Frequency (%) | Frequency (%) | χ2 | p | |
| Nationality | ||||
| Spanish | 154 (93.3) | 94 (93.1) | 0.07 | 0.934 |
| Other | 11 (6.7) | 7 (6.9) | ||
| Educational Level | ||||
| <12 years | 23 (13.9) | 15 (14.9) | 0.04 | 0.837 |
| >12 years | 142 (86.1) | 86 (85.1) | ||
| Parity | ||||
| Primiparous | 122 (73.9) | 79 (78.2) | 0.62 | 0.429 |
| Multiparous | 43 (26.1) | 22 (21.8) | ||
| Relationship Status | ||||
| Not in a Relationship | 42 (25.5) | 17 (16.8) | 2.70 | 0.100 |
| In a Relationship | 123 (74.5) | 84 (83.2) | ||
| Variable | Age | AM | N | E | PA | NA | SS | PRE Dep | POST Dep |
|---|---|---|---|---|---|---|---|---|---|
| Age | - | 0.14 | 0.17 | −0.8 | −0.15 | 0.13 | −0.18 | 0.21 * | 0.27 ** |
| AM | - | 0.26 ** | −0.01 | −0.13 | 0.29 ** | −0.17 | 0.38 *** | 0.20 * | |
| N | - | −0.21 * | −0.38 *** | 0.49 *** | −0.26 ** | 0.34 *** | 0.16 | ||
| E | - | 0.28 ** | −0.05 | 0.23 * | −0.15 | −0.18 | |||
| PA | - | −0.17 | 0.34 *** | −0.49 *** | −0.21 * | ||||
| NA | - | −0.03 | 0.36 *** | 0.10 | |||||
| SS | - | −0.16 | −0.10 | ||||||
| PRE Dep | - | 0.47 *** | |||||||
| POST Dep | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Borba, V.; Suso-Ribera, C.; Osma, J.; Andreu-Pejó, L. Predicting Postpartum Depressive Symptoms from Pregnancy Biopsychosocial Factors: A Longitudinal Investigation Using Structural Equation Modeling. Int. J. Environ. Res. Public Health 2020, 17, 8445. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228445
Martínez-Borba V, Suso-Ribera C, Osma J, Andreu-Pejó L. Predicting Postpartum Depressive Symptoms from Pregnancy Biopsychosocial Factors: A Longitudinal Investigation Using Structural Equation Modeling. International Journal of Environmental Research and Public Health. 2020; 17(22):8445. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228445
Chicago/Turabian StyleMartínez-Borba, Verónica, Carlos Suso-Ribera, Jorge Osma, and Laura Andreu-Pejó. 2020. "Predicting Postpartum Depressive Symptoms from Pregnancy Biopsychosocial Factors: A Longitudinal Investigation Using Structural Equation Modeling" International Journal of Environmental Research and Public Health 17, no. 22: 8445. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228445