Predictive Factors on the Incidence of Heart Failure in Patients with Ischemic Heart Disease: Using a 10-Year Population-Based Korea National Health Insurance Cohort Data


Abstract
:1. Introduction
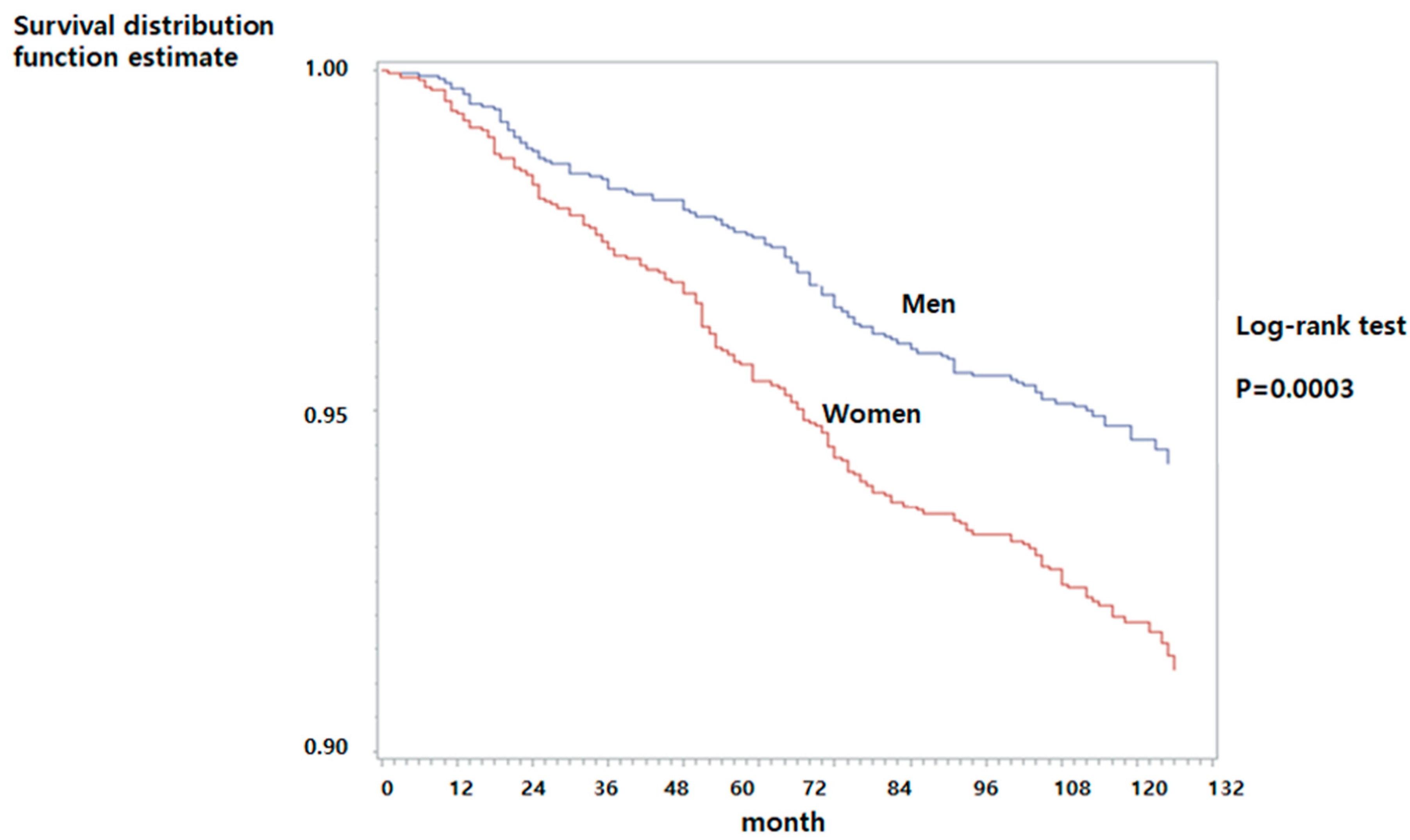
- To examine the incidence rate of HF among patients with IHD by gender for 10 years.
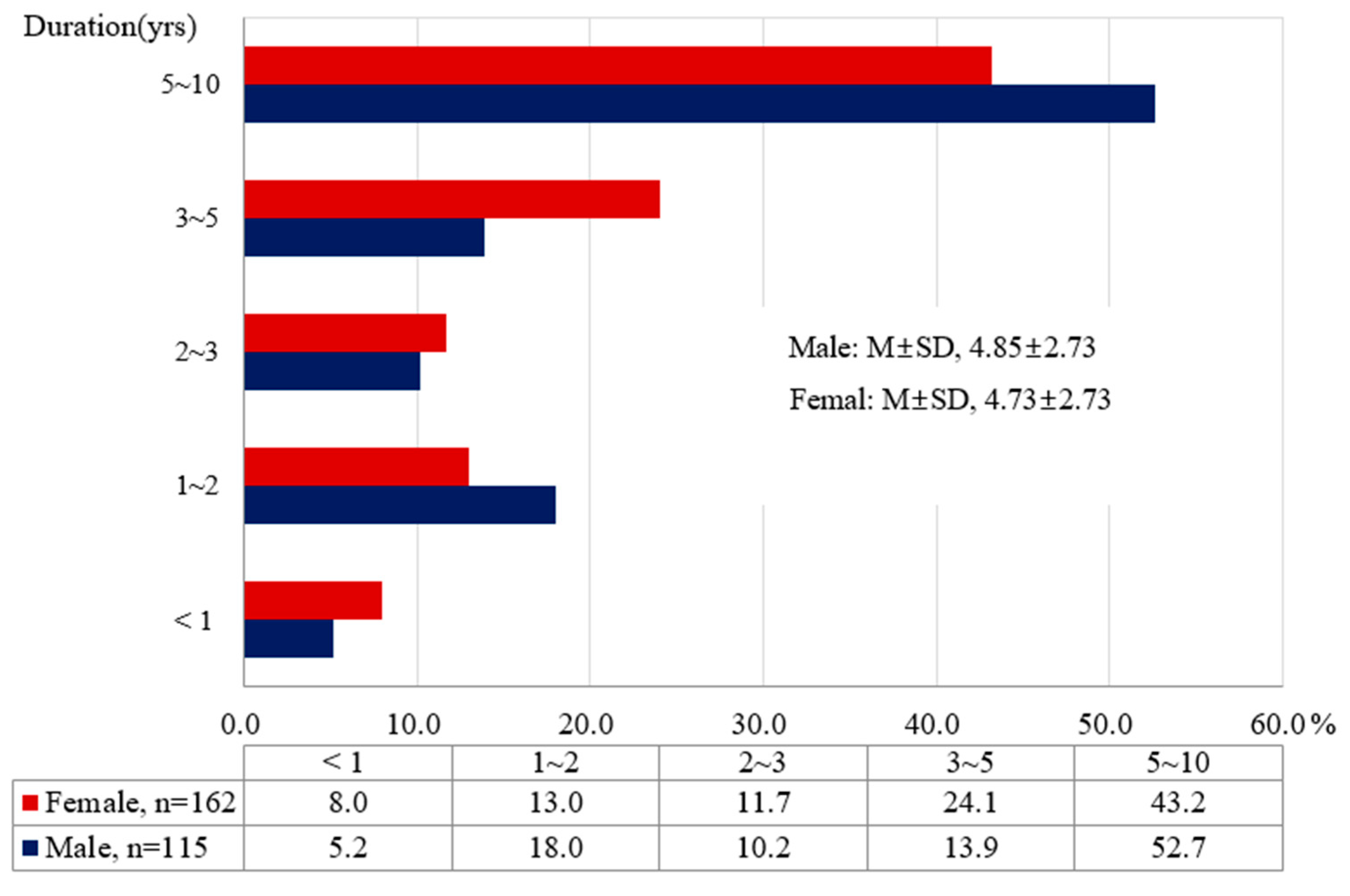
- To examine duration of transition to HF from IHD patients.
- To determine predicting factors affecting the development of HF after the treatment of IHD by gender.
2. Materials and Methods
2.1. Research Design
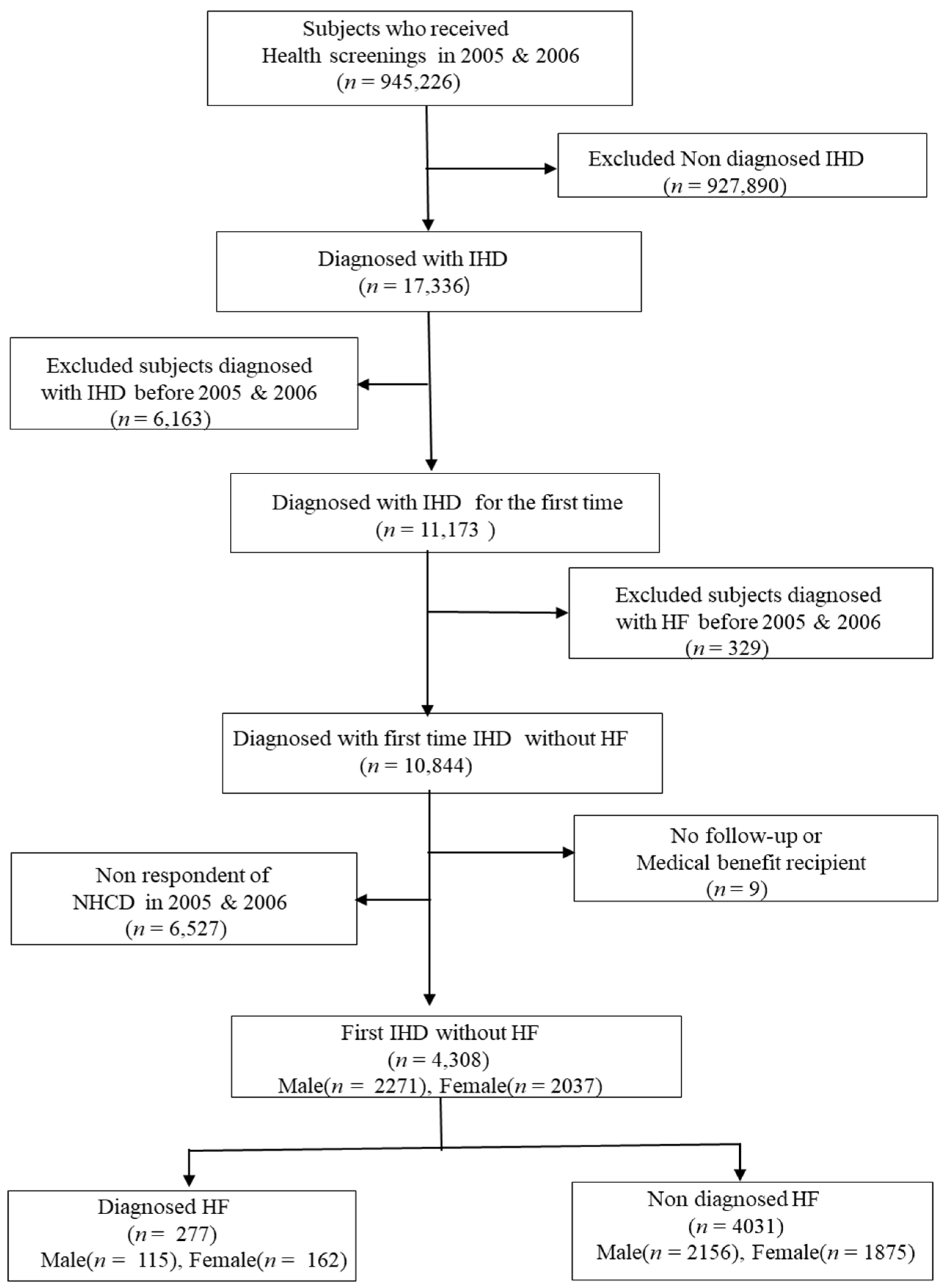
2.2. Study Participants and Data Collection
2.3. Ethical Consideration
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of the Subjects
3.2. Predictive Factors for the Incidence of HF in Men and Women
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Heidenreich, P.A.; Albert, N.M.; Allen, L.A.; Bluemke, D.A.; Butler, J.; Fonarow, G.C.; Ikonomidis, J.S.; Khavjou, O.; Konstam, M.A.; Maddox, T.M.; et al. American Heart Association Advocacy Coordinating Committee; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Radiology and Intervention; Council on Clinical Cardiology; Council on Epidemiology and Prevention; Stroke Council. Forecasting the impact of heart failure in the United States: A policy statement from the American Heart Association. Circ. Heart Fail. 2013, 6, 606–619. [Google Scholar] [PubMed] [Green Version]
- Cook, C.; Cole, G.; Asaria, P.; Jabbour, R.; Francis, D.P. The annual global economic burden of heart failure. Int. J. Cardiol. 2014, 171, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Cahill, T.J.; Kharbanda, R.K. Heart failure after myocardial infarction in the era of primary percutaneous coronary intervention: Mechanisms, incidence and identification of patients at risk. World J. Cardiol. 2017, 9, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Ambrosy, A.P.; Fonarow, G.C.; Butler, J.; Chioncel, O.; Greene, S.E.; Vaduganathan, M.; Nodari, S.; Lam, C.S.P.; Sato, N.; Shah, A.N.; et al. The global health and economic burden of hospitalizations for heart failure: Lessons learned from hospitalized heart failure registries. J. Am. Coll. Cardiol. 2014, 63, 1123–1133. [Google Scholar] [CrossRef]
- Farmakis, D.; Parissis, J.; Lekakis, J.; Filippatos, G. Acute heart failure: Epidemiology, risk factors, and prevention. Rev. Esp. Cardiol. 2015, 68, 245–248. [Google Scholar] [CrossRef]
- Lee, H.; Oh, S.H.; Cho, H.; Cho, H.; Kang, H.Y. Prevalence and socio-economic burden of heart failure in an aging society of South Korea. BMC Cardiovasc. Disord. 2016, 16, 215. [Google Scholar] [CrossRef] [Green Version]
- Gerber, Y.; Weston, S.A.; Enriquez-Sarano, M.; Manemann, S.M.; Chamberlain, A.M.; Jiang, R.; Roger, V.L. Atherosclerotic burden and heart failure after myocardial infarction. JAMA Cardiol. 2016, 1, 156–162. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.E.; Lee, H.Y.; Cho, H.J.; Choe, W.S.; Kim, H.; Choi, J.O.; Jeon, E.S.; Kim, M.S.; Kim, J.J.; Hwang, K.K.; et al. Clinical characteristics and outcome of acute heart failure in Korea: Results from the Korean Acute Heart Failure Registry (KorAHF). Korean Circ. J. 2017, 47, 341–353. [Google Scholar] [CrossRef] [Green Version]
- National Health Insurance Service. 2018 Sample Cohort Database. Available online: https://nhiss.nhis.or.kr/bd/ab/bdaba016lv.do (accessed on 28 January 2018).
- National Health Insurance Service. 2016 National Health Insurance Statistical Year Book; National Health Insurance, Health Insurance Review & Assessment Service: Seoul, Korea, 2016. [Google Scholar]
- National Health Insurance Service. National Health Insurance Sharing Service, 2015 Sample Cohort DB User Manual. Available online: https://nhiss.nhis.or.kr/bd/ab/bdaba002cv.do# (accessed on 5 May 2018).
- Triposkiadis, F.; Xanthopoulos, A.; Butler, J. Cardiovascular aging and heart failure: JACC review topic of the week. J. Am. Coll. Cardiol. 2019, 74, 804–813. [Google Scholar] [CrossRef]
- Song, P.S.; Ryu, D.R.; Kim, M.J.; Jeon, K.H.; Choi, R.K.; Park, J.S.; Song, Y.B.; Hahn, J.Y.; Gwon, H.C.; Ahn, Y.; et al. Korea Acute Myocardial Infarction Registry Investigators. Risk scoring system to assess outcomes in patients treated with contemporary guideline-adherent optimal therapies after acute myocardial infarction. Korean Circ. J. 2018, 48, 492–504. [Google Scholar] [CrossRef]
- Desta, L.; Jernberg, T.; Spaak, J.; Hofman-Bang, J.; Persson, H. Risk and predictors of readmission for heart failure following a myocardial infarction between 2004 and 2013: A Swedish nationwide observational study. Int. J. Cardiol. 2017, 248, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Chen, O.; Donahue, C.; Wang, B.; Fang, Y.; Donnino, R.; Natarajan, S. Impact of diabetes on heart failure incidence in adults with ischemic heart disease. J. Diabetes Complicat. 2017, 31, 1597–1601. [Google Scholar] [CrossRef] [PubMed]
- Dei Cas, A.; Khan, S.S.; Butler, J.; Mentz, R.J.; Bonow, R.O.; Avogaro, A.; Tschoepe, D.; Doehner, W.; Greene, S.J.; Senni, M.; et al. Impact of diabetes on epidemiology, treatment, and outcomes of patients with heart failure. JACC Heart Fail. 2015, 3, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Newman, J.D.; Schwartzbard, A.Z.; Weintraub, H.S.; Goldberg, I.J.; Berger, J.S. Primary prevention of cardiovascular disease in diabetes mellitus. J. Am. Coll. Cardiol. 2017, 70, 883–893. [Google Scholar] [CrossRef] [PubMed]
- Boonman-de Winter, L.J.; Rutten, F.H.; Cramer, M.J.; Landman, M.J.; Liem, A.H.; Rutten, G.E.; Hoes, A.W. High prevalence of previously unknown heart failure and left ventricular dysfunction in patients with type 2 diabetes. Diabetologia 2012, 55, 2154–2162. [Google Scholar] [CrossRef] [Green Version]
- Matsushita, K.; Blecker, S.; Pazin-Filho, A.; Bertoni, A.; Chang, P.P.; Coresh, J.; Selvin, E. The association of hemoglobin a1c with incident heart failure among people without diabetes: The atherosclerosis risk in communities study. Diabetes 2010, 59, 2020–2026. [Google Scholar] [CrossRef] [Green Version]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar]
- Tousoulis, D.; Oikonomou, E.; Siasos, G.; Stefanadis, C. Diabetes mellitus and heart failure. Eur. Cardiol. Rev. 2014, 9, 37–42. [Google Scholar] [CrossRef]
- McMurray, J.J.; Adamopoulos, S.; Anker, S.D.; Auricchio, A.; Böhm, M.; Dickstein, K.; Falk, V.; Filippatos, G.; Fonseca, C.; Gomez-Sanchez, M.A.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The task force for the diagnosis and treatment of acute and chronic heart failure 2012 of the European Society of Cardiology. Eur. J. Heart Fail. 2012, 4, 803–869. [Google Scholar]
- Andersson, C.; Norgaard, M.L.; Hansen, P.R.; Fosbølet, E.L.; Schmiegelow, M.; Weeke, P.; Olesen, J.B.; Raunsø, J.; Jørgensen, C.H.; Vaag, A.; et al. Heart failure severity, as determined by loop diuretic dosages, predicts the risk of developing diabetes after myocardial infarction: A nationwide cohort study. Eur. J. Heart Fail. 2010, 12, 1333–1338. [Google Scholar] [CrossRef]
- Lim, N.K.; Lee, S.E.; Lee, H.Y.; Cho, H.J.; Choe, W.S.; Kim, H.; Choi, J.O.; Jeon, E.S.; Kim, M.S.; Kim, J.J.; et al. Risk prediction for 30 days heart failure-specific readmission or death after discharge: Data from the Korean Acute Heart Failure (KorAHF) registry. J. Cardiol. 2019, 73, 108–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goel, S.; Sharma, A.; Garg, A. Effect of alcohol consumption on cardiovascular health. Curr. Cardiol. Rep. 2018, 20, 19. [Google Scholar] [CrossRef] [PubMed]
- Ejlersen, H.; Andersen, Z.J.; von Euler-Chelpin, M.C.; Johansen, P.P.; Schnohr, P.; Prescott, E. Prognostic impact of physical activity prior to myocardial infarction: Case fatality and subsequent risk of heart failure and death. Eur. J. Prev. Cardiol. 2017, 24, 1112–1119. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Men (n = 2271) | p | Women (n = 2037) | p | ||
|---|---|---|---|---|---|---|
| No HF (n = 2156, %) | HF (n = 115, %) | No HF (n = 1875, %) | HF (n = 162, %) | |||
| Age, yr M ± SD | 54.1 ± 12.7 | <0.001 | 58.4 ± 11.1 | <0.001 | ||
| 30–39 | 306 (14.2) | 1 (0.8) | 83 (4.4) | 0 (0.0) | ||
| 40–49 | 532 (24.7) | 11 (9.7) | 344 (18.4) | 5 (3.1) | ||
| 50–59 | 585 (27.1) | 30 (26.0) | 593 (31.6) | 33 (20.4) | ||
| 60–69 | 494 (22.9) | 43 (37.4) | 585 (31.2) | 64 (39.5) | ||
| 70–85 | 239 (11.1) | 30 (26.1) | 270 (14.4) | 60 (37.0) | ||
| Household income * (M = 2235, F = 2014) | 0.912 | 0.594 | ||||
| Low (1–2 decile) | 242 (11.4) | 14 (12.2) | 324 (17.5) | 32 (19.7) | ||
| Middle (3–8 decile) | 1113 (52.5) | 62 (53.9) | 929 (50.2) | 74 (45.7) | ||
| High (9–10 decile) | 766 (36.1) | 39 (33.9) | 600 (32.3) | 56 (34.6) | ||
| Body Mass Index | 0.021 | 0.119 | ||||
| Normal < 23 Kg/m2 | 626 (29.0) | 47 (40.9) | 637 (34.0) | 45 (27.7) | ||
| Overweight < 23–25 Kg/m2 | 577 (26.8) | 23 (20.0) | 532 (28.4) | 44 (27.2) | ||
| Obesity ≥ 25 Kg/m2 | 953 (44.2) | 45 (39.1) | 705 (37.6) | 73 (45.1) | ||
| Hypertension, yes | 388 (20.0) | 31 (27.0) | 0.016 | 467 (24.9) | 63 (38.9) | <0.001 |
| Diabetes, yes | 142 (6.6) | 19 (16.5) | <0.001 | 126 (6.7) | 27 (16.7) | <0.001 |
| Family history of stroke, yes | 21 (5.6) | 4 (3.5) | 0.336 | 116 (6.2) | 7 (4.3) | 0.348 |
| Total cholesterol ≥ 240 mg/dL | 243 (11.3) | 17 (14.8) | 0.253 | 309 (16.5) | 29 (17.9) | 0.618 |
| Alcohol drinking (M = 2224, F = 1978) | 0.027 | 0.228 | ||||
| No or Seldom | 933 (44.2) | 63 (56.3) | 1585 (87.0) | 143 (91.7) | ||
| Moderate (1–2 times/week) | 854 (40.4) | 32 (28.6) | 210 (11.5) | 12 (7.7) | ||
| Severe (>3 times/week) | 325 (15.4) | 17 (15.1) | 27 (1.5) | 1 (0.6) | ||
| Smoking (M = 2213, F = 1952) | 0.733 | 0.624 | ||||
| Never | 1081 (51.4) | 61 (54.4) | 1734 (96.5) | 148 (95.5) | ||
| Ex-smoker | 365 (17.4) | 20 (17.8) | 16 (8.9) | 1 (0.6) | ||
| Current smoker | 655 (31.2) | 31 (27.8) | 47 (2.6) | 6 (3.9) | ||
| Exercise (M = 2197, F = 1965) | 0.009 | 0.006 | ||||
| Seldom (No or hardly ever) | 985 (47.2) | 66 (60.0) | 1098 (60.6) | 110 (71.9) | ||
| Regular (≥1 time/ week) | 1102 (52.8) | 44 (40.0) | 714 (39.4) | 43 (28.1) | ||
| Variables | Male (n = 2271) No HF (n = 2156) vs. HF (n = 115) | Female (n = 2037) No HF (n = 1915) vs. HF (n = 162) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | p | HR | 95% CI | β | SE | p | HR | 95% CI | |
| Age, yr (ref: 30–39) | ||||||||||
| 40–49 | −0.04 | 0.07 | 0.587 | 0.96 | 0.85–1.10 | 0.25 | 0.13 | 0.054 | 1.29 | 0.95–0.99 |
| 50–59 | −0.04 | 0.07 | 0.594 | 0.96 | 0.91–1.13 | 0.18 | 0.13 | 0.154 | 1.20 | 0.82–0.93 |
| 60–69 | 0.06 | 0.08 | 0.404 | 1.07 | 0.68–1.05 | 0.17 | 0.13 | 0.202 | 1.18 | 0.75–0.81 |
| 70–85 | 0.38 | 0.09 | <0.001 | 1.46 | 1.31–1.55 | 0.36 | 0.14 | <0.001 | 1.44 | 1.05–1.45 |
| Body Mass Index, kg/m2 (ref: <23) | ||||||||||
| 23–25 | −0.03 | 0.06 | 0.601 | 0.97 | 0.91–1.35 | −0.11 | 0.06 | 0.085 | 0.90 | 0.91–0.98 |
| ≥25 | −0.02 | 0.05 | 0.763 | 0.98 | 0.83–1.05 | −0.09 | 0.06 | 0.151 | 0.92 | 0.68–0.82 |
| Hypertension (ref: No) | ||||||||||
| Yes | −0.24 | 0.06 | <0.001 | 0.78 | 1.15–1.48 | −0.14 | 0.06 | 0.025 | 0.87 | 1.09–1.78 |
| Diabetes (ref: No) | ||||||||||
| Yes | 0.21 | 0.09 | 0.021 | 1.23 | 1.06–1.35 | 0.08 | 0.10 | 0.380 | 1.09 | 0.78–0.85 |
| Exercise (ref: Regular) | ||||||||||
| Seldom | −0.04 | 0.04 | 0.302 | 0.95 | 0.80–1.15 | −0.08 | 0.05 | 0.102 | 0.92 | 0.68–0.88 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, S.Y.; Kim, K.A.; Choi, O.J. Predictive Factors on the Incidence of Heart Failure in Patients with Ischemic Heart Disease: Using a 10-Year Population-Based Korea National Health Insurance Cohort Data. Int. J. Environ. Res. Public Health 2020, 17, 8670. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228670
Hwang SY, Kim KA, Choi OJ. Predictive Factors on the Incidence of Heart Failure in Patients with Ischemic Heart Disease: Using a 10-Year Population-Based Korea National Health Insurance Cohort Data. International Journal of Environmental Research and Public Health. 2020; 17(22):8670. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228670
Chicago/Turabian StyleHwang, Seon Young, Kyung Ae Kim, and Oh Jong Choi. 2020. "Predictive Factors on the Incidence of Heart Failure in Patients with Ischemic Heart Disease: Using a 10-Year Population-Based Korea National Health Insurance Cohort Data" International Journal of Environmental Research and Public Health 17, no. 22: 8670. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228670