Timing of Spheno-Occipital Synchondrosis Ossification in Children and Adolescents with Cleft Lip and Palate: A Retrospective Case-Control Study


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design and Registration
2.2. Selection and Description of Participants
2.3. Methods
- In the axial view, by positioning the vertical plane in the middle of the anterior border of the foramen magnum (Figure 1A).
- In the frontal view, by leveling the horizontal plane with the palatal plane (Figure 1B).
- A mid-sagittal section of the skull base, passing through the middle of the sella turcica (Figure 2A,B) and the anterior border of the foramen magnum (Figure 2C,D), was considered as the view of choice to assess the SOS. The full extent of the synchondral cartilage was then observed in search of bone bridges. This method increased the total amount of information collected by the 3D exam.
2.4. Statistical Analysis
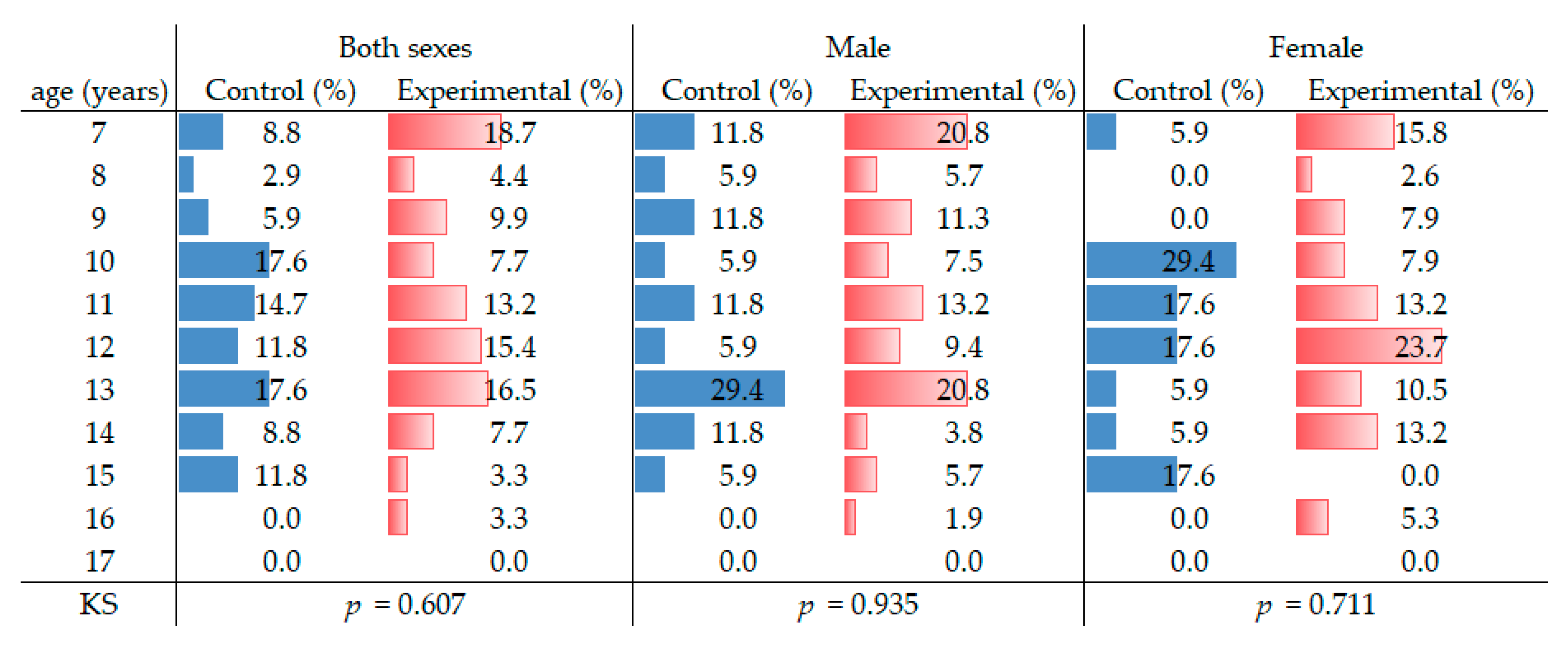
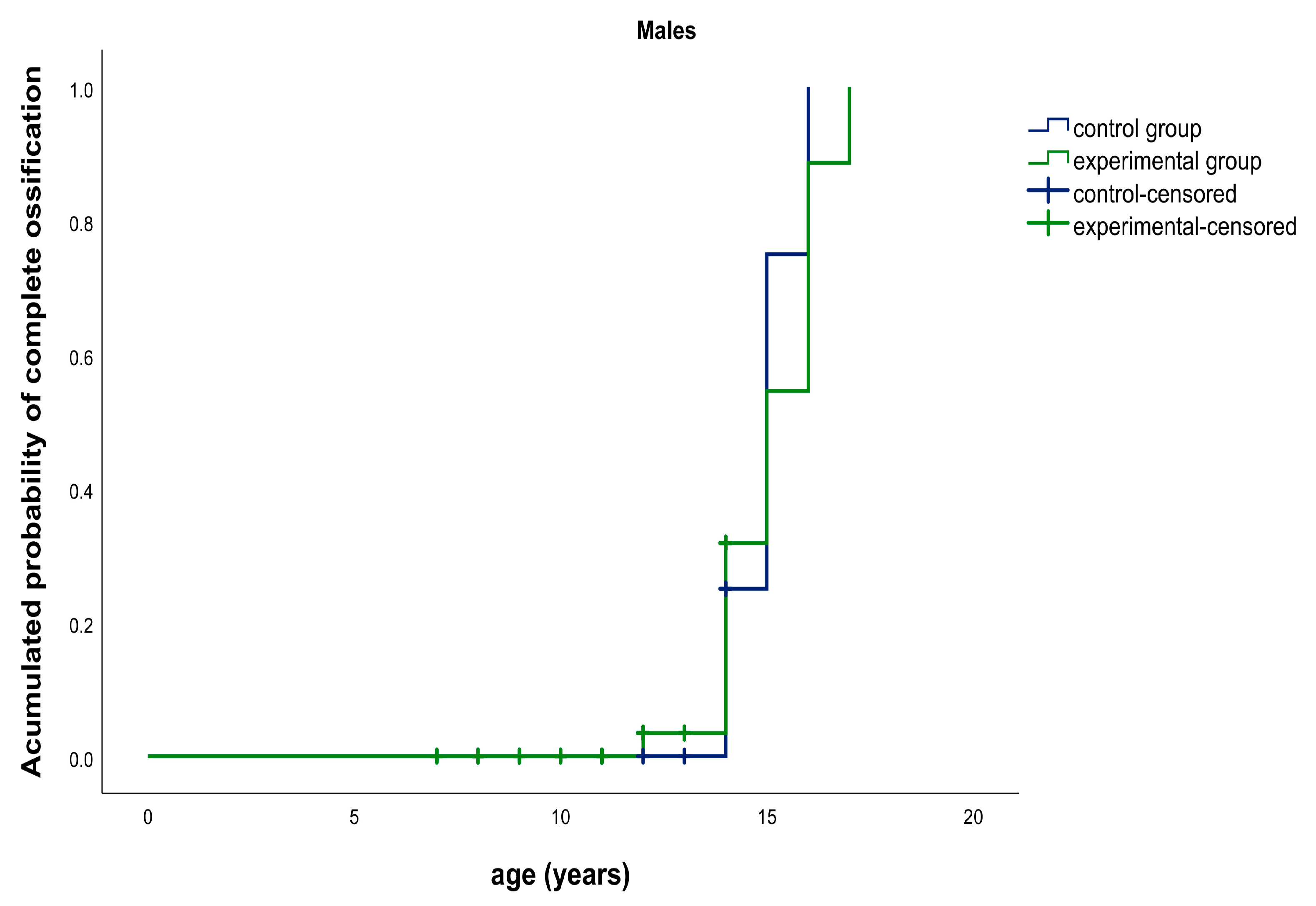
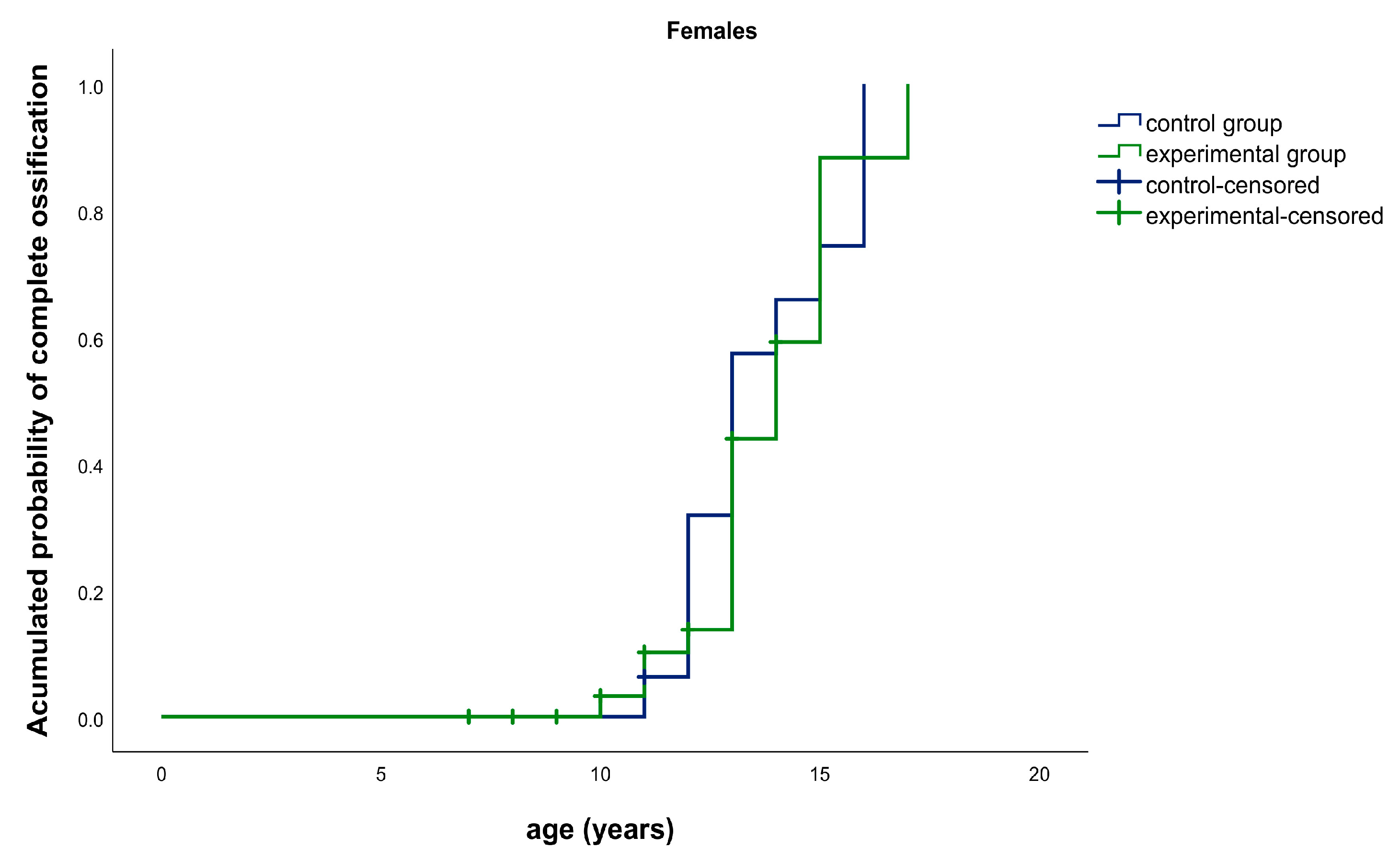
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
CBCT Images of the Fusion Stages of the Spheno-Occipital Synchondrosis

Appendix B
Spheno-Occipital Synchondrosis Fusion Based on a Five-Stage System Proposed by Bassed et al. 2010
| Stage | Definition |
| 1 | Synchondrosis is completely open and unfused. |
| 2 | Superior border has fused while the remaining fusion site is open. |
| 3 | Superior half of the synchondrosis is fused. |
| 4 | Complete fusion with a fusion scar in site still visible. |
| 5 | Synchondrosis has been completely obliterated with the appearance of normal bone in site. |
References
- Shkoukani, M.A.; Chen, M.; Vong, A. Cleft lip—A comprehensive review. Front. Pediatr. 2013, 1, 53. [Google Scholar] [CrossRef]
- Watkins, S.E.; Meyer, R.E.; Strauss, R.P.; Aylsworth, A.S. Classification, Epidemiology, and Genetics of Orofacial Clefts. Clin. Plast. Surg. 2014, 41, 149–163. [Google Scholar] [CrossRef]
- Horswell, B.B.; Gallup, B.V. Cranial base morphology in cleft lip and palate: A cephalometric study from 7 to 18 years of age. J. Oral Maxillofac. Surg. 1992, 50, 681–685. [Google Scholar] [CrossRef]
- Liu, X.; Chen, Z. Effects of Palate Repair on Cranial Base and Maxillary Morphology in Patients with Unilateral Complete Cleft Lip and Palate. Cleft Palate-Craniofacial J. 2018, 55, 1367–1374. [Google Scholar] [CrossRef]
- Abuhijleh, E.; Aydemir, H.; Memikoglu, T.U.T. Three-dimensional craniofacial morphology in unilateral cleft lip and palate. J. Oral Sci. 2014, 56, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Meyer-Marcotty, P.D.P.; Stellzig-Eisenhauer, A. Dentofacial Self-Perception and Social Perception of Adults with Unilateral Cleft Lip and Palate. J. Orofac. Orthop. 2009, 70, 224–236. [Google Scholar] [CrossRef]
- Staderini, E.; De Luca, M.; Candida, E.; Rizzo, M.I.; Zadeh, O.R.; Bucci, D.; Zama, M.; Lajolo, C.; Cordaro, M.; Gallenzi, P. Lay People Esthetic Evaluation of Primary Surgical Repair on Three-Dimensional Images of Cleft Lip and Palate Patients. Medicina 2019, 55, 576. [Google Scholar] [CrossRef] [Green Version]
- Jahanbin, A.; Eslami, N.; Zarch, H.H.; Kobravi, S. Comparative Evaluation of Cranial Base and Facial Morphology of Cleft Lip and Palate Patients with Normal Individuals in Cone Beam Computed Tomography. J. Craniofacial Surg. 2015, 26, 785–788. [Google Scholar] [CrossRef]
- Harris, E.F. Size and form of the cranial base in isolated cleft lip and palate. Cleft Palate-Craniofacial J. 1993, 30, 170–174. [Google Scholar] [CrossRef]
- Molsted, K.; Kjaer, I.; Dahl, E. Cranial base in newborns with complete cleft lip and palate: Radiographic study. Cleft Palate-Craniofacial J. 1995, 32, 199–205. [Google Scholar] [CrossRef]
- Powell, T.V.; Brodie, A.G. Closure of the spheno-occipital synchondrosis. Anat. Rec. 1963, 147, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.H. The cranial base. Am. J. Phys. Anthropol. 1958, 16, 319–348. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, J.A.; Paliga, J.T.; Wink, J.D.; Bartlett, S.P.; Nah, H.-D.; Taylor, J.A. Earlier Evidence of Spheno-Occipital Synchondrosis Fusion Correlates with Severity of Midface Hypoplasia in Patients with Syndromic Craniosynostosis. Plast. Reconstr. Surg. 2014, 134, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Driessen, C.; Rijken, B.F.; Doerga, P.N.; Dremmen, M.H.; Joosten, K.F.; Mathijssen, I.M. The effect of early fusion of the spheno-occipital synchondrosis on midface hypoplasia and obstructive sleep apnea in patients with Crouzon syndrome. J. Cranio-Maxillofac. Surg. 2017, 45, 1069–1073. [Google Scholar] [CrossRef]
- Kanchan, T.; Krishan, K. Evaluation of spheno-occipital synchondrosis: A review of literature and considerations from forensic anthropologic point of view. J. Forensic Dent. Sci. 2013, 5, 72–76. [Google Scholar] [CrossRef] [Green Version]
- Coben, S. The spheno-occipital synchondrosis: The missing link between the profession’s concept of craniofacial growth and orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 1998, 114, 709–712. [Google Scholar] [CrossRef]
- Singh, G.D. Morphologic determinants in the etiology of class III malocclusions: A review. Clin. Anat. 1999, 12, 382–405. [Google Scholar] [CrossRef]
- Yang, J.-H.; Cha, B.-K.; Choi, D.S.; Park, J.H.; Jang, I. Time and pattern of the fusion of the spheno-occipital synchondrosis in patients with skeletal Class I and Class III malocclusion. Angle Orthod. 2019, 89, 470–479. [Google Scholar] [CrossRef] [Green Version]
- Tahiri, Y.; Paliga, J.T.; Vossough, A.; Bartlett, S.P.; Taylor, J.A. The Spheno-Occipital Synchondrosis Fuses Prematurely in Patients with Crouzon Syndrome and Midface Hypoplasia Compared with Age- and Gender-Matched Controls. J. Oral Maxillofac. Surg. 2014, 72, 1173–1179. [Google Scholar] [CrossRef]
- Ingervall, B.; Thilander, B. The Human Sphenooccipital Synchondrosis I. The Time of Closure Appraised Macroscopically. Acta Odontol. Scand. 1972, 30, 349–356. [Google Scholar] [CrossRef]
- Lottering, N.; MacGregor, D.M.; Alston-Knox, C.; Gregory, L.S. Ontogeny of the spheno-occipital synchondrosis in a modern Queensland, Australian population using computed tomography. Am. J. Phys. Anthr. 2014, 157, 42–57. [Google Scholar] [CrossRef] [PubMed]
- McGrath, J.; Gerety, P.A.; Derderian, C.A.; Steinbacher, D.M.; Vossough, A.; Bartlett, S.P.; Nah, H.-D.; Taylor, J.A. Differential Closure of the Spheno-occipital Synchondrosis in Syndromic Craniosynostosis. Plast. Reconstr. Surg. 2012, 130, 681e–689e. [Google Scholar] [CrossRef] [PubMed]
- Coll, G.; Sakka, L.; Botella, C.; Pham-Dang, N.; Collet, C.; Zerah, M.; Arnaud, E.; Di Rocco, F. Pattern of Closure of Skull Base Synchondroses in Crouzon Syndrome. World Neurosurg. 2018, 109, e460–e467. [Google Scholar] [CrossRef] [PubMed]
- Horner, K.; Islam, M.; Flygare, L.; Tsiklakis, K.; Whaites, E. Basic principles for use of dental cone beam computed tomography: Consensus guidelines of the European Academy of Dental and Maxillofacial Radiology. Dentomaxillofacial Radiol. 2009, 38, 187–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Commission. Radiation Protection No 172: Cone Beam CT for Dental and Maxillofacial Radiology. Evidence Based Guidelines. 2012. Available online: http://www.sedentexct.eu/files/radiation_protection_172.pdf (accessed on 24 March 2020).
- Bassed, R.B.; Briggs, C.; Drummer, O.H. Analysis of time of closure of the spheno-occipital synchondrosis using computed tomography. Forensic Sci. Int. 2010, 200, 161–164. [Google Scholar] [CrossRef]
- Mølsted, K.; Kjaer, I.; Dahl, E. Spheno-occipital synchondrosis in three-month-old children with clefts of the lip and palate: A radiographic study. Cleft Palate-Craniofacial J. 1993, 30, 569–573. [Google Scholar] [CrossRef]
- Shah, N.; Bansal, N.; Logani, A. Recent advances in imaging technologies in dentistry. World J. Radiol. 2014, 6, 794–807. [Google Scholar] [CrossRef]
- Sinanoglu, A.; Kocasarac, H.D.; Noujeim, M. Age estimation by an analysis of spheno-occipital synchondrosis using cone-beam computed tomography. Leg. Med. 2016, 18, 13–19. [Google Scholar] [CrossRef]
- Kim, J.H.; Jeong, H.-G.; Hwang, J.J.; Lee, J.-H.; Han, S.-S. The impact of reorienting cone-beam computed tomographic images in varied head positions on the coordinates of anatomical landmarks. Imaging Sci. Dent. 2016, 46, 133–139. [Google Scholar] [CrossRef] [Green Version]
- Angelieri, F.; Franchi, L.; Cevidanes, L.H.S.; McNamara, J.A., Jr. Diagnostic performance of skeletal maturity for the assessment of midpalatal suture maturation. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 1010–1016. [Google Scholar] [CrossRef]
- De Grauwe, A.; Ayaz, I.; Shujaat, S.; Dimitrov, S.; Gbadegbegnon, L.; Vannet, B.V.; Jacobs, R. CBCT in orthodontics: A systematic review on justification of CBCT in a paediatric population prior to orthodontic treatment. Eur. J. Orthod. 2019, 41, 381–389. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Oral and Maxillofacial Radiology. Clinical recommendations regarding use of cone beam computed tomography in orthodontics. Position statement by the American Academy of Oral and Maxillofacial Radiology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 238–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fusion Stage | Sex | Number of Individuals | Mean Age | Min | Max | CI95% | SD |
|---|---|---|---|---|---|---|---|
| 1 | M | 29 | 10 | 7 | 14 | [9.4; 11.1] | 2.2 |
| F | 9 | 9 | 7 | 13 | [7.3; 10.5] | 2.1 | |
| 2 | M | 9 | 11 | 8 | 14 | [9.4; 12.9] | 2.3 |
| F | 3 | 11 | 10 | 12 | [8.5; 14.2] | 1.2 | |
| 3 | M | 3 | 14 | 13 | 14 | [12.2; 15.1] | 0.6 |
| F | 5 | 12 | 8 | 14 | [9.0; 14.6] | 2.3 | |
| 4 | M | 7 | 15 | 12 | 17 | [13.3; 16.4] | 1.7 |
| F | 9 | 12 | 10 | 14 | [11.3; 13.4] | 1.4 | |
| 5 | M | 5 | 15 | 14 | 16 | [13.5; 15.7] | 0.9 |
| F | 12 | 15 | 13 | 17 | [13.7; 15.5] | 1.4 |
| Fusion Stage | Sex | Number of Individuals | Mean Age | Min | Max | CI95% | SD |
|---|---|---|---|---|---|---|---|
| 1 | M | 8 | 10 | 8 | 14 | [8.5; 12.0] | 2.1 |
| F | 3 | 10 | 8 | 11 | [5.7; 14.3] | 1.7 | |
| 2 | M | 4 | 13 | 12 | 14 | [11.7; 14.8] | 1.0 |
| F | 2 | 11 | 11 | 11 | [11.0; 11.0] | 0.0 | |
| 3 | M | 0 | 0 | 0 | 0 | [0.0; 0.0] | 0.0 |
| F | 0 | 0 | 0 | 0 | [0.0; 0.0] | 0.0 | |
| 4 | M | 2 | 14 | 14 | 14 | [14.0; 14.0] | 0.0 |
| F | 8 | 13 | 11 | 16 | [11.5; 14.0] | 1.5 | |
| 5 | M | 3 | 15 | 15 | 16 | [13.9; 16.8] | 0.6 |
| F | 4 | 15 | 14 | 16 | [13.7; 16.8] | 1.0 |
| Experimental Group (n = 91) | Control Group (n = 34) | ||
|---|---|---|---|
| Sex | 0.409 * | ||
| Male | 53 (58.2%) | 17 (50%) | |
| Female | 38 (41.8%) | 17 (50%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vale, F.; Francisco, I.; Lucas, A.; Roseiro, A.; Caramelo, F.; Sobral, A. Timing of Spheno-Occipital Synchondrosis Ossification in Children and Adolescents with Cleft Lip and Palate: A Retrospective Case-Control Study. Int. J. Environ. Res. Public Health 2020, 17, 8889. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17238889
Vale F, Francisco I, Lucas A, Roseiro A, Caramelo F, Sobral A. Timing of Spheno-Occipital Synchondrosis Ossification in Children and Adolescents with Cleft Lip and Palate: A Retrospective Case-Control Study. International Journal of Environmental Research and Public Health. 2020; 17(23):8889. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17238889
Chicago/Turabian StyleVale, Francisco, Inês Francisco, António Lucas, Ana Roseiro, Francisco Caramelo, and Adriana Sobral. 2020. "Timing of Spheno-Occipital Synchondrosis Ossification in Children and Adolescents with Cleft Lip and Palate: A Retrospective Case-Control Study" International Journal of Environmental Research and Public Health 17, no. 23: 8889. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17238889