A Nationwide Survey on Working Hours and Working Environment among Hospital Dentists in Japan




Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.1.1. Sociodemographic Characteristics
2.1.2. Working Hours and Work Sharing
2.1.3. Working Environment
2.1.4. Preference of Future Career
2.2. Data Analysis
2.3. Ethical Approval
3. Results
3.1. Sociodemographics and General Characteristics of the Study Subjects
Sociodemographic Factors of Respondents
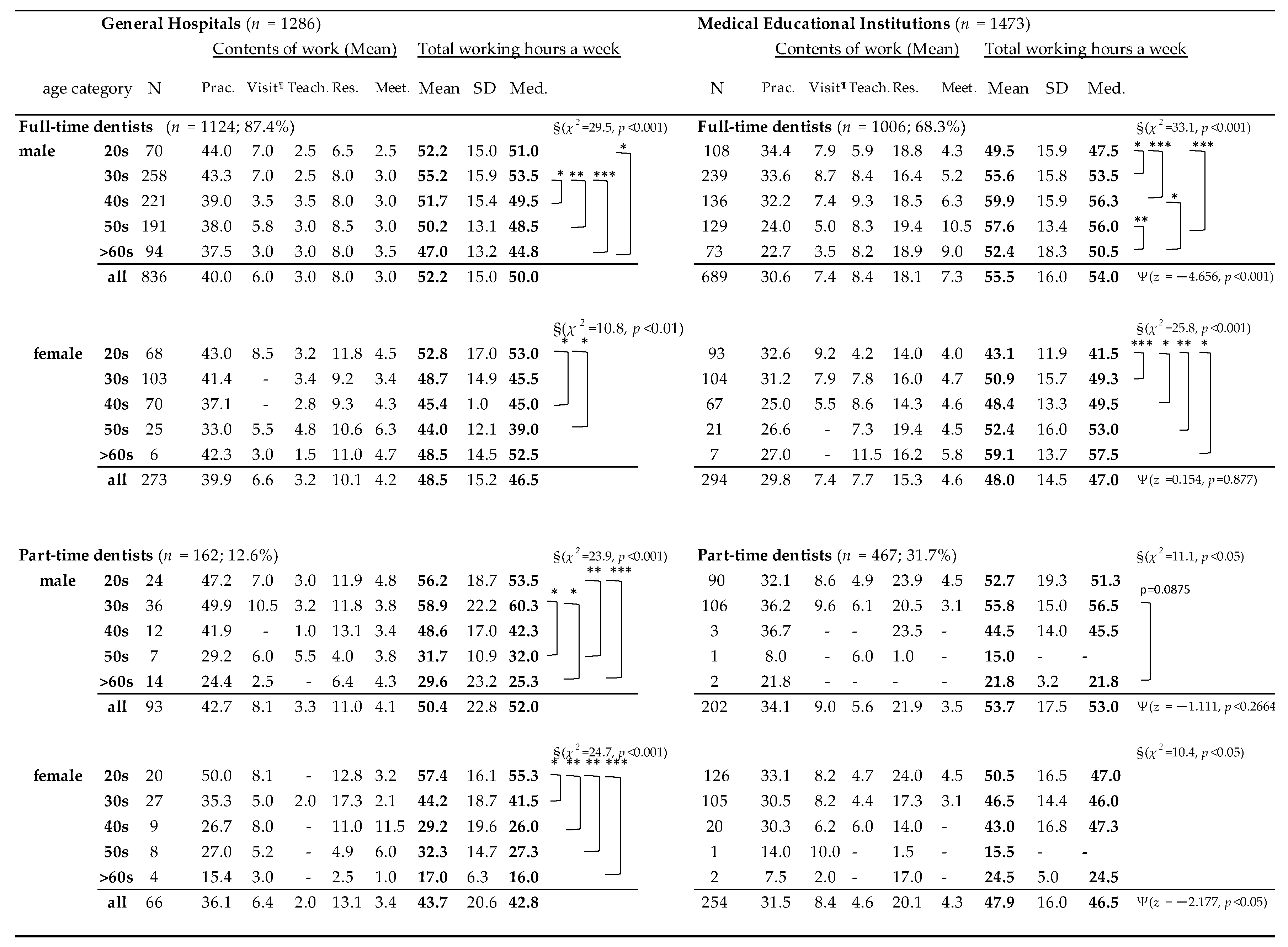
3.2. Working Hours of Hospital Dentists
3.2.1. Working Hours of Hospital Dentists
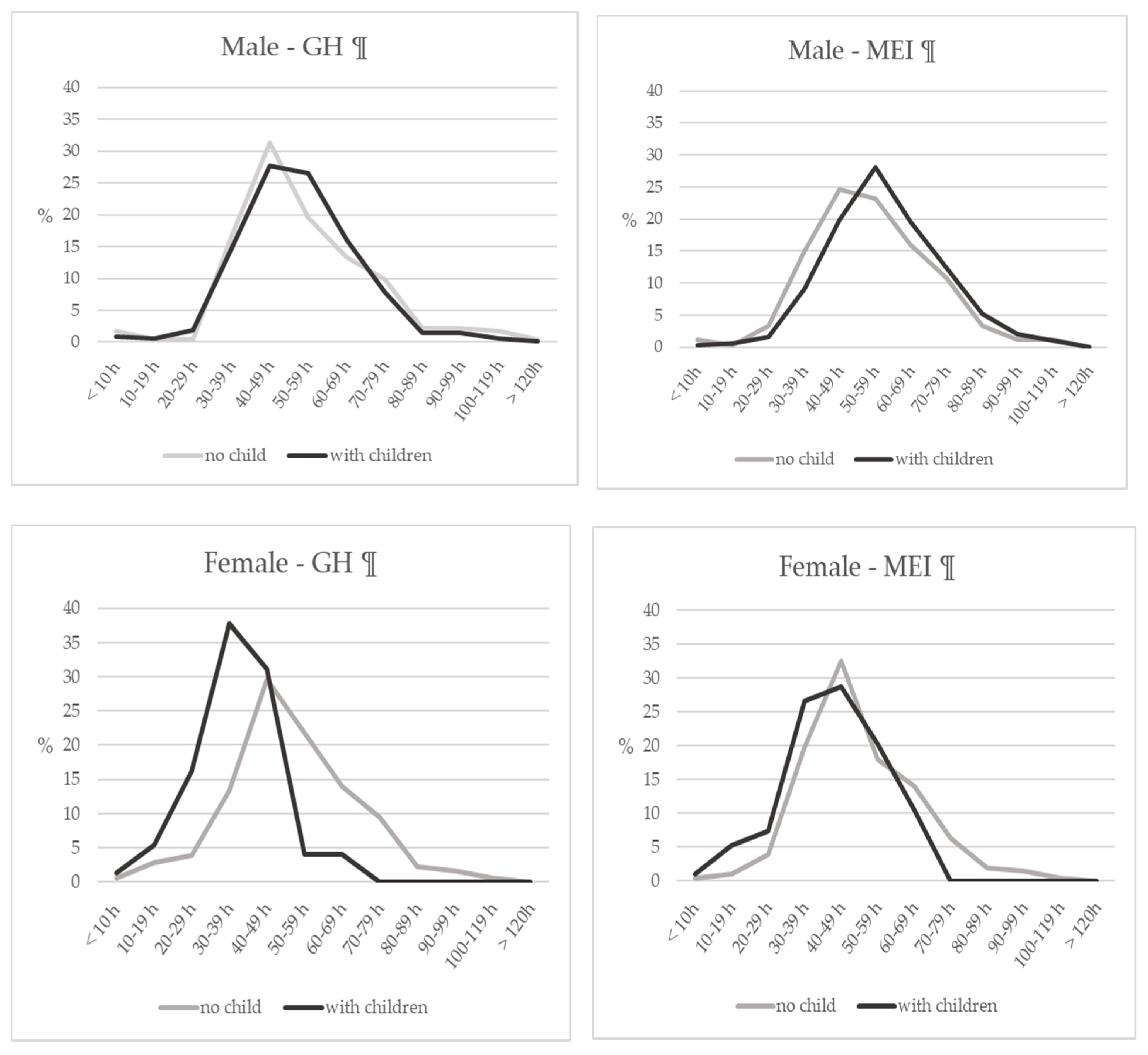
3.2.2. Weekly Working Hours
3.2.3. Factors Associated with Working over 60 h per Week
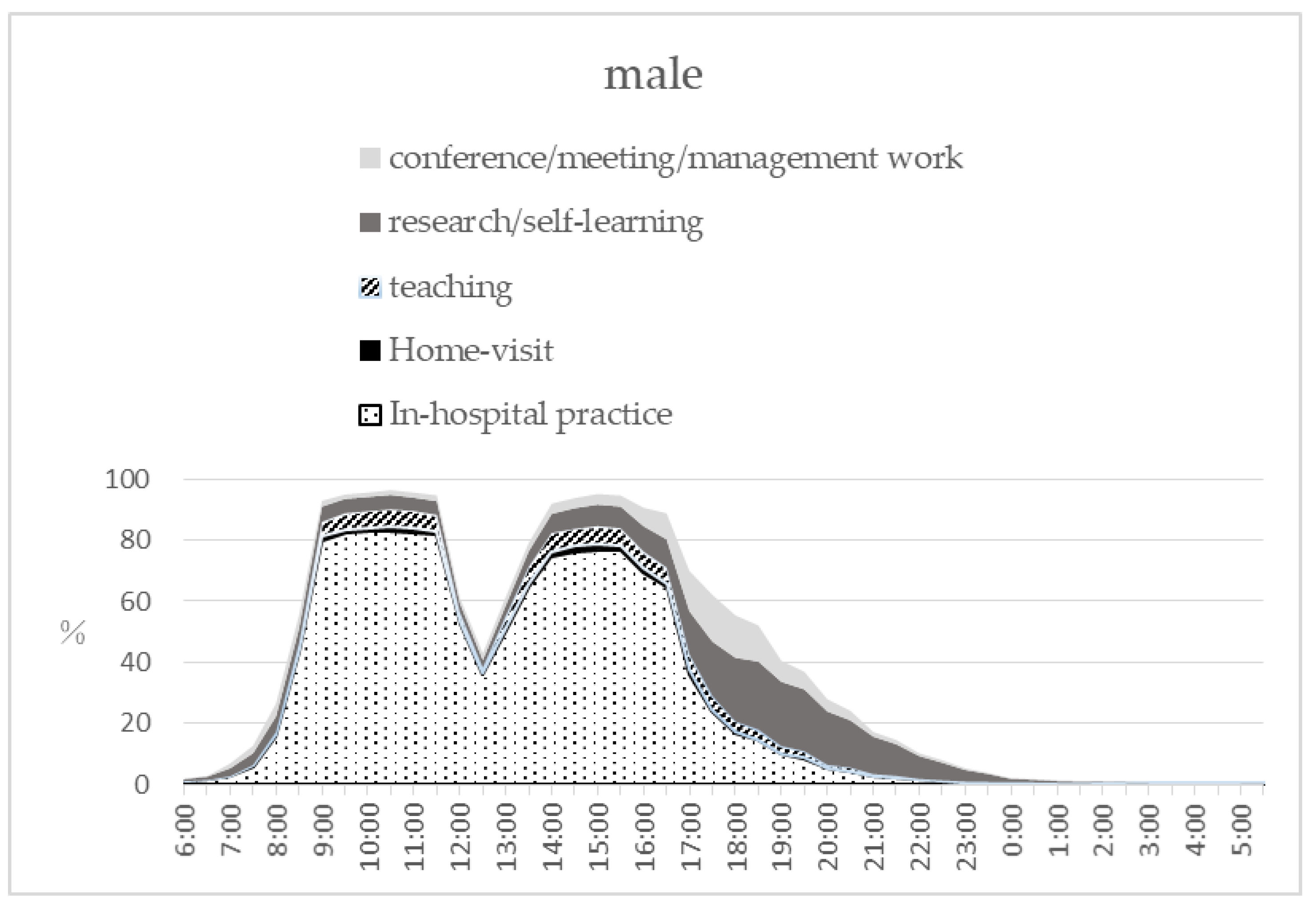
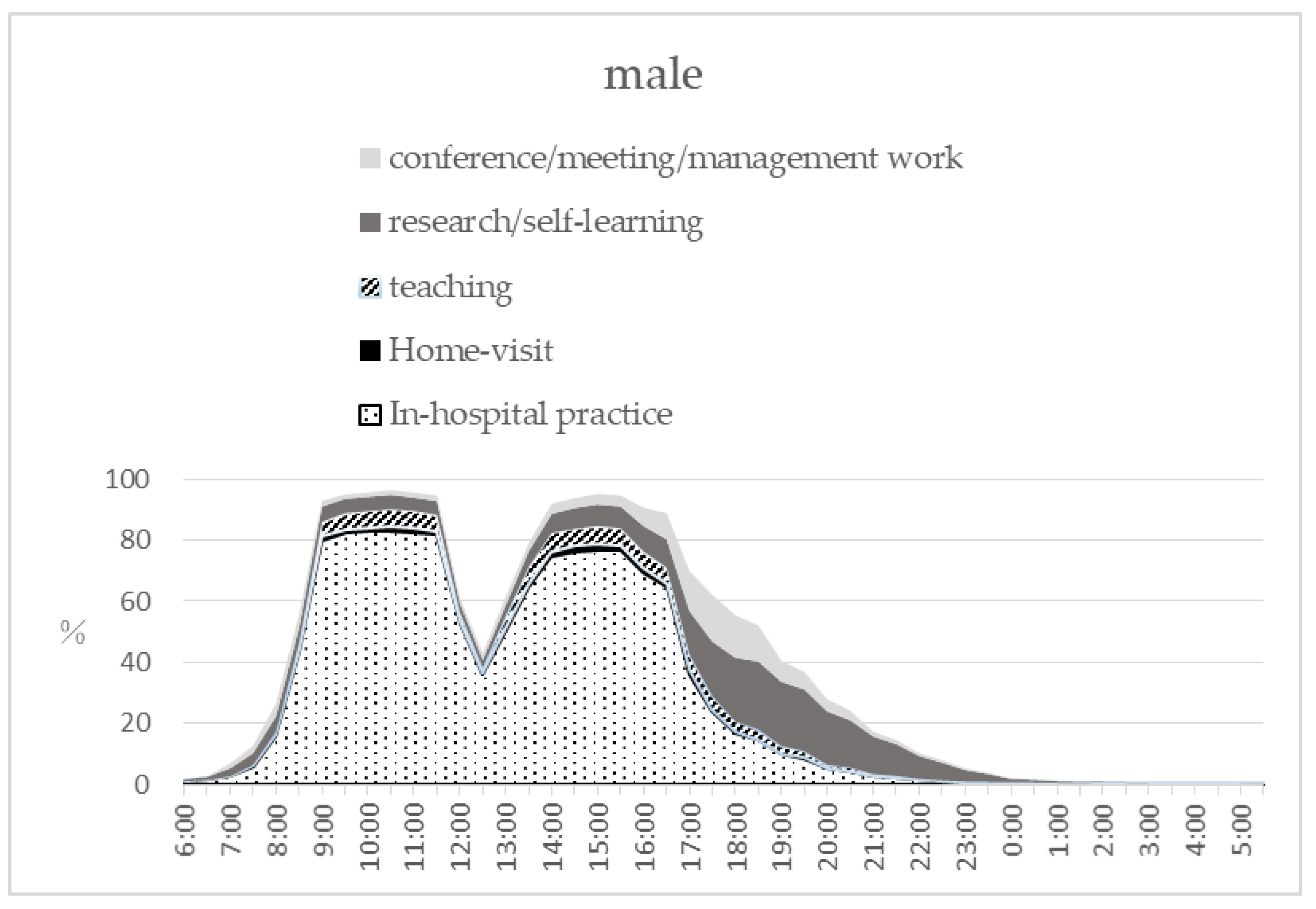
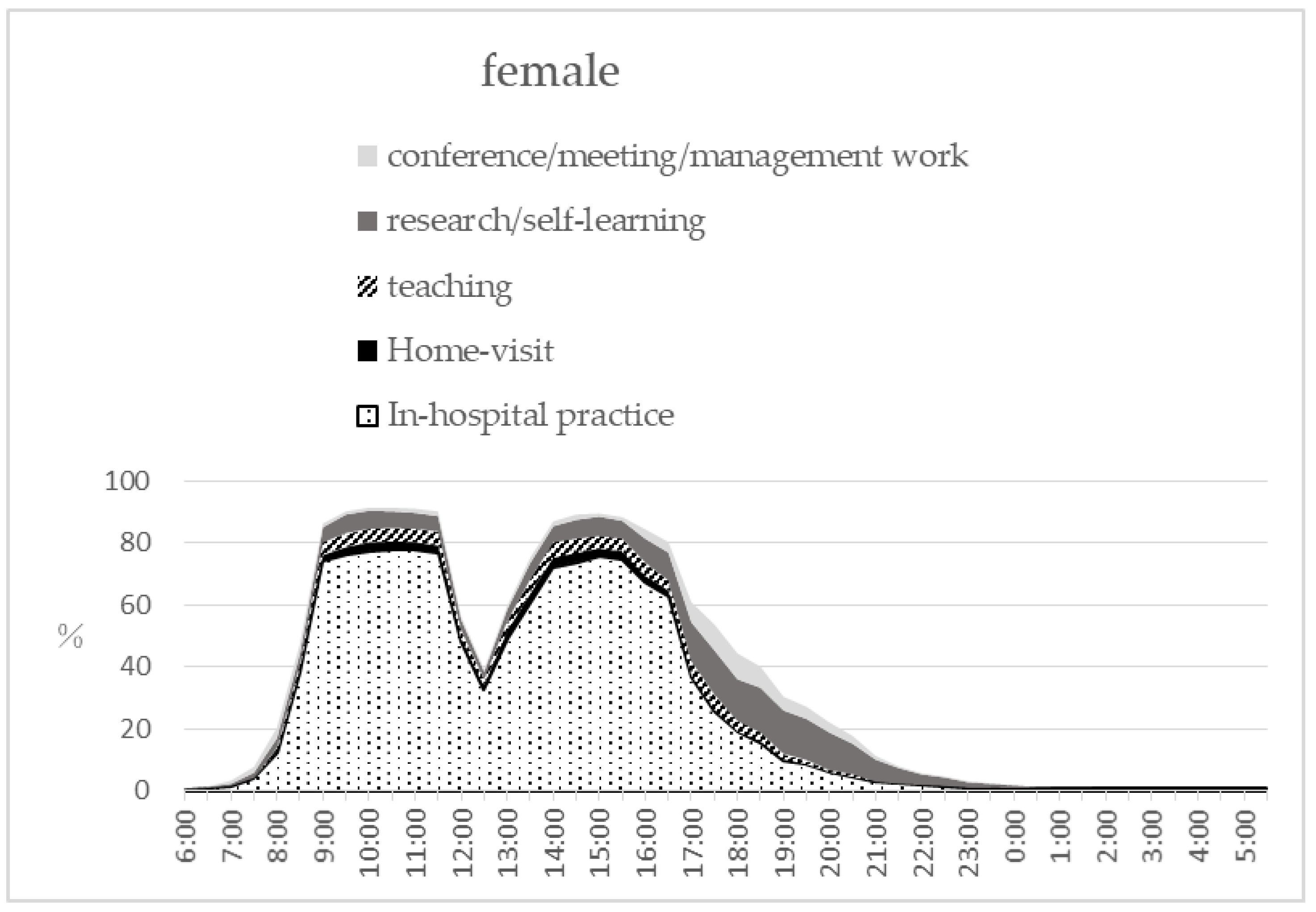
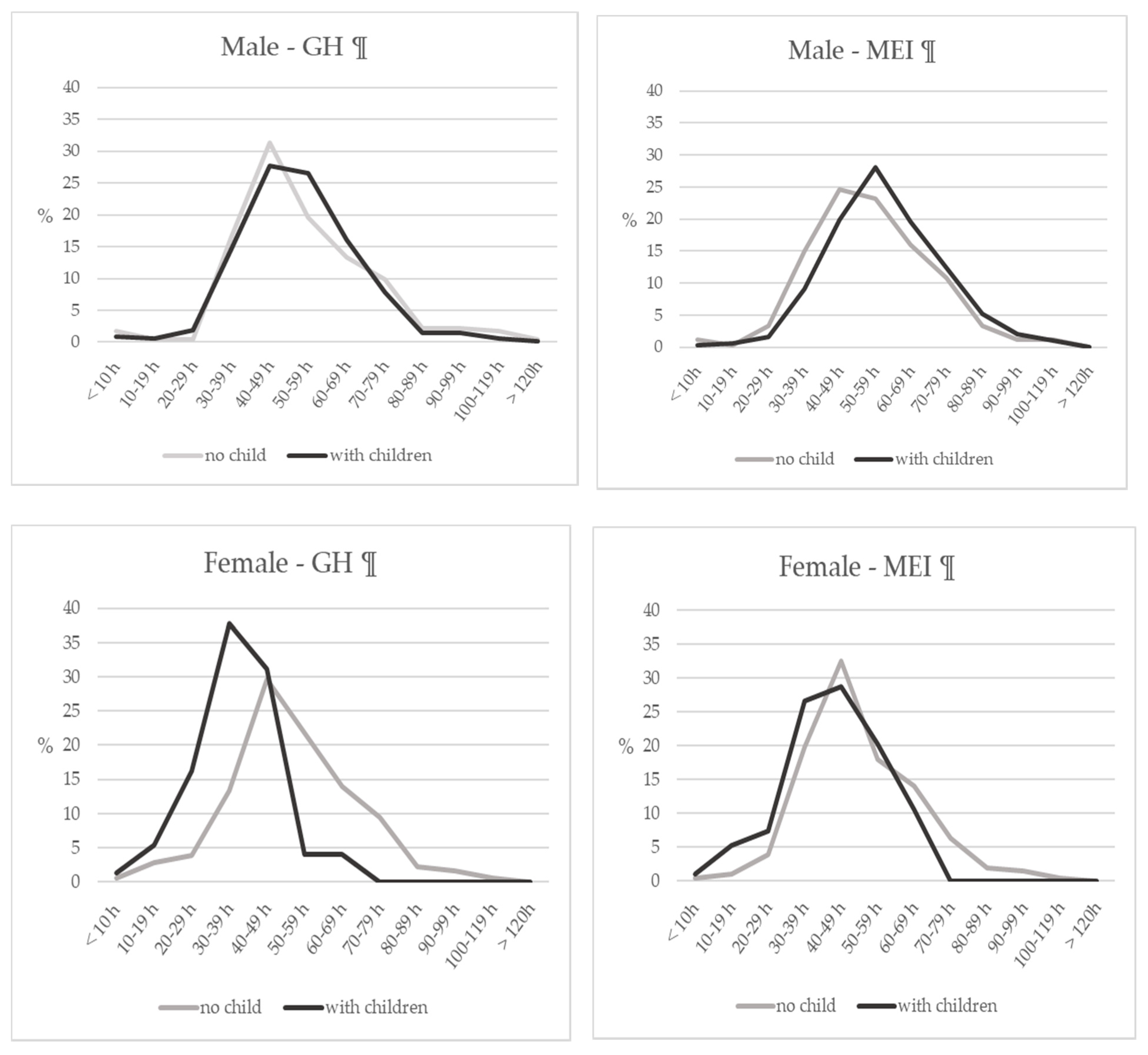
3.2.4. Time Distribution of Working Hours by Gender and Workplace
3.2.5. Task Shifting
3.3. Working Environment for Who Needs Childcare or Nursing Care of Their Aged Parents
3.4. Unwillingness to Work Outside of Urban Areas and Future Career
4. Discussion
4.1. Representativeness of the Subjects
4.2. Working Hours among Hospital Dentists and Expected Task Shift
4.3. Excess Working Hours over 60 h per Week
4.4. Annual Leave among Hospital Dentists
4.5. Working Environment and Facility Work Engagement
4.6. Specialty Area of Practice in General Hospitals
4.7. Adequate Work-Balance for Dentists—Childcare, Nursing Care, and Division of Duties
4.8. Location Preference—Urban and Rural Areas
4.9. Limitations of this Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Kossioni, A.E.; Hajto-Bryk, J.; Maggi, S.; McKenna, G.; Petrovic, M.; Roller-Wirnsberger, R.E.; Schimmel, M.; Tamulaitienè, M.; Vanobbergen, J.; Müller, F. An Expert Opinion from the European College of Gerodontology and the European Geriatric Medicine Society: European Policy Recommendations on Oral Health in Older Adults. J. Am. Geriatr. Soc. 2018, 66, 609–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramsay, S.E.; Papachristou, E.; Watt, R.G.; Tsakos, G.; Lennon, L.T.; Papacosta, A.O.; Moynihan, P.; Sayer, A.A.; Whincup, P.H.; Wannamethee, S.G. Influence of Poor Oral Health on Physical Frailty: A Population-Based Cohort Study of Older British Men. J. Am. Geriatr. Soc. 2018, 66, 473–479. [Google Scholar] [CrossRef] [Green Version]
- Comprehensive Survey of Living Conditions; Household Statistics Office, Ministry of Health, Labours and Welfare: Tokyo, Japan, 2019. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/k-tyosa/k-tyosa19/index.htmlb (accessed on 30 August 2020).
- Interim Report of “Study Group on Improving Dentist Qualities”~Proposal of “Dental Health Vision”; Ministry of Health, Labours and Welfare: Tokyo, Japan, 25 December 2017. Available online: https://www.mhlw.go.jp/file/05-Shingikai-10801000-Iseikyoku-Soumuka/0000189586.pdf (accessed on 30 August 2020).
- Gallagher, J.E.; Kleinman, E.R.; Harper, P.R. Modelling workforce skill-mix: How can dental professionals meet the needs and demands of older people in England? Br. Dent. J. 2010, 208, E6. [Google Scholar] [CrossRef] [Green Version]
- Russek, H.I. Emotional stress and coronary heart disease in American physicians, dentists and lawyers. Am. J. Med. Sci. 1962, 243, 716–726. [Google Scholar] [CrossRef]
- Davidovich, E.; Pessov, Y.; Baniel, A.; Ram, D. Levels of Stress among General Practitioners, Students and Specialists In Pediatric Dentistry during Dental Treatment. J. Clin. Pediatric Dent. 2015, 39, 419–422. [Google Scholar] [CrossRef]
- Pouradeli, S.; Shahravan, A.; Eskandarizdeh, A.; Rafie, F.; Hashemipour, M.A. Occupational Stress and Coping Behaviours Among Dentists in Kerman, Iran. Sultan Qaboos Univ. Med. J. 2016, 16, e341–e346. [Google Scholar] [CrossRef]
- Singh, P.; Aulak, D.S.; Mangat, S.S.; Aulak, M.S. Systematic review: Factors contributing to burnout in dentistry. Occup. Med. 2016, 66, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Jugale, P.V.; Mallaiah, P.; Krishnamurthy, A.; Sangha, R. Burnout and Work Engagement Among Dental Practitioners in Bangalore City: A Cross-Sectional Study. J. Clin. Diagn. Res. JCDR 2016, 10, Zc63–Zc67. [Google Scholar] [CrossRef]
- Davidson, P.L.; Nakazono, T.T.; Carreon, D.C.; Gutierrez, J.J.; Shahedi, S.; Andersen, R.M. Reforming dental workforce education and practice in the USA. Eur. J. Dent. Educ. Off. J. Assoc. Dent. Educ. Eur. 2011, 15, 73–79. [Google Scholar] [CrossRef]
- Holmes, R.D.; Burford, B.; Vance, G. Development and retention of the dental workforce: Findings from a regional workforce survey and symposium in England. BMC Health Serv. Res. 2020, 20, 255. [Google Scholar] [CrossRef] [PubMed]
- Surveys and Research on Physician’s Working Conditions and Attitudes; Ministry of Health, Labours and Welfare: Tokyo, Japan, 2016. Available online: https://www.mhlw.go.jp/file/05-Shingikai-10801000-Iseikyoku-Soumuka/0000161146.pdf (accessed on 30 August 2020).
- Survey of Medical Institutions; Health Statistics Office, Minister’s Secretariat, Ministry of Health, Labour and Welfare: Tokyo, Japan, 2017.
- van Doorne-Huiskes, A. Women and work, with a specific focus on doctors and dentists. Ned. Tijdschr. Voor Tandheelkd. 2017, 124, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, R.; Seo, E.; Maeno, T.; Ito, M.; Sanuki, M.; Maeno, T. The relationship between long working hours and depression among first-year residents in Japan. BMC Med. Educ. 2018, 18, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishimura, Y.; Miyoshi, T.; Obika, M.; Ogawa, H.; Kataoka, H.; Otsuka, F. Factors related to burnout in resident physicians in Japan. Int. J. Med. Educ. 2019, 10, 129–135. [Google Scholar] [CrossRef]
- Saijo, Y.; Chiba, S.; Yoshioka, E.; Kawanishi, Y.; Nakagi, Y.; Itoh, T.; Sugioka, Y.; Kitaoka-Higashiguchi, K.; Yoshida, T. Effects of work burden, job strain and support on depressive symptoms and burnout among Japanese physicians. Int. J. Occup Med. Environ. Health 2014, 27, 980–992. [Google Scholar] [CrossRef]
- Calvo, J.M.; Kwatra, J.; Yansane, A.; Tokede, O.; Gorter, R.C.; Kalenderian, E. Burnout and Work Engagement Among US Dentists. J. Patient Saf. 2017, 10. [Google Scholar] [CrossRef]
- Collin, V.; Toon, M.; O’Selmo, E.; Reynolds, L.; Whitehead, P. A survey of stress, burnout and well-being in UK dentists. Br. Dent. J. 2019, 226, 40–49. [Google Scholar] [CrossRef]
- Choy, H.B.; Wong, M.C. Occupational stress and burnout among Hong Kong dentists. Hong Kong Med. J. Xianggang Yi Xue Za Zhi 2017, 23, 480–488. [Google Scholar] [CrossRef] [Green Version]
- Overview of 2016 General Survey on Working Conditions; Ministry of Health, Labor and Welfare: Tokyo, Japan, 2019. Available online: https://www.mhlw.go.jp/toukei/itiran/roudou/jikan/syurou/19/dl/gaikyou.pdf (accessed on 25 September 2020).
- Report of the Study Group on Working Style Reform for Doctors; Ministry of Health, Labours and Welfare: Tokyo, Japan, March 2019. Available online: https://www.mhlw.go.jp/content/10800000/000496522.pdf (accessed on 25 September 2020).
- Imoto, S.; Ohiso, G.; Nakamura, R.; Hashimoto, H.; Hasegawa, T.; Furutani, T.; Morita, T.; Morita-Takeuchi, M.; Yamaguchio, R.; Yuchi, K. Survey of physicians’ working conditions and working intentions. In Welfare Labor Administration Promotion Survey; Ministry of Health, Labours and Welfare: Tokyo, Japan, 2017. Available online: https://www.mhlw.go.jp/file/05-Shingikai-10801000-Iseikyoku-Soumuka/0000161146.pdf (accessed on 25 September 2020).
- Cheng, L.; Tandon, P. Out of hours cross-cover between oral and maxillofacial surgery and ear, nose and throat surgery. Ann. R. Coll. Surg. Engl. 1997, 79, 9–11. [Google Scholar]
- den Boer, J.C.L.; Zijderveld, S.A.; Bruers, J.J.M. Preferred and actual retirement age of oral and maxillofacial surgeons aged 55 and older in the Netherlands: A longitudinal study from 2003 to 2016. Hum. Resour. Health 2018, 16, 25. [Google Scholar] [CrossRef]
- Abelsen, B.; Olsen, J.A. Task division between dentists and dental hygienists in Norway. Community Dent. Oral Epidemiol. 2008, 36, 558–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruers, J.J.; van Rossum, G.M.; Felling, A.J.; Truin, G.J.; van’t Hof, M.A. Business orientation and the willingness to distribute dental tasks of Dutch dentists. Int. Dent. J. 2003, 53, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Mishler, S.K.; Inglehart, M.R.; McComas, M.J.; Murdoch-Kinch, C.A.; Kinney, J.S. General Dentists’ Perceptions of Dental Hygienists’ Professional Role: A Survey. J. Dent. Hyg. JDH 2018, 92, 30–39. [Google Scholar] [PubMed]
- Al-Junaid, S.M.; Hodges, S.J.; Petrie, A.; Cunningham, S.J. Career satisfaction and work-life balance of specialist orthodontists within the UK/ROI. Br. Dent. J. 2017, 223, 53–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The National Survey on Family; The National Institute of Population and Social Security Research: Tokyo, Japan, 2019.
- Ono, H. Why do the Japanese work long hours? Sociological perspectives on long working hours in Japan. Jpn. Labor Issues 2018, 2, 40. [Google Scholar]
- Barnett, T.; Hoang, H.; Stuart, J.; Crocombe, L. The relationship of primary care providers to dental practitioners in rural and remote Australia. BMC Health Serv. Res. 2017, 17, 515. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sociodemographhic Factors | Total | Male | Female | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Age | 20s *** | 674 | 23.1 | 316 | 16.6 | 344 | 36.5 |
| 30s | 1023 | 35.1 | 658 | 34.6 | 351 | 37.2 | |
| 40s | 563 | 19.3 | 383 | 20.1 | 167 | 17.7 | |
| 50s *** | 409 | 14.0 | 341 | 17.9 | 57 | 6.0 | |
| >60s *** | 226 | 7.8 | 198 | 10.4 | 19 | 2.0 | |
| missing | 19 | 0.7 | - | - | - | ||
| Type of services | |||||||
| Hospital administrator | 36 | 1.2 | 30 | 1.6 | 4 | 0.4 | |
| Full-time employment *** | 2186 | 75.0 | 1552 | 82.5 | 587 | 63.7 | |
| Part-time employment *** | 641 | 22.0 | 299 | 15.9 | 331 | 35.9 | |
| Missing | 51 | 1.8 | |||||
| Area of specialty (duplicated) | |||||||
| Dentistry (including preservation and prosthesis) | 1555 | 53.4 | 1002 | 52.7 | 521 | 55.2 | |
| Orthodontics * | 159 | 5.5 | 90 | 4.7 | 66 | 7.0 | |
| Pediatric dentistry *** | 217 | 7.4 | 114 | 6.0 | 100 | 10.6 | |
| Dental and oral surgery *** | 1354 | 46.5 | 968 | 50.9 | 333 | 35.3 | |
| Other * | 221 | 7.6 | 128 | 6.7 | 88 | 9.3 | |
| Family or relatives living together (duplicate) | |||||||
| Spouse or partner *** | 1566 | 53.7 | 1222 | 64.2 | 305 | 32.3 | |
| Parents or relatives *** | 429 | 14.7 | 201 | 10.6 | 221 | 23.4 | |
| Children *** | 985 | 33.8 | 791 | 41.6 | 174 | 18.5 | |
| Others *** | 52 | 1.8 | 22 | 1.2 | 29 | 3.1 | |
| No housemate *** | 910 | 31.2 | 500 | 26.3 | 392 | 41.6 | |
| Missing | 14 | 0.5 | |||||
| Occupation of spouse or partner (n = 1606) | Male (n = 1245) | Female (n = 321) | |||||
| Dentist *** | 512 | 32.8 | 335 | 26.9 | 163 | 50.8 | |
| Doctor *** | 88 | 5.6 | 38 | 3.1 | 46 | 14.3 | |
| Dental hygienist *** | 104 | 6.7 | 102 | 8.2 | 0 | 0.0 | |
| Dental technician | 3 | 0.2 | 2 | 0.2 | 1 | 0.3 | |
| Other medical positions *** | 185 | 11.8 | 175 | 14.1 | 9 | 2.8 | |
| Other *** | 308 | 19.7 | 203 | 16.3 | 97 | 30.2 | |
| Unemployed *** | 406 | 26.0 | 390 | 31.3 | 5 | 1.6 | |
| Type of services of spouse or partner (n = 1571) | Male (n = 1215) | Female (n = 317) | |||||
| Full time *** | 536 | 35.0 | 292 | 24.0 | 233 | 73.5 | |
| Part time *** | 404 | 26.4 | 353 | 29.1 | 42 | 13.2 | |
| Self-employed *** | 104 | 6.8 | 64 | 5.3 | 37 | 11.7 | |
| Unemployed *** | 527 | 34.4 | 506 | 41.6 | 5 | 1.6 | |
| Annual leave acquisition rate | |||||||
| Not acquired | 1070 | 36.7 | 661 | 36.4 | 382 | 43.5 | |
| 1–5 days | 1064 | 36.5 | 725 | 39.9 | 315 | 35.8 | |
| 6–10 days | 454 | 15.6 | 311 | 17.1 | 134 | 15.2 | |
| 11–15 days | 117 | 4.0 | 81 | 4.5 | 34 | 3.9 | |
| 16 days or more | 52 | 1.8 | 37 | 2.0 | 14 | 1.6 | |
| Missing | 157 | 5.4 | - | - | |||
| Night shift for the last 4 weeks (days) | |||||||
| None *** | 2481 | 85.1 | 1622 | 85.2 | 859 | 91.1 | |
| 1–5 *** | 350 | 12.0 | 271 | 14.2 | 79 | 8.4 | |
| 6–10 | 12 | 0.4 | 9 | 0.5 | 3 | 0.3 | |
| ≥11 | 3 | 0.1 | 1 | 0.1 | 2 | 0.2 | |
| On call for the last 4 weeks (days) | |||||||
| None *** | 1850 | 86.5 | 1318 | 84.9 | 532 | 90.6 | |
| 1–5 *** | 277 | 12.9 | 226 | 14.6 | 51 | 8.7 | |
| 6–10 | 9 | 0.4 | 7 | 0.5 | 2 | 0.3 | |
| ≥11 | 3 | 0.1 | 1 | 0.1 | 2 | 0.3 | |
| Willingness to work in rural areas | |||||||
| No | 1475 | 50.6 | 762 | 40.0 | 419 | 44.4 | |
| Yes | 1181 | 40.5 | 1006 | 52.9 | 469 | 49.7 | |
| 20s * | 390 | 32.1 | 199 | 19.8 | 181 | 38.6 | |
| 30s | 574 | 47.2 | 386 | 38.4 | 183 | 39.0 | |
| 40s | 282 | 23.2 | 194 | 19.3 | 81 | 17.3 | |
| 50s * | 175 | 14.4 | 151 | 15.0 | 18 | 3.8 | |
| >60s | 83 | 6.8 | 76 | 7.6 | 6 | 1.3 | |
| NA | 2 | 0.2 | - | - | |||
| Missing | 258 | 8.9 | 135 | 7.1 | 55 | 5.8 | |
| Factors | Crude Model | Model I | Model II | ||||
|---|---|---|---|---|---|---|---|
| OR | 95% CI | (R2 = 0.0343) | (R2 = 0.0287) | ||||
| OR | 95% CI | OR | 95% CI | ||||
| Gender | Male | 1.76 *** | (1.46–2.13) | 1.95 *** | (1.60–2.38) | 1.83 *** | (1.50–2.22) |
| Age | 20s | ref | ref | ref | |||
| 30s | 1.29 * | (1.03–1.60) | 1.29 | (0.93–1.47) | 1.25 | (0.99–1.57) | |
| 40s | 1.07 | (0.83–1.38) | 0.96 | (0.73–1.26) | 1.03 | (0.79–1.35) | |
| 50s | 1.08 | (0.82–1.00) | 0.96 | (0.72–1.30) | 1.00 | (0.74–1.35) | |
| >60s | 0.69 | (0.48–1.00) | 0.55 ** | (0.37–0.82) | 0.58 ** | (0.39–0.86) | |
| Type of services | |||||||
| Full-time employment | 1.09 | (0.89–1.33) | |||||
| Workplace | |||||||
| General hospitals | ref | ref | ref | ||||
| Medical educational institutions | 1.22 * | (1.03–1.44) | 1.50 *** | (1.25–1.80) | 1.92 *** | (1.52–2.42) | |
| Area of specialty | |||||||
| Dentistry (including preservation and prosthesis) | 0.58 *** | (0.49–0.69) | 0.54 *** | (0.45–0.65) | |||
| Orthodontics | 0.81 | (0.55–1.18) | |||||
| Pediatric dentistry | 0.75 | (0.54–1.05) | |||||
| Dental and oral surgery | 1.32 ** | (1.12–1.56) | 1.85 *** | (1.47–2.32) | |||
| Family or relatives living together | |||||||
| Spouse or partner | 1.02 | (0.87–1.20) | |||||
| Parents or relatives | 0.94 | (0.74–1.18) | |||||
| Children | 1.03 | (0.87–1.23) | |||||
| Others | 0.71 | (0.36–1.38) | |||||
| No housemate | 1.08 | (0.91–1.29) | |||||
| Spouse of partner’s job | |||||||
| Full time | 0.90 | (0.73–1.12) | - | ||||
| Unemployed | 1.04 | (0.84–1.29) | - | ||||
| The Location Preference of Work and the Choice of Future Career | Full Time | Part Time | ||
|---|---|---|---|---|
| n | % | n | % | |
| The first reason for unwillingness to work outside of urban areas | (n = 992) | (n = 275) | ||
| To continue their desired line of work | 608 | 61.3 | 154 | 56.0 |
| For economic reasons (income/treatment) | 51 | 5.1 | 20 | 7.3 |
| Because there is no room for choice due to being medical personnel * | 76 | 7.7 | 11 | 4.0 |
| Because I am worried about the work environment * | 57 | 5.7 | 27 | 9.8 |
| Because the educational environment for children is not conducive | 61 | 6.1 | 22 | 8.0 |
| Because understanding from family is not obtained | 62 | 6.3 | 17 | 6.2 |
| For care of parents and relatives | 37 | 3.7 | 5 | 1.8 |
| Other * | 40 | 4.0 | 19 | 6.9 |
| The first choice for future career | (n = 2124) | (n = 630) | ||
| Employed practice | 1175 | 55.3 | 359 | 57.0 |
| Open own clinic for practice *** | 363 | 17.1 | 166 | 26.3 |
| Administrative positions (including local and central government or institutions) | 16 | 0.8 | 10 | 1.6 |
| Research or teaching (universities and research institutes) *** | 545 | 25.7 | 85 | 13.5 |
| Others | 25 | 1.2 | 10 | 1.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kodama, T.; Ida, Y.; Miura, H. A Nationwide Survey on Working Hours and Working Environment among Hospital Dentists in Japan. Int. J. Environ. Res. Public Health 2020, 17, 9048. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239048
Kodama T, Ida Y, Miura H. A Nationwide Survey on Working Hours and Working Environment among Hospital Dentists in Japan. International Journal of Environmental Research and Public Health. 2020; 17(23):9048. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239048
Chicago/Turabian StyleKodama, Tomoko, Yusuke Ida, and Hiroko Miura. 2020. "A Nationwide Survey on Working Hours and Working Environment among Hospital Dentists in Japan" International Journal of Environmental Research and Public Health 17, no. 23: 9048. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239048