Impact of Adverse Drug Reactions in Patients with End Stage Renal Disease in Greece

 ,
, 
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. ESRD Patients and Study Information
2.2. Drug–Drug Interactions
2.3. Adverse Drug Events (ADEs) and Adverse Drug Reactions (ADRs)
3. Results
3.1. Demographics, Comorbidities, and Lab Test Results
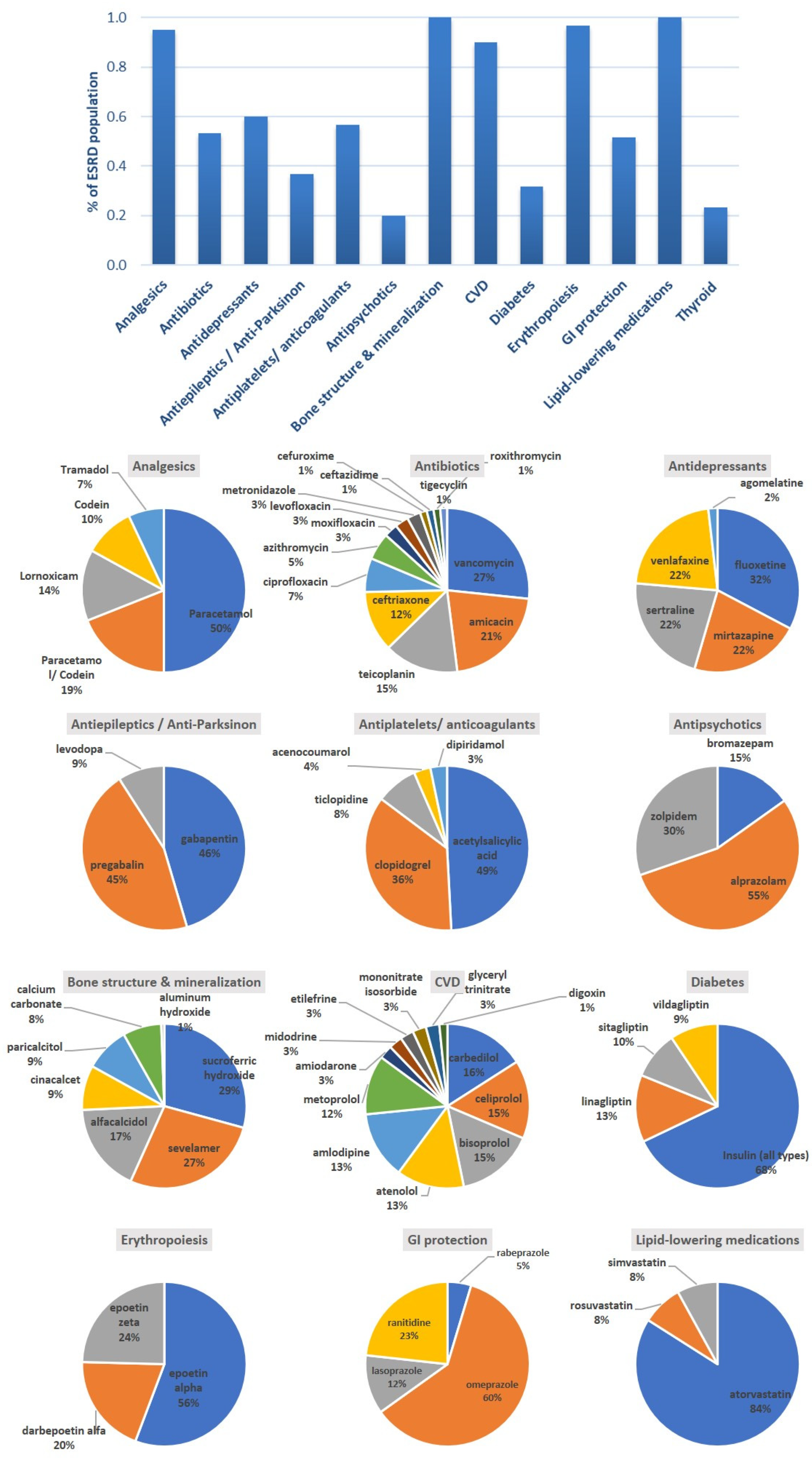
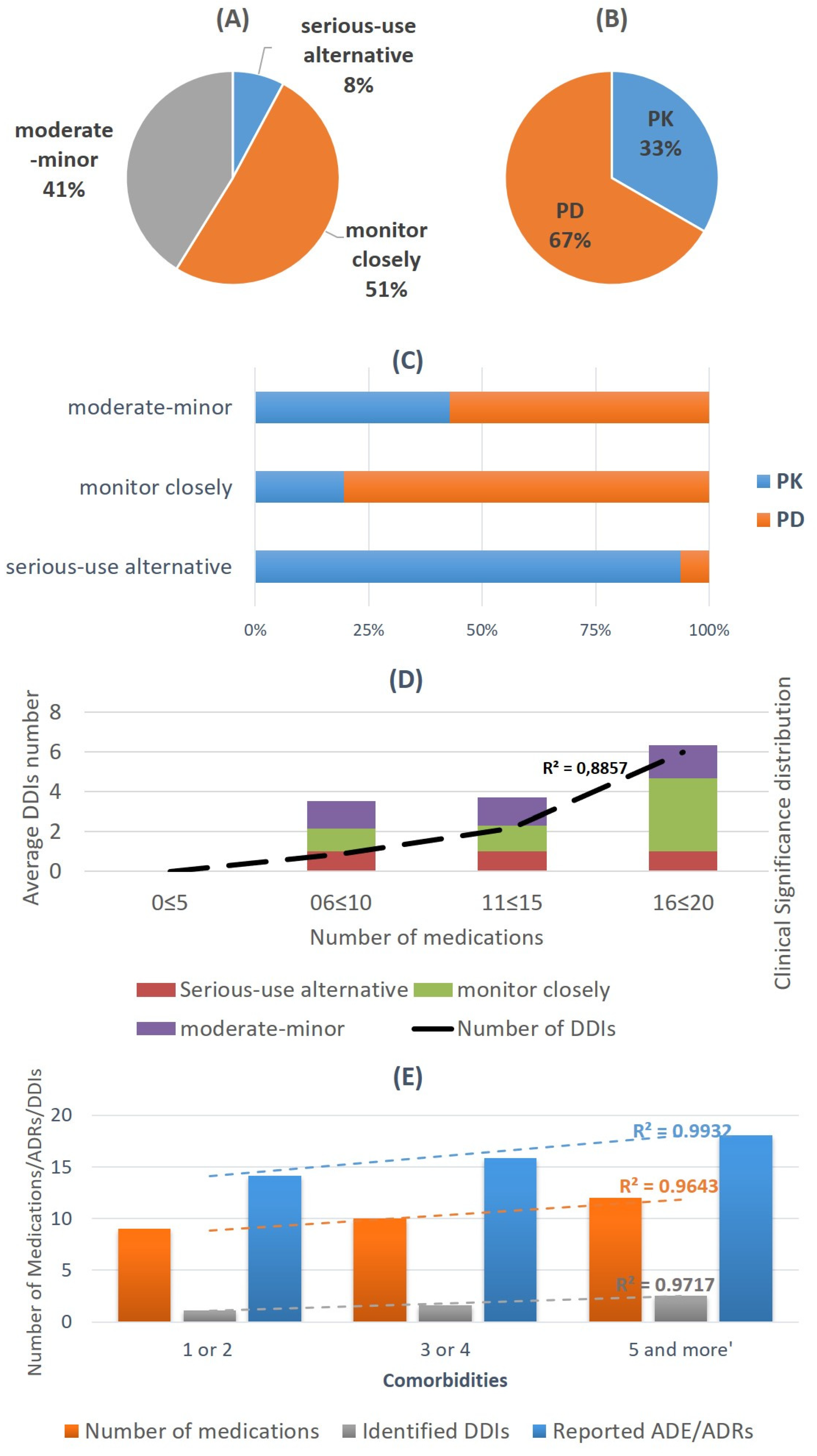
3.2. Drug Categories and Drug–Drug Interactions
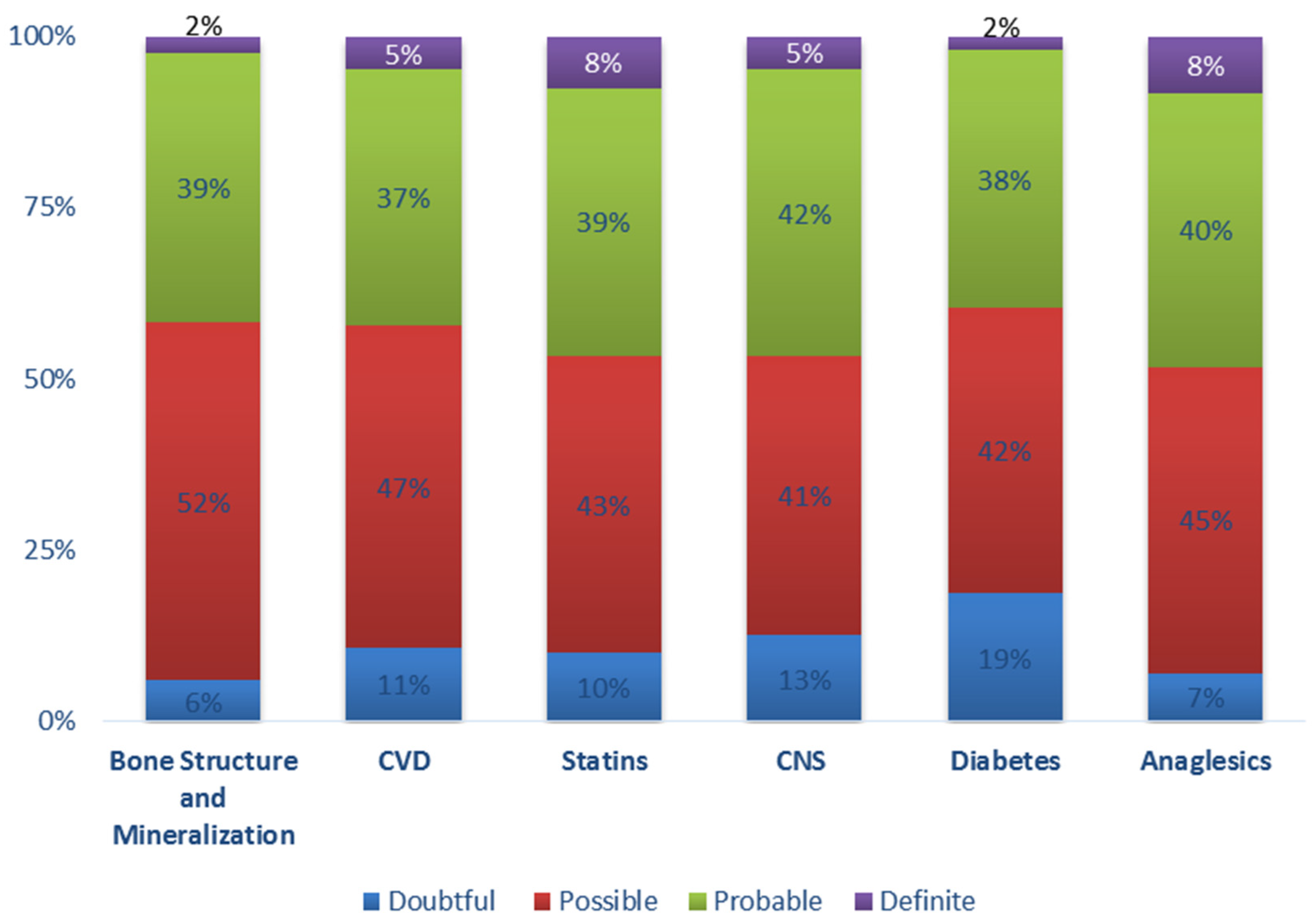
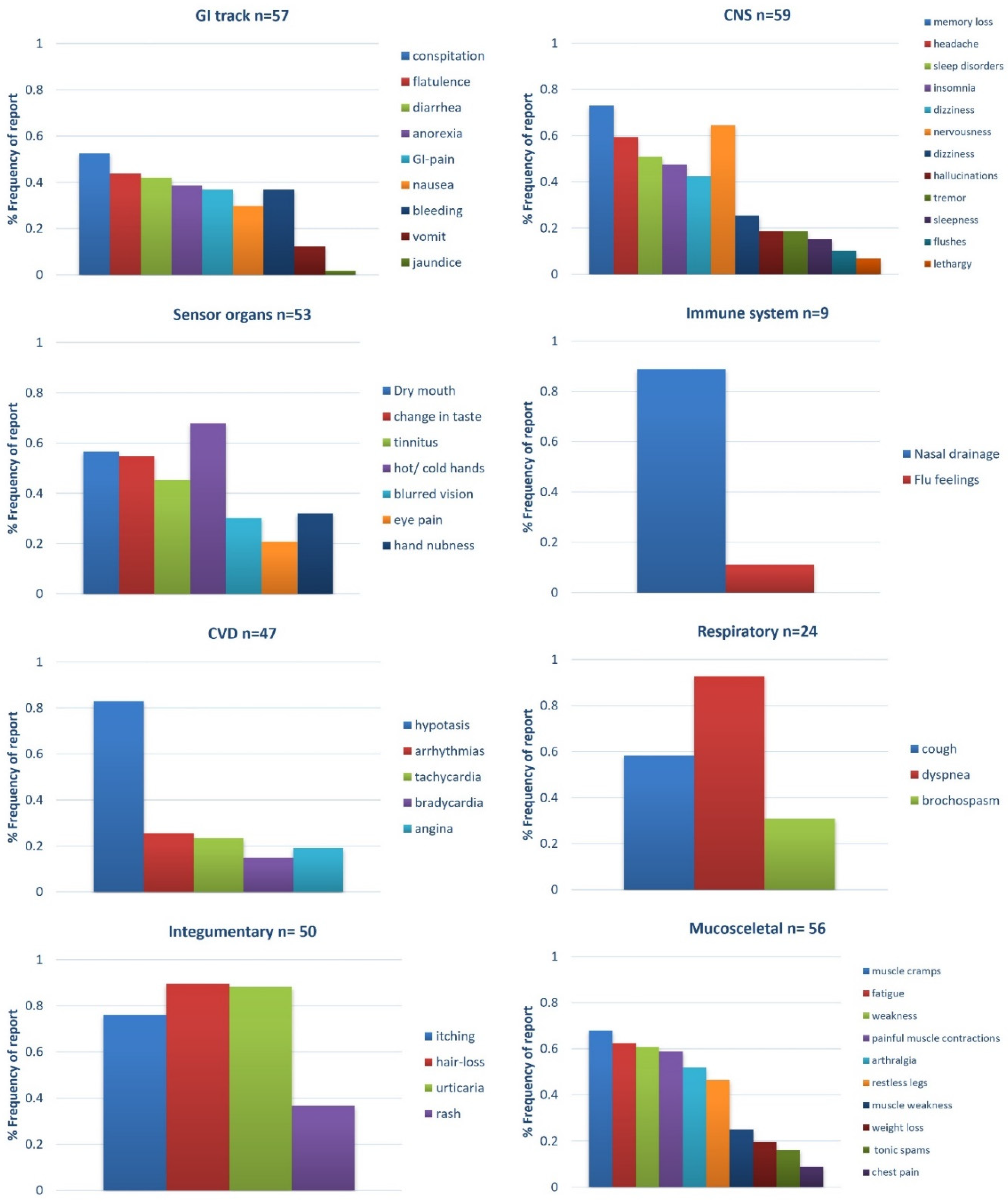
3.3. ADE/ADRs Recorded
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Carney, E.F. The impact of chronic kidney disease on global health. Nat. Rev. Nephrol. 2020, 16, 251. [Google Scholar] [CrossRef] [Green Version]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Breyer, M.D.; Susztak, K. The next generation of therapeutics for chronic kidney disease. Nat. Rev. Drug Discov. 2016, 15, 568–588. [Google Scholar] [CrossRef] [Green Version]
- Seckinger, J.; Dschietzig, W.; Leimenstoll, G.; Rob, P.M.; Kuhlmann, M.K.; Pommer, W.; Fraass, U.; Ritz, E.; Schwenger, V. Morbidity, mortality and quality of life in the ageing haemodialysis population: Results from the ELDERLY study. Clin. Kidney J. 2016, 9, 839–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sombolos, K.; Tsakiris, D.; Boletis, J.; Vlahakos, D.; Siamopoulos, K.C.; Vargemezis, V.; Nikolaidis, P.; Iatrou, C.; Dafnis, E.; Xynos, K.; et al. Multicenter epidemiological study to assess the population of CKD patients in Greece: Results from the PRESTAR study. PLoS ONE 2014, 9, e112767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lea-Henry, T.N.; Carland, J.E.; Stocker, S.L.; Sevastos, J.; Roberts, D.M. Clinical pharmacokinetics in kidney disease: Fundamental principles. Clin. J. Am. Soc. Nephrol. 2018, 13, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Velenosi, T.J.; Urquhart, B.L. Pharmacokinetic considerations in chronic kidney disease and patients requiring dialysis. Expert Opin. Drug Metab. Toxicol. 2014, 10, 1131–1143. [Google Scholar] [CrossRef] [PubMed]
- Dreisbach, A.W.; Lertora, J.J.L. The effect of chronic renal failure on drug metabolism and transport. Expert Opin. Drug Metab. Toxicol. 2008, 4, 1065–1074. [Google Scholar] [CrossRef] [Green Version]
- Tan, M.L.; Yoshida, K.; Zhao, P.; Zhang, L.; Nolin, T.D.; Piquette-Miller, M.; Galetin, A.; Huang, S.M. Effect of Chronic Kidney Disease on Nonrenal Elimination Pathways: A Systematic Assessment of CYP1A2, CYP2C8, CYP2C9, CYP2C19, and OATP. Clin. Pharmacol. Ther. 2018, 103, 854–867. [Google Scholar] [CrossRef]
- Roberts, D.M.; Sevastos, J.; Carland, J.E.; Stocker, S.L.; Lea-Henry, T.N. Clinical pharmacokinetics in kidney disease application to rational design of dosing regimens. Clin. J. Am. Soc. Nephrol. 2018, 13, 1254–1263. [Google Scholar] [CrossRef]
- Weir, M.R.; Fink, J.C. Safety of medical therapy in patients with chronic kidney disease and end-stage renal disease. Curr. Opin. Nephrol. Hypertens. 2014, 23, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulou, A.; Dourakis, S.P.; Mantzoukis, D.; Pitsariotis, T.; Kandyli, A.; Deutsch, M.; Archimandritis, A.J. Adverse drug reactions as a cause of hospital admissions: A 6-month experience in a single center in Greece. Eur. J. Intern. Med. 2008, 19, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Leporini, C.; De Sarro, G.; Russo, E. Adherence to therapy and adverse drug reactions: Is there a link? Expert Opin. Drug Saf. 2014, 13, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Hsu, K.L.; Fink, J.C.; Ginsberg, J.S.; Yoffe, M.; Zhan, M.; Fink, W.; Woods, C.M.; Diamantidis, C.J. Self-reported medication adherence and adverse patient safety events in CKD. Am. J. Kidney Dis. 2015, 66, 621–629. [Google Scholar] [CrossRef] [Green Version]
- Laville, S.M.; Gras-Champel, V.; Moragny, J.; Metzger, M.; Jacquelinet, C.; Combe, C.; Fouque, D.; Laville, M.; Frimat, L.; Robinson, B.M.; et al. Adverse Drug Reactions in Patients with CKD. Clin. J. Am. Soc. Nephrol. 2020, 15, 1090–1102. [Google Scholar] [CrossRef]
- Chapin, E.; Zhan, M.; Hsu, V.D.; Seliger, S.L.; Walker, L.D.; Fink, J.C. Adverse safety events in chronic kidney disease: The frequency of “Multiple Hits”. Clin. J. Am. Soc. Nephrol. 2010, 5, 95–101. [Google Scholar] [CrossRef]
- Tonelli, M.; Wiebe, N.; Guthrie, B.; James, M.T.; Quan, H.; Fortin, M.; Klarenbach, S.W.; Sargious, P.; Straus, S.; Lewanczuk, R.; et al. Comorbidity as a driver of adverse outcomes in people with chronic kidney disease. Kidney Int. 2015, 88, 859–866. [Google Scholar] [CrossRef] [Green Version]
- Marquito, A.B.; Fernandes, N.M.d.S.; Colugnati, F.A.B.; de Paula, R.B. Identifying potential drug interactions in chronic kidney disease patients. J. Bras. Nefrol. Orgão Of. Soc. Bras. Latino Am. Nefrol. 2014, 36, 26–34. [Google Scholar] [CrossRef]
- Rama, M.; Viswanathan, G.; Acharya, L.D.; Attur, R.P.; Reddy, P.N.; Raghavan, S. Assessment of drug-drug interactions among renal failure patients of nephrology ward in a south Indian tertiary care hospital. Indian J. Pharm. Sci. 2012, 74, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Nagasawa, H.; Tachi, T.; Sugita, I.; Esaki, H.; Yoshida, A.; Kanematsu, Y.; Noguchi, Y.; Kobayashi, Y.; Ichikawa, E.; Tsuchiya, T.; et al. The effect of quality of life on medication compliance among dialysis patients. Front. Pharmacol. 2018, 9, 488. [Google Scholar] [CrossRef] [Green Version]
- Offurum, A.; Wagner, L.A.; Gooden, T. Adverse safety events in patients with Chronic Kidney Disease (CKD). Expert Opin. Drug Saf. 2016, 15, 1597–1607. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, J.S.; Zhan, M.; Diamantidis, C.J.; Woods, C.; Chen, J.; Fink, J.C. Patient-reported and actionable safety events in CKD. J. Am. Soc. Nephrol. 2014, 25, 1564–1573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alikari, V.; Matziou, V.; Tsironi, M.; Kollia, N.; Theofilou, P.; Aroni, A.; Fradelos, E.; Zyga, S. A modified version of the Greek Simplified Medication Adherence Questionnaire for hemodialysis patients. Heal. Psychol. Res. 2017, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghimire, S.; Castelino, R.L.; Lioufas, N.M.; Peterson, G.M.; Zaidi, S.T.R. Nonadherence to medication therapy in haemodialysis patients: A systematic review. PLoS ONE 2015, 10, e0144119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trifirò, G.; Patadia, V.; Schuemie, M.J.; Coloma, P.M.; Gini, R.; Herings, R.; Hippisley-Cox, J.; Mazzaglia, G.; Giaquinto, C.; Scotti, L.; et al. EU-ADR healthcare database network vs. spontaneous reporting system database: Preliminary comparison of signal detection. Stud. Health Technol. Inform. 2011, 166, 25–30. [Google Scholar] [PubMed]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef] [Green Version]
- European Parliament and Council of the European Union: GDPR Regulation (EU) 2016/679 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data (General Data Protection Regulation—GDPR). Int. Eur. Labour Law 2018, 958–981.
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Adverse Drug Reaction Probability Scale (Naranjo) in Drug Induced Liver Injury. [Updated 2019 May 4]. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK548069/ (accessed on 8 October 2020).
- Medscape Reference Online Drug Interaction Checker [database on the Internet] New York, NY, USA: WebMD LLC; 2013. Available online: http://reference.medscape.com/drug-interactionchecker (accessed on 8 October 2020).
- Drug Interactions Checker—For Drugs, Food & Alcohol. Available online: https://www.drugs.com/drug_interactions.html (accessed on 5 October 2020).
- Alshamrani, M.; Almalki, A.; Qureshi, M.; Yusuf, O.; Ismail, S. Polypharmacy and Medication-Related Problems in Hemodialysis Patients: A Call for Deprescribing. Pharmacy 2018, 6, 76. [Google Scholar] [CrossRef] [Green Version]
- Alba, M.M.; Citarelli, A.N.; Menni, F.; Agricola, M.; Braicovich, A.; De Horta, E.; De Rosa, F.; Filanino, G.; Gaggiotti, R.; Junqueras, N.; et al. Tobacco and end stage renal disease: A multicenter, cross-sectional study in Argentinian Northern Patagonia. Tob. Induc. Dis. 2015, 13, 28. [Google Scholar] [CrossRef] [Green Version]
- Park, J.M.; Lee, J.H.; Jang, H.M.; Park, Y.; Kim, Y.S.; Kang, S.W.; Yang, C.W.; Kim, N.H.; Kwon, E.; Kim, H.J.; et al. Survival in patients on hemodialysis: Effect of gender according to body mass index and creatinine. PLoS ONE 2018, 13, e0196550. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.-C.; Lee, Y.-T.; Li, L.-C.; Ng, H.-Y.; Kuo, W.-H.; Lin, P.-T.; Liao, Y.-C.; Chiou, T.; Lee, C.-T. The Number of Comorbidities Predicts Renal Outcomes in Patients with Stage 3–5 Chronic Kidney Disease. J. Clin. Med. 2018, 7, 493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.; Li, X.-C.; Lu, L.; Cao, Y.; Sun, R.-R.; Chen, S.; Zhang, P.-Y. Cardiovascular disease and its relationship with chronic kidney disease. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 2918–2926. [Google Scholar] [PubMed]
- Chatsisvili, A.; Sapounidis, I.; Pavlidou, G.; Zoumpouridou, E.; Karakousis, V.-A.; Spanakis, M.; Teperikidis, L.; Niopas, I. Potential drug-drug interactions in prescriptions dispensed in community pharmacies in Greece. Pharm. World Sci. 2010, 32, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, B.; Makubate, B.; Hernandez-Santiago, V.; Dreischulte, T. The rising tide of polypharmacy and drug-drug interactions: Population database analysis 1995–2010. BMC Med. 2015, 13, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, N.R.C.; Hasinoff, B.B.; Stalts, H.; Rao, B.; Wong, N.C.W. Ferrous sulfate reduces thyroxine efficacy in patients with hypothyroidism. Ann. Intern. Med. 1992, 117, 1010–1013. [Google Scholar] [CrossRef] [PubMed]
- Sirtori, C.R. The pharmacology of statins. Pharmacol. Res. 2014, 88, 3–11. [Google Scholar] [CrossRef]
- Di Stasi, S.L.; MacLeod, T.D.; Winters, J.D.; Binder-Macleod, S.A. Effects of statins on skeletal muscle: A perspective for physical therapists. Phys. Ther. 2010, 90, 1530–1542. [Google Scholar] [CrossRef] [Green Version]
- Wyne, A.; Rai, R.; Cuerden, M.; Clark, W.F.; Suri, R.S. Opioid and benzodiazepine use in end-stage renal disease: A systematic review. Clin. J. Am. Soc. Nephrol. 2011, 6, 326–333. [Google Scholar] [CrossRef] [Green Version]
- Schmith, V.D.; Piraino, B.; Smith, R.B.; Kroboth, P.D. Alprazolam in end-stage renal disease. II. Pharmacodynamics. Clin. Pharmacol. Ther. 1992, 51, 533–540. [Google Scholar] [CrossRef]
- Al-Ramahi, R.; Raddad, A.R.; Rashed, A.O.; Bsharat, A.; Abu-Ghazaleh, D.; Yasin, E.; Shehab, O. Evaluation of potential drug- drug interactions among Palestinian hemodialysis patients. BMC Nephrol. 2016, 17, 96. [Google Scholar] [CrossRef] [Green Version]
- Fasipe, O.J.; Akhideno, P.E.; Nwaiwu, O.; Adelosoye, A.A. Assessment of prescribed medications and pattern of distribution for potential drug-drug interactions among chronic kidney disease patients attending the nephrology clinic of lagos university teaching hospital in sub-saharan West Africa. Clin. Pharmacol. Adv. Appl. 2017, 9, 125–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakraborty, S.; Ghosh, S.; Banerjea, A.; De, R.; Hazra, A.; Mandal, S. Prescribing patterns of medicines in chronic kidney disease patients on maintenance hemodialysis. Indian J. Pharmacol. 2016, 48, 586–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, A.M. Cognitive Impairment in the Aging Dialysis and Chronic Kidney Disease Populations: An Occult Burden. Adv. Chronic Kidney Dis. 2008, 15, 123–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gozubatik-Celik, G.; Uluduz, D.; Goksan, B.; Akkaya, N.; Sohtaoglu, M.; Uygunoglu, U.; Kircelli, F.; Sezen, A.; Saip, S.; Karaali Savrun, F.; et al. Hemodialysis-related headache and how to prevent it. Eur. J. Neurol. 2019, 26, 100–105. [Google Scholar] [CrossRef] [Green Version]
- Hamzi, M.A.; Hassani, K.; Asseraji, M.; El Kabbaj, D. Insomnia in hemodialysis patients: A multicenter study from morocco. Saudi J. Kidney Dis. Transpl. 2017, 28, 1112–1118. [Google Scholar] [CrossRef]
- Koiwa, F.; Yokoyama, K.; Fukagawa, M.; Terao, A.; Akizawa, T. Efficacy and safety of sucroferric oxyhydroxide compared with sevelamer hydrochloride in Japanese haemodialysis patients with hyperphosphataemia: A randomized, open-label, multicentre, 12-week phase III study. Nephrology 2017, 22, 293–300. [Google Scholar] [CrossRef] [Green Version]
- Van Der Borg, W.E.; Schipper, K.; Abma, T.A. Protocol of a mixed method, randomized controlled study to assess the efficacy of a psychosocial intervention to reduce fatigue in patients with End-Stage Renal Disease (ESRD). BMC Nephrol. 2016, 17, 73. [Google Scholar] [CrossRef] [Green Version]
- Weisshaar, E.; Weiss, M.; Passlick-Deetjen, J.; Tschulena, U.; Maleki, K.; Mettang, T. Laboratory and dialysis characteristics in hemodialysis patients suffering from chronic itch—Results from a representative cross-sectional study. BMC Nephrol. 2015, 16, 184. [Google Scholar] [CrossRef] [Green Version]
- Ozkan, G.; Ulusoy, S. Bleeding Diathesis in Hemodialysis Patients. In Hemodialysis; IntechOpen Limited: London, UK, 2013; Available online: https://www.intechopen.com/books/hemodialysis/bleeding-diathesis-in-hemodialysis-patients (accessed on 8 October 2020).
- Spanakis, M.; Patelarou, A.E.; Patelarou, E. Nursing Personnel in the Era of Personalized Healthcare in Clinical Practice. J. Pers. Med. 2020, 10, 56. [Google Scholar] [CrossRef]
- Spanakis, M.; Sfakianakis, S.; Spanakis, E.G.; Kallergis, G.; Sakkalis, V. PDCA: An eHealth service for the management of drug interactions with complementary and alternative medicines. In Proceedings of the 2018 IEEE EMBS International Conference on Biomedical and Health Informatics, BHI 2018, Las Vegas, NV, USA, 4–7 March 2018; Volume 2018-Janua. Available online: https://0-ieeexplore-ieee-org.brum.beds.ac.uk/abstract/document/8333446/ (accessed on 8 October 2020).
- Spanakis, M.; Sfakianakis, S.; Kallergis, G.; Spanakis, E.G.; Sakkalis, V. PharmActa: Personalized pharmaceutical care eHealth platform for patients and pharmacists. J. Biomed. Inform. 2019, 100, 103336. [Google Scholar] [CrossRef]
- Shalviri, G.; Mohebbi, N.; Mirbaha, F.; Majdzadeh, R.; Yazdizadeh, B.; Gholami, K. Improving adverse drug event reporting by health care professionals. Cochrane Database Syst. Rev. 2017, 2017. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Methods | |
|---|---|
| Study design | Analysis of DDIs 1 and ADE/ADRs 2 in ESRD 3 patients in Greece |
| Setting | Department of Nephrology of the General Hospital of Chania (GSC), in Crete Greece (6-month data collection). |
| Participants | Patients with ESRD that undergo hemodialysis 3 times per week and signed the informed consent form. |
| Variables | Record of demographic characteristics, comorbidities, medication regiments and laboratory test results; Analyze DDIs and ADE/ADRs as they are reported from the patients. |
| Data sources/measurement | DDIs and clinical significance based on a literature search of relative databases; ADE/ADRs: Greek National formulary of medicines, SOPs and European Medicine Agency (EMA); Naranjo algorithm. |
| Study size | Target population: All ESRD patients of Chania County in prefecture of Crete that visit GSC; Study population: Signed informed consent form to participate. |
| Bias | Diligence in informing the purpose and objectives of the study; Distinct questionnaires, patients were blind to each other; Record of demographics and medication (questionnaire No. 1); ADE/ADRs feedback (questionnaire No. 2); ADE/ADRs together without information if they are ESRD-related or specific-drug-related. |
| Results | |
| Participants | 60 ESRD patients that signed informed consent form (95% of total ESRD patients in the clinic, with 100% follow-up for the two questionnaires). |
| Descriptive data | 68.3% male and 31.7% female, mean age 64.9 years (51.7% elders > 65 years); Average years with ESRD: 4 years; Average medications: 10 per patient. |
| Outcome data | Comorbidities: Hypertension, Cardiovascular Disease and Diabetes; DDIs: 50 co-administered drug combinations (1–2 DDIs per patient), 8% of serious clinical significance; ADE/ADRs: average 16 ADE/ADRs. CNS-, GI-track- and Musculoskeletal-system-related ADE/ADRs were most often reported. |
| Main results | ADE/ADRs as clinical outcome from DDIs reported back in 64% of the total identified DDIs; 93% of reported ADE/ADRs are related with CNS, GI-track and musculoskeletal system; ADE/ADRs that are observed in ESRD can be also related to disease state in some cases. |
| Organ System | ADE/ADRs |
|---|---|
| Sensor organs (general) | change/loss of taste, tinnitus, blurred vision, dry mouth, eye pain, feeling of heat/cold (hands/feet), feeling of discomfort, hand numbness. |
| Respiratory | cough, bronchospasm, dyspnea, shortness of breath. |
| Gastro-Intestinal (GI) track | anorexia, diarrhea, vomiting, constipation, gastrointestinal bleeding, intestinal bleeding, weight loss, abdominal pain, flatulence, nausea, jaundice. |
| Immune | nasal drainage, flu feelings. |
| Integumentary system | rashes, itching, urticaria, hair loss. |
| Musculoskeletal system | weakness, restless legs, chest pain, painful muscle contractions, fatigue, myalgia, muscle weakness, arthralgia, tonic spasms, muscle cramps, trembling, weight loss. |
| Cardiovascular | arrhythmia, tachycardia, bradycardia, hypotension, hypertension. |
| Central Nervous System (CNS) | memory loss, insomnia, sleep disturbances, dizziness, vertigo, headache, lethargy, nervousness, drowsiness, hallucinations, nervousness, heat flushing, chills. |
| Demographics | Male (%) | Female (%) | Total (%) |
|---|---|---|---|
| Gender | 41 (68.3%) | 19 (21.7%) | 60 |
| Age (>65) (elder) | 24 (77.4%) | 7 (22.6%) | 29 (48.3%) |
| Age (≤65) (adults) | 17 (58.6%) | 12 (41.4%) | 31 (51.7%) |
| Physical characteristics | Height (meter ± SD) 1 | Body weight/Dry weight (kg ± SD) | BMI 2 (kg/m2 ± SD) & BMI dry weight |
| 1.7 ± 0.1 | 88.4 ± 20.4/76 ± 17.8 | 30.6 ± 5.6 & 25.5 ± 3.4 | |
| Educational attainment | Primary | High School | University or higher |
| 28 (46.6%) | 19 (31.6%) | 13 (21.6%) | |
| Socio-economic status | Low | Basic | Average-high |
| 6 (10%) | 29 (48.3%) | 25 (41.6%) | |
| Residence area | Urban | Suburban | Rural |
| 26 (43.3%) | 17 (28.3%) | 17 (28.3) | |
| Family status | Married | Single | Widowed/Divorced |
| 43 (71.6%) | 10 (16.7%) | 7 (11.6%) | |
| Lifestyle | Smoking (%) | Alcohol | Coffee |
| 22 (36.7%) | 5 (8.3%) | 37 (61.7%) | |
| Lab test results (mean ± SD) | |||
| Urea mg/dL | 128.9 ± 28.1 (before dialysis); 34.7 ± 13.4 (after dialysis) | ||
| Creatinine mg/dL | 9.1 ± 1.9 (before dialysis); 3.4 ± 1.0 (after dialysis) | ||
| KCl mEq/L | 5.3 ± 0.7 (before dialysis); 3.6 ± 0.7 (after dialysis) | ||
| SGOT IU/L | 14.1 ± 4.7 | ||
| SGPT IU/L | 14.3 ± 6.0 | ||
| γGT IU/L | 24.0 ± 28.3 | ||
| Hemoglobin g/dL | 11.6 ± 1.8 | ||
| Hematocrit % | 36.4 ± 4.2 | ||
| CaCl mg/dL | 9.1 ± 1.0 | ||
| Phosphate ng/mL | 5.3 ± 1.7 | ||
| Ferritin ng/mL | 462.9 ± 242.2 | ||
| Combination | Drug A | Drug B | Type | Mechanism | Drug Affected | Result | Significance | Report Relative ADE/ADR (No. of Patients) |
|---|---|---|---|---|---|---|---|---|
| 1 | sucroferric oxyhydroxide | levothyroxine | PK 1 | GI 3 absorption | levothyroxine | reduced F 4 | Serious | YES (7/11) |
| 2 | amiodarone | carvedilol | PD 2 | Synergism | both | bradycardia | monitor | YES (2/2) |
| 3 | amiodarone | acenocoumarol | PD | synergism | acenocoumarol | INR 5 increase | moderate | YES (1/1) |
| 4 | nifedipine | atorvastatin | PK | CYP 6 3A4 & Pgp 7 | atorvastatin | statin-ADRs 8 | monitor | YES (1/1) |
| 5 | azithromycin | atorvastatin | PK | CYP3A4 | atorvastatin | statin-ADRs | monitor | YES (1/1) |
| 6 | nifedipine | alprazolam | PK | CYP3A4 | alprazolam | increased action | moderate | YES (1/1) |
| 7 | aspirin | celiprolol | PD | Synergism | both | Increase K+ | moderate | NO (0/1) |
| 8 | aspirin | bemiparin | PD | synergism | both | bleeding | moderate | NO (0/1) |
| 9 | omeprazole | clopidorgrel | PK | CYP2C19 | clopidogrel | ADRs | moderate | YES (2/10) |
| 10 | metronidazole | atorvastatin | PK | CYP3A4 | atorvastatin | statin-ADRs | monitor | YES (1/1) |
| 11 | aspirin | sertraline | PD | platelet-serotonin | both | bleeding | monitor | NO (0/1) |
| 12 | aspirin | insulin | PD | insulin sensitivity | insulin | hypoglycemia | moderate | NO (0/2) |
| 13 | aspirin | carvedilol | PD | prostaglandin synthesis | carvedilol | reduced action | moderate | NO (0/6) |
| 14 | methylprednisolone | levofloxacin | PD | unknown | levofloxacin | tendinitis | monitor | YES (1/1) |
| 15 | methylprednisolone | monofloxacin | PD | unknown | monofloxacin | tendinitis | monitor | YES (0/1) |
| 16 | aspirin | clopidogrel | PD | synergism | both | bleeding | monitor | YES (5/12) |
| 17 | omeprazole | alprazolam | PK | CYP2C19 | alprazolam | PD enhance | moderate | YES (1/1) |
| 18 | fluoxetine | clopidogrel | PK | CYP2C19 | clopidogrel | PD reduction | serious | YES (1/1) |
| 19 | fluoxetine | aspirin | PD | platelet-serotonin | aspirin | PD enhance | monitor | NO (0/1) |
| 20 | fluoxetine | pregabalin | PD | reduced seizure threshold | pregabalin | PD reduction | moderate | NO (0/1) |
| 21 | gabapentin | alprazolam | PD | Synergism | both | PD enhance | monitor | YES (1/1) |
| 22 | alprazolam | codeine | PD | Synergism | both | sedation | moderate | YES (1/1) |
| 23 | sevelamer | ciprofloxacin | PK | GI absorption | ciprofloxacin | PD reduction | moderate | NO (1/1) |
| 24 | omeprazole | ciprofloxacin | PK | GI absorption | ciprofloxacin | PD reduction | moderate | NO (1/1) |
| 25 | aspirin | ciprofloxacin | PD | GABA 9 | ciprofloxacin | CNS 10 ADRs | moderate | YES (1/3) |
| 26 | ticlopidine | codeine | PK | CYP2D6 | codeine | PD reduction | moderate | YES (1/1) |
| 27 | prednisolone | aspirin | PD | increase anti-coagulation | aspirin | PD reduction | moderate | NO (0/2) |
| 28 | aspirin | enoxaparin | PD | Synergism | both | bleeding | moderate | YES (1/3) |
| 29 | alprazolam | pregabalin | PD | Synergism | both | ADRs | monitor | YES (1/1) |
| 30 | prednisolone | fondaparinux | PD | increase anti-coagulation | fondaparinux | bleeding | monitor | NO (0/1) |
| 31 | metoprolol | carvedilol | PD | Synergism | both | PD enhance | Serious | YES (1/1) |
| 32 | aspirin | lornoxicam | PD | Synergism | both | PD enhance | monitor | YES (1/1) |
| 33 | gabapentin | codeine | PD | Synergism | both | PD enhance | monitor | NO (1/1) |
| 34 | levothyroxine | acenocoumarol | PD | Synergism | acenocoumarol | PD enhance | monitor | YES (1/1) |
| 35 | nadroparin | acenocoumarol | PD | Synergism | both | PD enhance | monitor | YES (1/1) |
| 36 | sevelamer | ciprofloxacin | PK | GI absorption | ciprofloxacin | PD reduction | serious | NO (0/3) |
| 37 | calcium carbonate | ciprofloxacin | PK | GI absorption | ciprofloxacin | PD reduction | monitor | NO (0/2) |
| 38 | furosemide | amikacin | PD | Synergism | both | PD enhance | moderate | YES (1/1) |
| 39 | calcium carbonate | levothyroxine | PK | GI absorption | levothyroxine | PD reduction | monitor | NO (0/2) |
| 40 | omeprazole | ciprofloxacin | PK | GI absorption | ciprofloxacin | PD reduction | moderate | NO (0/2) |
| 41 | insulin | ciprofloxacin | PD | glucose homeostasis | insulin | PD-ADRs | monitor | YES (1/2) |
| 42 | cinacalcet | codeine | PK | CYP2D6 | codeine | PD reduction | moderate | YES (1/2) |
| 43 | ciprofloxacin | vildagliptin | PD | Synergism | vildagliptin | PD enhance | monitor | YES (1/1) |
| 44 | tramadol | pregabalin | PD | Synergism | both | PD enhance | monitor | YES (1/1) |
| 45 | azithromycin | nardoparin | PD | increase anti-coagulation | nardoparin | PD enhance | moderate | NO (0/1) |
| 46 | azithromycin | sunitinib | PD | QT-prolongation | sunitinib | PD enhance | monitor | YES (1/1) |
| 47 | fenofibrate | insulin | PD | insulin sensitivity | insulin | hypoglycemia | monitor | NO (0/1) |
| 48 | omeprazole | escitalopram | PK | CYP2C19 | escitalopram | PD-adrs | monitor | YES (1/1) |
| 49 | lornoxicam | escitalopram | PD | Synergism | both | bleeding | moderate | NO (0/1) |
| 49 | clopidogrel | escitalopram | PD | platelet activation | clopidogrel | bleeding | monitor | YES (1/1) |
| 50 | gabapentin | escitalopram | PD | seizure threshold | gabapentin | sedation | monitor | YES (1/1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spanakis, M.; Roubedaki, M.; Tzanakis, I.; Zografakis-Sfakianakis, M.; Patelarou, E.; Patelarou, A. Impact of Adverse Drug Reactions in Patients with End Stage Renal Disease in Greece. Int. J. Environ. Res. Public Health 2020, 17, 9101. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239101
Spanakis M, Roubedaki M, Tzanakis I, Zografakis-Sfakianakis M, Patelarou E, Patelarou A. Impact of Adverse Drug Reactions in Patients with End Stage Renal Disease in Greece. International Journal of Environmental Research and Public Health. 2020; 17(23):9101. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239101
Chicago/Turabian StyleSpanakis, Marios, Marianna Roubedaki, Ioannis Tzanakis, Michail Zografakis-Sfakianakis, Evridiki Patelarou, and Athina Patelarou. 2020. "Impact of Adverse Drug Reactions in Patients with End Stage Renal Disease in Greece" International Journal of Environmental Research and Public Health 17, no. 23: 9101. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239101