Mouthwash Based on Ozonated Olive Oil in Caries Prevention: A Preliminary In-Vitro Study


 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
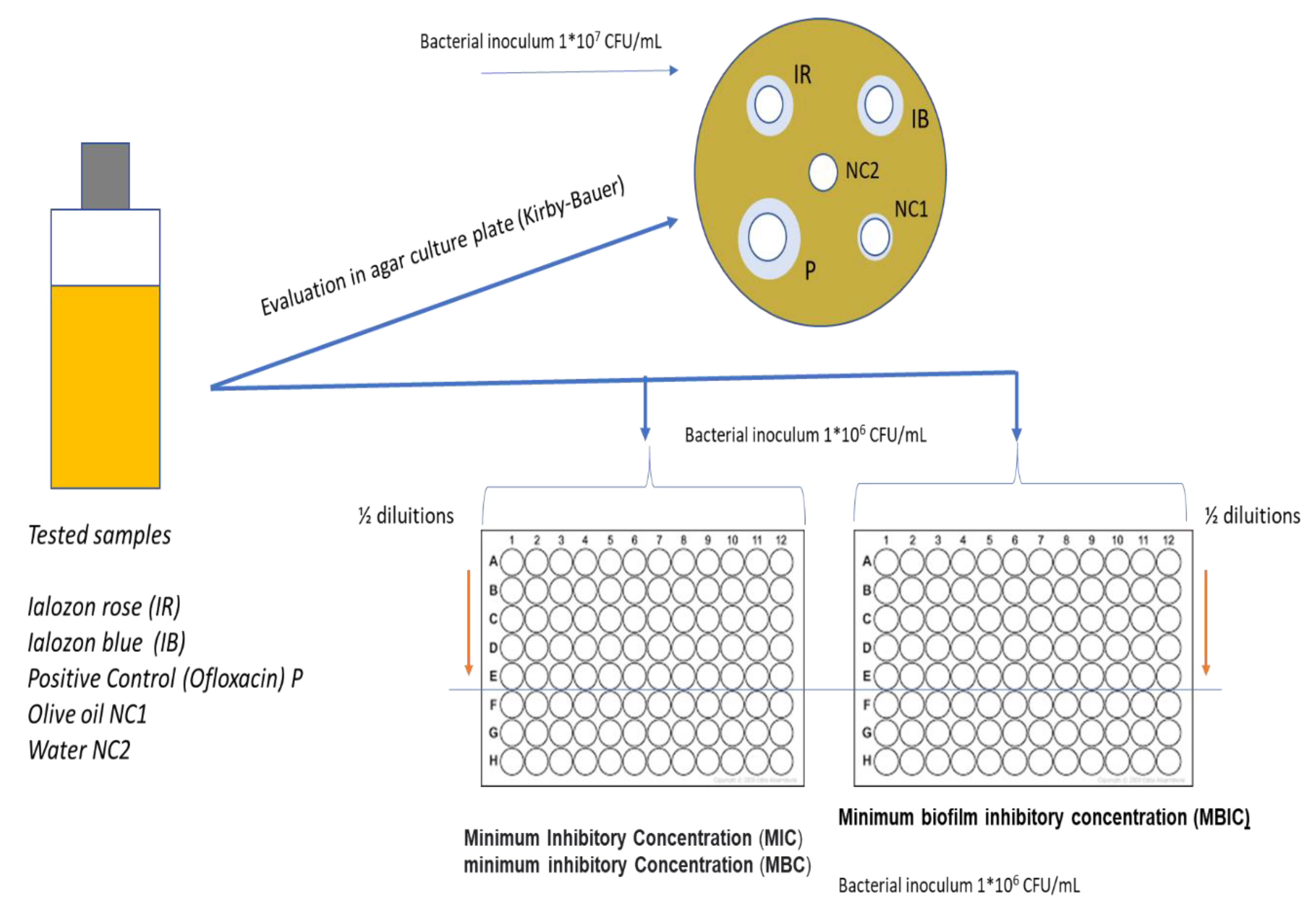
2.1. Study Design
2.2. Olive Oil Ozonated Mouthwashes and Negative Control
2.3. Bacterial Strain and Microbiological Analysis
- Preparation of culture medium with 15 mL of Scheadler-agar medium (Microbiol, Uta, Cagliari) at 55 °C, in a 90 mm diameter Petri dish. The plate was characterized by 1 sterile iron rivet with a diameter of Ø 10 mm and a thickness of 2 mm which was removed after the agar solidification;
- Standardized bacterial inoculum (5 × 107 CFU/mL) was seeded on the surface of the plate using a sterile swab;
- Insertion of the material to be tested: 50 µL of Ialozon mouthwash with different dilution for each dish (ozonated olive oil, Gemavip, Cagliari, Italy) was dispensed through a micropipette;
- Incubation of the plate with S. mutans at 37 °C with 5% CO2 for 24 h;
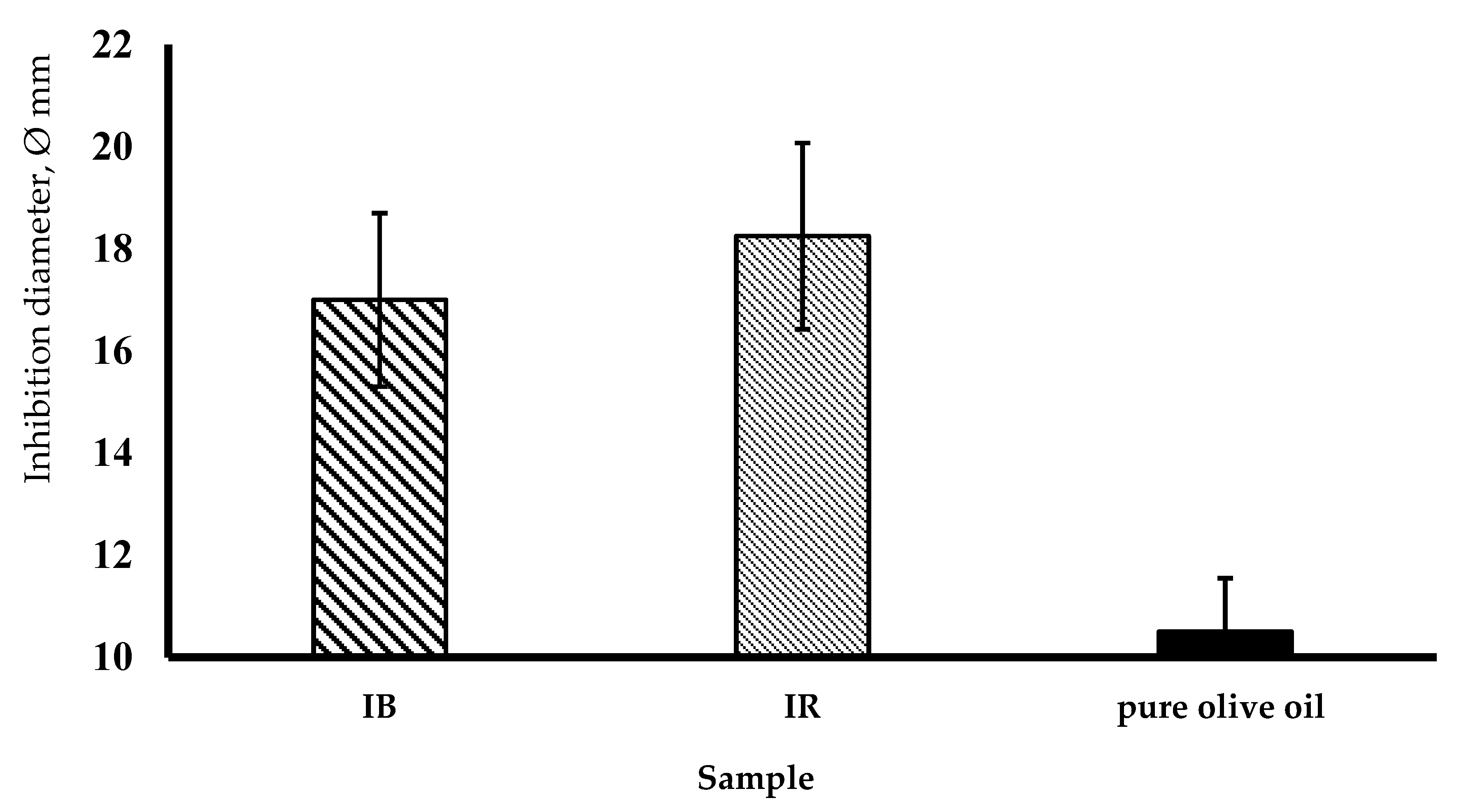
- After incubation, the diameter of the possible zone of inhibition was measured with a caliper for each dish, and dilutions of the tested substances, which determined an inhibition zone greater than 10 mm in diameter, were recorded.
2.4. Statistical Analysis
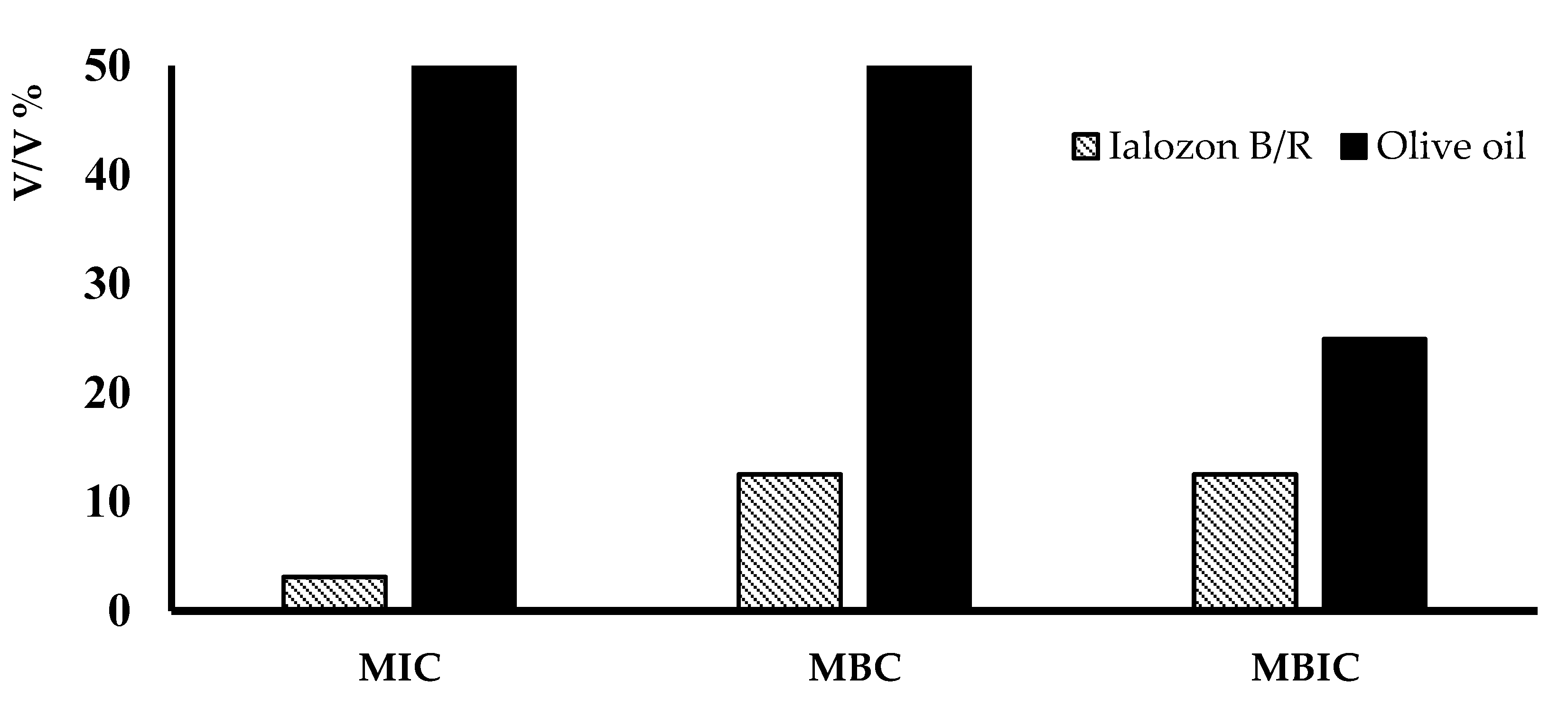
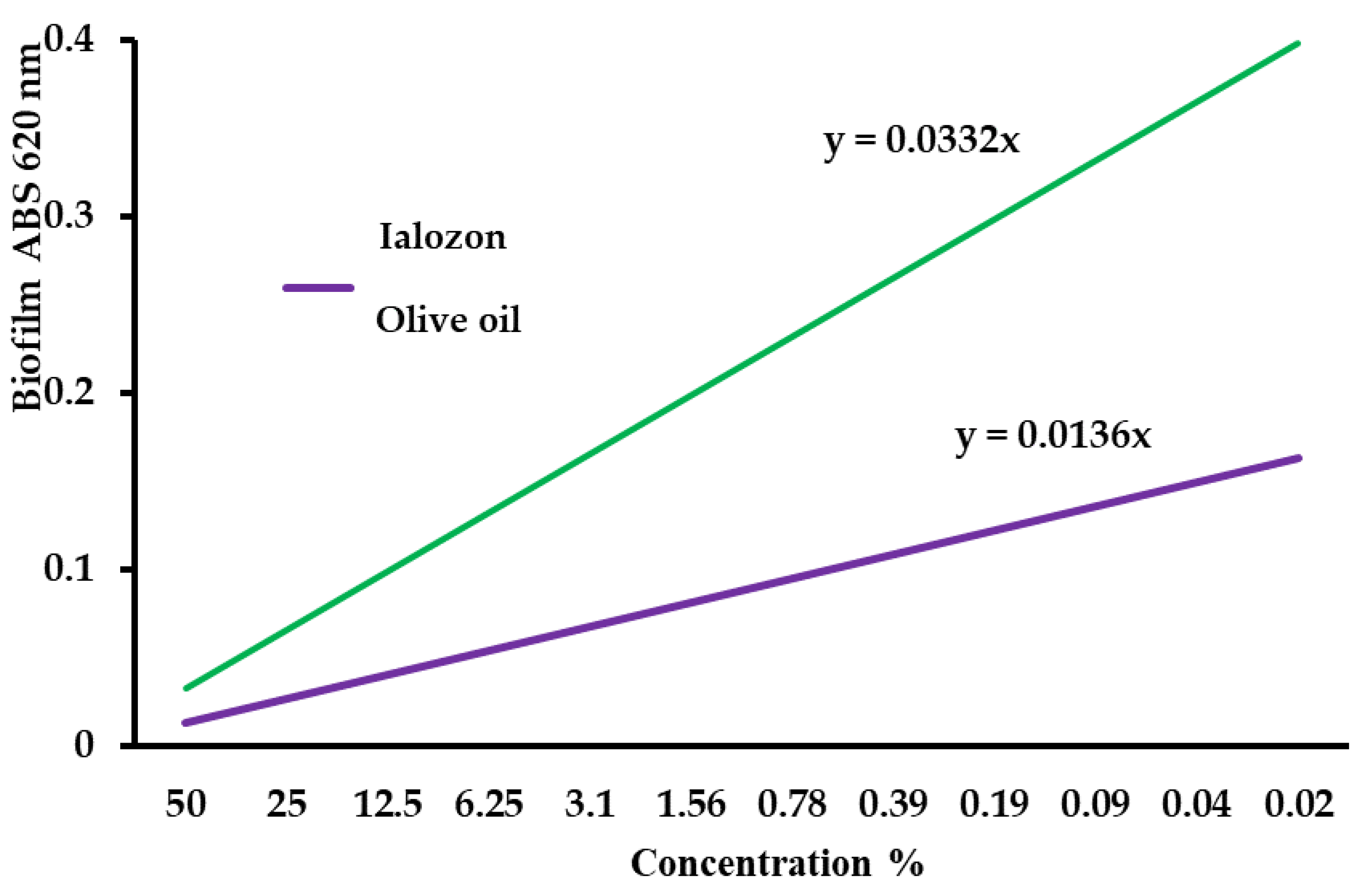
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Links/Footnotes
| CLSI’s Subcommittee on Antimicrobial Susceptibility Testing (AST) | https://clsi.org/meetings/ast/ |
| The European Committee on Antimicrobial Susceptibility Testing—EUCAST | https://eucast.org/ |
| Social Science Statistics web calculator | https://www.socscistatistics.com/tests/studentttest/default2.aspx |
References
- Uysal, B. Ozonated olive oils and the troubles. J. Intercul. Ethnopharmacol. 2014, 3, 49–50. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, Z.; Shalavi, S.; Soltani, M.K.; Asgary, S. A review of the properties and applications of ozone in endodontics: An update. Iran. Endod. J. 2013, 8, 40–43. [Google Scholar] [PubMed]
- Khatri, I.; Moger, G.; Kumar, N.A. Evaluation of effect of topical ozone therapy on salivary Candidal carriage in oral candidiasis. Indian J. Dent. Res. 2015, 26, 158–162. [Google Scholar] [PubMed]
- Pietrocola, G.; Ceci, M.; Preda, F.; Poggio, C.; Colombo, M. Evaluation of the antibacterial activity of a new ozonized olive oil against oral and periodontal pathogens. J. Clin. Exp. Dent. 2018, 10, e1103–e1108. [Google Scholar] [CrossRef] [PubMed]
- Nardi, G.M.; Cesarano, F.; Papa, G.; Chiavistelli, L.; Ardan, R.; Jedlinski, M.; Mazur, M.; Grassi, R.; Grassi, F.R. Evaluation of Salivary Matrix Metalloproteinase (MMP-8) in Periodontal Patients Undergoing Non-Surgical Periodontal Therapy and Mouthwash Based on Ozonated Olive Oil: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 6619. [Google Scholar] [CrossRef] [PubMed]
- Holmes, J. Clinical reversal of root caries using ozone, double-blind, randomized, controlled 18-month trial. Gerodontology 2003, 20, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Baysan, A.; Lynch, E. Effect of ozone on oral microbiota and clinical severity of primary root caries. Am. J. Dent. 2004, 18, 223–228. [Google Scholar]
- Huth, K.C.; Paschos, E.; Brand, K.; Hickel, R. Effect of ozone on non-cavitated fissure carious lesions in permanent molars. A controlled prospective clinical study. Am. J. Dent. 2005, 18, 223–228. [Google Scholar]
- Nagayoshi, M.; Fukuizumi, T.; Kitamura, C.; Yano, J.; Terashita, M.; Nishihara, T. Efficacy of ozone on survival and permeability of oral microorganisms. Oral. Microbiol. Immunol. 2004, 19, 240–246. [Google Scholar] [CrossRef]
- Polydorou, O.; Halili, A.; Wittmer, A.; Pelz, K.; Hahn, P. The antibacterial effect of gas ozone after 2 months of in vitro evaluation. Clin. Oral Investig. 2012, 16, 545–550. [Google Scholar] [CrossRef]
- Patel, P.V.; Patel, A.; Kumar, S.; Holmes, J.C. Effect of subgingival application of topical ozonated olive oil in the treatment of chronic periodontitis: A randomized, controlled, double-blind, clinical and microbiological study. Minerva Stomatol. 2012, 61, 381–398. [Google Scholar] [PubMed]
- Takenaka, S.; Ohsumi, T.; Noiri, Y. Evidence-based strategy for dental biofilms: Current evidence of mouthwashes on dental biofilm and gingivitis. Jpn. Dent. Sci. Rev. 2019, 55, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.V.; Kumar, S.; Vidya, G.D.; Patel, A.; Holmes, J.C.; Kumar, V. Cytological assessment of healing palatal donor site wounds and grafted gingival wounds after application of ozonated oil: An eighteen-month randomized controlled clinical trial. Acta Cytol. 2012, 56, 277–284. [Google Scholar] [CrossRef]
- Patel, P.V.; Kumar, V.; Kumar, S.; Patel, A. Therapeutic effect of topical ozonated oil on the epithelial healing of palatal wound sites: A planimetrical and cytological study. Acta Cytol. 2012, 56, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Barberis, A.; Deiana, M.; Spissu, Y.; Azara, E.; Fadda, A.; Serra, P.A.; D’hallewin, G.; Pisano, M.; Serreli, G.; Orrù, G.; et al. Antioxidant, Antimicrobial, and Other Biological Properties of Pompia Juice. Molecules 2020, 25, 3186. [Google Scholar] [CrossRef] [PubMed]
- Podda, E.; Arca, M.; Atzeni, G.; Coles, S.J.; Ibba, A.; Isaia, F.; Lippolis, V.; Orrù, G.; Orton, J.B.; Pintus, A.; et al. Antibacterial Activity of Amidodithiophosphonato Nickel(II) Complexes: An Experimental and Theoretical Approach. Molecules 2020, 28, 2052. [Google Scholar] [CrossRef]
- Palmas, L.; Aroffu, M.; Petretto, G.L.; Escribano-Ferrer, E.; Díez-Sales, O.; Usach, I.; Peris, J.E.; Marongiu, F.; Ghavam, M.; Fais, S.; et al. Entrapment of Citruslimon var. pompia Essential Oil or Pure Citral in Liposomes Tailored as Mouthwash for the Treatment of Oral Cavity Diseases. Pharmaceuticals 2020, 28, 216. [Google Scholar] [CrossRef]
- Orrù, G.; Demontis, C.; Mameli, A.; Tuveri, E.; Coni, P.; Pichiri, G.; Coghe, F.; Rosa, A.; Rossi, P.; D’hallewin, G. The Selective Interaction of Pistacia lentiscus Oil vs. Human Streptococci, an Old Functional Food Revisited with New Tools. Front. Microbiol. 2017, 24, 2067. [Google Scholar] [CrossRef] [Green Version]
- Forssten, S.D.; Björklund, M.; Ouwehand, A.C.S. mutans, Caries and Simulation Models. Nutrients 2010, 2, 290–298. [Google Scholar] [CrossRef] [Green Version]
- Weatherly, L.M.; Gosse, J.A. Triclosan exposure, transformation, and human health effects. J. Toxicol. Environ. Health B Crit. Rev. 2017, 20, 447–469. [Google Scholar] [CrossRef]
- Almaz, M.E.; Sönmez, I.Ş. Ozone therapy in the management and prevention of caries. J. Formos. Med. Assoc. 2015, 114, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.R.; Shang, G.W.; Hu, L.F.; Wang, X.P.; Huang, W.; Li, M.Y.; Zhu, C.L. The disinfecting effect of ozone on four kinds of bacteria. Shanghai Kou Qiang Yi Xue 2008, 17, 92–95. [Google Scholar] [PubMed]
- Nazzaro, F.; Fratianni, F.; Cozzolino, R.; Martignetti, A.; Malorni, L.; De Feo, V.; Cruz, A.G.; d’Acierno, A. Antibacterial Activity of Three Extra Virgin Olive Oils of the Campania Region, Southern Italy, Related to Their Polyphenol Content and Composition. Microorganisms 2019, 5, 321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, J.N.; Kim, M.A.; Jung, J.E.; Pandit, S.; Song, K.Y.; Jeon, J.G. Effects of combined oleic acid and fluoride at sub-MIC levels on EPS formation and viability of S. mutansUA159 biofilms. Biofouling 2015, 31, 555–563. [Google Scholar] [CrossRef]
- Pan, S.W.; Li, Y.G.; Su, H.; Li, X.; Zhang, Y.B. Oleic acid impedes adhesion of Porphyromonas gingivalis during the early stages of biofilm formation. Int. J. Clin. Exp. Med. 2019, 12, 9881–9889. [Google Scholar]
- Samuel, S.R.; Dorai, S.; Khatri, S.G.; Patil, S.T. Effect of ozone to remineralize initial enamel caries: In situ study. Clin. Oral Investig. 2016, 20, 1109–1113. [Google Scholar] [CrossRef]
- Anumula, L.; Kumar, K.S.; Krishna, C.M.; Lakshmi, K.S. Antibacterial Activity of Freshly Prepared Ozonated Water and Chlorhexidine on Mutans Streptococcus When Used as an Oral Rinse—A Randomised Clinical Study. J. Clin. Diagn. Res. 2017, 11, ZC05–ZC08. [Google Scholar] [CrossRef]
- Ximenes, M.; Cardoso, M.; Astorg, F.; Arnold, R.; Pimenta, L.A.; de Sousa Vieria, R. Antimicrobial activity of ozone and NaF-chlorhexidine on early childhood caries. Braz. Oral Res. 2017, 5, 31:e2. [Google Scholar] [CrossRef] [Green Version]
- Mummolo, S.; Nota, A.; Caruso, S.; Quinzi, V.; Marchetti, E.; Marzo, G. Salivary Markers and Microbial Flora in Mouth Breathing Late Adolescents. BioMed Res. Int. 2018, 5, 8687608. [Google Scholar] [CrossRef]
- Mummolo, S.; Nota, A.; Albani, F.; Marchetti, E.; Gatto, R.; Marzo, G.; Quinzi, V.; Tecco, S. Salivary levels of Streptococcus mutans and Lactobacilli and other salivary indices in patients wearing clear aligners versus fixed orthodontic appliances: An observational study. PLoS ONE 2020, 15, e0228798. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nardi, G.M.; Fais, S.; Casu, C.; Mazur, M.; Di Giorgio, R.; Grassi, R.; Grassi, F.R.; Orrù, G. Mouthwash Based on Ozonated Olive Oil in Caries Prevention: A Preliminary In-Vitro Study. Int. J. Environ. Res. Public Health 2020, 17, 9106. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239106
Nardi GM, Fais S, Casu C, Mazur M, Di Giorgio R, Grassi R, Grassi FR, Orrù G. Mouthwash Based on Ozonated Olive Oil in Caries Prevention: A Preliminary In-Vitro Study. International Journal of Environmental Research and Public Health. 2020; 17(23):9106. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239106
Chicago/Turabian StyleNardi, Gianna Maria, Sara Fais, Cinzia Casu, Marta Mazur, Roberto Di Giorgio, Roberta Grassi, Felice Roberto Grassi, and Germano Orrù. 2020. "Mouthwash Based on Ozonated Olive Oil in Caries Prevention: A Preliminary In-Vitro Study" International Journal of Environmental Research and Public Health 17, no. 23: 9106. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239106