Adaptations to Swimming Training in Athletes with Down’s Syndrome



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Training Intervention
2.3. Procedure
2.4. Swimming Performance
2.5. Vertical Jump Test
2.6. Body Composition
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sugimoto, D.; Bowen, S.L.; Meehan, W.P.; Stracciolini, A. Effects of Neuromuscular Training on Children and Young Adults with Down Syndrome: Systematic Review and Meta-Analysis. Res. Dev. Disabil. 2016, 55, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Whitt-Glover, M.C.; O’Neill, K.L.; Stettler, N. Physical activity patterns in children with and without Down syndrome. Pediatr. Rehabil. 2006, 9, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Boer, P. The effect of 8 weeks of freestyle swim training on the functional fitness of adults with Down syndrome. J. Intellect. Disabil. Res. 2020, 64, 770–781. [Google Scholar] [CrossRef] [PubMed]
- Ordonez, F.J.; Rosety, M.; Rosety-Rodríguez, M. Ángel Influence of 12-week exercise training on fat mass percentage in adolescents with Down syndrome. Med. Sci. Monit. 2006, 12, CR416-9. [Google Scholar]
- Boer, P.; De Beer, Z. The effect of aquatic exercises on the physical and functional fitness of adults with Down syndrome: A non-randomised controlled trial. J. Intellect. Disabil. Res. 2019, 63, 1453–1463. [Google Scholar] [CrossRef]
- Shields, N.; Taylor, N.F.; Wee, E.; Wollersheim, D.; O’Shea, S.D.; Fernhall, B. A community-based strength training programme increases muscle strength and physical activity in young people with Down syndrome: A randomised controlled trial. Res. Dev. Disabil. 2013, 34, 4385–4394. [Google Scholar] [CrossRef]
- Shields, N.; Hussey, J.; Murphy, J.; Gormley, J.; Hoey, H. An exploratory study of the association between physical activity, cardiovascular fitness and body size in children with Down syndrome. Dev. Neurorehabilit. 2015, 20, 1–7. [Google Scholar] [CrossRef]
- Shields, N.; Taylor, N.F.; Dodd, K. Effects of a Community-Based Progressive Resistance Training Program on Muscle Performance and Physical Function in Adults with Down Syndrome: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2008, 89, 1215–1220. [Google Scholar] [CrossRef]
- Cowley, P.M.; Ploutz-Snyder, L.L.; Baynard, T.; Heffernan, K.S.; Jae, S.Y.; Hsu, S.; Lee, M.; Pitetti, K.H.; Reiman, M.P.; Fernhall, B. The effect of progressive resistance training on leg strength, aerobic capacity and functional tasks of daily living in persons with Down syndrome. Disabil. Rehabil. 2011, 33, 2229–2236. [Google Scholar] [CrossRef]
- Ruiz-González, L.; Lucena-Anton, D.; Salazar, A.; Martín-Valero, R.; Moral-Munoz, J.A. Physical therapy in Down syndrome: Systematic review and meta-analysis. J. Intellect. Disabil. Res. 2019, 63, 1041–1067. [Google Scholar] [CrossRef] [Green Version]
- Bompa, T.O.; Haff, G.G. Periodization: Theory and Methodology of Training; Human Kinetics: Champaign, IL, USA, 1999. [Google Scholar]
- Pollock, S.; Gaoua, N.; Johnston, M.J.; Cooke, K.; Girard, O.; Mileva, K.N. Training Regimes and Recovery Monitoring Practices of Elite British Swimmers. J. Sports Sci. Med. 2019, 18, 577–585. [Google Scholar] [PubMed]
- Tate, A.; Harrington, S.; Buness, M.; Murray, S.; Trout, C.; Meisel, C. Investigation of In-Water and Dry-Land Training Programs for Competitive Swimmers in the United States. J. Sport Rehabil. 2014, 24, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Seiler, S. What is Best Practice for Training Intensity and Duration Distribution in Endurance Athletes? Int. J. Sports Physiol. Perform. 2010, 5, 276–291. [Google Scholar] [CrossRef] [PubMed]
- Seiler, K.S.; Kjerland, G.O. Quantifying training intensity distribution in elite endurance athletes: Is there evidence for an "optimal" distribution? Scand. J. Med. Sci. Sports 2006, 16, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Fernhall, B.; Mendonca, G.V.; Baynard, T. Reduced Work Capacity in Individuals with Down Syndrome: A consequence of autonomic dysfunction? Exerc. Sport Sci. Rev. 2013, 41, 138–147. [Google Scholar] [CrossRef]
- Bosco, C.; Luhtanen, P.; Komi, P. A simple method for measurement of mechanical power in jumping. Eur. J. Appl. Physiol. 1983, 50, 273–282. [Google Scholar] [CrossRef]
- Gonzalez-Ravé, J.M.; Juárez, D.; Rubio-Arias, J.Á.; Clemente-Suárez, V.J.; Martinez-Valencia, M.A.; Abián-Vicen, J. Isokinetic Leg Strength and Power in Elite Handball Players. J. Hum. Kinet. 2014, 41, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Malavolti, M.; Mussi, C.; Poli, M.; Fantuzzi, A.L.; Salvioli, G.; Battistini, N.; Bedogni, G. Cross-calibration of eight-polar bioelectrical impedance analysis versus dual-energy X-ray absorptiometry for the assessment of total and appendicular body composition in healthy subjects aged 21–82 years. Ann. Hum. Biol. 2003, 30, 380–391. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Hellard, P.; Avalos-Fernandes, M.; Lefort, G.; Pla, R.; Mujika, I.; Toussaint, J.-F.; Pyne, D.B. Elite Swimmers’ Training Patterns in the 25 Weeks Prior to Their Season’s Best Performances: Insights Into Periodization From a 20-Years Cohort. Front. Physiol. 2019, 10, 363. [Google Scholar] [CrossRef] [Green Version]
- Hellard, P.; Scordia, C.; Avalos, M.; Mujika, I.; Pyne, D.B. Modelling of optimal training load patterns during the 11 weeks preceding major competition in elite swimmers. Appl. Physiol. Nutr. Metab. 2017, 42, 1106–1117. [Google Scholar] [CrossRef] [PubMed]
- Sweetenham, B.; Atkinson, J. Championship Swim Training; Human Kinetics: Champaign, IL, USA, 2003; Volume 1. [Google Scholar]
- Chatard, J.C.; Stewart, A.M. Training load and performance in swimming. In World Book of Swimming: From Science to Performance; Seifert, L., Chollet, D., Mujika, I., Eds.; Nova Science Publishers: New York, NY, USA, 2011. [Google Scholar]
- Morais, J.E.; Balasekaran, G.; Vilas-Boas, J.P.; Barbosa, T.M. Physiological Adaptations to Training in Competitive Swimming: A Systematic Review. J. Hum. Kinet. 2015, 49, 179–194. [Google Scholar] [CrossRef] [Green Version]
- Newton, R.; Jones, J.; Kraemer, W.J.; Wardle, H. Strength and Power Training of Australian Olympic Swimmers. Strength Cond. J. 2002, 24, 7–15. [Google Scholar] [CrossRef]
- Morouço, P.; Marinho, D.A.; Izquierdo, M.; Neiva, H.P.; Marques, M.C. Relative Contribution of Arms and Legs in 30 s Fully Tethered Front Crawl Swimming. BioMed Res. Int. 2015, 2015, 1–6. [Google Scholar] [CrossRef]
- Shafer, K.J.; Siders, W.A.; Johnson, L.K.; Lukaski, H.C. Validity of segmental multiple-frequency bioelectrical impedance analysis to estimate body composition of adults across a range of body mass indexes. Nutrition 2009, 25, 25–32. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Month | February | March | ||||
|---|---|---|---|---|---|---|
| Competition | Baseline Test | C | ||||
| Period | Competitive | Transition | ||||
| Intervention week | 0 | 1 | 2 | 3 | 4 | 5 |
| Week of season | 23 | 24 | 25 | 26 | 27 | 28 |
| DTI (% of total training time) | z1: 87.2 ± 1.2% z2: 6.1 ± 0.7% z3: 6.6 ± 0.9% | z1: 96.3 ± 1.1% z2: 2.2 ± 0.7% z3: 1.5 ± 0.9% | ||||
| Training days/week | 3 | 3 | 3 | 3 | 2 | 2 |
| Daily volume (m) | 1600 | 1000 | 1100 | 1000 | 1500 | 1800 |
| Session duration (h) | 1.5 | 1 | 1.5 | 1 | 1.5 | 1.5 |
| Month | March | April | May | June | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Competition | C | C | C | Post-Test | Main C | |||||||||
| Period | Preparation (Basic) | Preparation (Specific) | Pre-Competitive | Competitive | ||||||||||
| Intervention week | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 |
| Week of season | 29 | 30 | 31 | 32 | 33 | 34 | 35 | 36 | 37 | 38 | 39 | 40 | 41 | 42 |
| DTI (% of total training time) | z1: 90.2 ± 2.2% z2: 6.1 ± 1% z3: 4.3 ± 1% | z1:86.2 ± 2.1% z2: 6.8 ± 0.7% z3: 6.6 ± 0.9% | z1: 82.2 ± 2% z2: 1 ± 2% z3: 8 ± 1% | |||||||||||
| Training days/week | 3 | 2 | 3 | 3 | 3 | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Daily volume (m) | 1500 | 1400 | 1200 | 1800 | 1600 | 1700 | 1400 | 1400 | 1400 | 1500 | 1600 | 1000 | 1100 | 1000 |
| Session duration (h) | 1.5 | 1.2 | 1.5 | 1.5 | 1.5 | 1.5 | 1.5 | 1.5 | 1.2 | 1.2 | 1.2 | 1 | 1.2 | 1 |
| Dependent Variables | Baseline | Post−Training | Mean % Change | p−Value | Cohen’s d |
|---|---|---|---|---|---|
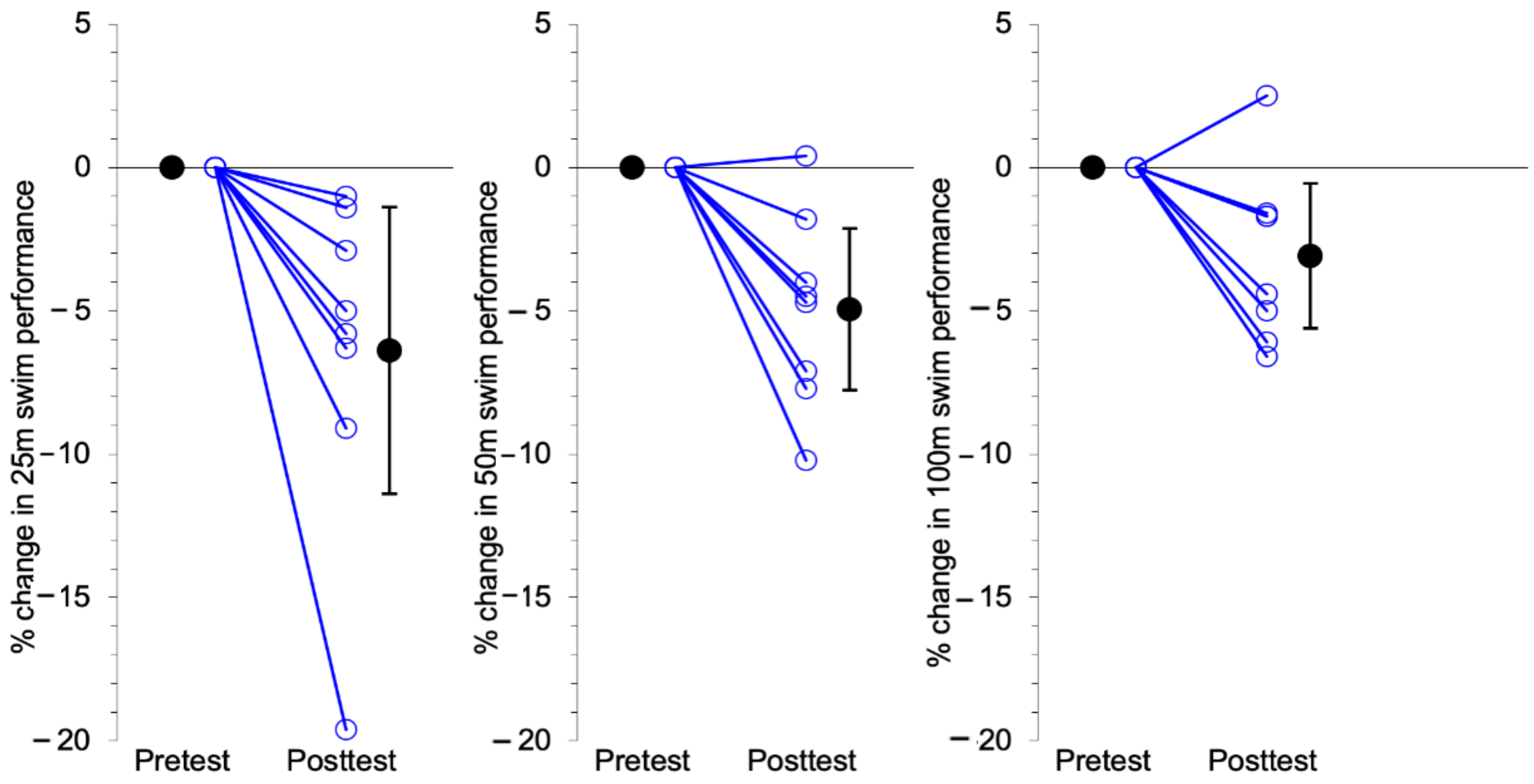
| 25m freestyle time (s) | 29.75 (10.8) | 27.35 (7.9) | −6.39 * | 0.019 | 1.51 |
| 50 m freestyle time (s) | 62.55 (16.49) | 59.5 (16.06) | −4.95 * | 0.004 | 2.08 |
| 100 m freestyle time (s) | 139.48 (57.36) | 135.78 (57.2) | −3.08 * | 0.024 | 1.44 |
| CMJ jump height (cm) | 0.14 (0.03) | 0.15 (0.02) | 8.4 | 0.157 | 0.74 |
| CMJ relative peak force (%BW) | 166.2 (29.5) | 139.3 (24.3) | −14.6 * | 0.031 | 1.23 |
| CMJ mean force (N) | 835.4 (208.1) | 818.8 (250.6) | −2.28 | 0.558 | 0.29 |
| CMJ mean power (W) | 889.9 (100.1) | 855.8 (230.4) | 3.9 | 0.635 | 0.23 |
| Body Mass (kg) | 58.3 (12.2) | 57.9 (11.4) | −0.19 | 0.909 | 0.06 |
| Fat Mass (kg) | 21.7 (10.5) | 21.01 (10.4) | −1.07 | 0.825 | 0.11 |
| Fat−Free Mass (kg) | 19.6 (3.7) | 20.0 (3.5) | 2.4 | 0.144 | 0.76 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Ravé, J.M.; Turner, A.P.; Phillips, S.M. Adaptations to Swimming Training in Athletes with Down’s Syndrome. Int. J. Environ. Res. Public Health 2020, 17, 9175. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249175
González-Ravé JM, Turner AP, Phillips SM. Adaptations to Swimming Training in Athletes with Down’s Syndrome. International Journal of Environmental Research and Public Health. 2020; 17(24):9175. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249175
Chicago/Turabian StyleGonzález-Ravé, José María, Anthony P. Turner, and Shaun M. Phillips. 2020. "Adaptations to Swimming Training in Athletes with Down’s Syndrome" International Journal of Environmental Research and Public Health 17, no. 24: 9175. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249175