The Psychological Impact of ‘Mild Lockdown’ in Japan during the COVID-19 Pandemic: A Nationwide Survey under a Declared State of Emergency

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Data Collection
2.2. Measurements
2.2.1. Psychological Distress
2.2.2. Loneliness and Social Networks
2.2.3. Socio-Demographic Data
2.2.4. Lifestyle, Stress Management, and Stressors Related to Mild Lockdown
2.3. Data Records
2.4. Statistical Analyses
3. Results
3.1. Socio-Demographic Characteristics by Psychological Distress Severity
3.2. Psychometric Characteristics by Psychological Distress Severity
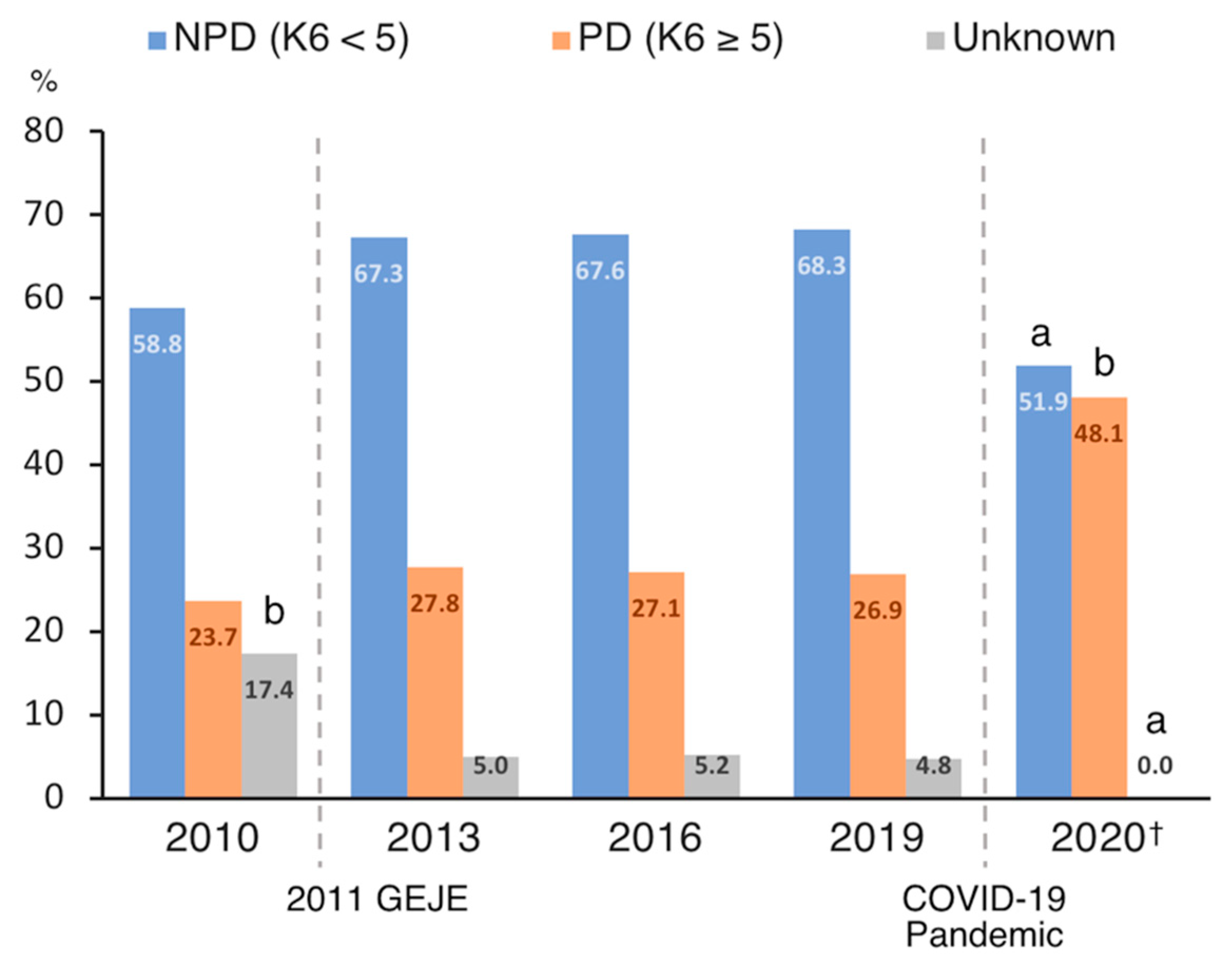
3.3. Chronological Comparison of Psychological Distress
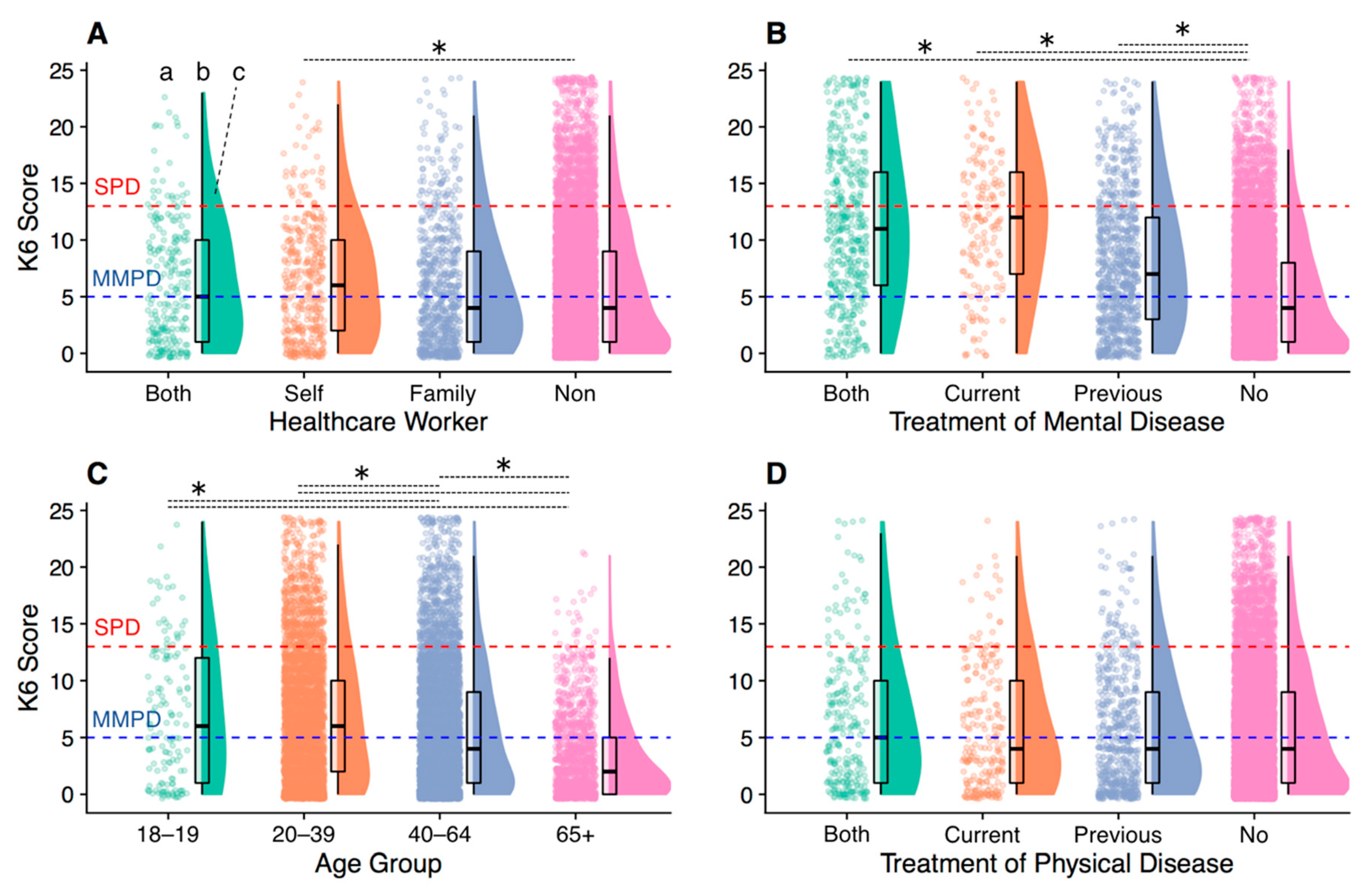
3.4. Psychological Distress in Vulnerable Groups
3.5. Risk and Preventive Factors for Psychological Distress
3.6. Comprehensive Interaction Structure of Psychosocial Variables Associated with Psychological Distress
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| COVID-19 | coronavirus disease 2019 |
| CSLC | Comprehensive Survey of Living Conditions |
| GEJE | Great East Japan Earthquake |
| K6 | Kessler Psychological Distress Scale |
| LSNS-6 | abbreviated Lubben Social Network Scale |
| MMPD | mild-to-moderate psychological distress |
| NPD | no or low psychological distress |
| PD | psychological distress |
| PHQ-9 | Patient Health Questionnaire-9 |
| SPD | serious psychological distress |
| UCLA-LS3 | UCLA Loneliness Scale version 3 |
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Age Group | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Psychometric Data, M (SD) | Total | 18–19 | 20–39 | 40–64 | ≥65 | F | df | p | |||||
| Psychological distress, loneliness and social network | |||||||||||||
| K6 | 5.58 | (5.43) | 6.87 a | (5.97) | 6.67 a | (5.76) | 5.46 a | (5.35) | 3.09 | (3.65) | 159.22 | (3, 11,329) | <0.001 |
| PHQ-9 | 4.90 | (5.53) | 6.44 a | (6.25) | 5.95 a | (5.79) | 4.79 a | (5.53) | 2.45 | (3.66) | 147.82 | (3, 11,329) | <0.001 |
| UCLA-LS3 | 23.46 | (5.70) | 23.70 a | (5.54) | 23.54 a | (5.70) | 23.94 a | (5.66) | 21.18 | (5.32) | 92.81 | (3, 11,329) | <0.001 |
| LSNS-6 | 10.56 | (6.17) | 13.13 a | (6.48) | 11.31 | (6.01) | 9.83 a | (6.11) | 11.39 | (6.38) | 64.33 | (3, 11,329) | <0.001 |
| Lifestyle and stress management during mild lockdown | |||||||||||||
| Exercise | 4.17 | (1.81) | 4.26 | (1.92) | 4.21 a | (1.79) | 4.04 a | (1.82) | 4.59 | (1.76) | 37.68 | (3, 11,329) | <0.001 |
| Healthy eating habits | 4.34 | (1.56) | 4.01 a | (1.68) | 4.25 a | (1.57) | 4.28 a | (1.55) | 4.82 | (1.43) | 54.95 | (3, 11,329) | <0.001 |
| Healthy sleep habits | 4.63 | (1.79) | 3.82 a | (2.00) | 4.24 a | (1.84) | 4.70 a | (1.74) | 5.40 | (1.54) | 165.38 | (3, 11,329) | <0.001 |
| Activity | 4.03 | (1.67) | 4.73 | (1.73) | 4.10 a | (1.70) | 3.88 a | (1.66) | 4.38 | (1.59) | 46.77 | (3, 11,329) | <0.001 |
| Offline interaction with family or friends | 3.53 | (1.88) | 4.17 a | (2.02) | 3.52 | (1.95) | 3.50 | (1.84) | 3.61 | (1.79) | 6.99 | (3, 11,329) | <0.001 |
| Online interaction with family or friends | 3.27 | (2.00) | 4.34 a | (2.14) | 3.85 a | (2.05) | 2.91 a | (1.88) | 3.17 | (1.98) | 193.29 | (3, 11,329) | <0.001 |
| Altruistically motivated preventive behaviours of COVID-19 | 5.58 | (1.66) | 5.87 | (1.45) | 5.72 a | (1.60) | 5.48 | (1.70) | 5.57 | (1.67) | 16.84 | (3, 11,329) | <0.001 |
| Optimism | 4.06 | (1.57) | 4.26 | (1.74) | 4.08 a | (1.65) | 3.94 a | (1.54) | 4.45 | (1.39) | 41.27 | (3, 11,329) | <0.001 |
| Stressors related to mild lockdown | |||||||||||||
| Deterioration of household economy | 3.80 | (1.83) | 3.95 a | (1.93) | 3.92 a | (1.89) | 3.85 a | (1.80) | 3.24 | (1.66) | 51.41 | (3, 11,329) | <0.001 |
| Deterioration of relationships with familiar people | 2.38 | (1.54) | 2.45 a | (1.66) | 2.36 a | (1.58) | 2.47 a | (1.55) | 2.00 | (1.33) | 36.13 | (3, 11,329) | <0.001 |
| Frustration | 3.31 | (1.75) | 3.52 a | (1.84) | 3.65 a | (1.80) | 3.28 a | (1.71) | 2.54 | (1.54) | 143.69 | (3, 11,329) | <0.001 |
| COVID-19-related anxiety | 4.04 | (1.70) | 3.98 a | (1.75) | 4.26 a | (1.69) | 4.01 a | (1.68) | 3.57 | (1.69) | 59.97 | (3, 11,329) | <0.001 |
| COVID-19-related sleeplessness | 2.44 | (1.54) | 2.17 | (1.55) | 2.47 a | (1.61) | 2.51 a | (1.53) | 2.12 | (1.32) | 26.68 | (3, 11,329) | <0.001 |
| Difficulties due to the lack of daily necessities | 3.63 | (1.85) | 3.39 a | (1.92) | 3.84 a | (1.90) | 3.68 a | (1.80) | 2.86 | (1.71) | 103.62 | (3, 11,329) | <0.001 |
| Difficulties in work or schoolwork | 3.82 | (2.05) | 4.94 a | (1.97) | 4.23 a | (2.07) | 3.84 a | (1.97) | 2.56 | (1.79) | 260.75 | (3, 11,329) | <0.001 |
References
- WHO. Coronavirus Disease (COVID-19) Situation Report, 137. 2020. Available online: https://www.who.int/docs/default-source/sri-lanka-documents/20200605-covid-19-sitrep-137.pdf?sfvrsn=a13df572_2 (accessed on 25 November 2020).
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, W.; Hu, T.; Hu, B.; Jin, C.; Wang, G.; Xie, C.; Chen, S.; Xu, J. Prevalence and correlates of PTSD and depressive symptoms one month after the outbreak of the COVID-19 epidemic in a sample of home-quarantined Chinese university students. J. Affect. Disord. 2020, 274, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Losada-Baltar, A.; Jiménez-Gonzalo, L.; Gallego-Alberto, L.; Pedroso-Chaparro, M.D.S.; Fernandes-Pires, J.; Márquez-González, M. “We’re staying at home”. Association of self-perceptions of aging, personal and family resources and loneliness with psychological distress during the lock-down period of COVID-19. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moccia, L.; Janiri, D.; Pepe, M.; Dattoli, L.; Molinaro, M.; De Martin, V.; Chieffo, D.; Janiri, L.; Fiorillo, A.; Sani, G.; et al. Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: An early report on the Italian general population. Brain. Behav. Immun. 2020. [Google Scholar] [CrossRef]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A nationwide survey of psychological distress among italian people during the covid-19 pandemic: Immediate psychological responses and associated factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Cases in Japan (NHK Report). Available online: https://www3.nhk.or.jp/news/special/coronavirus/data-all/ (accessed on 25 November 2020).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A.; Ahmed Khan, F.; Napolean Shanmugam, G.; et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain. Behav. Immun. 2020. [Google Scholar] [CrossRef]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ 2020, 369, m1642. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, M.R.; Agho, K.E.; Stevens, G.J.; Raphael, B. Factors influencing psychological distress during a disease epidemic: Data from Australia’s first outbreak of equine influenza. BMC Public Health 2008, 8, 347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comprehensive Survey of Living Conditions. Available online: https://www.mhlw.go.jp/english/database/db-hss/cslc-index.html (accessed on 25 November 2020).
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.T.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, T.A.; Kessler, R.C.; Slade, T.; Andrews, G. The performance of the K6 and K10 screening scales for psychological distress in the Australian National Survey of Mental Health and Well-Being. Psychol. Med. 2003, 33, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.L.T.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Veldhuizen, S.; Cairney, J.; Kurdyak, P.; Streiner, D.L. The sensitivity of the K6 as a screen for any disorder in community mental health surveys: A cautionary note. Can. J. Psychiatry 2007, 52, 256–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prochaska, J.J.; Sung, H.Y.; Max, W.; Shi, Y.; Ong, M. Validity study of the K6 scale as a measure of moderate mental distress based on mental health treatment need and utilization. Int. J. Methods Psychiatr. Res. 2012, 21, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Merikangas, K.R.; Berglund, P.; Eaton, W.W.; Koretz, D.S.; Walters, E.E. Mild Disorders Should Not Be Eliminated from the DSM-V. Arch. Gen. Psychiatry 2003, 60, 1117–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Galea, S.; Gruber, M.J.; Sampson, N.A.; Ursano, R.J.; Wessely, S. Trends in mental illness and suicidality after Hurricane Katrina. Mol. Psychiatry 2008, 13, 374–384. [Google Scholar] [CrossRef] [Green Version]
- Muramatsu, K.; Miyaoka, H.; Kamijima, K.; Muramatsu, Y.; Tanaka, Y.; Hosaka, M.; Miwa, Y.; Fuse, K.; Yoshimine, F.; Mashima, I.; et al. Performance of the Japanese version of the Patient Health Questionnaire-9 (J-PHQ-9) for depression in primary care. Gen. Hosp. Psychiatry 2018, 52, 64–69. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Siu, A.L.; Bibbins-Domingo, K.; Grossman, D.C.; Baumann, L.C.; Davidson, K.W.; Ebell, M.; García, F.A.R.; Gillman, M.; Herzstein, J.; Kemper, A.R.; et al. Screening for depression in adults: US preventive services task force recommendation statement. JAMA J. Am. Med. Assoc. 2016, 315, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, L.M.; Gullone, E. The clinical significance of loneliness: A literature review. Clin. Psychol. Rev. 2006, 26, 695–718. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, J.T.; Hawkley, L.C.; Thisted, R.A. Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the chicago health, aging, and social relations study. Psychol. Aging 2010, 25, 453–463. [Google Scholar] [CrossRef] [Green Version]
- Koizumi, Y.; Awata, S.; Kuriyama, S.; Ohmori, K.; Hozawa, A.; Seki, T.; Matsuoka, H.; Tsuji, I. Association between social support and depression status in the elderly: Results of a 1-year community-based prospective cohort study in Japan. Psychiatry Clin. Neurosci. 2005, 59, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Arimoto, A.; Tadaka, E. Reliability and validity of Japanese versions of the UCLA loneliness scale version 3 for use among mothers with infants and toddlers: A cross-sectional study. BMC Womens Health 2019, 19, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurimoto, A.; Awata, S.; Ohkubo, T.; Tsubota-Utsugi, M.; Asayama, K.; Takahashi, K.; Suenaga, K.; Satoh, H.; Imai, Y. Reliability and validity of the Japanese version of the abbreviated Lubben Social Network Scale. Jpn. J. Geriatr. 2011, 48, 149–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, D.W. UCLA Loneliness Scale (Version 3): Reliability, validity, and factor structure. J. Pers. Assess. 1996, 66, 20–40. [Google Scholar] [CrossRef] [PubMed]
- Durak, M.; Senol-Durak, E. Psychometric qualities of the ucla loneliness scale-version 3 as applied in a turkish culture. Educ. Gerontol. 2010, 36, 988–1007. [Google Scholar] [CrossRef]
- Shevlin, M.; Murphy, S.; Murphy, J. The Latent Structure of Loneliness: Testing Competing Factor Models of the UCLA Loneliness Scale in a Large Adolescent Sample. Assessment 2015, 22, 208–215. [Google Scholar] [CrossRef]
- Zarei, S.; Memari, A.H.; Moshayedi, P.; Shayestehfar, M. Validity and reliability of the UCLA loneliness scale version 3 in Farsi. Educ. Gerontol. 2016, 42, 49–57. [Google Scholar] [CrossRef]
- Lubben, J.E. Assessing social networks among elderly populations. Fam. Community Health 1988, 11, 42–52. [Google Scholar] [CrossRef]
- Ceria, C.D.; Masaki, K.H.; Rodriguez, B.L.; Chen, R.; Yano, K.; David Curb, J. The relationship of psychosocial factors to total mortality among older Japanese-American men: The Honolulu Heart Program. J. Am. Geriatr. Soc. 2001, 49, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Martire, L.M.; Schulz, R.; Mittelmark, M.B.; Newsom, J.T. Stability and change in older adults’ social contact and social support: The Cardiovascular Health Study. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1999, 54B, S302–S311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okwumabua, J.O.; Baker, F.M.; Wong, S.P.; Pilgram, B.O. Characteristics of depressive symptoms in elderly urban and rural African Americans. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1997, 52, M241–M246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, T.; Uchiumi, C.; Suzuki, N.; Sugaya, N. The mental health impact of COVID-19 in Japan. Open Sci. Framew. 2020. [Google Scholar] [CrossRef]
- Sugaya, N.; Yamamoto, T.; Suzuki, N.; Uchiumi, C. A real-time survey on the psychological impact of mild lockdown for COVID-19 in the Japanese population. Sci. Data 2020, 7. [Google Scholar] [CrossRef] [PubMed]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 5th ed.; SAGE Publications Ltd.: London, UK; Philadelphia, PA, USA, 2018; ISBN 9781526436566. [Google Scholar]
- Wang, P.; Laskey, K.B.; Domeniconi, C.; Jordan, M.I. Nonparametric Bayesian Co-clustering Ensembles. SIAM Int. Conf. Data Min. 2011, 331–342. [Google Scholar]
- RStudio Team RStudio: Integrated Development for R 2015. Available online: http://www.rstudio.com/ (accessed on 25 November 2020).
- Allen, M.; Poggiali, D.; Whitaker, K.; Marshall, T.R.; Kievit, R.A. Raincloud plots: A multi-platform tool for robust data visualization [version 1; peer review: 2 approved]. Wellcome Open Res. 2019, 4, 63. [Google Scholar] [CrossRef] [Green Version]
- Nickell, L.A.; Crighton, E.J.; Tracy, C.S.; Al-Enazy, H.; Bolaji, Y.; Hanjrah, S.; Hussain, A.; Makhlouf, S.; Upshur, R.E.G. Psychosocial effects of SARS on hospital staff: Survey of a large tertiary care institution. CMAJ 2004, 170, 793–798. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, N.; Docherty, M.; Gnanapragasam, S.; Wessely, S. Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ 2020, 368, m1211. [Google Scholar] [CrossRef] [Green Version]
- Brooks, S.K.; Dunn, R.; Amlôt, R.; Rubin, G.J.; Greenberg, N. A Systematic, Thematic Review of Social and Occupational Factors Associated with Psychological Outcomes in Healthcare Employees during an Infectious Disease Outbreak. J. Occup. Environ. Med. 2018, 60, 248–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hao, F.; Tan, W.; Jiang, L.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; Jiang, X.; McIntyre, R.S.; et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain. Behav. Immun. 2020, 87, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Iasevoli, F.; Fornaro, M.; D’Urso, G.; Galletta, D.; Casella, C.; Paternoster, M.; Buccelli, C.; De Bartolomeis, A. Psychological distress in serious mental illness patients during the COVID-19 outbreak and one-month mass quarantine in Italy. Psychol. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, S.K. Covid-19, Coronavirus and Mental Health Rehabilitation at Times of Crisis. J. Psychosoc. Rehabil. Ment. Health 2020, 7, 1–2. [Google Scholar] [CrossRef]
- Branley-Bell, D.; Talbot, C.V. Exploring the impact of the COVID-19 pandemic and UK lockdown on individuals with experience of eating disorders. J. Eat. Disord. 2020, 8, 44. [Google Scholar] [CrossRef]
- Wang, H.; Xia, Q.; Xiong, Z.; Li, Z.; Xiang, W.; Yuan, Y.; Liu, Y.; Li, Z. The psychological distress and coping styles in the early stages of the 2019 coronavirus disease (COVID-19) epidemic in the general mainland Chinese population: A web-based survey. PLoS ONE 2020, 15, e0233410. [Google Scholar] [CrossRef]
- United Nations Department of Economic Social Affairs. Population Division World Population Prospects 2019: Data Booklet (ST/ESA/SER.A/424); United Nations Department of Economic Social Affairs: New York, NY, USA, 2019. [Google Scholar]
- Ministry of Internal Affairs and Communications Report on Information and Communication Media Usage Time and Information Behavior in 2018. Available online: https://www.soumu.go.jp/main_sosiki/joho_tsusin/eng/pressrelease/2020/9/30_04.html (accessed on 25 November 2020).
- Ministry of Health Labour and Welfare Report on the 2011 Public Opinion Survey. 2012. Available online: https://www.mhlw.go.jp/english/new-info/2012.html (accessed on 25 November 2020).
- Hawryluck, L.; Gold, W.L.; Robinson, S.; Pogorski, S.; Galea, S.; Styra, R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg. Infect. Dis. 2004, 10, 1206–1212. [Google Scholar] [CrossRef]
- Alvaro, P.K.; Roberts, R.M.; Harris, J.K. A Systematic Review Assessing Bidirectionality between Sleep Disturbances, Anxiety, and Depression. Sleep 2013, 36, 1059–1068. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain. Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- Beck, J.S. Cognitive Behavior Therapy: Basics and Beyond, 2nd ed.; Guilford Press: Washington, DC, USA, 2011; ISBN 978-1-60918-504-6 (Hardcover), 978-1-60918-506-0 (PDF). [Google Scholar]
- Sehmi, R.; Maughan, B.; Matthews, T.; Arseneault, L. No man is an island: Social resources, stress and mental health at mid-life. Br. J. Psychiatry 2020, 217, 638–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]



| Psychological Distress | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics, n (%) | Total | No or Low | Mild-to-Moderate | Serious | χ2 | df | p | V | |||
| Overall | 11,333 | 5884 | (51.9) | 4146 | (36.6) | 1303 | (11.5) | 2831.00 | 2 | <0.001 | n.a. |
| Age | |||||||||||
| 18–19 | 143 | 62 | (43.4) | 50 | (35.0) | 31 | (21.7) | 428.66 | 6 | <0.001 | 0.138 |
| 20–39 | 3745 | 1633 | (43.6) | 1508 | (40.3) | 604 | (16.1) | ||||
| 40–64 | 6024 | 3157 | (52.4) | 2230 | (37.0) | 637 | (10.6) | ||||
| ≥65 | 1421 | 1032 | (72.6) | 358 | (25.2) | 31 | (2.2) | ||||
| Sex | |||||||||||
| Male | 5391 | 3098 | (57.5) | 1789 | (33.2) | 504 | (9.3) | 134.68 | 2 | <0.001 | 0.109 |
| Female | 5942 | 2786 | (46.9) | 2357 | (39.7) | 799 | (13.4) | ||||
| Occupationcategory | |||||||||||
| Employed | 7685 | 3948 | (51.4) | 2852 | (37.1) | 885 | (11.5) | 75.60 | 8 | <0.001 | 0.058 |
| Homemaker | 1806 | 919 | (50.9) | 699 | (38.7) | 188 | (10.4) | ||||
| Student | 407 | 175 | (43.0) | 158 | (38.8) | 74 | (18.2) | ||||
| Unemployed | 1068 | 662 | (62.0) | 304 | (28.5) | 102 | (9.6) | ||||
| Other | 367 | 180 | (49.0) | 133 | (36.2) | 54 | (14.7) | ||||
| Healthcare worker (self) | |||||||||||
| Yes | 661 | 299 | (45.2) | 288 | (43.6) | 74 | (11.2) | 15.46 | 2 | <0.001 | 0.037 |
| No | 10,672 | 5585 | (52.3) | 3858 | (36.2) | 1229 | (11.5) | ||||
| Healthcare worker (family) | |||||||||||
| Yes | 991 | 493 | (49.7) | 373 | (37.6) | 125 | (12.6) | 2.49 | 2 | 0.287 | 0.015 |
| No | 10,342 | 5391 | (52.1) | 3773 | (36.5) | 1178 | (11.4) | ||||
| Marital status | |||||||||||
| Married | 7043 | 3933 | (55.8) | 2500 | (35.5) | 610 | (8.7) | 191.36 | 2 | <0.001 | 0.130 |
| Unmarried | 4290 | 1951 | (45.5) | 1646 | (38.4) | 693 | (16.2) | ||||
| Annual household income (JPY) | |||||||||||
| < 2.0 million | 633 | 273 | (43.1) | 233 | (36.8) | 127 | (20.1) | 149.24 | 10 | <0.001 | 0.081 |
| 2.0–3.9 million | 1990 | 1020 | (51.3) | 739 | (37.1) | 231 | (11.6) | ||||
| 4.0–5.9 million | 2214 | 1174 | (53.0) | 797 | (36.0) | 243 | (11.0) | ||||
| 6.0–7.9 million | 1495 | 817 | (54.6) | 529 | (35.4) | 149 | (10.0) | ||||
| ≥ 8.0 million | 2130 | 1267 | (59.5) | 694 | (32.6) | 169 | (7.9) | ||||
| Unknown | 2871 | 1333 | (46.4) | 1154 | (40.2) | 384 | (13.4) | ||||
| Current treatment of severe physical diseases | |||||||||||
| Yes | 482 | 248 | (51.5) | 168 | (34.9) | 66 | (13.7) | 1.85 | 2 | 0.397 | 0.013 |
| No | 10,851 | 5636 | (51.9) | 3978 | (36.7) | 1237 | (11.4) | ||||
| Previous treatment of severe physical diseases | |||||||||||
| Yes | 851 | 440 | (51.7) | 304 | (35.7) | 107 | (12.6) | 1.12 | 2 | 0.571 | 0.010 |
| No | 10,482 | 5444 | (51.9) | 3842 | (36.7) | 1196 | (11.4) | ||||
| Current treatment of psychological problems | |||||||||||
| Yes | 641 | 110 | (17.2) | 271 | (42.3) | 260 | (40.6) | 663.31 | 2 | <0.001 | 0.242 |
| No | 10,692 | 5774 | (54.0) | 3875 | (36.2) | 1043 | (9.8) | ||||
| Previous treatment of psychological problems | |||||||||||
| Yes | 1366 | 383 | (28.0) | 600 | (43.9) | 383 | (28.0) | 563.09 | 2 | <0.001 | 0.223 |
| No | 9967 | 5501 | (55.2) | 3546 | (35.6) | 920 | (9.2) | ||||
| Psychological Distress | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Psychometric Data, M (SD) | Total | No or Low | Mild-to-Moderate | SERIOUS | F | df | p | ||||
| Psychological distress, loneliness and social network | |||||||||||
| K6 | 5.58 | (5.43) | 1.39 | (1.45) | 8.07 a | (2.30) | 16.58 a,b | (3.19) | 34,224.57 | (2, 11,330) | <0.001 |
| PHQ-9 | 4.90 | (5.53) | 1.71 | (2.50) | 6.49 a | (4.41) | 14.27 a,b | (5.84) | 6468.81 | (2, 11,330) | <0.001 |
| UCLA-LS3 | 23.46 | (5.70) | 21.43 | (5.32) | 24.71 a | (4.82) | 28.63 a,b | (5.50) | 1228.45 | (2, 11,330) | <0.001 |
| LSNS-6 | 10.56 | (6.17) | 11.41 | (6.33) | 10.09 a | (5.79) | 8.25 a,b | (5.85) | 163.06 | (2, 11,330) | <0.001 |
| Lifestyle and stress management during mild lockdown | |||||||||||
| Exercise | 4.17 | (1.81) | 4.26 | (1.87) | 4.12 a | (1.69) | 3.90 a,b | (1.90) | 22.89 | (2, 11,330) | <0.001 |
| Healthy eating habits | 4.34 | (1.56) | 4.43 | (1.59) | 4.30 a | (1.44) | 4.01 a,b | (1.70) | 41.65 | (2, 11,330) | <0.001 |
| Healthy sleep habits | 4.63 | (1.79) | 4.94 | (1.78) | 4.40 a | (1.66) | 3.93 a,b | (1.95) | 229.43 | (2, 11,330) | <0.001 |
| Activity | 4.02 | (1.67) | 4.17 | (1.69) | 3.94 a | (1.58) | 3.65 a,b | (1.81) | 59.19 | (2, 11,330) | <0.001 |
| Offline interaction with family or friends | 3.53 | (1.88) | 3.62 | (1.94) | 3.49 a | (1.78) | 3.24 a,b | (1.85) | 24.01 | (2, 11,330) | <0.001 |
| Online interaction with family or friends | 3.27 | (2.00) | 3.28 | (2.08) | 3.31 | (1.89) | 3.11 a,b | (1.98) | 5.10 | (2, 11,330) | 0.006 |
| Altruistically motivated preventive behaviours of COVID-19 | 5.58 | (1.67) | 5.62 | (1.70) | 5.50 a | (1.61) | 5.61 | (1.67) | 7.05 | (2, 11,330) | <0.001 |
| Optimism | 4.06 | (1.57) | 4.35 | (1.54) | 3.89 a | (1.43) | 3.24 a,b | (1.76) | 321.64 | (2, 11,330) | <0.001 |
| Stressors related to mild lockdown | |||||||||||
| Deterioration of household economy | 3.80 | (1.83) | 3.41 | (1.80) | 4.04 a | (1.69) | 4.78 a,b | (1.86) | 385.95 | (2, 11,330) | <0.001 |
| Deterioration of relationships with familiar people | 2.38 | (1.54) | 1.92 | (1.31) | 2.68 a | (1.51) | 3.47 a,b | (1.82) | 754.72 | (2, 11,330) | <0.001 |
| Frustration | 3.31 | (1.75) | 2.59 | (1.58) | 3.85 a | (1.49) | 4.88 a,b | (1.61) | 1554.34 | (2, 11,330) | <0.001 |
| COVID-19-related anxiety | 4.04 | (1.70) | 3.50 | (1.70) | 4.47 a | (1.42) | 5.11 a,b | (1.62) | 780.16 | (2, 11,330) | <0.001 |
| COVID-19-related sleeplessness | 2.44 | (1.54) | 1.92 | (1.25) | 2.84 a | (1.48) | 3.53 a,b | (1.90) | 925.94 | (2, 11,330) | <0.001 |
| Difficulties owing to the lack of daily necessities | 3.63 | (1.85) | 3.16 | (1.84) | 3.97 a | (1.66) | 4.65 a,b | (1.81) | 500.75 | (2, 11,330) | <0.001 |
| Difficulties in work or schoolwork | 3.82 | (2.05) | 3.37 | (2.07) | 4.14 a | (1.88) | 4.84 a,b | (1.94) | 374.40 | (2, 11,330) | <0.001 |
| Mild-to-Moderate Psychological Distress | Serious Psychological Distress | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Predictor | β (SE) | OR [95% CI] | p | β (SE) | OR [95% CI] | p | ||||
| Age | ||||||||||
| ≥65 (ref.) | 0 | 0 | ||||||||
| 18–19 | 0.34 | (0.23) | 1.40 | [0.89–2.20] | 0.141 | 1.91 | (0.36) | 6.78 | [3.33–13.82] | <0.001 |
| 20–39 | 0.31 | (0.09) | 1.36 | [1.14–1.62] | 0.001 | 1.25 | (0.22) | 3.50 | [2.29–5.36] | <0.001 |
| 40–64 | 0.11 | (0.08) | 1.11 | [0.95–1.30] | 0.179 | 0.58 | (0.21) | 1.79 | [1.18–2.70] | 0.006 |
| Sex | ||||||||||
| Male (ref.) | 0 | 0 | ||||||||
| Female | 0.23 | (0.05) | 1.25 | [1.13–1.39] | <0.001 | 0.28 | (0.09) | 1.32 | [1.11–1.56] | 0.002 |
| Healthcare worker (self) | ||||||||||
| No (ref.) | 0 | 0 | ||||||||
| Yes | 0.27 | (0.10) | 1.31 | [1.07–1.59] | 0.009 | –0.07 | (0.17) | 0.94 | [0.67–1.32] | 0.707 |
| Previous treatment of severe physical diseases | ||||||||||
| No (ref.) | 0 | 0 | ||||||||
| Yes | 0.24 | (0.10) | 1.27 | [1.06–1.53] | 0.012 | 0.36 | (0.16) | 1.43 | [1.04–1.95] | 0.026 |
| Current treatment of psychological problems | ||||||||||
| No (ref.) | 0 | 0 | ||||||||
| Yes | 0.95 | (0.14) | 2.59 | [1.96–3.41] | <0.001 | 1.88 | (0.17) | 6.58 | [4.68–9.23] | <0.001 |
| Previous treatment of psychological problems | ||||||||||
| No (ref.) | 0 | 0 | ||||||||
| Yes | 0.57 | (0.09) | 1.77 | [1.50–2.10] | <0.001 | 0.98 | (0.12) | 2.66 | [2.10–3.37] | <0.001 |
| Psychosocial variables | ||||||||||
| UCLA-LS3 | 0.12 | (0.01) | 1.13 | [1.12–1.14] | <0.001 | 0.27 | (0.01) | 1.30 | [1.28–1.33] | <0.001 |
| LSNS-6 | 0.02 | (0.01) | 1.02 | [1.01–1.03] | <0.001 | 0.03 | (0.01) | 1.03 | [1.02–1.05] | <0.001 |
| Online interaction with family or friends | 0.03 | (0.01) | 1.03 | [1.01–1.06] | 0.017 | 0.08 | (0.02) | 1.08 | [1.03–1.13] | 0.002 |
| Optimism | −0.12 | (0.02) | 0.89 | [0.86–0.92] | <0.001 | −0.28 | (0.03) | 0.76 | [0.71–0.80] | <0.001 |
| Healthy sleep habits | −0.08 | (0.02) | 0.92 | [0.90–0.95] | <0.001 | −0.14 | (0.03) | 0.87 | [0.83–0.91] | <0.001 |
| Deterioration of household economy | 0.04 | (0.02) | 1.04 | [1.01–1.07] | 0.018 | 0.13 | (0.03) | 1.14 | [1.08–1.20] | <0.001 |
| Deterioration of relationships with familiar people | 0.06 | (0.02) | 1.07 | [1.03–1.11] | 0.001 | 0.19 | (0.03) | 1.21 | [1.15–1.28] | <0.001 |
| Frustration | 0.26 | (0.02) | 1.30 | [1.26–1.35] | <0.001 | 0.53 | (0.03) | 1.70 | [1.60–1.81] | <0.001 |
| COVID-19-related anxiety | 0.23 | (0.02) | 1.26 | [1.22–1.30] | <0.001 | 0.40 | (0.03) | 1.49 | [1.40–1.60] | <0.001 |
| COVID-19-related sleeplessness | 0.20 | (0.02) | 1.22 | [1.17–1.27] | <0.001 | 0.33 | (0.03) | 1.40 | [1.32–1.48] | <0.001 |
| Difficulties in work or schoolwork | 0.04 | (0.01) | 1.04 | [1.01–1.07] | 0.007 | 0.10 | (0.03) | 1.11 | [1.05–1.16] | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamamoto, T.; Uchiumi, C.; Suzuki, N.; Yoshimoto, J.; Murillo-Rodriguez, E. The Psychological Impact of ‘Mild Lockdown’ in Japan during the COVID-19 Pandemic: A Nationwide Survey under a Declared State of Emergency. Int. J. Environ. Res. Public Health 2020, 17, 9382. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249382
Yamamoto T, Uchiumi C, Suzuki N, Yoshimoto J, Murillo-Rodriguez E. The Psychological Impact of ‘Mild Lockdown’ in Japan during the COVID-19 Pandemic: A Nationwide Survey under a Declared State of Emergency. International Journal of Environmental Research and Public Health. 2020; 17(24):9382. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249382
Chicago/Turabian StyleYamamoto, Tetsuya, Chigusa Uchiumi, Naho Suzuki, Junichiro Yoshimoto, and Eric Murillo-Rodriguez. 2020. "The Psychological Impact of ‘Mild Lockdown’ in Japan during the COVID-19 Pandemic: A Nationwide Survey under a Declared State of Emergency" International Journal of Environmental Research and Public Health 17, no. 24: 9382. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249382