Adverse Childhood Experiences and Risk of Subsequently Engaging in Self-Harm and Violence towards Other People—“Dual Harm”

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Description of the Study Cohort
3.2. Prevalence of Personal and Family Risk Factors among Cases and Controls with Histories of Self-Harm, Violent Criminality and Dual Harm
3.3. Relative Risks for Violent Criminality, Self-Harm and Dual Harm by Exposure Group
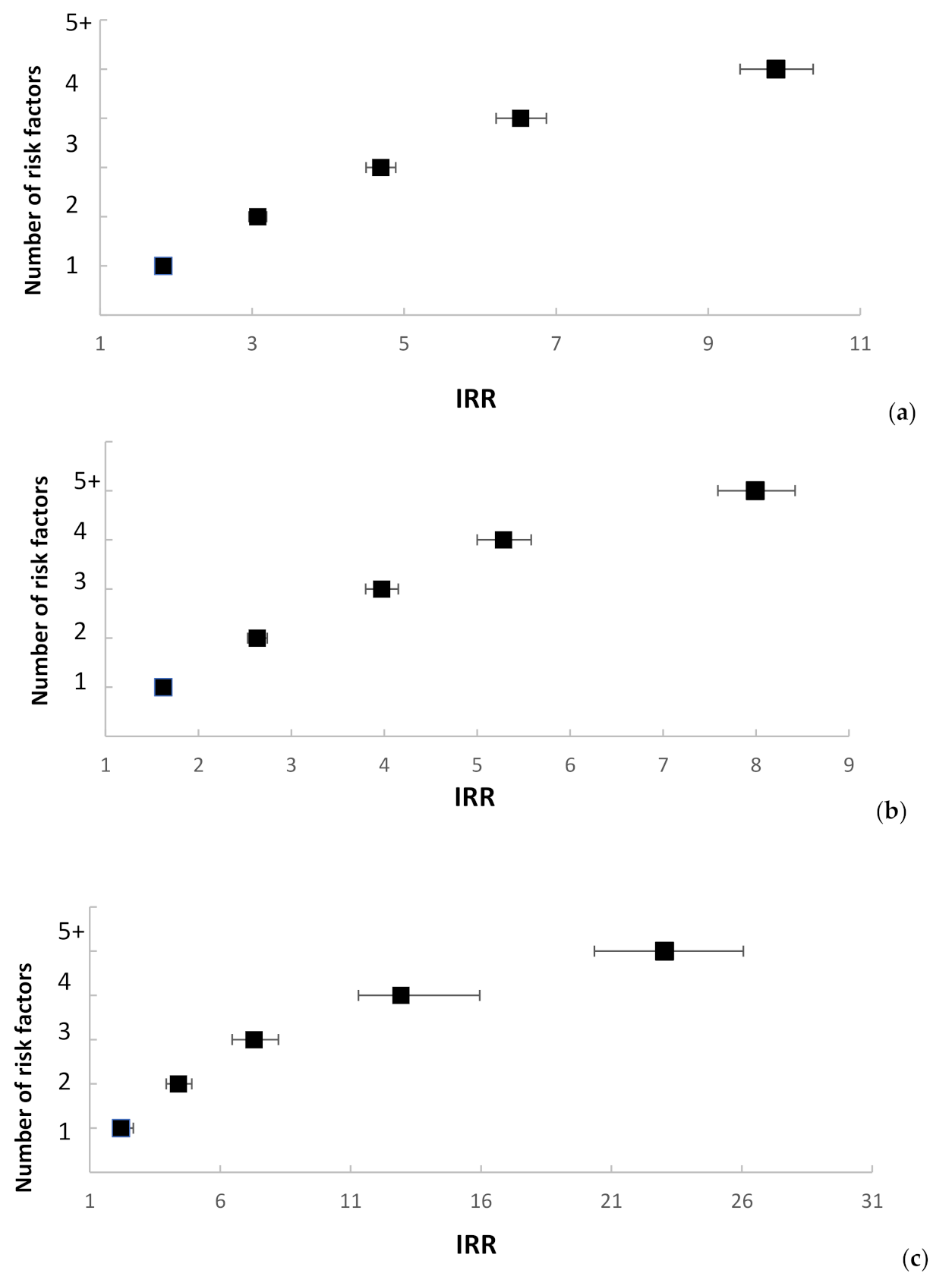
3.4. Relative Risks of Violent Criminality, Self-Harm and Dual Harm by Number of Adverse Childhood Experiences
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Geulayov, G.; Metcalfe, C.; Heron, J.; Kidger, J.; Gunnell, D. Parental Suicide Attempt and Offspring Self-Harm and Suicidal Thoughts: Results from the Avon Longitudinal Study of Parents and Children (ALSPAC) Birth Cohort. J. Am. Acad. Child. Adolesc. Psychiatry 2014, 53, 509–517.e2. [Google Scholar] [CrossRef]
- Serafini, G.; Muzio, C.; Piccinini, G.; Flouri, E.; Ferrigno, G.; Pompili, M.; Girardi, P.; Amore, M. Life adversities and suicidal behavior in young individuals: A systematic review. Eur. Child. Adolesc. Psychiatry 2015, 24, 1423–1446. [Google Scholar] [CrossRef]
- Evans, E.; Hawton, K.; Rodham, K. Factors associated with suicidal phenomena in adolescents: A systematic review of population-based studies. Clin. Psychol. Rev. 2004, 24, 957–979. [Google Scholar] [CrossRef]
- Hawton, K.; Kingsbury, S.; Steinhardt, K.; James, A.; Fagg, J. Repetition of deliberate self-harm by adolescents: The role of psychological factors. J. Adolesc. 1999, 22, 369–378. [Google Scholar] [CrossRef]
- Christoffersen, M.; Poulsen, H.D.; Nielsen, A. Attempted suicide among young people: Risk factors in a prospective register based study of Danish children born in 1966. Acta Psychiatr. Scand. 2003, 108, 350–358. [Google Scholar] [CrossRef]
- Hawton, K.; Bergen, H.; Waters, K.; Ness, J.; Cooper, J.; Steeg, S.; Kapur, N. Epidemiology and nature of self-harm in children and adolescents: Findings from the multicentre study of self-harm in England. Eur. Child. Adolesc. Psychiatry 2012, 21, 369–377. [Google Scholar] [CrossRef]
- Mok, P.L.; Astrup, A.; Carr, M.J.; Antonsen, S.; Webb, R.T.; Pedersen, C.B. Experience of Child-Parent Separation and Later Risk of Violent Criminality. Am. J. Prev. Med. 2018, 55, 178–186. [Google Scholar] [CrossRef]
- Mok, P.L.; Pedersen, C.B.; Springate, D.; Astrup, A.; Kapur, N.; Antonsen, S.; Mors, O.; Webb, R.T. Parental psychiatric disease and risks of attempted suicide and violent criminal offending in offspring a population-based cohort study. JAMA Psychiatry 2016, 73, 1015–1022. [Google Scholar] [CrossRef] [Green Version]
- Mok, P.H.K.; Antonsen, S.; Pedersen, C.B.; Carr, M.J.; Kapur, N.; Nazroo, J.; Webb, R.T. Family income inequalities and trajectories through childhood and self-harm and violence in young adults: A population-based, nested case-control study. Lancet Public Health 2018, 3, e498–e507. [Google Scholar] [CrossRef] [Green Version]
- Fazel, S.; Grann, M.; Carlström, E.; Lichtenstein, P.; Långström, N. Risk factors for violent crime in Schizophrenia: A national cohort study of 13,806 patients. J. Clin. Psychiatry 2009, 70, 362–369. [Google Scholar] [CrossRef]
- O’Donnell, O.; House, A.; Waterman, M. The co-occurrence of aggression and self-harm: Systematic literature review. J. Affect. Disord. 2015, 175, 325–350. [Google Scholar] [CrossRef] [PubMed]
- Richmond-Rakerd, L.S.; Caspi, A.; Arseneault, L.; Baldwin, J.; Danese, A.; Houts, R.M.; Matthews, T.; Wertz, J.; Moffitt, T.E. Adolescents Who Self-Harm and Commit Violent Crime: Testing Early-Life Predictors of Dual Harm in a Longitudinal Cohort Study. Am. J. Psychiatry 2019, 176, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Slade, K.; Forrester, A.; Baguley, T. Coexisting violence and self-harm: Dual harm in an early-stage male prison population. Leg. Criminol. Psychol. 2020, 25, 182–198. [Google Scholar] [CrossRef] [Green Version]
- Steeg, S.; Webb, R.T.; Mok, P.L.H.; Pedersen, C.B.; Antonsen, S.; Kapur, N.; Carr, M.J. Risk of dying unnaturally among people aged 15–35 years who have harmed themselves and inflicted violence on others: A national nested case-control study. Lancet Public Health 2019, 4, e220–e228. [Google Scholar] [CrossRef] [Green Version]
- Harford, T.C.; Yi, H.-Y.; Grant, B.F. Other- and self-directed forms of violence and their relationships to DSM-IV substance use and other psychiatric disorders in a national survey of adults. Compr. Psychiatry 2013, 54, 731–739. [Google Scholar] [CrossRef] [Green Version]
- Carr, M.J.; Mok, P.; Antonsen, S.; Pedersen, C.B.; Webb, R. Self-harm and violent criminality linked with parental death during childhood. Psychol. Med. 2019, 50, 1224–1232. [Google Scholar] [CrossRef] [Green Version]
- McMahon, K.; Hoertel, N.; Olfson, M.; Wall, M.; Wang, S.; Blanco, C. Childhood maltreatment and impulsivity as predictors of interpersonal violence, self-injury and suicide attempts: A national study. Psychiatry Res. 2018, 269, 386–393. [Google Scholar] [CrossRef]
- Harford, T.C.; Chen, C.M.; Kerridge, B.T.; Grant, B.F. Self- and other-directed forms of violence and their relationship with lifetime DSM-5 psychiatric disorders: Results from the National Epidemiologic Survey on Alcohol Related Conditions−III (NESARC−III). Psychiatry Res. 2018, 262, 384–392. [Google Scholar] [CrossRef]
- Kar, H.L. Acknowledging the victim to perpetrator trajectory: Integrating a mental health focused trauma-based approach into global violence programs. Aggress. Violent Behav. 2019, 47, 293–297. [Google Scholar] [CrossRef]
- Bruffaerts, R.; Demyttenaere, K.; Borges, G.; Haro, J.M.; Chiu, W.T.; Hwang, I.; Karam, E.G.; Kessler, R.C.; Sampson, N.; Alonso, J.; et al. Childhood adversities as risk factors for onset and persistence of suicidal behaviour. Br. J. Psychiatry 2010, 197, 20–27. [Google Scholar] [CrossRef] [Green Version]
- Sahlin, H.; Kuja-Halkola, R.; Bjureberg, J.; Lichtenstein, P.; Molero, Y.; Rydell, M.; Hedman, E.; Runeson, B.; Jokinen, J.; Ljótsson, B.; et al. Association Between Deliberate Self-harm and Violent Criminality. JAMA Psychiatry 2017, 74, 615–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plutchik, R.; Van Praag, H.M.; Conte, H.R. Correlates of suicide and violence risk: III. A two-stage model of countervailing forces. Psychiatry Res. 1989, 28, 215–225. [Google Scholar] [CrossRef]
- Fazel, S.; Wolf, A.; Palm, C.; Lichtenstein, P. Violent crime, suicide, and premature mortality in patients with schizophrenia and related disorders: A 38-year total population study in Sweden. Lancet Psychiatry 2014, 1, 44–54. [Google Scholar] [CrossRef] [Green Version]
- Breslow, N.E.; Day, N.E.; Halvorsen, K.T.; Prentice, R.L.; Sabai, C. Estimation of Multiple relative risk functions in matched case-control studies. Am. J. Epidemiol. 1978, 108, 299–307. [Google Scholar] [CrossRef]
- Clayton, M.; Hills, D. Statistical Models in Epidemiology; Oxford University Press: Oxford, UK, 1993. [Google Scholar]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (strobe) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lynge, E.; Sandegaard, J.L.; Matejka, R.M. The Danish National Patient Register. Scand. J. Public Health 2011, 39, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Mors, O.; Perto, G.P.; Mortensen, P.B. The danish psychiatric central research register. Scand. J. Public Health 2011, 39, 54–57. [Google Scholar] [CrossRef]
- Nordentoft, M.; Mortensen, P.B.; Pedersen, C.B. Absolute Risk of Suicide After First Hospital Contact in Mental Disorder. Arch. Gen. Psychiatry 2011, 68, 1058–1064. [Google Scholar] [CrossRef]
- Hawton, K.; Bergen, H.; Casey, D.; Simkin, S.; Palmer, B.; Cooper, J.; Kapur, N.; Horrocks, J.; House, A.; Lilley, R.; et al. Self-harm in England: A tale of three cities—Multicentre study of self-harm. Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 513–521. [Google Scholar] [CrossRef]
- Kapur, N.; Cooper, J.; O’Connor, R.C.; Hawton, K. Non-suicidal self-injury v. attempted suicide: New diagnosis or false dichotomy? Br. J. Psychiatry 2013, 202, 326–328. [Google Scholar] [CrossRef] [Green Version]
- Jensen, M.V.; Greve, H.G.; Spencer, M. The Principal Danish Criminal Acts, 3rd ed.; DJØF Publishing: Copenhagen, Denmark, 2006. [Google Scholar]
- StataCorp. Stata: Release 13; StataCorp LP: College Station, TX, USA, 2013. [Google Scholar]
- Pitkänen, J.; Remes, H.; Aaltonen, M.; Martikainen, P. Experience of maternal and paternal adversities in childhood as determinants of self-harm in adolescence and young adulthood. J. Epidemiol. Community Health 2019, 73, 1040–1046. [Google Scholar] [CrossRef]
- Kessler, R.C.; McLaughlin, K.A.; Green, J.G.; Gruber, M.J.; Sampson, N.A.; Zaslavsky, A.M.; Aguilar-Gaxiola, S.; Alhamzawi, A.O.; Alonso, J.; Angermeyer, M.; et al. Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. Br. J. Psychiatry 2010, 197, 378–385. [Google Scholar] [CrossRef] [Green Version]
- White, H.R.; Johnson, V.; Buyske, S. Parental modeling and parenting behavior effects on offspring alcohol and cigarette use: A growth curve analysis. J. Subst. Abus. 2000, 12, 287–310. [Google Scholar] [CrossRef]
- Thompson, R.; Flaherty, E.G.; English, D.J.; Litrownik, A.J.; Dubowitz, H.; Kotch, J.B.; Runyan, D.K. Trajectories of Adverse Childhood Experiences and Self-Reported Health at Age 18. Acad. Pediatr. 2015, 15, 503–509. [Google Scholar] [CrossRef] [Green Version]
- Webb, R.T.; Antonsen, S.; Carr, M.J.; Appleby, L.; Pedersen, C.B.; Mok, P.L.H. Self-harm and violent criminality among young people who experienced trauma-related hospital admission during childhood: A Danish national cohort study. Lancet Public Health 2017, 2, e314–e322. [Google Scholar] [CrossRef] [Green Version]
- Geulayov, G.; Casey, D.; McDonald, K.C.; Foster, P.; Pritchard, K.; Wells, C.; Clements, C.; Kapur, N.; Ness, J.; Waters, K.; et al. Incidence of suicide, hospital-presenting non-fatal self-harm, and community-occurring non-fatal self-harm in adolescents in England (the iceberg model of self-harm): A retrospective study. Lancet Psychiatry 2018, 5, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Diggins, E.; Kelley, R.; Cottrell, D.J.; House, A.; Owens, D. Age-related differences in self-harm presentations and subsequent management of adolescents and young adults at the emergency department. J. Affect. Disord. 2017, 208, 399–405. [Google Scholar] [CrossRef] [Green Version]
- Hawton, K.; Harriss, L. Deliberate self-harm by under-15-year-olds: Characteristics, trends and outcome. J. Child. Psychol. Psychiatry 2008, 49, 441–448. [Google Scholar] [CrossRef]
- Goldman-Mellor, S.J.; Caspi, A.; Harrington, H.; Hogan, S.; Nada-Raja, S.; Poulton, R.; Moffitt, T.E. Suicide attempt in young people a signal for long-term health care and social needs. JAMA Psychiatry 2014, 71, 119–127. [Google Scholar] [CrossRef]
- Moran, P.; Coffey, C.; Romaniuk, H.; Olsson, C.; Borschmann, R.; Carlin, J.B.; Patton, G.C. The natural history of self-harm from adolescence to young adulthood: A population-based cohort study. Lancet 2012, 379, 236–243. [Google Scholar] [CrossRef] [Green Version]
- Björkenstam, E.; Hjern, A.; Björkenstam, C.; Kosidou, K. Association of Cumulative Childhood Adversity and Adolescent Violent Offending with Suicide in Early Adulthood. JAMA Psychiatry 2018, 75, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Decker, M.; Wilcox, H.C.; Holliday, C.N.; Webster, D.W. An Integrated Public Health Approach to Interpersonal Violence and Suicide Prevention and Response. Public Health Rep. 2018, 133, 65S–79S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NICE. Self-Harm: Longer-Term Management; Evidence Update April 2013; Evidence Update 39; National Collaborating Centre for Mental Health: London, UK, 2013. [Google Scholar]


{kind=link}
| Childhood Adversities | 1. Violent Crime (but Not Self-Harm) | 2. Self-Harm (but Not Violent Crime) | 3. Dual Harm | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cases | Controls | Cases | Controls | Cases | Controls | |||||||
| (N = 28,596) | (N = 571,920) | (N = 25,826) | (N = 516,520) | (N = 3987) | (N = 79,740) | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| Personal risk factors | ||||||||||||
| Hospitalization due to | ||||||||||||
| Self-harm ‡ | 432 | 1.5 | 2997 | 0.5 | 925 | 3.6 | 3299 | 0.6 | 132 | 3.3 | 446 | 0.6 |
| Assault ‡ | 173 | 0.6 | 712 | 0.1 | 109 | 0.4 | 542 | 0.1 | 47 | 1.2 | 127 | 0.2 |
| Serious accident ‡ | 4522 | 15.8 | 62,868 | 11.0 | 3533 | 13.7 | 49,056 | 9.5 | 715 | 17.9 | 8498 | 10.7 |
| Parental/family risk factors | ||||||||||||
| Sociodemographic factors | ||||||||||||
| Unemployment ƚ | 3545 | 12.4 | 20,776 | 3.6 | 2847 | 11.0 | 19,361 | 3.7 | 697 | 17.5 | 3151 | 4.0 |
| Low educational attainment—both parents ƚ | 6535 | 22.9 | 61,360 | 10.7 | 5222 | 20.2 | 55,101 | 10.7 | 1116 | 28.0 | 9053 | 11.4 |
| Younger maternal age | 2268 | 7.9 | 15,336 | 2.7 | 1770 | 6.9 | 14,061 | 2.7 | 438 | 11.0 | 2449 | 3.1 |
| Older paternal age | 1529 | 5.3 | 35,531 | 6.2 | 1552 | 6.0 | 32,098 | 6.2 | 205 | 5.1 | 4826 | 6.1 |
| Residential transience ‡ | 4004 | 14.0 | 29,215 | 5.1 | 3341 | 12.9 | 27,139 | 5.3 | 791 | 19.8 | 4269 | 5.4 |
| Adverse events | ||||||||||||
| Sibling death ‡ | 905 | 3.2 | 13,496 | 2.4 | 835 | 3.2 | 12,094 | 2.3 | 159 | 4.0 | 1901 | 2.4 |
| Parental death | ||||||||||||
| External causes ‡ | 701 | 2.5 | 4986 | 0.9 | 602 | 2.3 | 4710 | 0.9 | 159 | 4.0 | 749 | 0.9 |
| Natural causes ‡ | 911 | 3.2 | 11,758 | 2.1 | 780 | 3.0 | 10,888 | 2.1 | 147 | 3.7 | 1717 | 2.2 |
| All causes | 1601 | 5.6 | 16,660 | 2.9 | 1367 | 5.3 | 15,538 | 3.0 | 302 | 7.6 | 2453 | 3.1 |
| Hospitalization due to | ||||||||||||
| Self-harm ‡ | 1995 | 7.0 | 13,252 | 2.3 | 1966 | 7.6 | 12,171 | 2.4 | 437 | 11.0 | 1946 | 2.4 |
| Assault ‡ | 1085 | 3.8 | 5119 | 0.9 | 798 | 3.1 | 4935 | 1.0 | 227 | 5.7 | 808 | 1.0 |
| Serious accident ‡ | 5661 | 19.8 | 75,776 | 13.2 | 4826 | 18.7 | 68,567 | 13.3 | 924 | 23.2 | 10,655 | 13.4 |
| Mental illness diagnosis | ||||||||||||
| Substance misuse disorder ‡ | 2422 | 8.5 | 16,268 | 2.8 | 2181 | 8.4 | 15,073 | 2.9 | 536 | 13.4 | 2359 | 3.0 |
| Any other disorder ‡ | 4468 | 15.6 | 44,290 | 7.7 | 4516 | 17.5 | 41,020 | 7.9 | 849 | 21.3 | 6142 | 7.7 |
| Violent criminality ‡ | 3619 | 12.7 | 16,459 | 2.9 | 2400 | 9.3 | 16,095 | 3.1 | 662 | 16.6 | 2521 | 3.2 |
| Child–parent separation ‡ | 13,053 | 45.6 | 162,190 | 28.4 | 11,441 | 44.3 | 148,400 | 28.7 | 2006 | 50.3 | 22,779 | 28.6 |
| Number of Childhood and Parental/Family Risk Factors | 1. Violent Crime (but Not Self-Harm) | 2. Self-Harm (but Not Violent Crime) | 3. Dual Harm | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cases | Controls | Cases | Controls | Cases | Controls | |||||||
| (N = 28,596) | (N = 571,920) | (N = 25,826) | (N = 516,520) | (N = 3987) | (N = 79,740) | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| None | 5579 | 19.5 | 239,005 | 41.8 | 5732 | 22.2 | 216,667 | 42.0 | 524 | 13.1 | 32,857 | 41.2 |
| 1 | 7875 | 27.5 | 184,573 | 32.3 | 7099 | 27.5 | 166,376 | 32.2 | 893 | 22.4 | 25,589 | 32.1 |
| 2 | 5940 | 20.8 | 83,564 | 14.6 | 5145 | 19.9 | 74,837 | 14.5 | 820 | 20.6 | 11,951 | 15.0 |
| 3 | 3739 | 13.1 | 34,288 | 6.0 | 3164 | 12.3 | 30,556 | 5.9 | 566 | 14.2 | 4926 | 6.2 |
| 4 | 2218 | 7.8 | 15,210 | 2.7 | 1867 | 7.2 | 14,026 | 2.7 | 413 | 10.4 | 2142 | 2.7 |
| 5 or more | 3245 | 11.4 | 15,280 | 2.7 | 2819 | 10.9 | 14,058 | 2.7 | 771 | 19.3 | 2275 | 2.9 |
| Childhood Adversities | IRR (95% CI) | ||
|---|---|---|---|
| 1. Violent Crime (Not Self-Harm) | 2. Self-Harm (Not Violent Crime) | 3. Dual Harm | |
| Personal risk factors: | |||
| Hospitalization due to | |||
| Self-harm ‡ | 2.92 (2.64, 3.23) | 5.83 (5.41, 6.28) | 6.12 (5.02, 7.46) |
| Assault ‡ | 4.90 (4.14, 5.79) | 4.04 (3.29, 4.97) | 7.42 (5.31, 10.38) |
| Serious accident ‡ | 1.52 (1.47, 1.57) | 1.51 (1.46, 1.57) | 1.83 (1.69, 1.99) |
| Parent/family risk factors: | |||
| Sociodemographic factors | |||
| Unemployment ƚ | 3.77 (3.63, 3.91) | 3.20 (3.06, 3.33) | 5.15 (4.71, 5.64) |
| Low educational attainment - both parents ƚ | 2.73 (2.66, 2.82) | 2.30 (2.23, 2.38) | 3.55 (3.29, 3.83) |
| Younger maternal age | 3.16 (3.02, 3.31) | 2.65 (2.51, 2.79) | 3.94 (3.54, 4.39) |
| Older paternal age | 0.85 (0.81, 0.90) | 0.96 (0.92, 1.02) | 0.84 (0.73, 0.97) |
| Residential transience ‡ | 3.03 (2.92, 3.13) | 2.68 (2.58, 2.79) | 4.38 (4.02, 4.76) |
| Adverse events | |||
| Sibling death ‡ | 1.35 (1.26, 1.45) | 1.39 (1.30, 1.50) | 1.70 (1.44, 2.01) |
| Parental death: | |||
| External causes ‡ | 2.86 (2.64, 3.10) | 2.59 (2.38, 2.83) | 4.37 (3.67, 5.20) |
| Natural causes ‡ | 1.57 (1.46, 1.68) | 1.45 (1.34, 1.56) | 1.74 (1.46, 2.06) |
| All causes | 1.98 (1.88, 2.08) | 1.80 (1.70, 1.91) | 2.57 (2.27, 2.91) |
| Hospitalization due to | |||
| Self-harm ‡ | 3.16 (3.01, 3.32) | 3.41 (3.25, 3.59) | 4.91 (4.40, 5.48) |
| Assault ‡ | 4.37 (4.08, 4.67) | 3.31 (3.07, 3.57) | 5.90 (5.07, 6.86) |
| Serious accident ‡ | 1.62 (1.57, 1.67) | 1.50 (1.46, 1.55) | 1.96 (1.81, 2.11) |
| Mental illness diagnosis | |||
| Substance misuse disorder ‡ | 3.16 (3.03, 3.31) | 3.07 (2.93, 3.22) | 5.09 (4.61, 5.63) |
| Any other disorder ‡ | 2.22 (2.15, 2.29) | 2.47 (2.39, 2.56) | 3.27 (3.01, 3.54) |
| Violent criminality ‡ | 4.90 (4.72, 5.09) | 3.19 (3.05, 3.34) | 6.11 (5.57, 6.70) |
| Child-parent separation ‡ | 3.01 (2.93, 3.10) | 2.57 (2.50, 2.65) | 4.58 (4.23, 4.96) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carr, M.J.; Steeg, S.; Mok, P.L.H.; Pedersen, C.B.; Antonsen, S.; Kapur, N.; Webb, R.T. Adverse Childhood Experiences and Risk of Subsequently Engaging in Self-Harm and Violence towards Other People—“Dual Harm”. Int. J. Environ. Res. Public Health 2020, 17, 9409. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249409
Carr MJ, Steeg S, Mok PLH, Pedersen CB, Antonsen S, Kapur N, Webb RT. Adverse Childhood Experiences and Risk of Subsequently Engaging in Self-Harm and Violence towards Other People—“Dual Harm”. International Journal of Environmental Research and Public Health. 2020; 17(24):9409. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249409
Chicago/Turabian StyleCarr, Matthew J., Sarah Steeg, Pearl L. H. Mok, Carsten Bøcker Pedersen, Sussie Antonsen, Nav Kapur, and Roger T. Webb. 2020. "Adverse Childhood Experiences and Risk of Subsequently Engaging in Self-Harm and Violence towards Other People—“Dual Harm”" International Journal of Environmental Research and Public Health 17, no. 24: 9409. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249409