Comparing the Scope and Efficacy of COVID-19 Response Strategies in 16 Countries: An Overview



Abstract
:1. Introduction
2. The Pandemic Challenged the Global Mechanisms for Coordinated Response
2.1. Politics and Early Chinese Response Issues
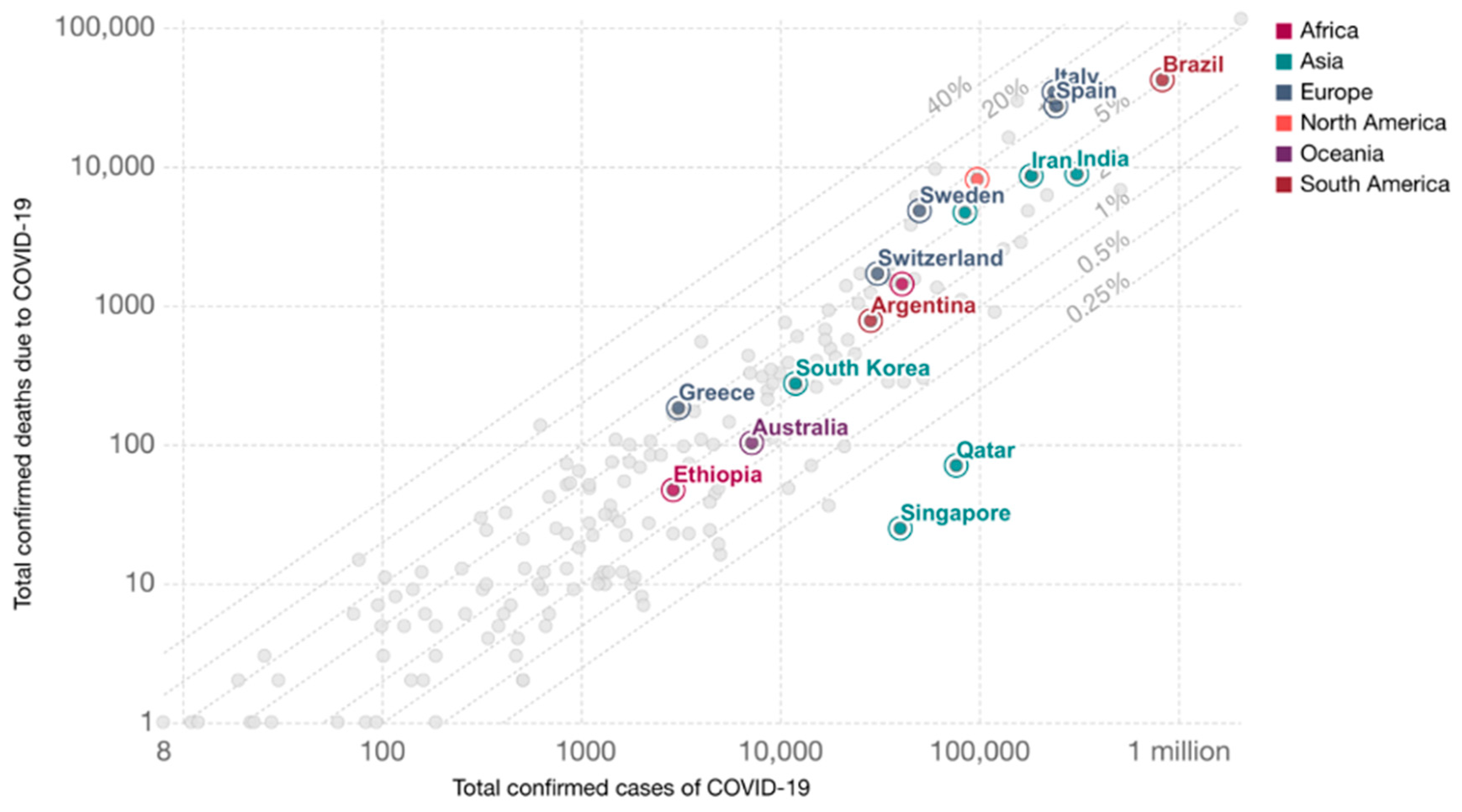
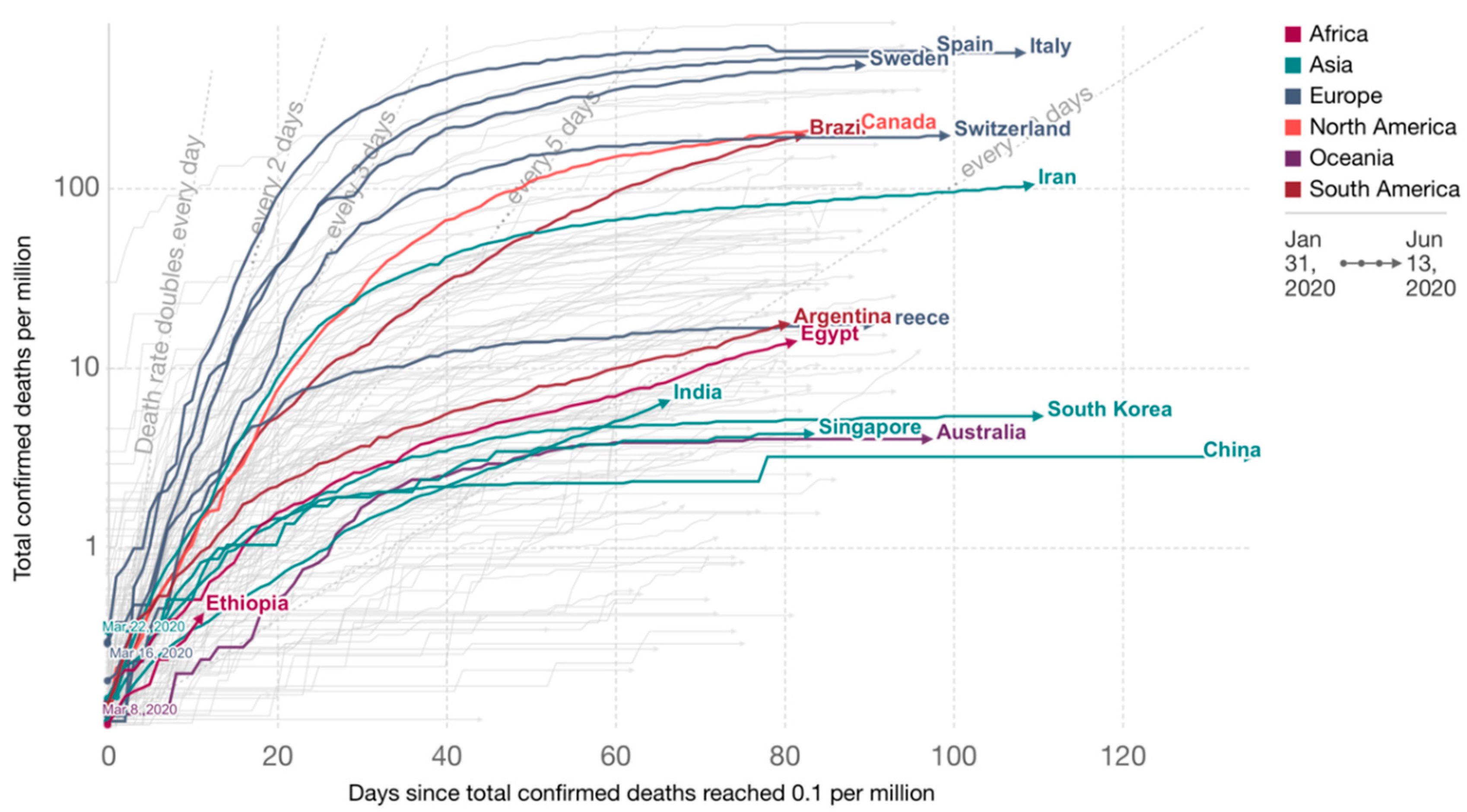
2.2. COVID-19 Epidemic Progression by Countries
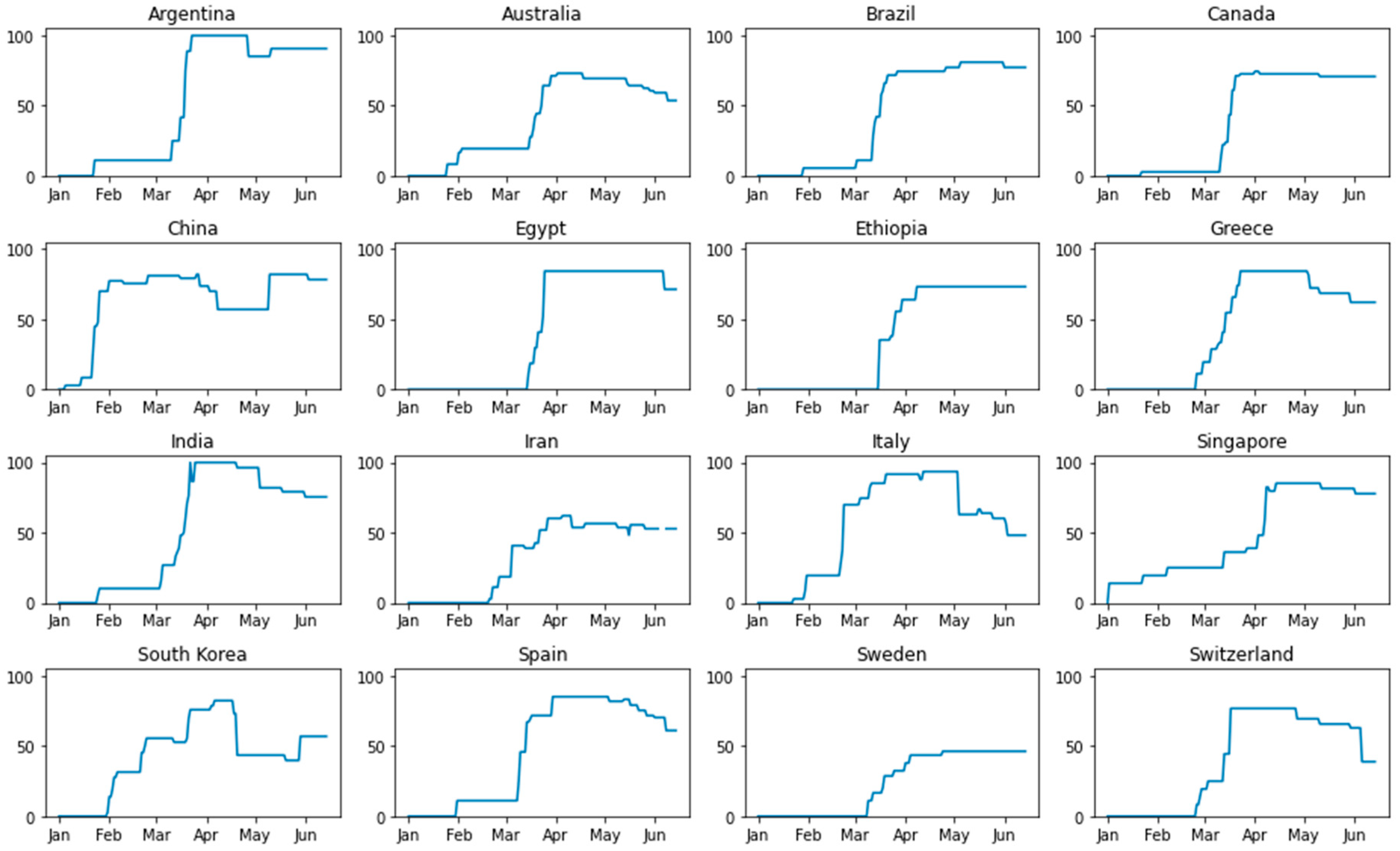
2.3. Strategies and Methods for the Response to COVID-19 Pandemic by Countries
2.3.1. Argentina
2.3.2. Australia
2.3.3. Brazil
2.3.4. Canada
2.3.5. China
2.3.6. Egypt
2.3.7. Ethiopia
2.3.8. Greece
2.3.9. India
2.3.10. Iran
2.3.11. Italy
2.3.12. Singapore
2.3.13. South Korea
2.3.14. Spain
2.3.15. Sweden
2.3.16. Switzerland
3. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Sanche, S.; Lin, Y.T.; Xu, C.; Romero-Severson, E.; Hengartner, N.; Ke, R. High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus 2. Emerg. Infect. Dis. 2020, 26, 7. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Lau, E.H.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiorillo, L.; Cervino, G.; Matarese, M.; D’Amico, C.; Surace, G.; Paduano, V.; Fiorillo, M.T.; Moschella, A.; La Bruna, A.; Romano, G.L.; et al. COVID-19 Surface Persistence: A Recent Data Summary and Its Importance for Medical and Dental Settings. Int. J. Environ. Res. Public Health 2020, 17, 3132. [Google Scholar] [CrossRef] [PubMed]
- Rombolà, G.; Hedemperger, M.; Pedrini, L.; Farina, M.; Aucella, F.; Messa, P.; Brunori, G. Practical indications for the prevention and management of SARS-CoV-2 in ambulatory dialysis patients: Lessons from the first phase of the epidemics in Lombardy. J. Nephrol. 2020, 33, 193–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cascella, M.; Rajnik, M.; Cuomo, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation and Treatment Coronavirus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2020. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK554776/ (accessed on 15 December 2020).
- Rinaldi, G.; Paradisi, M. An Empirical Estimate of the Infection Fatality Rate of COVID-19 from the First Italian Outbreak. Available online: https://0-doi-org.brum.beds.ac.uk/10.1101/2020.04.18.20070912 (accessed on 15 December 2020).
- Coronavirus: China’s First Confirmed Covid-19 Case Traced Back to November 17. Available online: https://www.scmp.com/news/china/society/article/3074991/coronavirus-chinas-first-confirmed-covid-19-case-traced-back (accessed on 15 December 2020).
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W. Severe Acute Respiratory Syndrome Coronavirus 2 Isolate Wuhan-Hu-1, Complete Genome. GenBank: MN908947.3. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/nuccore/MN908947 (accessed on 15 December 2020).
- WHO: Emergencies Preparedness, Response: Novel Coronavirus—China. Available online: https://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/ (accessed on 15 December 2020).
- Global Times: Latest Virus Outbreak Linked to Beijing Market ‘Basically Contained’. 24 June 2020. Available online: https://www.globaltimes.cn/content/1192612.shtml (accessed on 15 December 2020).
- The Mystery of the 12-Day Window of New Cases in Wuhan. Available online: https://www.yicai.com/news/100481417.html (accessed on 15 December 2020). (In Chinese).
- Imai, N.; Dorigatti, I.; Cori, A.; Riley, S.; Ferguson, N. Report 1: Estimating the Potential Total Number of Novel Coronavirus Cases in Wuhan City, China//Imperial College London COVID-19 Response Team. Available online: https://www.imperial.ac.uk/media/imperial-college/medicine/mrc-gida/2020-01-17-COVID19-Report-1.pdf (accessed on 15 December 2020).
- WHO: Emergencies Preparedness, Response: Pneumonia of Unknown Cause—China. Available online: https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-china/en/ (accessed on 15 December 2020).
- Boseley, S. China’s Handling of Coronavirus is a Diplomatic Challenge for WHO. The Guardian. 28 February 2020. Available online: https://www.theguardian.com/world/2020/feb/18/china-coronavirus-who-diplomatic-challenge (accessed on 15 December 2020).
- Policy Responses to the Coronavirus Pandemic. OurWorldInData. 26 June 2020. Available online: https://ourworldindata.org/policy-responses-covid (accessed on 15 December 2020).
- Ritchie, H.; Ortiz-Ospina, E.; Beltekian, D.; Mathieu, E.; Hasell, J.; Macdonald, B.; Giattino, C.; Roser, M. Total Confirmed COVID-19 Deaths and Cases, Countries. 2020. Available online: https://ourworldindata.org/grapher/total-deaths-and-cases-covid-19 (accessed on 15 December 2020).
- Ritchie, H.; Ortiz-Ospina, E.; Beltekian, D.; Mathieu, E.; Hasell, J.; Macdonald, B.; Giattino, C.; Roser, M. COVID-19: Government Response Stringency Index, Countries. 2020. Available online: https://ourworldindata.org/grapher/covid-stringency-index (accessed on 15 December 2020).
- Government Response to the COVID-19 Outbreak. Available online: https://www.health.gov.au/news/health-alerts/novel-coronavirus-2019-ncov-health-alert (accessed on 15 December 2020).
- Bolsonaro diz que ‘pequena crise’ do coronavírus é ‘mais fantasia’ e não ‘isso tudo’ que mídia propaga. (Bolsonaro Says Coronavirus ‘Little Crisis’ Is ‘More Fantasy’ and Not ‘All That’ the Media Propagates). Available online: https://g1.globo.com/politica/noticia/2020/03/10/bolsonaro-diz-que-questao-do-coronavirus-e-muito-mais-fantasia.ghtml (accessed on 15 December 2020).
- CTV News: Canadian Health Authority Warns Travellers over Mysterious Illness Sickening Dozens in China. Available online: https://www.ctvnews.ca/health/canadian-health-authority-warns-travellers-over-mysterious-illness-sickening-dozens-in-china-1.4757617 (accessed on 15 December 2020).
- Department of Justice Canada: Government of Canada Further Facilitates Enforcement of the Federal Quarantine Act. Available online: https://www.canada.ca/en/department-justice/news/2020/04/government-of-canada-further-facilitates-enforcement-of-the-federal-quarantine-act.html (accessed on 15 December 2020).
- Prime Minister Announces Canada’s Plan to Mobilize Industry to Fight COVID-19. Available online: https://pm.gc.ca/en/news/news-releases/2020/03/20/prime-minister-announces-canadas-plan-mobilize-industry-fight-covid (accessed on 15 December 2020).
- Smith, M. (11 September 2014). Egypt Tourist Numbers to Rise 5–10 pct in 2014—Minister Reuters. Retrieved. 9 October 2014. Available online: https://www.reuters.com/article/egypt-tourism-idUSL5N0RC3CF20140911 (accessed on 15 December 2020).
- WHO: At Least 80 Million Children under One at Risk of Diseases Such as Diphtheria, Measles and Polio as COVID-19 Disrupts Routine Vaccination Efforts, Warn Gavi, WHO and UNICEF. Available online: https://www.who.int/news-room/detail/22-05-2020-at-least-80-million-children-under-one-at-risk-of-diseases-such-as-diphtheria-measles-and-polio-as-covid-19-disrupts-routine-vaccination-efforts-warn-gavi-who-and-unicef (accessed on 15 December 2020).
- Ikkos, A.; Koutsos, S. The Contribution of Tourism to the Greek Economy in 2018; INSETE Report: Athens, Greece, 2019. [Google Scholar]
- OurWorldInData. 26 June 2020. Available online: https://ourworldindata.org (accessed on 15 December 2020).
- The Hindu: Actual COVID-19 Numbers in India May be Higher than Reported. Available online: https://www.thehindu.com/news/cities/mumbai/actual-covid-19-numbers-in-india-may-be-higher-than-reported/article31392290.ece (accessed on 15 December 2020).
- WHO Outbreaks and Emergencies/2015 MERS Outbreak in Republic of Korea. Available online: https://www.who.int/westernpacific/emergencies/2015-mers-outbreak (accessed on 15 December 2020).
- The World Bank: Population Ages 65 and Above (% of Total Population). Available online: https://data.worldbank.org/indicator/SP.POP.65UP.TO.ZS (accessed on 15 December 2020).
- Syrgasbehandling i Palliativ våRd vid Covid-19. (Oxygen therapy in palliative care at Covid-19). Available online: https://www.regiongavleborg.se/globalassets/landstinget_a-o/smittskyddsenhet/a-z/syrgasbehandling_vid_palliativ_vard_av_patienter_med_Covid-19.pdf (accessed on 15 December 2020).
- Arbetslösheten på väg Mot 600,000. (Unemployment on the way to 600,000). Available online: https://www.nsk.se/2020/04/24/finansministern-behov-av-fler-atgarder-okar/ (accessed on 15 December 2020).
- WHO: WHO/Europe publishes considerations for gradual easing of COVID-19 Measures. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/4/whoeurope-publishes-considerations-for-gradual-easing-of-covid-19-measures (accessed on 15 December 2020).




{kind=link}
{kind=link}
{kind=link}
| Country | Total Health Expenditures (%GDP) | Hospital Beds (per 1000 People) | WHO | Bloomberg, Healthcare Efficiency Rating |
|---|---|---|---|---|
| Argentina | 9.12 | 5.0 (2014) | 75 | 11 |
| Australia | 9.3 (2017–2018) 16.3 (2019) | 3.84 (2016) | 32 | 10 |
| Brazil | 9.47 | 1.98 (2018) | 125 | 54 |
| Canada | 10.57 | 2.52 (2017) | 30 | 16 |
| China | 5.15 (2017) 6.57 (2018) | 4.34(2017) | 144 | 19 |
| Egypt | 5.29 | 1.6 (2014) | 63 | |
| Ethiopia | 3.5 | 0.3(2015) | 180 | |
| Greece | 8.04 | 4.21(2017) | 14 | |
| India | 3.53 | 0.53(2017) | 112 | |
| Iran | 8.66 | 1.5(2014) | 93 | 30 |
| Italy | 8.84 (2017) 8.9 (2019) | 3.18 (2.17) | 2 | 6 |
| South Korea | 7.6 | 12.27 (2017) | 58 | 4 |
| Singapore | 4.44 | 2.4(2015) | 6 | 2 |
| Spain | 8.87 (2017) | 2.97(2017) | 7 | 3 |
| Sweden | 11.02 | 2.22 (2017) | 23 | 27 |
| Switzerland | 12.35 (2017) | 4.53(2017) | 20 | 14 |
| Country | 1st Case Date | Workplaces Closures | Face Coverings | School Closure | Cancelation of Public Events | Restrictions on Public Gatherings |
|---|---|---|---|---|---|---|
| Argentina | 3 March 2020 | 19 March 2020 | 14 April 2020 Required in all public spaces | 16 March 2020 | 11 March 2020 | 19 March 2020 <10 people |
| Australia | 25 January 2020 | 23 March 2020 Required for some | - | 24 March 2020 | 16 March 2020 Recommended 18 March 2020 Required | 16 March 2020 100–1000 people 24 March 2020, 10–100 people 29 March 2020 <10 people |
| Brazil | 25 February 2020 | 13 March 2020 Recommended 17 March 2020 Required for all | 2 March 2020 Recommended 22 March 2020 Required in some public spaces 11 April 2020 Required outside the home | 12 March 2020 | 12 March 2020 | 14 March 2020 100–1000 people 18 March 2020 10–100 people 26 April 2020 <10 people |
| Canada | 25 January 2020 | 18 March 2020 | 20 April 2020 Recommended | 16 March 2020 | 12 February 2020 | 16 March 2020 10–100 people 23 March 2020 <10 people |
| China | 1 December 2020 | 26 January 2020 | December 2019 Recommended 22 January 2020 Required in all public spaces 24 March 2020 Required in some public spaces | 26 January 2020 | 22 January 2020 | 22 January 2020 <10 people |
| Egypt | 14 February 2020 | 16 March 2020 Required for some | 26 April 2020 Required in some public spaces | 15 March 2020 | 21 March 2020 | 25 March 2020 >1000 people |
| Ethiopia | 13 March 2020 | 25 March 2020 Required for some | 8 April 2020 Required in all public spaces | 16 March 2020 Partial 25 March 2020 Full | 16 March 2020 | 16 March 2020 >1000 people 8 April 2020 <10 people |
| Greece | 26 February 2020 | 13 March 2020 Required for some | 28 April 2020 Recommended | 5 March 2020 | 29 February 2020 | 18 March 2020 <10 people |
| India | 30 January 2020 | 16 March 2020 Recommended 21 March 2020 Required for all 20 April 2020 Required for some | 2 April 2020 Recommended 9 April 2020 Required outside the home | 5 March 2020 Partial 13 March 2020 Full | 5 March 2020 Recommended 14 March 2020 Required | 19 March 2020 <10 people |
| Iran | 19 February 2020 | 26 February 2020 Recommended 22 March 2020 Required for all 11 April 2020 Required for some | - | 5 March 2020 | 21 February 2020 Recommended 22 February 2020 Required | 19 April 2020 >1000 people |
| Italy | 30 January 2020 | 22 February 2020 Required for all | 4 April 2020 Required outside the home | 23 February 2020 | 23 February 2020 | 23 February 2020 <10 people |
| South Korea | 20 January 2020 | 24 February 2020 Recommended 22 March 2020 Required for some 7 April 2020 Required for all | 15 March 2020 Recommended | 3 February 2020 Partial 5 February 2020 Full | 31 January 2020 Recommended 21 February 2020 Required 20 April 2020 Recommended | 21 February 2020 100–1000 people 22 March 2020 10–100 people 4 April 2020 <10 people 20 April 2020 No restrictions |
| Singapore | 23 January 2020 | 7 April 2020 Required for all | 3 April 2020 Recommended 14 April 2020 Required in public spaces | 8 April 2020 Full 02 June 2020 Partial | 7 February 202020 Recommended 13 March 2020Required | 13 March 202020 >250 people 27 March 2020 All |
| Spain | 31 January 2020 | 9 March 2020 Recommended 14 March 2020 Required for some 30 March 2020 Required for all | - | 9 March 2020 | 10 March 2020 | 10 March 2020 >1000 people 30 March 2020 <10 people |
| Sweden | 31 January 2020 | 25 March 2020 Recommended | 17 March 2020 Partial | 12 March 2020 | 12 April 2020 100–1000 people 29 March 2020 10–100 people | |
| Switzerland | 25 February 2020 | 17 March 2020 Required for all | 30 April 2020 Recommended | 13 March 2020 | 25 February 2020 | 28 February 2020 >1000 17 March 2020 <10 people |
| Country | Testing Policy | Contact Tracing | Stay-at-Home Restrictions | Restrictions on Internal Movement | International Travel Controls |
|---|---|---|---|---|---|
| Argentina | 32 January 2020 Symptoms and key groups | 4 March 2020 Comprehensive tracing | 19 March 2020 Required 27 April 2020 Required with exceptions | 20 March 2020 Restrict movement 27 April 2020 Recommended | 10 March 2020 Quarantine from high-risk regions 16 March 2020 Total border closure |
| Australia | 25 January 2020 Symptoms and key groups 27 April 2020 Open public testing | 25 January 2020 Comprehensive tracing | 24 March 2020 Recommended 3 April 2020 Required with exceptions | 19 March 2020 Restrict movement | 1 February 2020 Ban on high-risk regions 20 March 2020 Total border closure |
| Brazil | 23 January 2020 Symptoms and key groups | 1 April 2020 Comprehensive tracing | 13 March 2020 Recommended | 17 March 2020 Restrict movement | 13 March 2020 Quarantine from high-risk regions 19 March 2020 Ban on high-risk regions 27 March 2020 Total border closure |
| Canada | 25 January 2020 Symptoms and key groups 9 March 2020 Anyone with symptoms 19 March 2020 Open public testing | December, 2019 Limited tracing | 14 March 2020 Recommended | 20 March 2020 Restrict movement | 22 January 2020 Screening 18 March 2020 Total border closure |
| China | December, 2019 Symptoms and key groups 16 February 2020 Anyone with symptoms 31 March 2020 Open public testing | December, 2019 Limited tracing 5 January 2020 Comprehensive tracing | 23 January 2020 Recommended 1 February 2020 Required 8 April 2020 Recommended | 23 January 2020 Restrict movement 8 April 2020 Recommended | 25 February 2020 Quarantine from high-risk regions 26 March 2020 Ban on high-risk regions |
| Egypt | 14 February 2020 Symptoms and key groups | 14 February 2020 Comprehensive tracing | 25 March 2020 Required with exceptions | 25 March 2020 Restrict movement | 19 March 2020 Total border closure |
| Ethiopia | 14 February 2020 Symptoms and key groups | 13 March 2020 Limited tracing | 8 April 2020 Recommended | 26 March 2020 Restrict movement | 28 January 2020 Screening 23 March 2020 Ban on high-risk regions |
| Greece | 8 April 2020 Anyone with symptoms | - | 23 March 2020 Required with exceptions | 21 March 2020 Restrict movement | 14 March 2020 Ban on high-risk regions |
| India | 25 January 2020 Symptoms and key groups 9 April 2020 Open public testing | 26 January 2020 Limited tracing 31 January 2020 Comprehensive tracing | 26 January 2020 Recommended 22 March 2020 Required | 16 March 2020 Recommended 20 March 2020 Restrict movement | 26 January 2020 Screening 13 March 2020 Quarantine from high-risk regions 15 March 2020 Ban on high-risk regions 22 March 2020 Total border closure |
| Iran | - | - | 19 March 2020 Recommended | 5 March 2020 Restrict movement | - |
| Italy | 31 January 2020 Symptoms and key groups 26 February 2020 Anyone with symptoms | 31 January 2020 Comprehensive tracing | 23 February 2020 Required with exceptions 20 March 2020 Required 10 April 2020 Required with exceptions | 21 February 2020 Restrict movement | 23 January 2020 Screening 30 January 2020 Ban on high-risk regions |
| South Korea | 22 January 2020 Symptoms and key groups 7 February 2020 Open public testing | 29 January 2020 Limited tracing 11 February 2020 Comprehensive tracing | 23 February 2020 Recommended 21 March 2020 Required with exceptions 18 April 2020 Recommended 20 April 2020 No measures | 23 February 2020 Recommended 21 March 2020 Restrict movement 18 April 2020 Recommended 21 April 2020 No measures | 4 February 2020 Ban on high-risk regions |
| Singapore | 2 January 2020 Symptoms and key groups 23 January 2020 Anyone with symptoms | 20 January 2020 Comprehensive tracing | 3 April 2020 Recommended 8 April 2020 Required with exceptions 19 June 2020 Recommended | 3 April 2020 Recommended 8 April 2020 Restrict movement 19 June 2020 No restrictions | 2 January 2020 Screening 23 January 2020 Ban on high-risk region 10 April 2020 Quarantine from high-risk regions |
| Spain | 24 January 2020 Symptoms and key groups 5 April 2020 Anyone with symptoms 11 April 2020 Symptoms and key groups | 31 January 2020 Comprehensive tracing | 14 March 2020 Required with exceptions | 9 March 2020 Recommended | 10 March 2020 Ban on high-risk regions 17 March 2020 Total border closure |
| Sweden | 31 January 2020 Symptoms and key groups | 31 January 2020 Comprehensive tracing | 25 March 2020 Recommended | 4 April 2020 Recommended | 19 March 2020 Ban on high-risk regions |
| Switzerland | 7 March 2020 Symptoms and key groups | 15 February 2020 Limited tracing | 17 March 2020 Recommended | 17 March 2020 Recommended | 13 March 2020 Ban on high-risk regions |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rozanova, L.; Temerev, A.; Flahault, A. Comparing the Scope and Efficacy of COVID-19 Response Strategies in 16 Countries: An Overview. Int. J. Environ. Res. Public Health 2020, 17, 9421. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249421
Rozanova L, Temerev A, Flahault A. Comparing the Scope and Efficacy of COVID-19 Response Strategies in 16 Countries: An Overview. International Journal of Environmental Research and Public Health. 2020; 17(24):9421. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249421
Chicago/Turabian StyleRozanova, Liudmila, Alexander Temerev, and Antoine Flahault. 2020. "Comparing the Scope and Efficacy of COVID-19 Response Strategies in 16 Countries: An Overview" International Journal of Environmental Research and Public Health 17, no. 24: 9421. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249421